Thyroid Function Tests: reference ranges, testing strategy, and clinical interpretation
Finlay MacKenzie1and Wassif S Wassif2
1Birmingham Quality, University Hospitals Birmingham NHS Foundation Trust
2Bedfordshire Hospitals NHS Foundation Trust
Aim: The aim was to collate and feedback data on the national picture and to highlight extremes of variation and to encourage laboratories to re-evaluate their local practice. Free Hormone and TSH assay formulations and analytical characteristics change over time as does the relative proportions of users of assays from the major global diagnostics providers. For this reason, it is important to keep up to date with the evolving practice in the UK, as it cannot be assumed older literature findings remain valid. Ranges set by one method are not necessarily easily converted to a second method.
Standards/Guidelines: The Audit was not directly comparing against any single existing guideline but was more than a simple data gathering exercise. It did use an earlier UK NEQAS for Thyroid Hormones Adult Reference Range data as a starting point and anchor to further questions. It could be considered as a re-benchmarking exercise.
Audit Method: A Survey Monkey audit was constructed with input from local and national audit leads to ascertain what the current practice across a range of patient types and demographics. This included adults, different pregnancy trimesters, paediatric, and neonates. In addition, the raw Reference Ranges themselves were collected.
Summary of Results: The number of responses varied from approximately 30 to 80, with fewest for the Paediatric and Free T3 responses.
The results confirmed our expectation about the variety of approaches in use for Paediatrics and Neonates, but there was much closer agreement for the adult and trimester-specific data.
Outcome: Audit Recommendations: For Paediatrics, the findings would suggest that a more targeted approach is required from laboratories to data mine their own Laboratory Information Systems and share data across as many sites as possible. There doesn’t seem to be any possibility of collecting data in any other way.
Telephoning urgent cortisol results and the impact of an ONDST-cortisol test code
Megan Souness and Sophie Barnes.Blood Sciences, NHS North West London Pathology, Charing Cross Hospital, London, UK
The Royal College of Pathologists communication of critical and unexpected pathology results (2017) recommend telephoning cortisol results <50 nmol/L, unless part of an overnight dexamethasone suppression test (ONDST). Accordingly, all cortisol results <50 nmol/L go to our ‘CallBack’ LIMS telephone module for immediate communication along with those 50-100 nmol/L for action the following day. Request details or clinical history are searched for evidence of ONDST. The aim of this audit was to assess the appropriateness of cortisol requesting and cortisol-related telephone calls before and after the addition of a new CORDEX test code. The new code was built following a suggestion from an Endocrinology Consultant to prevent appropriately suppressed (<50 nmol/L) post-ONDST being telephoned.
The CORDEX test code was launched in February 2024 across our six hospital sites. Lists were generated of all the cortisol results <100 nmol/L sent to the LIMS CallBack queue for a month-long period prior to and after the test code launch: 09/12/23–08/01/24 and 09/12/24–8/01/2025. Cortisol data was categorised based on the result, whether the call back was deemed clinically necessary, and whether our CallBack protocol was correctly followed by the laboratory. Audit results showed a reduction in the proportion of unnecessary results in the CallBack queue from 63% to 41%, and an improvement in the proportion of calls made for results due to genuinely suspected adrenal failure, from 24% to 52%. The new test code was requested 69 times in this period. However, 14% of ONDSTs were requested with the routine cortisol test code instead of the appropriate CORDEX code, indicating use of CORDEX could be further improved.
Recommendations following this audit include re-educating both clinicians about the availability of the CORDEX test code and laboratory staff on our cortisol CallBack criteria, in order to further reduce unwarranted telephoning.
Investigation and management of iron deficiency in patients hospitalised with heart failure: a clinical audit against ESC guidelines
Waleed Khan, Sanat Kulkarni, Grazia Bernui Vigo, Nishta Ramjee, Fatma Abdulsalam, Irene Mathias, Sungha Cho, Bernard Chan, Maria Siddiqui, Haytham Emara, Jennifer Rayner
John Radcliffe Hospital, Oxford University Hospitals NHS Foundation Trust, Oxford, UK
Aim: To assess compliance with ESC guidelines for iron deficiency testing and IV iron use in heart failure (HF) inpatients, and evaluate the impact of a teaching intervention.
Standards/Guidelines: ESC Guidelines recommend iron studies in all HF inpatients and IV iron replacement in those with iron deficiency.
Audit Method: Two-cycle audit of HF inpatients admitted to Cardiology ward/RAU. Cycle 1: Sept 2024 | Cycle 2: Feb–Mar 2025.
Intervention: Teaching session for junior doctors on guideline recommendations. Data: Demographics, Hb, iron studies, IV iron administration, discharge planning.
Summary of Results: Cycle 1: 34% had iron studies checked, 20% of eligible received IV iron. Cycle 2: 27% had iron studies checked, 38% of eligible received IV iron. No patients were referred for IV iron post-discharge in either cycle.
Outcome: Audit Recommendations:
• Include prompts within EPR for HF admissions with high NTproBNP.
• Ensure ward-level access to IV iron. Pharmacist to ensure there is enough stock in wards
• Involve HF nurses for follow-up and outpatient infusions.
• Include iron studies in HF admission checklist
Improving Post-Discharge Iron Monitoring in Heart Failure Patients Treated with Intravenous Iron: A Closed-Loop Retrospective Audit
Christos Charalambous, Nuala Pepper, Chara Rossou, Richard Andrews Lincoln County Hospital, United Lincolnshire Hospitals NHS Trust, Lincoln, UK
Aim: To determine whether post-discharge iron status follow-up in patients with heart failure with reduced ejection fraction (HFrEF) receiving IV iron meets ESC guideline standards, assessing the impact of an educational intervention.
Standards/Guidelines: The 2021 ESC Guidelines for the diagnosis and treatment of heart failure recommend reassessment of iron status 4–16 weeks after IV iron therapy, with clear discharge documentation to ensure community follow-up. Correction of iron with intravenous infusion improves symptoms and quality of life, reducing cardiovascular mortality and heart failure hospitalisations in HFrEF patients.
Audit Method: A retrospective audit of HFrEF inpatients treated with IV iron between 01/08/2023 and 31/07/2024 was undertaken (Cycle 1). Discharge summaries and electronic records were reviewed for documentation of iron follow-up and repeat iron studies within 4–16 weeks post-discharge. Following this, an educational intervention was implemented, consisting of ward posters, emails to staff, team briefings, and involvement of heart failure specialist nurses. Cycle 2 data were collected between 01/03/2025 and 15/06/2025 using the same methodology. Statistical analysis was performed using the chi-square test.
Summary of Results: In Cycle 1, 43.08% of patients (28/65) had iron follow-up documented in their discharge summaries compared with 72.92% (35/48) in Cycle 2, representing a statistically significant improvement (p=0.003). The proportion of patients who underwent repeat iron studies within 4–16 weeks also increased from 37.70% (23/61) in Cycle 1 to 61.11% (22/36) in Cycle 2, which was statistically significant (p=0.043).
Outcome/Audit Recommendations: A simple, cost-neutral educational intervention significantly improved compliance with guideline-recommended monitoring of iron status in HFrEF patients. To build on this improvement, ward posters have been refreshed, email updates were circulated to medical teams and heart failure nurses, and local GPs were informed of the findings to support continuity of care in the community.
Hearts and Budgets: Cost-Benefit Analysis of Guideline Directed Rejection Strategies for NT-proBNP
Piper, M., Ifrahim, R., Street, C., Thurston-Postle, A. Blood Sciences, Colchester Hospital, East Suffolk and North Essex NHS Foundation Trust, Colchester, UK.
Aim: At ESNEFT, we aimed to determine the magnitude and appropriateness of repeat NT-proBNP testing and develop request rejection strategies to reduce costs without compromising patient safety.
Standards/Guidelines: N-Terminal pro-B type Natriuretic Peptide (NT-proBNP) measurement is used to rule in or rule out the possibility of heart failure (HF) and determine referral for echocardiogram. Royal College of Pathologists (RCPath) and NICE guidelines recommend NT-proBNP should only be requested once in a patient’s lifetime unless there is a suspicion of new onset HF, when the condition had previously been ruled out. Within East Suffolk and North Essex NHS Foundation
Trust (ESNEFT), many patients have several NT-proBNP requests, many of which are inappropriate given their previous history. The cost of this unnecessary repeat testing is significant.
Audit Method: Of 30,234 patients analysed for NT-proBNP between October 2023 and September 2024, 400 were reviewed for NT-proBNP requests along with their clinical notes. Rejection strategies (3-, 6-, and 12-month minimum retesting intervals (MRI)) were retrospectively applied to determine potential savings and missed diagnosis rate.
Summary of Results: Results suggest that 42.8% of patients had previous results/previous diagnosis of HF and 39.3% of requests were inappropriate (RCPath guidelines). Extrapolation to the 30,234 patients indicated potential savings of up to £347,698 per year, at the risk of 5.3% (∼1587) missed diagnoses. Missed diagnosis rates (cost savings) were 2% (£2695) for 12-month repeat rejection, 0.75% (£1787) for 6-month, and 0.25% (£967) for 3-month. Extrapolation to 30,234 patients indicated 605 missed diagnoses (∼£203,746 saved), 227 missed diagnoses (£135,093 saved), and 76 missed diagnoses (∼£73,083 saved) respectively.
Outcome: Audit Recommendations: Hence, strict application of RCPath MRI guidelines results in significant missed diagnosis rate, but supports GIRFT recommendations for a 6-month repeat rejection rule which maintains patient safety. Discussion with the cardiology team will determine the final selection of MRI and rejection strategy to reduce costs and mitigate clinical risk.
Diagnostic performance of FOB-Gold and HM-JACKarc in symptomatic primary care patients
Alan Cheung and Steven McCann Blood Sciences, Stockport NHS Foundation Trust, Stockport, Uk
Aim: To perform a retrospective audit of HM-JACKarc and FOB-Gold faecal immunochemical test (FIT) results against patient outcomes to compare the performance of both assays.
Guidelines: FIT is recommended by NICE DG56 to triage symptomatic patients of suspected colorectal cancer (CRC). HM-JACKarc and OC-Sensor are recommended with a 10 µg Hb/g cut-off, whereas FOB-Gold has been reclassified as requiring further research.
Audit Method: This study assessed the outcome of FOB-Gold results between June-23 and June-24 and HM-JACKarc between June-21 and June-24 in symptomatic primary care patients. The results were correlated with outcome data (CRC v non-CRC) from the Somerset cancer register.
Summary of Results: In total, 2,663 and 15,403 patients were tested using FOB-Gold and HM-JACKarc, respectively. FIT positivity rate was 1,853 (14.2%) and 3,092 (19.2%), respectively. Outcome data was missing on 377 (20.3%) and 742 (24.0%), respectively. Cancers detected in positive referred patients were 89 (4.8%) and 132 (4.3%), respectively. As part of safety netting 617 from 11,190 patients and 2,711 from 13,053 were referred for investigations of these 9 (1.5%) and 18 (0.7%) CRC cases were found. All FIT negative patients in each group without follow-up >6 months were considered as true negatives. Using the 10 µgHb/g cut-off, the FOB-Gold CRC sensitivity was 90.8%; specificity 89.0%; PPV 6.0%, NPV 99.9%, and the ROC AUC was 0.92. For HM-JACKarc, the sensitivity was 88.0%; specificity 85.5%; PPV 5.6%, NPV 99.9%, the ROC AUC was 0.90.
Outcome: Introduction of FOB-Gold has reduced the number of positive FIT cases from 19.2% to 14.2% or decreased by 26%. The FOB-Gold cohort has shown reduced safety netting as the guidelines have changed over time. Overall, the performance of FOB-Gold was comparable with HM-JACKarc. FOB-Gold is an effective FIT assay for detection of CRC, comparable with the assays recommended by NICE DG56.
Clinical impact of interpretive comments on prolactin results
Tanya Hart Clinical Biochemistry, University Hospitals Dorset NHS Foundation Trust, UK
Aim: Do interpretive comments add value? Prolactin was chosen because our individualised interpretation is covered by an SOP, outcomes are simple to define, and we can compare to a site in our network where prolactin is reported without comment.
Standards/Guidelines: For GP patients with a new elevated prolactin result:
1) How many were referred to endocrinology?
2) How many referred patients had pituitary pathology?
3) How do results differ between Site A (interpretation) and Site B (no interpretation)?
Audit Method: Elevated historic prolactin results from GPs, for patients with no previous elevated result. Exclusions: antipsychotic monitoring, pituitary pathology, and transgender men with prolactin in the female range.
Site A: 145 results; Site B: 104 results
Site A interpretations include causes of mildly raised prolactin, medications, advice to repeat after rest, and advice to refer. Site A routinely tests for macroprolactin; Site B only at clinician request.
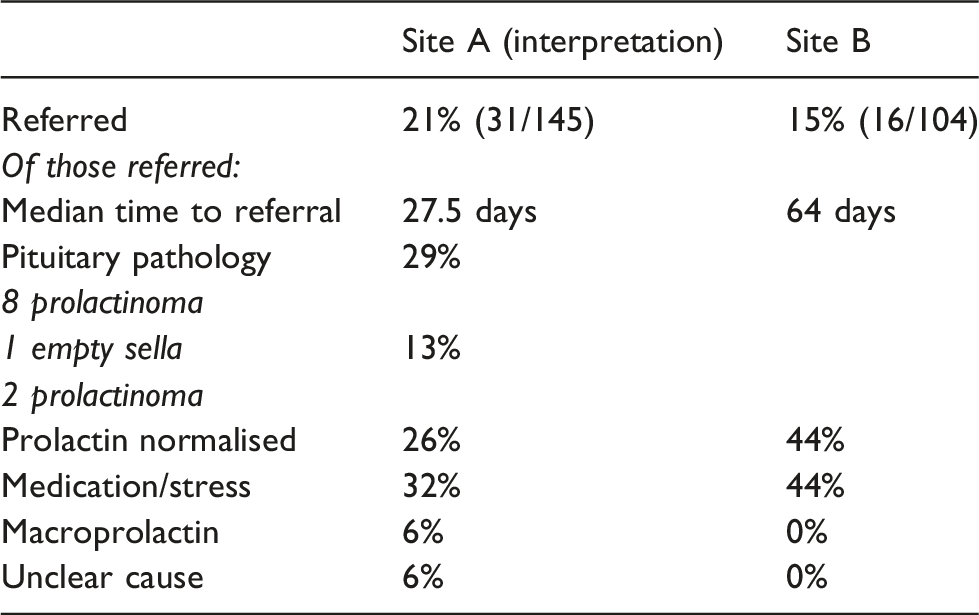
Summary of Results: At Site A, more patients were referred, but a higher percentage of those had pituitary pathology.
There was a tendency for Site B GPs to view stable raised prolactin as reassuring. Actually a persistent, stably elevated prolactin is more suspicious for prolactinoma than a fluctuating result.
Site A (interpretation)
Site B
Referred
21% (31/145)
15% (16/104)
Of those referred:
Median time to referral
27.5 days
64 days
Pituitary pathology
29%
8 prolactinoma
1 empty sella
13%
2 prolactinoma
Prolactin normalised
26%
44%
Medication/stress
32%
44%
Macroprolactin
6%
0%
Unclear cause
6%
0%
Outcome:Audit Recommendations: Test interpretation is a vital part of a laboratory service. The impact of interpretation (or lack of) can and should be audited as part of quality management.
Individualised interpretation of prolactin should be offered, to improve diagnosis of pituitary pathology.
Audit of in-use reference ranges for homovanillic acid and vanillylmandelic acid for the diagnosis of neuroblastoma in the UK
Natalie Mullee, Matthew Whitlock, Saliha Khan Clinical Blood Sciences, NHS South West London Pathology, St George’s University Hospitals Foundation NHS Trust, London, UK
Aim: Neuroblastoma is a rare childhood cancer, but it is the most common cancer within the first year of life. Homovanillic acid (HVA) and vanillylmandelic acid (VMA) are catecholamines that are measured in urine as part of the diagnostic workup of neuroblastoma. The aim of this audit was to review our local reference ranges against those in use throughout the UK.
Standards/Guidelines: Although there are guidelines for the diagnosis and management of neuroblastoma, there are no specific recommendations for reference ranges or cut-offs for HVA or VMA. The European Society for Paediatric Oncology recommends the measurement of both HVA and VMA as part of the diagnostic workup.
Audit Method: The UKAS website was searched for accredited providers of HVA/VMA using varying iterations to identify UK-based providers of these tests. Trusts or laboratory websites were then searched for their reference range information where available, method in use, and age delineations. Where this information was not publicly available, individual laboratories were contacted for their in-use ranges and sources. Lastly a search engine (Google) was used to find other UK providers of these tests for non-UKAS accredited laboratories.
Summary of Results: Reference range information was recorded from 9 UK laboratories for VMA and 11 for HVA so not all laboratories offered both tests. There were 47 different age demarcations in use across these for VMA and 54 for HVA. Despite the wide variations in age delineations in use, the reference ranges employed were broadly in agreement with some outliers. The majority of these laboratories had in house derived ranges or were from unknown historic sources.
Outcome: Audit Recommendations: Given there is limited consensus and wide variations in age delineations in use in the UK, further validation and harmonisation of reference ranges is required, particularly amongst laboratories using similar or identical methods.
Assessment of Erythropoietin Levels in Patients with Sickle Cell Disease
Dr Janan Arabi, MBBS MRes BSc and Dr Basabi Chatterjee, MBBS MRCP FRCPat 1Clinical Haematology, Homerton University Hospital, Homerton Healthcare NHS Foundation Trust, London, UK
Aim: The aim of this audit is to evaluate the appropriateness and frequency of erythropoietin (EPO) level testing in adult patients with sickle cell disease (SCD) at Homerton University Hospital. The audit seeks to identify patterns of underuse and overuse, assess alignment with clinical indications, and propose improvements to ensure EPO testing is used effectively to support patient management and optimise resource utilisation.
Standards/Guidelines: At the time of the audit, no formal national or institutional guidelines were in place regarding the frequency or indications for EPO testing in patients with SCD. Therefore, audit standards were developed based on current best clinical practice, relevant literature, and expert consensus.
Audit Method: This retrospective audit analysed a random sample of 50 adult patients with confirmed SCD who attended the Haematology Clinic within the past 13 months. Patients were categorised into three treatment groups: hydroxyurea, regular transfusions, or no treatment. The frequency and appropriateness of EPO testing were assessed across these groups.
Summary of Results: The audit revealed inconsistent testing patterns resulting in overuse among hydroxyurea-treated patients and underuse in those receiving transfusions. Statistical analysis showed that EPO levels were highest in the hydroxyurea group and lowest in the transfusion group. The absence of formal guidelines further contributed to variability in EPO testing. The findings highlight the importance of targeted, indication-based testing to optimise patient care and resource use.
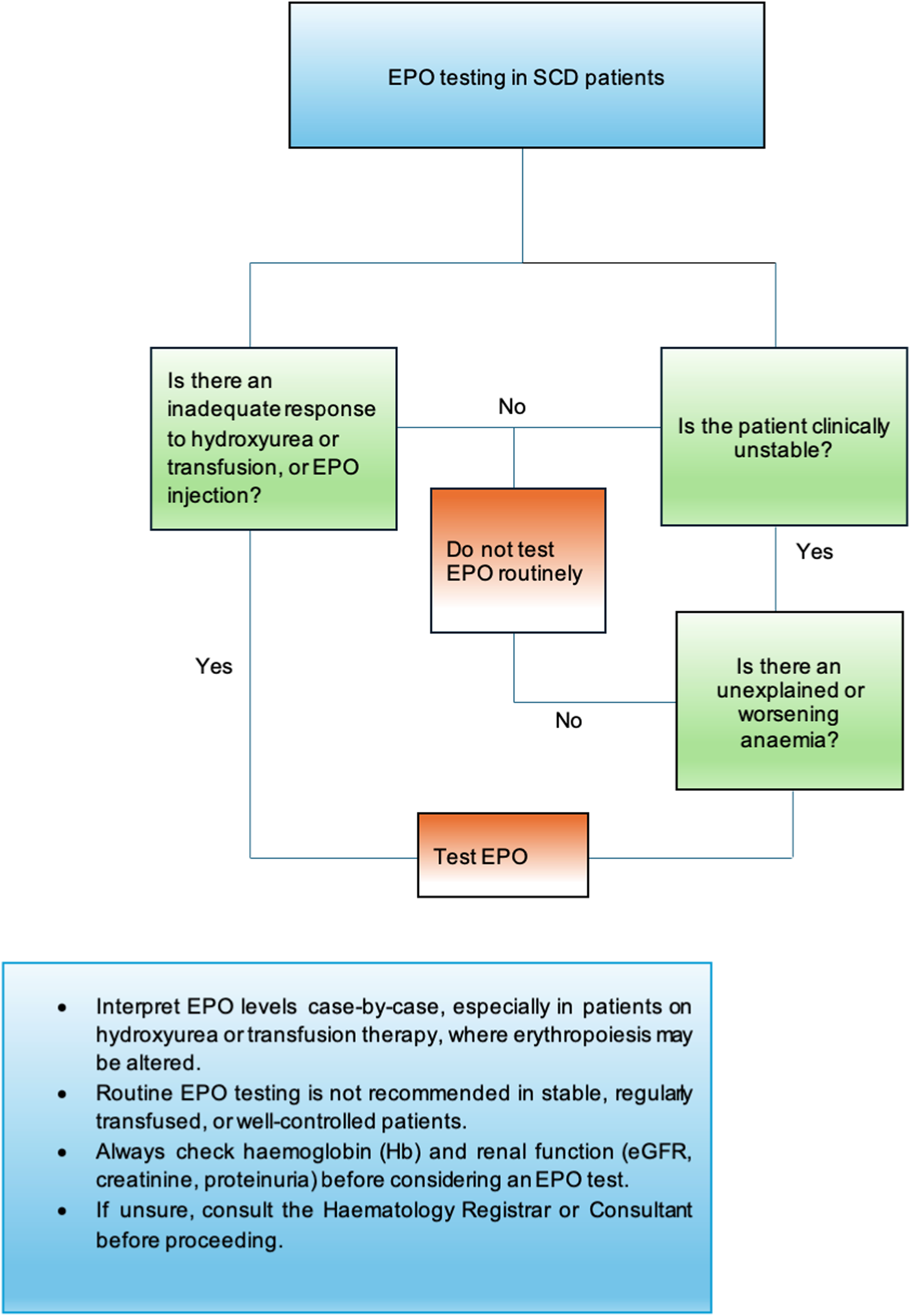
A clinical flowchart was developed as part of the audit to guide appropriate EPO ordering.
Outcome: Audit Recommendations: Recommendations included limiting EPO testing to clinically indicated scenarios (e.g., unexplained anaemia, suspected renal dysfunction, or treatment resistance) and removing it from routine test panels.
Assessing performance of LDL-C assayed by direct method compared to calculation by Friedewald and Sampson equations to improve the provision of lipid-lowering therapy
Tanmin Rahman*1, Julie Tarling*1, Sunita Sardiwal2, James Sheffield1, Stephen Quayle1, Louise Ward1, WS Wassif1
*First co-authors.
1Clinical Biochemistry, Bedfordshire Hospitals NHS Foundation Trust, Bedford MK42 9DJ
2Synnovis, St Thomas' Hospital, London SE1 7EH
Aim/Standards/Guidelines: Accurate low-density lipoprotein cholesterol (LDL-C) quantification is essential for cardiovascular disease risk stratification and therapeutic decision-making. Calculating LDL-C by Friedewald equation is simple and accessible, however demonstrates significant limitations when triglyceride ≥4.5 mmol/L or LDL-C <1.5 mmol/L.
The Sampson equation has recently been devised to calculate LDL-C, using beta quantification on 8,656 samples compared to only 448 for Friedewald, with improved accuracy for triglyceride concentrations up to 9 mmol/L and LDL-C <1.5 mmol/L.
The aim is to evaluate the clinical impact of Sampson equation implementation, in line with 2025 Heart UK and Association of Clinical Biochemistry and Laboratory Medicine guidelines.
Methods: LDL-C was calculated using Friedewald and Sampson equations on all lipid requests measured by Roche Cobas c702 analysers over 4 months; 48 samples spanning the triglyceride analytical range were also measured using the Direct Roche LDL-C method. Agreement between methods was assessed using ANOVA and linear regression and evaluated with regard to eligibility for lipid-lowering therapy according to guidelines.
Results: A total of 45,915 lipid requests were processed. No significant difference was observed between calculated and directly measured LDL-C (ANOVA F 0.24, p=0.79); although variation was greater at LDL-C <1.5 mmol/L (R2 0.76) compared to higher concentrations (R2 0.98), reflecting Friedewald’s poor performance at low LDL-C concentrations.
LDL-C could not be calculated by Sampson in 175 (0.4%) samples, compared to 1042 (2.3%) by Friedewald. Among 867 samples reportable only by Sampson, significant proportions exceeded treatment thresholds for: statin (NICE NG238; 67%), ESC/EAS risk-based targets (31-88%), inclisiran (NICE TA733; 47%), and PCSK9 inhibitor (NICE TA393/394; 1-15%).
Outcome/Recommendations: The Sampson equation significantly reduces unreportable LDL-C, thus improving cardiovascular risk assessment and identifying a substantial numbers of patients eligible for lipid-lowering therapy with moderate hypertriglyceridemia who would be missed by Friedewald. Implementation of Sampson equation is thus recommended in line with guidelines.
An audit of the incidence and causes of low serum alkaline phosphatase (ALP)
Department of Biochemistry, Broomfield Hospital, Mid & South Essex NHS Trust, Chelmsford, UK CM1 7ET.
Aim: It is reported that low alkaline phosphatase concentrations remain unnoticed and rarely followed up clinically. After excluding artefactual causes, the most common causes of low ALP are poor malnutrition with low zinc and magnesium and less commonly due to a familial condition hypophosphatasia (HPP). HPP carries considerable morbidity and yet remains largely undetected in affected individuals. The aim of this audit was to determine the incidence of low ALP in our local population with the view to delineate the potential causes.
Audit Method: Following local approval, all low ALP results defined pragmatically as less than 30 U/L with corresponding vitamin B6 (pyridoxal phosphate), magnesium, zinc, calcium, and phosphate results were gathered from our local database over the period July 2023 to July 2025. We also searched the electronic patient records for relevant clinical information.
Summary of Results: There were 2187 ALP results <30 U/L over the period examined, which was 0.4% of the total ALP requests. Of those with low ALP concentrations, 14 (0.6%) had a raised vitamin B6 concentration, 8 (0.4%) had a low Zinc concentration, and 91 (4.2%) had a low magnesium concentration. The combination of low ALP with raised vitamin B6 and the clinical presentation was consistent with a presumptive diagnosis of hypophosphatasia in all 14 cases demonstrating that the incidence of this condition may be higher than reported in the literature where the incidence of ‘mild’ presentations remains unknown. The most common presenting clinical symptom was recurrent fractures and/or joint pain.
Outcome and Recommendations: Low alkaline phosphatase concentrations remain undetected mostly due to inappropriate age-related reference intervals used and lack of flagging of such results in many hospitals. This audit highlights the importance of implementing a reflex testing protocol for low ALP to include zinc, magnesium, and vitamin B6, together with a referral pathway for the patient. We hope this study will prompt a national audit, stimulate the creation of local guidelines on the investigation of hypophosphatasia, and reignite the debate on using appropriate reference intervals.
An audit of NT-proBNP requesting in primary and secondary care settings, with insight on minimum retesting interval interventions
Ellen Donnarumma, Kia Langford-Smith, Sarah Robinson North Midlands and Cheshire Pathology Service, Leighton Hospital, University Hospitals of North Midlands NHS Trust, UK
Aim: To assess compliance of the NT-proBNP service with NICE and GIRFT guidance and assess requesting.
Standards/Guidelines: NICE NG106: Chronic Heart Failure in adults: diagnosis and management, NICE CG187: Acute Heart Failure, diagnosis and management, Getting it Right First Time – NT-proBNP April 2025.
Audit Method: A retrospective audit of NT-proBNP requests received at the four laboratories within the North Midlands and Cheshire Pathology Service, over a 4-month period, 1st January 2025 to 31st April 2025.
Summary of Results: In accordance with the guidelines, all sites and locations have access to NT-proBNP requesting, and ng/L are the reporting units. 98.0% of results are reported within 2 days. Harmonised advice and interpretation is provided based on NG106 for primary and secondary care and on NG187 for primary care only.
A total of 14,463 NT-proBNP requests were received: 8,412 (58%) from GPs, and 6,051 (42%) from secondary care. 2,621 (43%) of secondary care requests were from emergency care. Of reported results, 7,528 (57%) had a value of 0–399 ng/L, 3,157 (24%) of 400–2000 ng/L, and 2,450 (19%) of >2000 ng/L. No sex-specific differences were identified. Expected increased frequencies of lower results in primary care (76% of <400 ng/L results) were seen.
1,958 (7.39%) of all requests were received within the 6-month minimum retesting interval (MRI) in place for the network. 653 (33%) of these ‘duplicate’ requests were reinstated following clinical review, with pre-operative assessment requests having highest rates of reinstatement.
Outcome: To propose updated advice and interpretation for secondary care requests to include information on the NG187 rule-out threshold of <300 ng/L. No changes are to be made to the technical service provided by the laboratory. The minimum retest intervals are going to be clinically reviewed, particularly to discuss appropriateness of location-based NT-proBNP MRI rules.
An audit of Hospital Point Of Care (POC) INR testing in the age of Direct Oral Anticoagulants (DOACs)
de Ferrars M., Edwards C., Lampard R., Chandrajay D. Biochemistry, York hospital, York and Scarborough Teaching Hospitals NHS Foundation Trust, York, UK.
Aim: POC INR testing quickly and conveniently assesses anti-coagulation in patients prescribed Warfarin. It is contraindicated in patients on DOACs, since drug interference can cause falsely normal INRs and underestimate bleeding risk.
Despite a national decline in Warfarin prescribing since 2014, local POC INR testing has not reduced. We therefore aimed to identify whether POC INR tests were being confined to patients prescribed Warfarin.
Standards/Guidelines: Based on local SOP and Roche Coaguchek IFU:
1) 100% samples should have valid patient ID
2) 100% of patients receiving POC INR tests should be prescribed warfarin
3) INR should not be performed in patients on DOACs
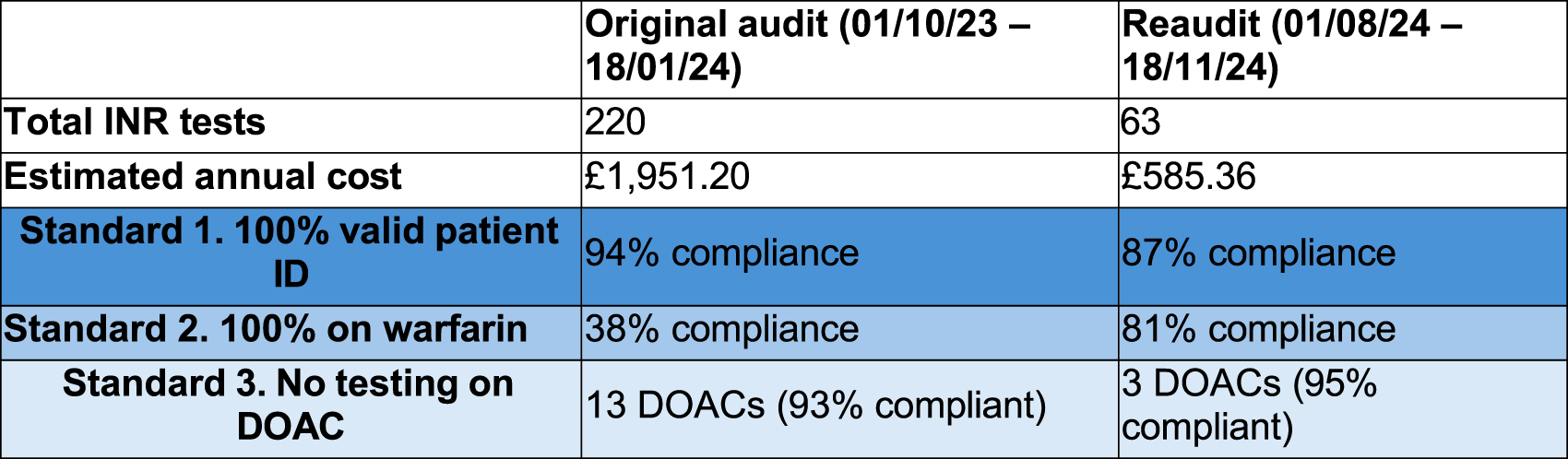
Audit Method: A list of Roche Coaguchek Pro II results, NHS numbers, test times, and meter locations was downloaded from Cobas Infinity middleware for 01/10/23–18/01/24.
Using the NHS number, medications at the time of INR testing were taken from electronic GP Records, recorded, and assessed against our standards.
A reaudit was carried out between 01/08/24 and 18/11/24 to assess the effectiveness of initial recommendations.
Summary of Results:
By promoting POC INRs in appropriate patients, our audit reduced the number of patients on DOACs undergoing tests (which will improve patient safety) and overall testing by ∼70% (may reduce costs).
Outcome: Audit Recommendations: Audit findings were presented to the endoscopy operations group and the following proposed:
- No antithrombotic medications → replace POC INR with formal pre-operative coagulation testing
- DOAC prescribed → Stop drug in line with published guidance, do not recheck INR
Remove fields on pre-operative paperwork that prompt for ‘today’s INR’
A study to assess the impact of different clinical cut-offs and analytical methods on test positive rates for asymptomatic PSA screening
Sarah Curtis and Hannah Fearon, Liverpool Clinical Laboratories (LCL), NHS University Hospitals of Liverpool Group, Liverpool, UK
Aims: To conduct a retrospective study on 45,369 primary care PSA results by three different methods to assess the impact of using different clinical cut-offs upon potential referral rates for further investigation of prostate cancer, and to assess the impact of known method-related differences.
Guidelines: The European Association of Urology (EAU, 2025) recommends primary care physicians further investigate asymptomatic males with PSA >3.0 µg/L, while NICE CKS Diagnosis of Prostate Cancer (2025) states that PSA >3.0 µg/L in asymptomatic males is ‘raised’. There are different, age-related, PSA cut-offs outlined in NICE NG12 for those with symptoms.
Methods: All PSA requests over one year were obtained from four laboratories using three methods and inclusion criteria applied. These 45,369 results comprised the total PSA set. A ‘screening’ subset of 10,970 results was produced by exclusion of all requests containing any of 71 clinical detail phrases suggestive of prostate cancer.
Results: Median PSA varied between methods, correlating with bias shown in external quality assurance (EQA) reports. LCL (Roche, positive bias on EQA) produced the highest median for all age categories >50 years, and COCH (Beckman, negative bias on EQA) the lowest. The proportion of ‘raised’ results when symptomatic age-related cut-offs were applied to 50–69 year olds in the ‘screening’ subset was 9.1% across all laboratories, increasing to 15.2% using the asymptomatic cut-off. For individual laboratory datasets, the proportion of raised results was 4% (COCH), 5% (STHK, WHTH), and 11% (LCL). When the asymptomatic cut-off was applied, positive rates rose at all laboratories; to 13% (COCH), 14% (STHK), 15% (WHTH), and 20% (LCL).
Recommendations: Laboratories should request the reason for PSA tests, reporting appropriate reference intervals to ensure results are flagged correctly. Laboratories should educate clinicians on the bias between different analytical platforms and the impact that this may have on the proportion of patients exceeding the clinical cut-offs for further investigation.
A regional audit of investigation of hypertension
Heather Stoddart, Ellen Ridler Blood Sciences, Frimley Park Hospital, NHS Berkshire and Surrey Pathology Services, UK
Aim: There are various guidelines for the investigation of the biochemical causes of secondary hypertension.
This audit aimed to:
- Review practice in pathology laboratories across London and the south of England and compare to the published standards
- Identify areas for improvement and harmonisation
- Publish standards
Standards/Guidelines: National and international guidelines exist for Primary Hyperaldosteronism (Endocrine Society 2016), phaeochromocytoma (Endocrine Society 2014), and Cushing’s disease (Pituitary Society, 2021).
Audit Method: A questionnaire was distributed to members of the Association for Laboratory Medicine in the region. The questionnaire was divided into three sections (Cushing’s syndrome, phaeochromocytoma, and primary hyperaldosteronism), and covered areas including the recommended first and second line tests, the assays in use, pre-analytical factors including patient preparation, and consideration of specific patient groups.
The results were compiled and presented at the meeting of the Thames Audit Group in November 2024.
Summary of Results: 14 responses were received. There was variation in the tests recommended, likely due to local availability, but largely this was in line with guidelines. There were variations in reference ranges quoted which were not explained by the assay used. There was variation in advice offered to clinicians with regard to patient preparation including medication and timing/patient position for sampling.
Outcome; Audit Recommendations: Regional standards were agreed at the meeting and subsequently published on the Association for Laboratory Medicine website. Briefly, some areas for improvement identified include
1) The use of cortisol reference ranges and cut-offs appropriate for the analytical method
2) Advice regarding the choice of tests for investigation of Cushing’s syndrome in patient groups where standard tests may be misleading
3) The inclusion of 3-methoxytyramine in metadrenaline profiles
4) Availability of advice regarding the effect of medications on metadrenalines
5) The use of seated or supine reference ranges for plasma metadrenalines for confirmatory testing for primary hyperaldosteronism
A National Audit on Wilson Disease
Nicola L Barlow1, Chris Harrington2, Aftab Ala3, James Liu Yin3, Louise J Ward4 and Wassif S Wassif4
1Clinical Biochemistry, Black Country Pathology Services, Sandwell Health Campus, UK; 2Berkshire and Surrey Pathology Services, Guildford, UK; 3Institute of Liver Studies, King’s College Hospital, London, UK; 4Clinical Biochemistry, Bedford Hospital, Bedfordshire Hospital NHS Foundation Trust, UK
Wilson Disease is a rare autosomal recessive disorder of copper metabolism, which can lead to hepatic, neurological, and psychiatric manifestations.
The audit aimed to capture current clinical and laboratory practice around screening for, diagnosing, and monitoring treatment of Wilson Disease. A questionnaire was distributed to LabMed members via Survey Monkey. The findings were critically assessed against BASL (2022), EASL (2012), and AASLD (2022) guidance.
The 52 respondents represented secondary care and paediatric hospitals, and specialist Wilson Disease centres.
Only 36% (n=18) of respondents had a clinical protocol for Wilson Disease, commonly as part of a liver protocol (n=11) with no neurology or laboratory involvement. Exclusion of Wilson Disease using age featured in nine (50%) protocols. Eleven sites used the Leipzig diagnostic scoring system.
To assess suspected Wilson Disease, routinely performed tests included caeruloplasmin, serum copper, 24h-urine copper excretion, and haemolysis markers. Tests occasionally performed included, the D-penicillamine challenge test and random urine copper, whilst the copper-65 absorption test and calculated non-caeruloplasmin bound copper were rarely used. Nine sites indicated use of D-penicillamine challenge tests in adults.
Diagnostic cut-off values provided for caeruloplasmin were: <0.04–0.2g/L (strongly suggestive); <0.15–0.35g/L (may support); and <0.15–0.45g/L (unlikely); and for 24h-urine copper: >1.6 or >4.0µmol/24h (strongly suggestive); >0.55–1.6µmol/24h (may support); and <0.1–1.0µmol/24h (unlikely).
Routine tests for treatment monitoring included caeruloplasmin, serum copper, and 24h-urine copper. Few or no sites used urine zinc excretion, random urine copper, or calculated non-caeruloplasmin bound copper. A wide range of 24h-urine copper treatment monitoring thresholds were provided by respondents.
A standardised UK approach would reduce variation in practice due to use of different guidance, for example, use of D-penicillamine challenge tests or varying diagnostic thresholds. Practice contrary to all guidance needs to be addressed, for example, excluding Wilson Disease using age, D-penicillamine challenge tests in adults, random urine copper for diagnosis, and over-requesting of serum copper.