
Abstract
On 11 March 2020 the World Health Organization declared the novel coronavirus outbreak (COVID-19) a global pandemic. At the time of writing, over 16 million cases of COVID-19 had been confirmed worldwide, and more than 650,000 people had died from the virus. A priority amongst governments globally is limiting the spread of the virus. In Australia, this response included mandatory ‘lockdown’ restrictions which limited citizens’ freedom of movement. This article uses survey data from 1595 Australians to examine compliance with COVID-19 lockdown restrictions in the early stages of the pandemic. Results revealed that a substantial number of Australians did not comply fully with the measures. Further, while self-interest and health concerns motivated compliance, normative concerns regarding duty to support the authorities dominated compliance decisions. The findings’ implications for both compliance research and for authorities wanting to nurture voluntary compliance with public health orders are discussed.
Introduction
Australia’s first confirmed case of COVID-19 was reported on 26 January 2020. In the ensuing weeks, Australia’s cases rapidly increased and authorities moved to contain the outbreak. On 15 March, acting on the advice of Australia’s Chief Medical Officer, Prime Minister Scott Morrison announced a series of immediate, mandatory restrictions. The restrictions, mostly implemented and enforced by state and territory governments, limited public gatherings and freedom of movement. Border restrictions were introduced, and many businesses, schools and universities closed. Only four reasons for leaving one’s house were allowable: travelling to and from medical appointments or work, shopping for ‘essential’ supplies, and exercise. People were also forbidden from socialising with friends or family. ‘Social distancing’ became a new household term, and people were directed to keep physical distance from others if they had to leave the house.
Naturally, the introduction of mandatory restrictions created enhanced enforcement. Police were granted powers to issue on-the-spot fines of AUD$1600 to those caught leaving their home without a legitimate excuse. Depending upon violation severity, fines could exceed AUD$10,000. Police were also granted powers to arrest non-compliant individuals, and courts were given powers to imprison non-compliers for up to six months.
As lockdown restrictions continued into April and May, signs emerged that Australians had become restless in social isolation and had become complacent in abiding by restrictions. Thousands of infringement notices were issued to those flouting lockdown restrictions. For example, by 3 May, Queensland Police had issued 1664 fines totalling more than $2 million (Cartwright, 2020), and by 21 May, Victoria Police had issued more than 5719 fines totalling more than $9.4 million (Zagon, 2020). On May 10, anti-lockdown protests occurred in Melbourne, resulting in 10 arrests.
Australia had early success in controlling the COVID-19 outbreak (approx. 7000 confirmed cases and 100 deaths at the end of the lockdown period). Part of this early success was due to the willingness of many Australians to comply with lockdown restrictions. However, ensuring continued and widespread public support for, and compliance with, restrictions that limit personal liberties is a tenuous game. In a country where citizens expect freedom of movement, long-term restrictions can become increasingly difficult for authorities to maintain.
Our article examines Australians’ compliance with the COVID-19 lockdown restrictions in the early stage of the pandemic, and explores the factors that motivated compliance behaviour. The article draws on survey data from 1595 Australians five weeks after lockdown restrictions began. Before presenting the findings, we review the criminology and public health literature, identifying factors that motivate peoples’ willingness to comply with laws and to adopt protective health behaviours during pandemics.
Why do people comply with laws?: A criminology perspective
Criminological research shows that compliance is motivated by instrumental and normative concerns. Instrumental models of compliance suggest that people are rational self-interested actors who act to maximise personal benefits and minimise personal losses (e.g., Murphy, 2008). For example, individuals assess criminal opportunities and risks associated with legal compliance and obey the law when the risks of non-compliance outweigh the benefits. Here, risk assessment primarily drives compliance. The assumption that individuals are rational actors influences how authorities deter non-compliance. For example, authorities use deterrent messaging to convey that potential offenders will be caught and punished (e.g., fines, arrest) if they disobey laws. This strategy was implemented in Australia in response to COVID-19. Police were granted powers to enforce lockdown measures through issuing fines or threatening arrest if people purposely flouted lockdown restrictions.
Importantly, research shows that legal sanctions do not guarantee compliance. Studies show that increasing the severity of fines or threatening arrest does little to encourage voluntary compliance with laws (e.g., Pratt et al., 2008). Increasing the probability of detection has more success (Nagin, 2013), but again in many contexts the probability of being caught and punished for violating laws is often low. Authorities therefore rely on people perceiving the risk of detection to be high. Indeed, research shows that individuals can be deterred from non-compliance if they perceive legal sanctions to be certain (see Murphy et al., 2016).
When applying the instrumental perspective to compliance during a pandemic, we must also consider that viral infections can instil fear and anxiety in a population. The rational choice perspective in criminology would suggest that if an individual believes they are at increased risk of serious illness from COVID-19, this will serve as a deterrent to non-compliance. That is, those in ‘at-risk groups’ (i.e., aged 65+ or with co-morbid disease) may comply more readily with restrictions as their risk perceptions may be heightened. However, assessments of risk may have limited utility if people are not in an at-risk group. At the time of writing, females in their twenties were most likely to have COVID-19 in Australia, yet most deaths have occurred in those aged over 60 years. Moreover, the death rate (deaths/reported cases) sits at around 1% (health.gov.au). As such, deterrence as the sole strategy for compelling all people to abide by laws is questionable in these circumstances.
The limits of the instrumental perspective have led criminologists to focus on the importance of normative factors when explaining why people comply with laws. As Tyler (2006, p. 4) explains, a ‘normative perspective leads to a focus on people’s internalized norms of justice and obligation’. Research demonstrates that persuasion and education encourage normative compliance with laws because they promote a sense that people should comply with laws because ‘it is the right thing to do’ (e.g., Murphy, 2008). This normative perspective of compliance moves thinking away from a purely instrumental ‘what’s in it for me’ mentality. When introducing the COVID-19 restrictions, the Australian Government explained that due to the dangers of COVID-19, social distancing restrictions would save lives. Here, the Government was appealing to Australians’ sense of altruism and duty, insinuating that it is important and morally right for all people to abide by lockdown restrictions to save vulnerable peoples’ lives.
Studies show that when people feel a greater duty to support and obey an authority’s decisions, they comply more readily (e.g., see Jackson et al., 2015; Murphy, 2008; Murphy et al., 2016; Tyler, 2006). Duty to support and obey authorities is generally developed from a young age through a process of legal socialisation (Tyler & Trinkner, 2017). This process teaches children that they should abide by laws and that authorities are legitimate and should be supported. Importantly, people may disagree with laws or restrictions that limit their civil liberties. However, the duty to support an authority involves people recognising that social order requires laws and that compliance with laws should take precedence over their own personal self-interest. Studies find that duty to authorities predicts compliance, even when controlling for perceptions of sanction risk (e.g., Murphy et al., 2016; Tyler & Jackson, 2014).
Trust in authorities is also important for encouraging voluntary compliance (Goldsmith, 2005). Governments play a central role in managing disease outbreaks. Public health research reveals that trust in authorities can predict compliance with health recommendations during pandemics. Trust in the public health literature, however, is usually measured as trust in the ‘competence’ of authorities to handle disease outbreaks (see next section). Criminological research also reveals that when people trust authorities to act with integrity, and to be fair and benevolent, they are also more likely to comply with their decisions and laws (see Goldsmith, 2005; Murphy et al., 2014).
Finally, prior research shows that differences between individuals can predict compliance. Men are generally less compliant than women, and younger people are generally less compliant than older people. Gender and age effects have been explained by the fact that women tend to be more prosocial than men (Bennett et al., 2005), and men and youth are less risk-averse (Leigh, 1999).
In sum, compliance behaviour is motivated by a combination of demographic, instrumental and normative factors. However, criminological research consistently reveals that normative, not instrumental, factors tend to dominate people’s decisions to comply with laws, even after controlling for demographic differences (e.g., Jackson et al., 2015; Murphy et al., 2016; Tyler, 2006).
Compliance in pandemics: A brief summary of public health research
Numerous studies have been undertaken in Australia and abroad to understand people’s willingness to comply with public health recommendations during disease outbreaks (for a meta review see Bish & Michie, 2010). To date, existing Australian studies are limited as they only ask people about their knowledge of pandemics, or their intention to comply with public health orders in the event of a hypothetical pandemic (e.g., Barr et al., 2008; Brown et al., 2010; Eastwood et al., 2009). While ‘intention to comply’ was high in Australian studies, the underlying factors associated with such intentions were not studied. Hence, why people might comply with public health restrictions during a real pandemic in Australia has not been studied before.
Several international studies provide evidence that perceptions of health risk and trust in authorities are associated with compliance with official advice in a pandemic. The literature related to the H1N1 influenza pandemic of 2009 revealed that people were more likely to say they would comply with health recommendations if they perceived themselves to be at greater risk of catching H1N1, if they perceived H1N1 to be a severe virus, and if they felt they could control their risk of catching H1N1 (e.g., Bish & Michie, 2010; Prati et al., 2011). Rubin et al. (2009) also showed that people with higher trust in the UK government’s handling of the H1N1 influenza outbreak were more likely to say they would follow recommendations to alter behaviour (e.g. wash hands more regularly; not visit a friend; self-isolate if diagnosed with influenza). A Hong Kong study amid the Severe Acute Respiratory Syndrome (SARS) outbreak of 2003 similarly found that trust in the government’s ability to control the spread of the pandemic was associated with higher compliance with health recommendations (Tang & Wong, 2003). Prati et al.’s (2011) Italian study, in contrast, found mixed evidence for trust in authorities. Trust in authorities only predicted uptake of vaccination and use of tissues during the H1N1 outbreak. Relatedly, a qualitative study from Canada found that inconsistent information from authorities led individuals to question the credibility of available information, which negatively affected their willingness to quarantine if sick (Cava et al., 2005).
Finally, research shows that individual differences can predict compliance with recommendations during pandemics. Greater knowledge of pandemics or how diseases are transmitted and higher levels of general anxiety are both associated with greater adoption of precautionary behaviours. Further, women and older respondents comply more readily with public health recommendations, but results regarding educational attainment, employment status and ethnicity yield inconsistent findings (see Bish & Michie, 2010 for a meta-review).
Despite being in the early stages of the COVID-19 pandemic, there is a rapidly emerging body of research into the public response to the virus. For example, in an unpublished study, Kooistra et al. (2020) found that duty to obey the law in the UK was associated with people’s enhanced compliance with COVID-19 restrictions, but sanction risk mattered little to compliance. In another American study, Wise et al. (2020) found that feeling personally at risk of contracting COVID-19 predicted a greater propensity for Americans to engage in hand washing and social distancing behaviours during the pandemic. However, the perceived severity of COVID-19 and the perceived consequences of the virus to others were not associated with these protective behaviours. Harper et al. (2020) surveyed adults in the UK and asked them about their self-perceived risk of contracting COVID-19, general anxiety/fear of the virus, and political orientation. The authors found that the only predictor of social distancing and improved hand hygiene was general anxiety/fear of COVID-19. There was no effect of the other social or politically relevant variables (see also Brouard et al., 2020).
The current study
The review of the literature demonstrates that various factors are associated with peoples’ compliance with laws, and their compliance with public health recommendations specifically. The limitation of many of the public health studies cited above, however, is that they: (1) asked people about their intention to comply with restrictions should a pandemic emerge; and (2) asked about people’s willingness to engage in ‘recommended’ behaviours to limit the spread of the disease. No study included a full complement of demographic, instrumental and normative variables known to predict compliance with restrictions during a mandated lockdown period affecting the entire population of a country.
The COVID-19 pandemic is the first global pandemic in 100 years. Further, in previous localised pandemics, quarantine and stay-at-home orders only applied to those who displayed flu-like symptoms. In the context of COVID-19, entire populations worldwide have been issued stay-at-home orders. Compliance with COVID-19 lockdown restrictions have also been enforced in many countries. Due to these unprecedented conditions, there is clearly much to learn about why people may or may not comply with mandatory pandemic lockdown restrictions. Understanding factors linked to public compliance with COVID-19 restrictions in Australia will help to inform preparedness for future outbreaks and pandemics.
The current article uses survey data to examine compliance with the COVID-19 lockdown restrictions implemented across Australia. 1 It does so in the early stages of the pandemic when preventative measures were most necessary but after people had already experienced five weeks of lockdown. This was a period of time when both complacency and fatigue over restrictions had begun to set in. By situating the current study in Australia, where freedom of movement has never before been restricted by a pandemic, the study extends prior research in two ways. First, it examines compliance with public health restrictions that have been mandated and enforced by law in an entire population in the early stages of a global pandemic. Second, the article extends prior research by examining an extensive range of criminological and public health factors known to be associated with compliance. As such, the relative importance of demographic, instrumental, and normative factors can be fully tested in the current study.
Methods
Participants and procedure
We draw on survey data collected from a national sample of 1595 Australians. 2 The anonymous survey was administered online through Facebook and was fielded for three weeks between 24 April and 15 May 2020. While there are limitations associated with using Facebook surveys (e.g., sample representativeness; difficult to calculate response rates), they are inexpensive and provide quick turnaround to researchers wishing to collect data on time-finite or topical subjects. This feature was imperative considering the time-sensitive nature of the research. The survey was advertised five weeks after Australian state and territory governments implemented lockdown restrictions. The advertisement was targeted at Facebook users who were 17+ years and currently living in Australia.
A total of 3175 Facebook users clicked on the survey link, but only 1773 Australians completed the survey in full. Of the 1773 completed surveys, 178 participants failed to correctly answer validity-checks. As such, they were deleted from the final data file, leaving 1595 complete and valid responses for analysis (or 50.2% of those who clicked on the survey link). Respondents were aged 17 to 89 years (M = 49.82; SD = 14.47), 56.5% were female, and 77.2% were born in Australia. Table 1 presents the profile and representativeness of those who completed the survey against Australian population estimates. The sample was broadly representative, but consistent with many surveys, women, those with university degrees, and those in the 55–64 age bracket were over-represented. Respondents living in Queensland were also over-represented, perhaps because the survey was conducted by a Queensland-based University.
Sample (N = 1595) representativeness against Australian census data.

*ABS proportions calculated without 0–14 year olds.
#Source: Australian Bureau of Statistics.
Measures
The survey included 227 questions (see survey technical report: Murphy et al., 2020). Questions canvassed respondents’ background, attitudes to police and government, attitudes regarding enhancing police powers during the pandemic, views regarding the virus, compliance with lockdown restrictions, and the impact that lockdown restrictions had on participants’ lives (e.g., loss of employment, well-being). Below are the measures used in this article. The independent variables are organised into instrumental, normative and demographic categories. Prior to forming scales, all multi-item variables were subjected to a factor analysis and items loaded as expected onto their own factor (see Appendix 1). Where multi-item scales were used, the mean score was computed (with the exception of compliance). Table 2 presents the correlations between all scale items. Exact wording of the measures is presented below or in Appendix 1.
Correlations between instrumental and normative variables.
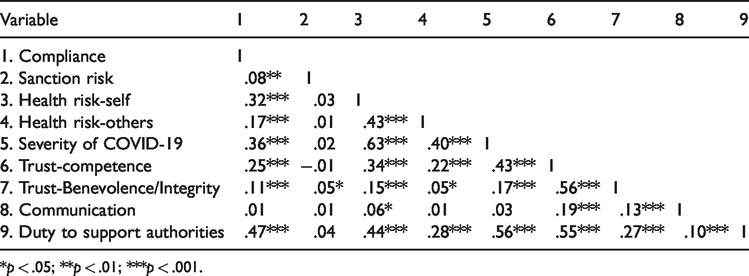
*p < .05; **p < .01; ***p < .001.
Dependent variable
Compliance. The dependent variable was self-reported compliance with COVID-19 lockdown restrictions. Respondents were asked how often they had engaged in five restricted behaviours during the previous week. Items were measured on a 1 = never, 2 = rarely, 3 = sometimes, 4 = often, 5 = very often scale. Due to skewness, each item was recoded (a response of (1) was recoded to ‘1’, while responses to (2), (3), (4) and (5) were recoded to ‘0’). The number of ‘1’ scores were then summed across the five recoded items to produce a compliance index ranging from 0 (full non-compliance) to 5 (full compliance); higher scores on this summative compliance index indicate greater compliance (M = 3.01, SD = 1.48; alpha = .80). This compliance index was normally distributed.
Independent variables–instrumental concerns
Sanction risk. Police were given powers to arrest or issue infringement notices to those caught flouting COVID-19 restrictions. Participants were asked about the likelihood of someone getting caught engaging in each of the five behaviours listed in the compliance scale (measured on a 1 = not at all likely to 5 = very likely scale). A higher score on this 5-item scale indicates greater perceptions of sanction risk (M = 2.19; SD = .79; alpha = .89).
Health risk of COVID-19 (to self and others). The perceived health risk posed by COVID-19 was measured in two ways. The first 1-item measure asked about its perceived risk to the respondents’ own physical health (‘How much of a threat do you believe COVID-19 poses to your personal physical health?’.) The second 1-item measure asked about its risk to others’ health (‘How much of a threat do you believe COVID-19 poses to a loved one’s physical health’). Both items were measured on a 1 = no threat to 5 = very high threat scale; higher scores on each indicate COVID-19 is perceived as a greater health risk (‘health risk-self’ M = 3.09; SD = 1.15; ‘health risk-others’ M = 3.29; SD = 1.23).
Severity of COVID-19. The perceived severity of COVID-19 was measured via one item (‘How serious a threat do you think the COVID-19 virus poses for the health of all Australians?’; measured on a 1 = no threat to 5 = a significant threat to all scale). Higher scores on this item indicate COVID-19 is deemed a more severe illness (M = 3.49; SD = 1.18).
Independent variables–normative concerns
Trust in authority (competence-based and benevolence/integrity-based trust). Public health studies have measured trust as confidence in authorities’ competence to handle pandemic outbreaks. Trust can also result from integrity and benevolence assessments. In the current study, trust in authority is measured two ways: as competence-based trust and as benevolence/integrity-based trust (integrity and benevolence were combined into one trust scale based on the factor analysis revealing one factor, not two – see Appendix 1).
Competence-based trust was measured via a 4-item scale asking respondents about their confidence in authorities to handle the COVID-19 pandemic (i.e., Federal Government and health authorities, State Government and health authorities). Items were measured on a 1 = no confidence at all to 5 = a lot of confidence scale, with higher scores indicating higher trust in the competence of the authorities (M = 3.32; SD = 1.12; alpha = .91). Benevolence/integrity-based trust was also measured via a 4-item scale. Respondents indicated how much they agreed that the Federal Government had acted with integrity or in the best interests of all Australians (measured on a 1 = strongly disagree to 5 = strongly agree scale). Higher scores on the benevolence/integrity-based trust scale indicate higher trust (M = 2.45; SD = 1.17; alpha = .95).
Consistency of communication. Governments that provide inconsistent/contradictory messages during pandemics risk damaging public trust (Khosravi, 2020). A 1-item measure gauged perceptions about whether the Federal and State Governments had provided conflicting advice about what citizens should do during the COVID-19 outbreak (‘Both the Federal Government and State/Territory Governments are giving conflicting advice from each other around what I need to do during the Coronavirus crisis’). The item was measured on a 1 = strongly disagree to 5 = strongly agree scale, with a higher score indicating they thought conflicting advice had been given (M = 3.18; SD = 1.65).
Duty to support authorities. The 5-item ‘duty to support authorities’ scale captured participants’ sense of obligation to support the government during the COVID-19 crisis. Respondents were asked about the extent to which they agree that it is everybody’s duty to support the Government by not engaging in the five behaviours in the compliance scale (measured on a 1 = not at all everybody’s duty to 5 = completely everybody’s duty scale). Higher scores on this scale indicate a stronger duty to support the authorities (M = 3.79; SD = 1.17; alpha = .87).
Independent variables–demographic/control variables
Demographic variables were also measured: age, gender (0 = male; 1 = female), ethnicity (0 = minority; 1 = Caucasian), employment status (0 = unemployed; 1 = employed), country of birth (0 = overseas; 1 = Australia), and educational attainment (1 = no/limited formal schooling to 9 = post-graduate degree). Four additional control variables also measured: time, general anxiety/fear, political affiliation, and knowledge about COVID-19. The time variable controlled for the day in which the survey was completed (a higher ‘time’ score indicated the survey was completed further into lockdown). The general anxiety/fear scale was created by combining responses to two survey items (‘Since the start of the COVID-19 outbreak in Australia, how often have you felt the following emotions?: (a) worry; (b) fear’; measured on a 1 = never to 5 = always scale); higher scores indicate greater anxiety/fear (M = 2.85; SD = 1.00; alpha = .83). Political affiliation was measured with: ‘Some people talk about “left” (e.g. Australian Labour Party; Greens), “right” (e.g. Liberal National Party; One Nation), and “centre” to describe political parties and politicians. With this in mind, where would you place yourself in terms of your support for political parties?’; measured on a 1 = very left-wing to 4 = centre to 7 = very right-wing scale; M = 3.37; SD = 1.53; 50.7% of the respondents reported being ‘left-leaning’, 27.0% reported being ‘centre’, and 22.3% reported being ‘right-leaning’). Finally, self-reported knowledge about COVID-19 was measured with one item (‘How would you rate your knowledge of COVID-19?’; measured on a 1 = bad to 5 = excellent scale; M = 4.28; SD = .67); a higher score indicates greater knowledge.
Results
Compliance
The full compliance rate (i.e., those who responded ‘never’) for each of the five COVID-19 restrictions were as follows: (1) socialised in person with friends/relatives you don’t live with (49.7%); 3 (2) left the house without a really good reason (54.5%); (3) travelled for leisure (60.4%); (4) went shopping for essential or non-essential items with COVID-19 symptoms (94.1%); and (5) went shopping for non-essential items when healthy (42.8%). Only 21.2% of the sample complied with all five restrictions (i.e., those scoring 5 on the summative compliance index); 2.5% did not comply with any of the five restrictions (i.e., those scoring 0 on the compliance index); 18.5% complied with one restriction, 17.4% complied with two, 19.4% complied with three, and 21.0% complied with four restrictions. Overall, these findings reveal that not all people complied fully with the lockdown restrictions.
Full compliance with each of the five restrictions was also examined amongst participants who completed the survey in the first seven days of the study (N = 638) and again after 14 days (N = 963). This accounted for the fact that in some states and territories, restrictions began to ease in early May before the survey link closed. After seven days, full compliance across all five restrictions was observed by 26.0% of the sample; after 14 days, full compliance was observed by 23.2% of the sample. Hence, compliance decreased slightly over time (correlation between time and compliance; r = −.133, p < .001).
Regression: Factors associated with compliance
Table 3 presents the results of a regression where compliance was the dependent variable. Data screening and assumption testing revealed no issues with the data. Independent variables were entered into the regression model in separate blocks to explore the relative contribution of demographic/control variables (Block 1), instrumental concerns (Block 2) and normative concerns (Block 3) on compliance. Table 3 shows that demographic and control variables explained about 10% of the variance in compliance, instrumental concerns contributed 9%, and normative concerns contributed another 9% to the variation explained. Due to the large number of variables in the model, and to account for Type I errors, only regression coefficients significant at p ≤ .01 are discussed as significant.
Regression: compliance with Australia’s COVID-19 restrictions (N = 1595).

Note. Bolded coefficients represent those that are significant at p < .01 or less. *p < .05; **p < .01; ***p < .001.
Table 3 shows that time was significant across all three blocks: people were less compliant the longer they had experienced lockdown. Of the other control variables, women were more likely than men to comply with the lockdown restrictions, and this continued even after taking account of the instrumental and normative variables in Blocks 2 and 3. Older respondents were also more likely to say they had complied. Political conservatives were less likely to say they had complied with the COVID-19 restrictions when compared to political liberals, but this relationship disappeared in Block 2. Similarly, while heightened anxiety/fear was associated with greater compliance in Block 1, this variable was not significant once instrumental and normative factors were considered. Knowledge of COVID-19 had no effect.
In Block 2, two instrumental variables were associated with compliance at the p < .01 level. Those who perceived there to be a greater risk to their own personal health reported being more compliant, along with those who perceived COVID-19 to be a more severe illness. Interestingly, neither sanction risk nor perceiving COVID-19 as a health risk to others was associated with compliance at p < .01. Importantly, the two significant instrumental effects discontinued being associated with compliance once respondents’ normative concerns were considered in Block 3.
In Block 3, neither of the two trust in authority measures were associated with compliance. However, ‘duty to support authorities’ was positively and strongly associated with compliance; those who felt a greater duty to support authorities reported being more compliant. Of all the variables in the model, duty to support authorities dominated compliance with COVID-19 restrictions in this Australian sample.
Finally, to account for the fact that restrictions had eased in some states and territories in the final week of the study, we repeated two regression analyses for survey respondents who completed the survey in the first seven days of the study (N = 638), and those who had completed it after 14 days (N = 963). The significant and insignificant findings in Block 3 of each analysis were identical to the full sample (N = 1,595) analysis; and duty to support authorities dominated decisions to comply even in the early period of the survey when lockdown restrictions had not been eased anywhere in the country. 4
Discussion
The COVID-19 pandemic provides a unique opportunity to examine factors associated with compliance with mandatory public health orders. Drawing on prior research from both criminology and public health, our study sought to determine which factors were associated with compliance with COVID-19 lockdown restrictions in Australia. Some of our results are consistent with prior research on compliance in pandemics, some are inconsistent. For example, we found that women and older people were more likely to comply with the COVID-19 restrictions. These findings are unsurprising given the fact that older people are at greater risk of serious illness from COVID-19, and health research often finds women and older people are more compliant with health directives (Bish & Michie, 2010). No other demographic/control variables were associated with compliance in our study once instrumental and normative concerns were taken into account.
Confirming prior public health research, we also found that people were more compliant when they perceived COVID-19 to pose a greater risk to their own health and when it was perceived to be a more severe disease (c.f., Plohl & Musil, 2020). Interestingly, however, concerns about personal health risks seemed more important in our study, while thinking the virus posed a health risk to others had no association with respondents’ compliance behaviour. Consistent with Kooistra et al.’s (2020) UK research, we also found sanction risk had no significant effect on compliance.
Importantly, we found no instrumental variables were associated with compliance once participants’ normative concerns were accounted for. Instrumental theories of compliance suggest that people are self-interested and comply with laws primarily due to a fear of consequences for doing otherwise (e.g., risk of legal sanctions; risk of illness in the case of COVID-19). Our results suggest that even in a context where one might expect assessments of health risk to dominate decisions, Australians cared less about health risks to them or to others and seemed more motivated to comply with COVID-19 restrictions out of a sense of duty to support authorities. In fact, duty to support the authorities dominated Australians’ decisions to comply with lockdown restrictions.
Implications for scholarship and practice
Our findings align with prior criminological research that shows that normative concerns, not instrumental concerns, are generally more important for fostering people’s intrinsic motivation to obey laws. Specifically, the criminology literature shows that duty to support and obey authorities is key to understanding why people obey laws voluntarily (Jackson et al., 2015; Tyler, 2006). The legal socialisation literature explains why this is so. Children are taught from an early age by parents and teachers that it is important to obey rules and to respect and support authorities (Tyler & Trinkner, 2017). Children are also taught that it is important to put aside their own personal desires and to act in altruistic ways to benefit others. As such, normative reasons to comply with regulations take precedence over instrumental concerns. These attitudes about laws and authorities transcend into adulthood and continue to shape how individuals interact with the law.
Intrinsic feelings of duty to support authorities are especially important in contexts where directives or laws are unpopular (Jackson et al., 2015). COVID-19 lockdown restrictions, for example, abruptly and significantly curtailed the freedoms of everyday citizens. Engaging in activities that violate these restrictions would not normally be considered morally or legally wrong. Socialising with friends, travelling for leisure, or shopping are normal everyday activities that have only been criminalised due to the introduction of COVID-19 public health orders and restrictions. While unpopular, many people have complied with these restrictions. Hence, our results confirm just how important feelings of duty can be in shaping voluntary compliance with unpopular laws.
While our analysis suggests that instrumental concerns regarding health and severity risks matter less once normative concerns are considered, it is certainly possible that instrumental concerns continue to indirectly impact compliance through the mediating influence of duty to support authorities. An additional regression revealed that both the perceived ‘severity’ (b = .44, SE = .03, ß = .44, p = .00) and ‘health risk-self’ (b = .14, SE = .03, ß = .14, p = .00) variables in our study were strongly associated with duty to support the authorities. Two Sobel tests revealed that the ‘severity’ (z = 9.76, p < .001) and ‘health risk-self’ (z = 4.62, p < .001) effects on compliance were both fully mediated by respondents’ duty to support the authorities. Given that the health consequences of COVID-19 are substantial, these findings suggest that health risk perceptions may enhance individuals’ sense of duty to authorities during a health crisis, which in turn increases their compliance with authority instructions.
Notably, and contrary to previous criminology and public health research, trust in authorities did not predict compliance in our study. Perhaps the characteristics of the COVID-19 pandemic increased the salience of duty to support authorities and decreased the salience of trust in authorities because the consequences of non-compliance have very tangible and potentially deadly consequences. In such contexts trust may become less relevant. It is possible that people may be more willing to support the government, even a poorly trusted government, if they believe compliance can reduce the risk of serious harm to themselves or loved ones. Public health studies often find that trust in authorities is important in pandemics. However, those studies generally fail to take account of the public’s duty to authorities. Had they done so, they too may find that duty trumps trust.
Importantly, our study revealed that perceived risk of legal sanctions played little role in predicting Australians’ compliance with lockdown restrictions (c.f., Kooistra et al., 2020). This finding is particularly interesting as it has implications for government responses to the COVID-19 pandemic. Our findings show that authorities cannot rely solely on legal sanctions to force compliance. Rather, authorities need to focus most on continuing to educate and remind citizens that COVID-19 is dangerous and they cannot become complacent in their compliance with restrictions. Importantly, authorities need to continue to persuade citizens that everyone has a duty to protect those most vulnerable to the disease. In other words, people should be asked to obey these regulations because they have a responsibility to act to protect others.
To an extent we are seeing examples of this. Businesses are encouraging patrons to use hand sanitizer before entering stores, they set limits on the number of people allowed inside stores, and they remind patrons to maintain their social distance from others. A helpful tactic for authorities may be to also remind the public to regularly ask friends and family to maintain their personal hygiene and restrict their movements when possible. Bennett and Mazerolle (2020) provided some practical tips for how police officers could play their role. As enforcers of public health orders, police play a critical role in encouraging people to comply with restrictions. Bennett and Mazerolle (2020) recommended that police adopt a procedurally just dialogue when interacting with the public and made suggestions for the type of verbal script officers could use in interactions. Procedural justice involves being respectful, communicating trustworthy motives, acting in a neutral manner and allowing citizens to voice concerns. Research on procedurally just dialogue consistently finds that when police are perceived as acting in a procedurally just manner, people feel a greater duty to support them and to cooperate willingly with laws (e.g., Tyler, 2006).
It is important for authorities to reiterate we are ‘all in this together’. That said, effectively marketing moral responsibility and duty to others will likely prove a public relations challenge, involving a fine balance between citizens’ freedom and state mechanisms for compliance. This raises obvious questions about how authorities should deal with those who openly question the credibility of government advice and disregard their duty. When people morally object to authorities and their rules it can be very difficult to encourage compliance with procedural justice strategies alone (Murphy, 2016). Punishment has its place, and some people simply require sanctions. But if done poorly, a heavy-handed approach can be fraught with difficulty, further entrenching resistance and negative views of authority (Murphy, 2016). It is therefore important for authorities to ensure that punishment does not destroy all vestiges of an individual’s duty to do right by the authorities or others. In the event that authorities must administer infringements to non-compliers, doing so in a procedurally just manner may avoid a situation where the non-compliers can criticize how the authority acted when issuing the infringement.
Limitations
Before concluding, it is important to acknowledge our study’s limitations. Our data are cross-sectional in nature. We suggested that heightened duty to support authorities is important for understanding compliance during a pandemic. However, without using longitudinal survey methods determining the causal relationships between the variables in our study cannot be ascertained. Our study also relied on participants’ honesty when answering questions. While responses were anonymous, and compliance rates were much lower than we expected, many participants may have been reluctant to divulge their actual rate of non-compliance. Further, it is possible that duty rather than self-interest was most strongly associated with compliance due to respondents answering in a socially desirable way. That is, people justified their compliance behaviour as being motivated by their duty to others, rather than due to self-interest. Finally, we acknowledge that at the time of data collection our study was situated in a country experiencing low numbers of COVID-19 cases. Perhaps in countries that have experienced greater COVID-19 cases and deaths, instrumental factors – such as sanction risk, perceiving the virus as severe or as a health threat to oneself or loved-ones – may prove more important than duty (see Brouard et al., 2020; Plohl & Musil, 2020).
Conclusion
Numerous studies have examined compliance with public health recommendations during pandemic outbreaks. Until now, however, no published studies have included a full complement of criminological and public health variables known to be associated with compliance behaviour. As such, the relative importance of demographic, instrumental and normative factors could not be determined in prior research. Our study revealed that instrumental and normative factors predicted compliance with mandatory public health restrictions. However, duty to support the authorities trumped the perceived risk of sanctions and the perceived health risks of COVID-19. To conclude, authorities and future public health studies may benefit from considering how both criminology and public health knowledge can inform our understanding of compliance during pandemic outbreaks. Doing so will better inform preparedness for future disease outbreaks.
Footnotes
Acknowledgements
We thank our anonymous reviewers for their helpful suggestions to the original version of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The first author was supported by an Australian Research Council Future Fellowship grant (Grant No. FT180100139).