
Abstract
Objectives
Neonatal respiratory distress syndrome (NRDS) is the most common respiratory disease in preterm infants (PIs). The implication of Angiopoietin-like 4 (ANGPTL4) was reported in lung diseases. We delved into the role of serum ANGPTL4 in NRDS diagnosis/prognosis.
Methods
Totally 256 PIs were prospectively selected, including 128 NRDS infants and 128 non-NRDS PIs. NRDS infants were assigned into Survival and Death groups. ANGPTL4 level in PIs and its diagnostic and prognostic value for NRDS were separately assessed by ELISA and receiver operating characteristic curve. The independent risk factors (IRFs) for death in NRDS infants were analysed by multivariate logistic regression.
Results
NRDS infants exhibited reduced gestational age, birth weight, and 5 min Apgar score. ANGPTL4 level rose in NRDS infants, and increased with NRDS severity. Serum ANGPTL4 level was negatively correlated with 5 min Apgar score in NRDS infants. The area under the curve of serum ANGPTL4 for the diagnosis of NRDS was 0.902, with 88.28% sensitivity, 86.72% specificity, and 255.98 ng/mL cut-off value; the AUC for the diagnosis of severe NRDS was 0.741, with 66.67% sensitivity, 79.52% specificity, and 625.5 ng/mL cut-off value. Low gestational age, birth weight and 5 min Apgar score, severe NRDS, and elevated serum ANGPTL4 levels were IRFs for death in NRDS infants. NRDS infants with increased serum ANGPTL4 level displayed decreased survival rate and short survival time.
Conclusions
ANGPTL4 exhibited high diagnostic value and predictive value for death in NRDS, and it served as a biomarker for the diagnosis and prognosis of NRDS.
Keywords
Introduction
Neonatal respiratory distress syndrome (NRDS), also known as neonatal pulmonary hyaline membrane disease, is a serious respiratory disease of the newborn.1–4 NRDS is associated with immature lung development and pulmonary surfactant (PS) deficiency, which leads to progressive alveolar collapse and symptoms of severe hypoxaemia, acidosis, and hyperventilation.3,5 NRDS is common in neonates, especially in preterm infants (PIs), with an incidence of 70-93% in those born at 28 weeks gestation, and the mortality of NRDS infants is related to their body weights, with higher mortality in infants with lower body weights. 6 The clinical manifestations of NRDS are dyspnoea, cyanosis, moaning, and the inspiratory triple concave sign within the first 6 h of birth, which, if left untreated, can lead to death due to respiratory failure in severe cases.7,8 Current treatment for NRDS includes ventilator therapy, surfactant replacement therapy, prenatal glucocorticoid therapy, and oxygen therapy.9–12 Early recognition and diagnosis of NRDS are essential for timely and effective treatment to reduce neonatal mortality. Therefore, it is clinically important to find promising biomarkers to rapidly assess the condition and prognosis of NRDS.
Angiopoietin-like 4 (ANGPTL4), a member of the angiopoietin-like protein subfamily, whose expression can be prominently induced under ischaemic and hypoxic conditions, participates in various physiological effects including lipid metabolism, wound healing, and vascular injury.13,14 Notably, ANGPTL4 was documented for its implication in the pathological process of lung injuries and lung diseases, 15 serving as a biomarker for the diagnosis and prognosis of some lung diseases. For instance, ANGPTL4 expression is distinctly elevated in lung tissues of idiopathic pulmonary fibrosis (IPF), which may be a marker of early diagnosis and a target for IPF treatment. 16 Knockdown of ANGPTL4 has been shown to protect against lipopolysaccharides-induced acute lung injury by modulating SIRT1/NF-kB pathway. 17 Moreover, ANGPTL4 is not only highly expressed in lung tissues of COVID-19 patients and lung epithelial cells and fibroblasts, but also correlates with the prognosis of patients with severe COVID-19.13,18,19 More importantly, ANGPTL4 expression is substantially elevated in bronchoalveolar lavage fluid and serum of patients with acute respiratory distress syndrome (ARDS) and correlated with disease mortality and severity. 20 Therefore, serum ANGPTL4 may be an underlying biomarker for the diagnosis and prognosis for NRDS. However, the role of serum ANGPTL4 level in the diagnosis and prognosis in NRDS remains elusive. In the light of this context, we investigated the specific role of serum ANGPTL4 level in ARDS to provide a scientific basis for finding biomarkers for rapid diagnosis and evaluation of the severity and prognosis of NRDS.
Materials and methods
Ethics statement
Approval for this study was obtained from the Ethics Committee of Children’s Hospital of Shanxi (Women Health Center of Shanxi). All guardians of the newborns participating in the study signed an informed consent. The study conformed with the Declaration of Helsinki.
Sample size estimation
The sample size for this study was estimated using the G*Power 3.0.10 software (Heinrich Heine University Düsseldorf, NRW, Germany) as described previously. 12 The main indicator analysed in this study was the difference in serum ANGPTL4 level between NRDS PIs (the NRDS group) and non-NRDS PIs (the control group), as well as the differences in the NRDS Survival group and NRDS Death group and its predictive value for NRDS severity. The serum ANGPTL4 levels followed a normal distribution. A Student's t-test was performed between the NRDS group (N1) and the control group (N2) using G*Power 3.0.10 software. The test was two-tailed with the following parameter settings: α = 0.05, power (1−β) = 0.95, and a medium estimated effect size (d = 0.5). The sample sizes for N1 and N2 were set at a 1:1 ratio. The estimated sample size was N1 > 105 cases and N2 > 105 cases. In the light of the NRDS Survival group and the NRDS Death group, as well as the previous clinical experience, the survival rate and mortality rate of infants were separately assumed to be 75% and 25%. The statistical method selected was the t test in G*Power 3.0.10 software, with the parameters set as below: two-tailed test, α = 0.05, 1−β = 0.95, high estimated effect size, effect size d = 0.8, sample size N3:sample size N4 = 3:1. N3 indicated the NRDS Survival group and N4 represented the NRDS Death group. The estimated sample size was N3 > 84 cases and N4 > 28 cases, that is, the sample size of the NRDS group should be > 112 cases. Considering an attrition rate of 10-15%, 128 PIs in the NRDS group and 128 in the control group were finally included in the study, and there were no lost cases in this study.
Research subject and general information
A total of 256 PIs born in the Department of Obstetrics and Gynecology of Children’s Hospital of Shanxi (Women Health Center of Shanxi) from January 2019 to January 2023 were prospectively selected, including 128 cases of NRDS, with 128 cases of non-NRDS PIs served as the control group. General clinical data were collected, including maternal age, gestational age, sex, birth weight, mode of delivery (spontaneous parturition or caesarean section), 5 min Apgar score (five items including muscle tension, pulse, frowning action, that is, response to stimulation, appearance, respiration, with a total score of 0–10, with higher score indicating lower degree of asphyxia), and prenatal steroid treatment.
Inclusion and exclusion criteria
Inclusion criteria were as follows: (1) PIs with gestational age of 25–36 weeks; (2) infants with NRDS who met the diagnostic criteria for NRDS were included in the NRDS group.
Exclusion criteria included (1) full-term newborns; (2) the newborns had other diseases causing dyspnoea, including congenital heart disease, respiratory malformations, intrauterine pneumonia, and meconium aspiration pneumonia; (3) transient Tachypnea of Newborn; (4) a family history of hereditary haemorrhagic disorders in neonates or maternal conditions associated with coagulation abnormalities; (5) respiratory depression caused by the use of sedatives; (6) lack of informed consent from family members or legal guardians.
The diagnosis of NRDS was mainly based on clinical symptoms and imaging manifestations, 7 including onset time within 6 h, respiratory rate > 60 times/min, respiratory moaning, three depressions sign during inspiratory, dyspnoea, shortness of breath, cyanosis, intercostal, subcostal or suprasternal retraction, as well as X-ray findings of bronchial congestion, reticular shadow or white lung; laboratory standards: blood pH < 7.25, CO2 concentration > 60 mmHg, and PaO2 concentration < 50 mmHg.
Inclusion criteria for the control group: (1) PIs with gestational age of 25 to 36 weeks; (2) infants who do not meet the diagnostic criteria for NRDS.
Exclusion criteria for the control group: (1) neonates with NRDS or other diseases causing dyspnoea; (2) chromosomal abnormalities; (3) structural heart defects or malformations of other major organs; (4) lack of informed consent from family members or legal guardians.
Prenatal medication regimens for premature pregnant women
After admission to the hospital and relevant examinations, pregnant women at risk of preterm birth were given the steroid drugs betamethasone (Shenglu Pharma, Jining, Shandong, China; 12 mg intramuscular injection, twice, an interval of 24 h per time) or dexamethasone (South Land Pharmaceutical, Zhanjiang, Guangdong, China; 6 mg intramuscular injection, 4 times, an interval of 12 h per time) 1 week before labour to promote fetal lung maturation. Pharmacological intervention was also administered in cases where preterm labour was imminent and there was insufficient time to complete the entire treatment regimen.
Treatment of PIs with NRDS
PIs were closely monitored for respiratory fluctuations following delivery. In PIs with heightened respiration and moaning, non-invasive ventilation was initially employed, and the possibility of RDS was assessed through chest radiographs and clinical manifestations. In PIs with severe RDS or inadequate response to non-invasive respiratory support, endotracheal intubation and mechanical ventilation were initiated, and subsequently, 200 mg/kg of PS (Curosurf, Chiesi Pharmaceutical, Parma, Italy) was administered via endotracheal intubation within 2 h of birth. The infant was positioned in a supine posture and underwent a change in position and received 3 uniform injections of the drugs.
NRDS severity classification
The severity of NRDS was determined based on the 2017 Montreux criteria, in conjunction with clinical manifestations, chest X-ray examination and arterial blood gas analysis.7,21 Chest X-ray classification criteria were as follows: Grade I (mild): lung displayed mild frosted glass texture; Grade II (moderate): bilateral lung displayed marked reticular nodular sclerosis; Grade III (moderate): lung with air bronchogram; and Grade IV (severe): with bilateral white lung. Mild NRDS: 4 ≤ oxygen index (OI) < 8, moderate NRDS: 8 ≤ OI < 16, and severe NRDS: OI ≥ 16, where OI = (inhaled oxygen concentration × mean airway pressure × 100)/arterial oxygen partial pressure. In the light of the above criteria, the infants were categorized into mild NRDS (n = 50), moderate NRDS (n = 33) and severe NRDS (n = 45).
Serum ANGPTL4 determination
Blood (1 mL) was collected from subjects by means of plantar blood collection within 24 h of birth and centrifuged at 120g and room temperature for 10 min, with the supernatant acquired and preserved at −20°C. Serum ANGPTL4 level was measured using the Human ANGPTL4 enzyme-linked immunosorbent assay (ELISA) kit (JL15325-96T, J&L Biological, Shanghai, China).
Follow-up and grouping of NRDS infants
Based on the 28-day follow-up outcomes after disease onset, Survival was defined as neonates who were cured and discharged, while Death referred to neonates who died from NRDS within 28 days of disease onset. The mortality rate was calculated as the proportion of deaths relative to the total number of cases. 22 The differences of infants between the Survival group and the Death group in maternal age, gestational age, sex, birth weight, mode of delivery, 5 min Apgar score, prenatal steroid use, PS administration after delivery and NRDS severity were analysed.
Statistical analysis of data
Data were statistically analysed and graphed using SPSS 22.0 (IBM, Armonk, NY, USA), GraphPad Prism 8.0 (GraphPad Software, San Diego, CA, USA) and MEDCALC (20.0.15, MedCalc Software, Mariakerke, Ostend, Belgium). The Shapiro-Wilk test was utilized for normal distribution test. Normally distributed measures were expressed as mean ± standard deviation. Comparisons between two groups were made using the t test. Non-normally distributed data were presented utilizing the median (minimal, maximal) [M (Min, Max)], with Mann-Whitney U test for comparisons between two groups. Counting data were expressed as number (n) and percentages (%), with Chi-square test for comparisons between two groups. p was a two-sided test and differences were considered statistically significant at p < .05. The correlation between serum ANGPTL4 level and 5 min Apgar score was analysed utilizing Spearman’s rank correlation coefficient method, with ρ as correlation coefficient. The receiver operating characteristic (ROC) curve was plotted to evaluate the diagnostic value of serum ANGPTL4 for NRDS and severe NRDS, and its predictive value for death in NRDS infants. Independent risk factors (IRFs) for death in NRDS infants were analysed using multivariate logistics regression. As per the cut-off value of serum ANGPTL4 for predicting death in NRDS infants, NRDS infants were divided into the low-ANGPTL4 and high-ANGPTL4 groups, with their 28-day survival analysed using the Kaplan-Meier survival curve.
Results
Analyzes of baseline data of the NRDS group and the control group
Analyses of baseline data of the NRDS group and the control group.

Note. NRDS, neonatal respiratory distress syndrome. Shapiro-Wilk test was utilized to test the normal distribution. The measurement data of normal distribution were expressed as mean ± standard deviation, including maternal age. T test was adopted for comparisons between two groups. The measurement data of non-normal distribution were expressed as M (Min, Max), including gestational age, birth weight and 5 min Apgar score. The Mann-Whitney U test was employed for comparisons between two groups. Counting data were presented as number (n) and percentage (%), including sex, mode of delivery, and whether prenatal steroid medication was used or not. Chi-square test was conducted for comparisons between two groups. p was the two-side test, and p < .05 was considered statistically significant.
Serum ANGPTL4 level was up-regulated in NRDS infants and elevated with NRDS severity
As shown in Figure 1, serum ANGPTL4 level was significantly elevated in the NRDS group compared to the control group (539.9 ± 249.6 vs 173.0 ± 102.2 ng/mL) (Figure 1(a), p < .0001). Serum ANGPTL4 level in the mild, moderate and severe NRDS groups was also markedly elevated versus the control group, with the level higher in the severe NRDS group than the mild and moderate NRDS groups (Figure 1(b), all p < .0001). But no significant difference was detected between the mild and moderate NRDS groups (p > .05). Spearman’s rank correlation coefficient results displayed that serum ANGPTL4 was distinctly adversely interrelated with 5 min Apgar score (Figure 1(c), ρ = −0.3297, p = .001). Serum ANGPTL4 level was significantly elevated in NRDS infants and associated with NRDS severity. (a) ELISA to determine serum ANGPTL4 levels in the NRDS and control groups; (b) analysis of serum ANGPTL4 levels in the mild/moderate NRDS and severe NRDS groups; (c) Spearman’s rank correlation coefficient to analyse the correlation between serum ANGPTL4 level and 5 min Apgar score. Shapiro-Wilk test was applied for normal distribution test. Data of serum ANGPTL4 level were expressed as mean ± standard deviation, with t test for comparisons between two groups, and one-way analysis of variance for comparisons among groups. p was a two-sided test. **** p < .0001, ns: p > .05.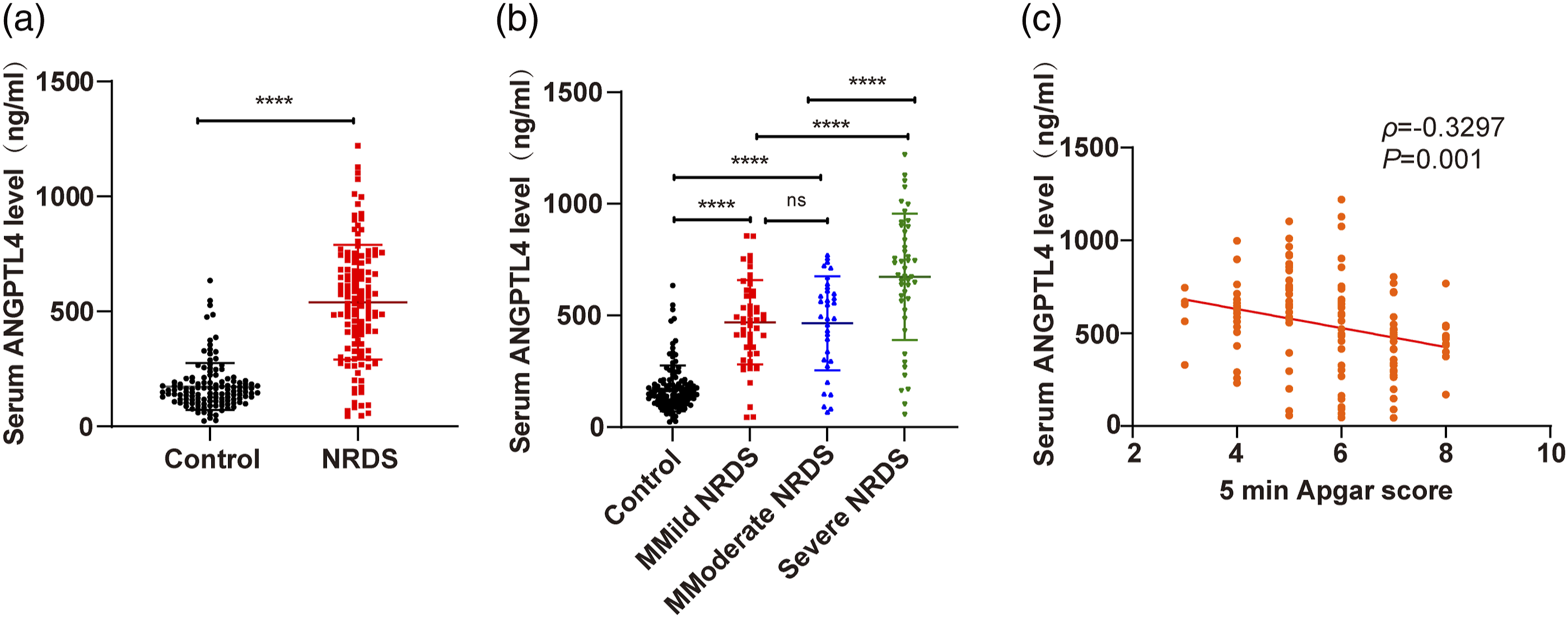
Serum ANGPTL4 level had high diagnostic value on NRDS severity
To delve into the role of serum ANGPTL4 in the diagnosis of NRDS, the diagnostic value of serum ANGPTL4 for NRDS and severe NRDS were separately analysed by ROC curves. As presented in Figure 2, the area under the curve (AUC) of serum ANGPTL4 for the diagnosis of NRDS was 0.902 (95% CI 0.859–0.936), with a sensitivity of 88.28%, a specificity of 86.72% and a cut-off value of 255.98 ng/mL (Figure 2(a), p < .0001). AUC of serum ANGPTL4 for the diagnosis of severe NRDS was 0.741 (95% CI 0.656–0.814) (sensitivity 66.67%, specificity 79.52%, cut-off value 625.5 ng/mL) (Figure 2(b), p < .0001). Serum ANGPTL4 level had high diagnostic value for NRDS severity. (a) PIs were included in the control and NRDS groups, and ROC curve was plotted to analyse the diagnostic value of serum ANGPTL4 for NRDS; (b) PIs with mild/moderate NRDS and severe NRDS were recruited, and ROC curve was plotted to analyse the diagnostic value of serum ANGPTL4 for Severe NRDS.
Baseline data analyses of the NRDS survival group and death group
Baseline data analyses of the NRDS survival and death groups.

Note. NRDS, neonatal respiratory distress syndrome; PS, pulmonary surfactant. Shapiro-Wilk test was utilized for normal distribution. Normally distributed measures were expressed as mean ± standard deviation, including maternal age. Comparisons between two groups were made using t test. Non-normally distributed measures were presented utilizing M (Min, Max), including gestational age, birth weight, and 5-min Apgar score. Mann-Whitney U test was used to compare two groups. Counting data were expressed as the number (n) and percentage (%), including sex, mode of delivery and NRDS severity. Comparisons between two groups were made using the Chi-square test. With p being a two-sided test, differences were considered statistically significant at p < .05.
Serum ANGPTL4 level had good predictive value for death in infants with NRDS
The difference in serum ANGPTL4 level between the Survival and Death groups of NRDS infants was compared. The results unveiled that ANGPTL4 level in the Death group was remarkably elevated versus the Survival group (741.2 ± 208.0 vs 451.7 ± 211.9) (Figure 3(a), p < .0001). As reflected by the results of the ROC curve analyses, the AUC of serum ANGPTL4 for predicting death in NRDS infants was 0.854 (95% CI 0.780–0.910), with a sensitivity of 87.18%, a specificity of 76.40%, and a cut-off value of 587.3 ng/mL (Figure 3(b), p < .0001). Serum ANGPTL4 level had good predictive value for death in infants with NRDS. (a) ELISA to assess serum ANGPTL4 level in the NRDS Survival and Death groups; (b) ROC curve to analyse the predictive value of serum ANGPTL4 on the death of NRDS infants. Shapiro-Wilk test was used for normal distribution test. The data of serum ANGPTL4 level were expressed as mean ± standard deviation. Comparisons between two groups were made using the t test, p was a two-sided test. **** p < .0001.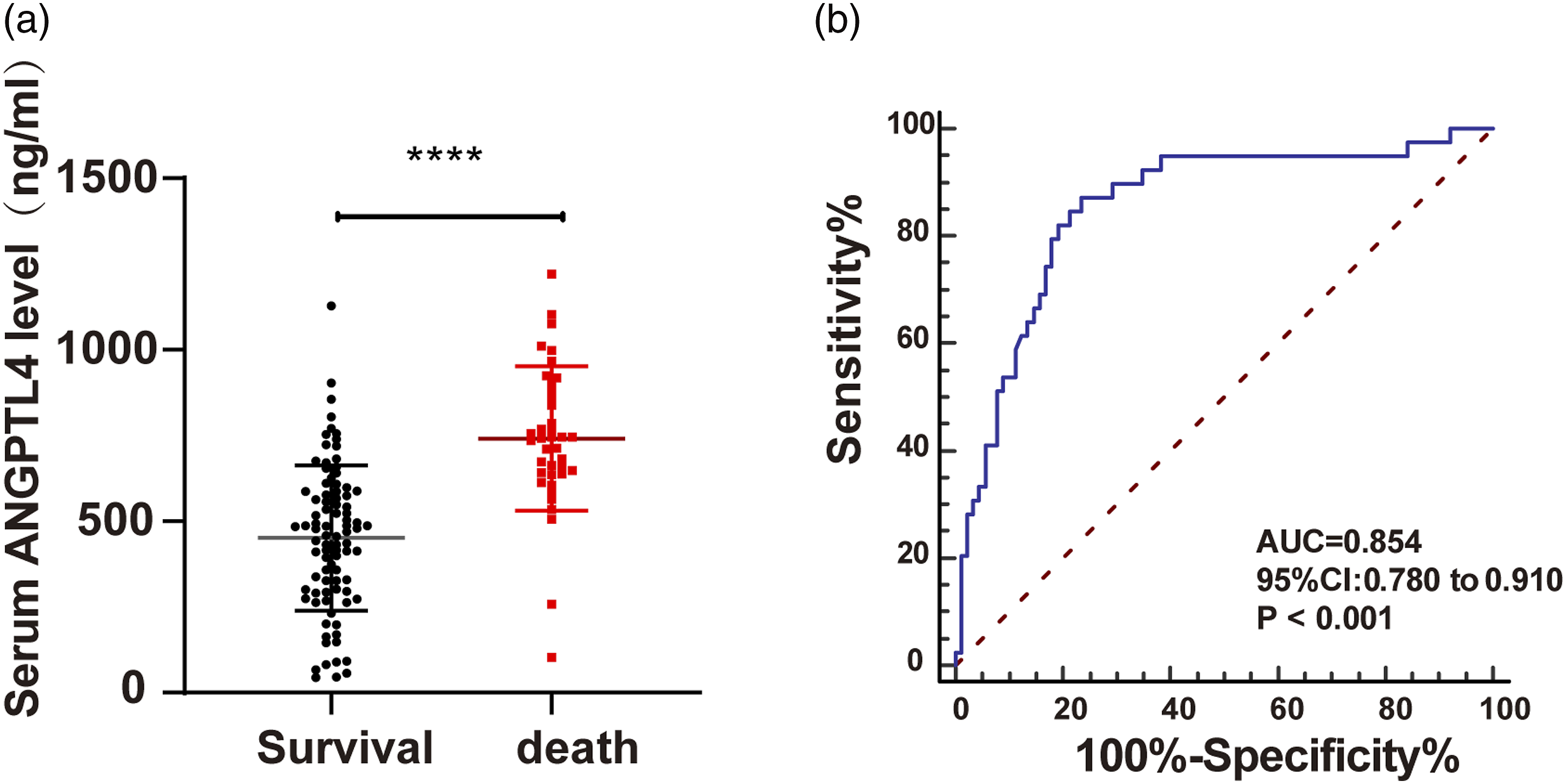
Multivariate logistic regression analyses of IRFs for death in infants with NRDS
Multivariate logistic regression analyses of IRFs for death in infants with NRDS.
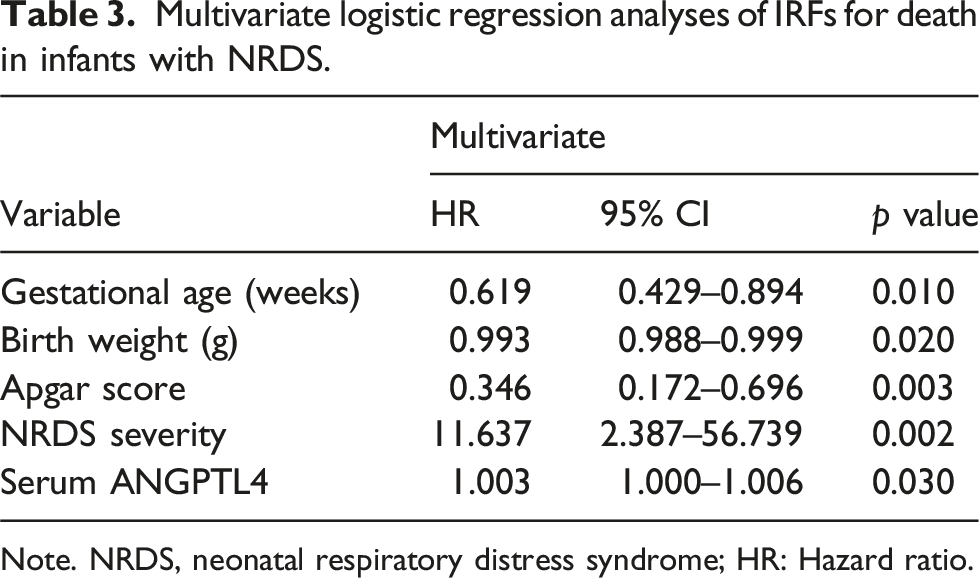
Note. NRDS, neonatal respiratory distress syndrome; HR: Hazard ratio.
Effects of serum ANGPTL4 level on survival rate and survival period of NRDS infants
Effect of serum ANGPTL4 level on survival of infants with NRDS.
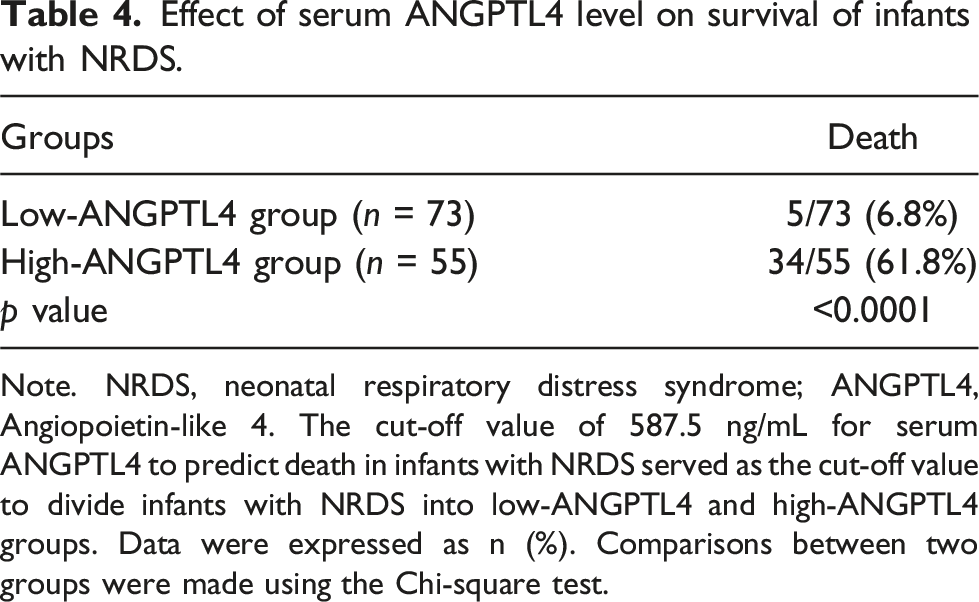
Note. NRDS, neonatal respiratory distress syndrome; ANGPTL4, Angiopoietin-like 4. The cut-off value of 587.5 ng/mL for serum ANGPTL4 to predict death in infants with NRDS served as the cut-off value to divide infants with NRDS into low-ANGPTL4 and high-ANGPTL4 groups. Data were expressed as n (%). Comparisons between two groups were made using the Chi-square test.
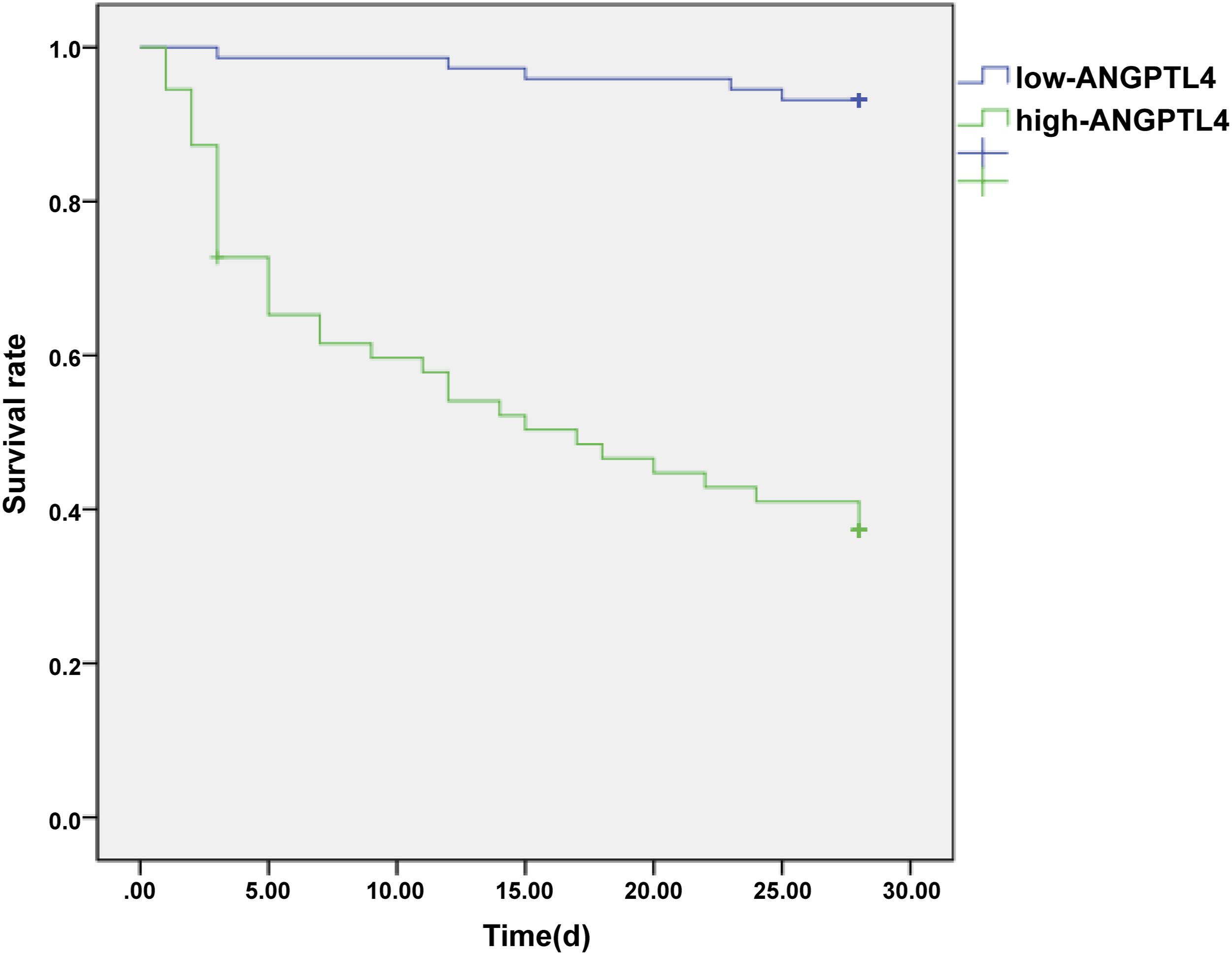
Kaplan-Meier survival curve analyses of the effects of serum ANGPTL4 level on survival rate and survival period of NRDS infants. The 28-day survival rate and survival period of infants with NRDS in the low-ANGPTL4 and high-ANGPTL4 groups were analysed by Kaplan-Meier survival curves.
Discussion
NRDS is one of the most common critical illnesses in neonatal intensive care unit,24,25 caused by a primary or secondary deficiency of PS and characterized by extensive alveolar collapse.4,26,27 Although the clinical application of neonatal PS has made significant progress by reducing the morbidity and mortality of NRDS in recent years, NRDS still poses a serious threat to the lives of newborns. 28 Therefore, early assessment of the severity and prognosis of infants with NRDS is of great significance. Evidence has shown that highly expressed ANGPTL4 was implicated in the pathological process of lung diseases, such as acute lung injury.17,29,30 Currently, the diagnosis of NRDS is still based on clinical symptoms and imaging manifestations. However, these diagnostic methods have a certain time lag and the mortality of NRDS can be reduced if timely and effective treatment measures can be taken. Therefore, there is a need to find sensitive biomarkers to help rapid diagnosis and disease classification. In this study, we defined serum ANGPTL4 as a biomarker that could assist in the diagnosis, classification and prognosis of NRDS. However, serum ANGPTL4 or other biomarkers currently still cannot replace the role of clinical symptoms and imaging in the diagnosis of NRDS.
In addition to lack of primary PS, pathogenesis of NRDS is featured by inflammatory response in the interstitium and airways, which in turn impacts the function of PS and the surfactant metabolism. 31 Serum biomarkers offer the advantage of rapidity, sensitivity, and specificity, thereby enhancing the precision of diagnostic criteria for clinical symptoms and imaging. ANGPTL comprise a class of secreted proteins structurally similar to angiopoietins, which play pivotal part in the regulation of various pathophysiological and physiological processes.32,33 ANGPTL4 belongs to the angiopoietin-like protein family and associates with lipid metabolism, angiogenesis, redox reactions, and glucose metabolism.34–37 Another prior study has unveiled that ANGPTL4 is not only involved in the regulation of previously mentioned biological processes, but also in related to the manipulation of inflammatory responses and vascular permeability in various tissues. 38 Notably, ANGPTL4 has been reported to be closely associated with inflammation and injury in the lung. 39 Upregulation of ANGPTL4 facilitates inflammation-led lung injury and increases the leakiness of pulmonary tissues, while knockdown of ANGPTL4 mitigates lung damage. 39 Accordingly, we speculated that ANGPTL4 might also play a vital role in NRDS. We used X-ray classification to determine the severity of NRDS and classified the NRDS infants into mild, moderate, and severe NRDS based on their severity. In this study, serum ANGPTL4 level was increased in severe NRDS, and had good diagnostic value for mild/moderate and severe NRDS. Our study found that the AUC for serum ANGPTL4 in diagnosing NRDS was 0.902, with high sensitivity (88.28%) and specificity (86.72%), indicating that serum ANGPTL4 has significant diagnostic value for NRDS. Furthermore, our findings disclosed that ANGPTL4 was expressed at a high level in NRDS PIs, with the expression higher in PIs with severe NRDS than with mild or moderate NRDS, but no significant difference was found between the mild NRDS and moderate NRDS groups. There is some overlap in the data among these three groups, especially between the mild and moderate NRDS groups. We further performed an ROC analysis, which showed that the AUC for serum ANGPTL4 in diagnosing severe NRDS was 0.741, with a sensitivity of 66.67% and specificity of 79.52%. The relatively low sensitivity suggests that serum ANGPTL4 has certain limitations in grading NRDS. In future studies, other inflammatory markers, such as angiopoietin-2, IL-6, and TNF-α levels 20 should be explored, for more accurate classification of NRDS, with the goal of improving the diagnostic and evaluative value of serum ANGPTL4. The 5 min Apgar score is a universal indicator of infant health at birth. 40 The 5-min Apgar score is a simple and intuitive method for quickly assessing a neonate’s health status at birth. A normal score typically ranges from 7 to 10, with lower scores indicating more severe levels of asphyxia in the neonate.40,41 Study has shown that while the Apgar score has high sensitivity in diagnosing neonatal asphyxia, its specificity is relatively low. 42 When the 5-min Apgar score is between 0 and 3, the risk of neonatal death may increase; however, it should not be considered as a sole predictor of long-term neurological dysfunction.43,44 Our findings found reduced 5 min Apgar score in the NRDS PIs, and a negative correlation between serum ANGPTL4 and 5 min Apgar score. Consistently, a clinical study has suggested that serum ANGPTL4 levels are significantly increased and closely associated with the inflammation and lung injury in patients with ARDS, thus may be a novel biomarker of ARDS prognosis. 20 We observed a positive but weak correlation (ρ = −0.3297) between the 5-min Apgar score and serum ANGPTL4 level. A possible explanation could be that serum ANGPTL4 level and the 5-min Apgar score, both of which are important tools for evaluating neonate health, reflect different physiological and pathological states. The underlying mechanisms behind this correlation still require further investigation. To conclude, serum ANGPTL4 was highly expressed in neonates with NRDS, and was elevated as the disease progressed, suggesting that serum ANGPTL4 levels were closely related to the severity of the disease of neonates with NRDS.
What’s more, ANGPTL4 expression was also demonstrated to be elevated in the Death group of NRDS PIs, which had good predictive value for the death in NRDS PIs. NRDS PIs with high-ANGPTL4 expression exhibited lower survival rate and survival time. Additionally, lower birth weight, lower gestational age, lower 5 min Apgar score, severe NRDS and higher ANGPTL4 level were the IRFs for death in the NRDS PIs. In a similar light, ANGPTL4 is expressed in pulmonary fibroblasts and epithelial cells and is related to clinical prognosis in critically ill COVID-19 patients. 13 The level of ANGPTL4 is raised in ARDS patients and markedly correlated with disease severity and the mortality. 20 Previous studies have demonstrated that certain biomarkers have significant clinical utility in the diagnosis and prognosis of NRDS. For instance, umbilical cord blood miR-375 exhibits great diagnostic and prognostic potential for NRDS and adverse outcomes in PIs, with high accuracy and sensitivity. 7 Both serum IL-17 and IL-23 manifest the ability to distinguish between patients with NRDS, particularly those with severe NRDS, and non-NRDS patients, with high sensitivity and specificity. 45 Serum biomarkers are of great clinical value as they have the advantage of being rapid, sensitive and specific, and can help improve the accuracy of diagnostic criteria for clinical symptoms and imaging. It has been documented that cesarean delivery is tied up with a reduced risk of overall neonatal mortality in comparison to vaginal delivery. 46 Caesarean section ensures early delivery of preterm infants and increases the survival rate of preterm infants. Therefore, the proportion of caesarean section in this study was relatively high, which might have contributed to the higher incidence of NRDS. Furthermore, the low average gestational age and relatively low average birth weight of the NRDS PIs included in this study may explain the high mortality rate.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Approval for this study was obtained from the Ethics Committee of Children’s Hospital of Shanxi (Women Health Center of Shanxi) (approval number: IRB-KY-2019-016). All guardians of the newborns participating in the study signed an informed consent. The study conformed with the Declaration of Helsinki.
Guarantor
XS.
Contributorship
Xiuyun Song contributed to conceptualization, methodology, validation, formal analysis, investigation, resources, data curation, writing, review and editing, and visualization.