
Abstract

Recently, the Diagnostic and Statistical Manual of Mental Disorders–Fifth Edition (DSM-5) introduced the mixed features specifier to describe the coterminous occurrence of manic and depressive symptoms (American Psychiatric Association [APA], 2013). Three symptoms from the opposing pole of the illness are needed to attach this specifier to an episode of hypomania, mania or depression. This means that a mixed mood state can occur in a variety of contexts with different symptom patterns defining mixed features (Malhi, 2013). However, the exclusion by DSM-5 of key symptoms as potential mixed features, on the assumption that they lack discrimination, has been challenged (Malhi et al., 2014), and an important clinical question as to which symptoms best define a mixed state remains unanswered (Reinares et al., 2015).
Clinically, mixed features are likely to be nuanced by the context within which they arise, such that mixed features occurring in depression (Mixed Depression) will likely differ from those that occur in mania/hypomania (Mixed Mania). Naturally, this presupposes that mixed mood states occur at the intersection of processes that underpin mania/hypomania and depression resulting in an admixture of symptoms from seemingly disparate poles.
To investigate this, we prospectively compared patients with mixed features occurring in the context of depression or mania. A total of 72 consecutive admissions to a specialist Mood Disorders Unit (Northside Clinic – a private adult inpatient facility in Sydney) were assessed during the first week of their inpatient stay. Patients were defined as having a major depressive or manic/hypomanic episode in accordance with DSM-5 and designated as having mixed features if they reported three or more symptoms from the opposite pole of illness – including the three excluded symptoms in DSM-5, distractibility, psychomotor agitation and irritability. Diagnosis was assigned following a comprehensive clinical assessment at the time of admission using DSM diagnostic criteria, an in-depth review by an experienced consultant and a further appraisal in an extensive multidisciplinary review involving up to 10 clinicians and three psychologists within the first week of admission.
A total of 61 patients met criteria for major depressive disorder (MDD), and of these, 10 reported experiencing symptoms of mania and met criteria for Mixed Depression (depression with mixed features). The remaining 51 patients reported only depressive symptoms. An additional 11 patients met criteria for a manic episode and also reported experiencing depressive symptoms, and were therefore designated as having Mixed Mania (mania with mixed features).
The profile of symptoms endorsed by the two mixed features groups was compared using a series of chi-square analyses. Among the symptoms of depression, only two symptoms distinguished the mixed groups (refer to Figure 1(a) and Table 1). Patients with Mixed Depression endorsed fatigue/loss of energy (80%) significantly more frequently than those with Mixed Mania (27%). Conversely, psychomotor agitation was significantly more common in those with Mixed Mania (91%) as compared to those with Mixed Depression (50%). In contrast to depressive symptoms, virtually all the symptoms of mania were endorsed significantly more frequently by those with Mixed Mania compared to those with Mixed Depression (refer to Figure 1(b) and Table 1). The most notable difference, however, occurred once again with respect to psychomotor agitation or an increase in goal-directed activity, with 100% of those with Mixed Mania endorsing these symptoms.
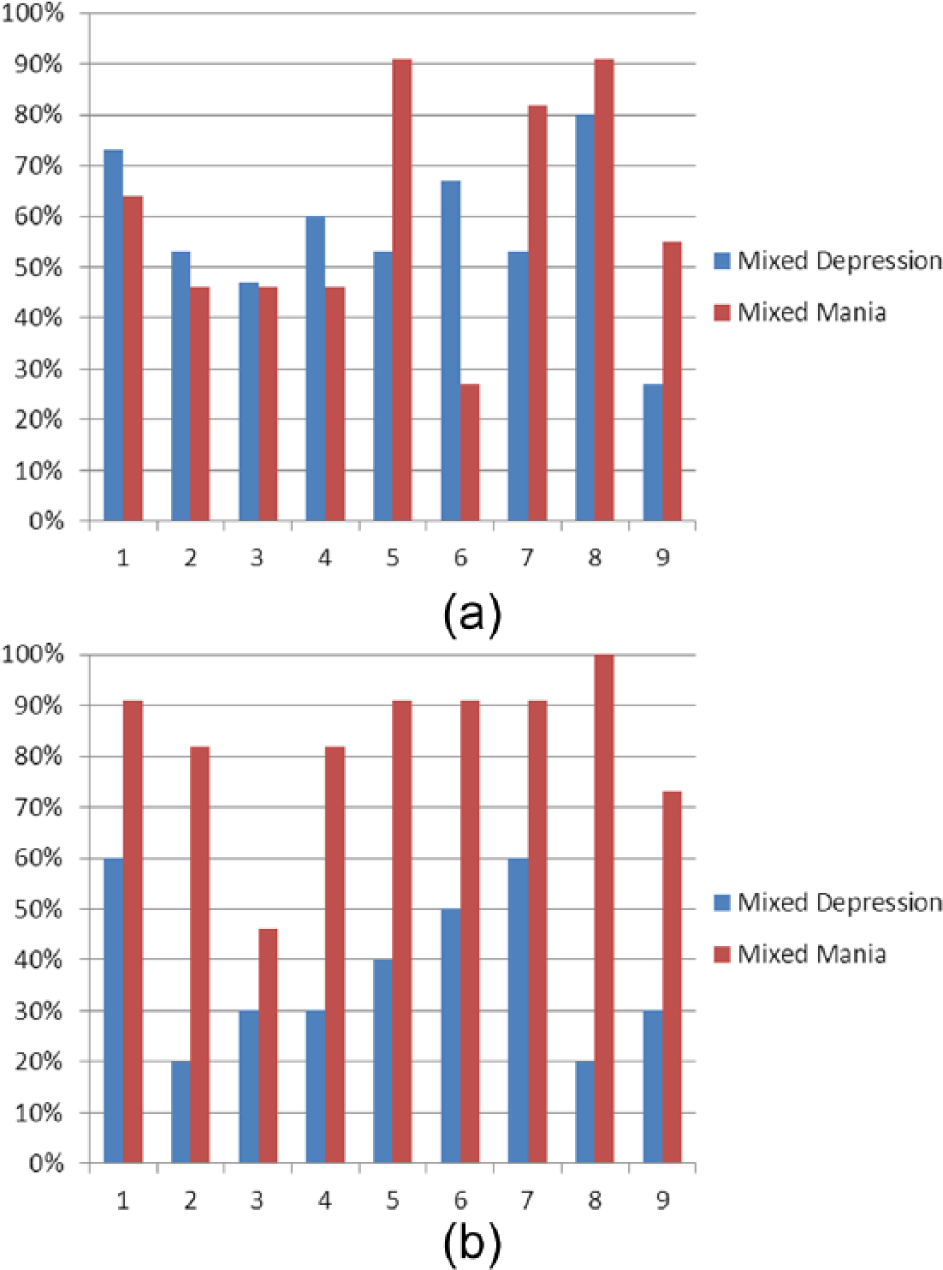
(a) Percent endorsed depressive symptoms based on group and (b) percent endorsed manic symptoms based on group. (a): 1 = depressed mood; 2 = diminished interest or pleasure in activities; 3 = weight or appetite change; 4 = insomnia or hypersomnia; 5 = psychomotor agitation or retardation; 6 = fatigue or loss of energy; 7 = feelings of worthlessness or excessive guilt; 8 = diminished ability to think or concentrate; 9 = recurrent thoughts of death or suicidal ideation or suicide attempt. (b): 1 = elevated, expansive or irritable mood; 2 = increased activity or energy; 3 = inflated self-esteem or grandiosity; 4 = decreased need for sleep; 5 = more talkative than usual or pressured speech; 6 = flight of ideas or racing thoughts; 7 = distractibility; 8 = increase in goal-directed activity or psychomotor agitation; 9 = high risk activity.
Mixed depression and mixed mania percentages and statistics for depressive and manic symptoms.

Only agitation was endorsed.
p < .05; **p < .01; ***p < .001.
This suggests that in a mixed mood state, psychomotor agitation and fatigue or a loss of energy can be useful in differentiating whether the predominant mood state and context of the mixed symptoms are that of mania or depression, respectively. It is noteworthy that among manic symptoms, increased activity or energy is a strong indicator of Mixed Mania and that just as energy ranges from diminished (fatigue) to increased, so too psychomotor activity varies from retardation to agitation; on a continuum that extends from depression and then mixed depression through mixed mania to hypomania/mania (see Figure 2).
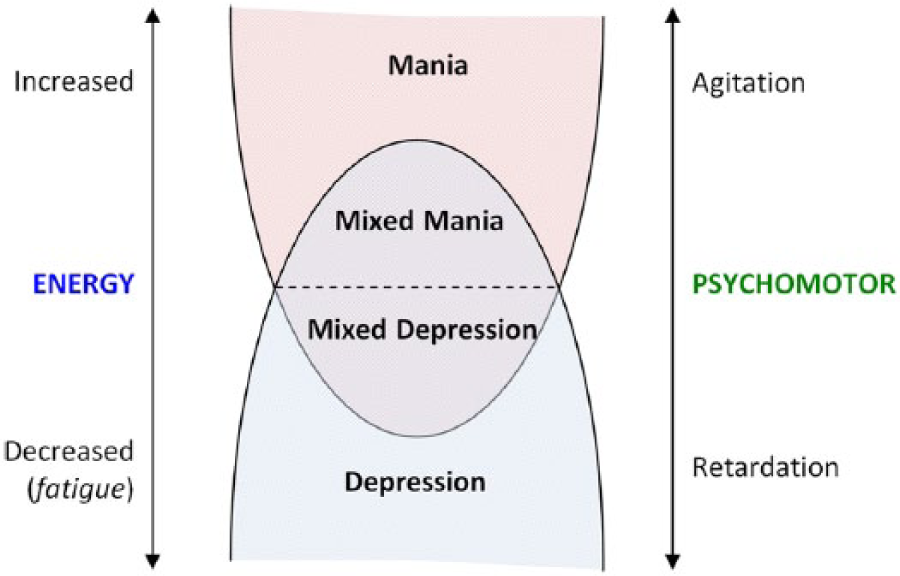
Levels of Energy and Psychomotor activity distinguish Mixed Mania and Mixed Depression.
The findings of this preliminary study, though constrained by small sample size and confounded by medication, suggest that mixed mood states can be separated clinically into Mixed Mania and Mixed Depression on the basis of psychomotor activity and energy. We suggest that consideration of these features is critical to the accurate description of mixed states and that there is a pressing need for further investigation that facilitates the development of a meaningful definition.
Footnotes
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.