
Abstract
Objective:
The objective is to investigate associations between anxiety accessing mental health services and structural stigma as self-reported by people with borderline personality disorder.
Methods:
A retrospective cohort design was used to investigate data from the 2017 National Consumer Survey undertaken in Australia between June and July 2017. Analyses were performed using multivariate binary logistic regression models.
Results:
Data comprised 423 people with borderline personality disorder aged 18 years and above, where 384 (93.7%) were females. Associations were found between anxiety and stigma in relation to mental health service access for borderline personality disorder. Strikingly, most people with borderline personality disorder reported experiencing anxiety accessing mental health services irrespective of having anxiety disorder/s, indicative of stigma leading to anxiety rather than a by-product of anxiety disorder/s. People with borderline personality disorder and anxiety disorder/s were 9.8 times more likely to feel very anxious about not being taken seriously in mental health services, than respondents with no anxiety disorder/s. Contrastingly, people with borderline personality disorder and anxiety disorder/s were 79% less likely to feel anxious about cost of services, than respondents with no anxiety disorder/s. People with borderline personality disorder previously refused public hospital admission were 8.7 times more likely to feel very anxious about cost of services and 5.3 times more likely to feel very anxious about long wait lists for services than people with borderline personality disorder not refused hospital admission.
Conclusion:
Associations were observed for people with borderline personality disorder experiencing anxiety accessing mental health services, attributed to stigma in health systems. Findings provide nuanced understanding of structural mechanisms and system-level problems affecting services and advances knowledge on the impact of borderline personality disorder–related stigma in healthcare.
Introduction
People living with borderline personality disorder (BPD) experience immense adversity in life, including challenges accessing adequate healthcare as a consequence of structural stigma in health systems (Klein et al., 2022a, 2022b; Ring and Lawn, 2019). Structural stigma in healthcare is manifested and perpetuated through organisational policies, practices and cultural norms that intentionally or unintentionally undermine resources available for people with mental illness to receive adequate provision of mental health services (MHS) (Corrigan et al., 2004; Hatzenbuehler, 2016). These structural stigma-related processes typically lead to a constellation of disadvantage and health inequities among people with BPD, shown by this psychiatric disorder being considerably underfunded and underresourced compared to other mental illnesses, such as bipolar disorder (Zimmerman, 2015).
BPD is a serious and complex mental illness constituting five or more classes of symptoms relating to chronic instability in mood, impulsivity, suicidality (i.e. deliberate self-harm, suicide ideation or suicide attempts) (American Psychiatric Association, 2013), impairment in psychosocial functioning (Ansell et al., 2007) and comorbidity (Chapman et al., 2023). The aetiology of BPD remains unclear (Kulacaoglu and Kose, 2018); however, evidence suggests that onset of BPD is linked to genetics and neurological anomalies (Bozzatello et al., 2021), and early adverse environmental (trauma-related) events (De-la-Morena-Perez et al., 2023).
The global prevalence of BPD is approximately 1–3% (Trull et al., 2010; Volkert et al., 2018) in the general population. While there is limited international data on mental health presentation rates of people with BPD in clinical settings (Broadbear et al., 2022; Smith et al., 2024), estimates suggest the prevalence of BPD extends to 12% in outpatient services, and nearly doubles (22%) for inpatient services (Ellison et al., 2018). In Australia, a recent 12-month audit of hospital data reveals people with BPD contribute to only 1.8% of outpatient services, and 21% of inpatient services (Broadbear et al., 2022). Broadbear et al.’s findings relating to outpatient service usage is substantially lower than previous estimates (Ellison et al., 2018; Widiger and Weissman, 1991), and contrary to commonly held beliefs in health systems regarding high rates of health service utilisation among the BPD patient group. The discrepancies between international and Australian health service utilisation rates for BPD may reflect omissions or inaccuracies in documenting psychiatric diagnoses in hospital records, resulting in an underestimate of BPD-related presentations to emergency departments (ED) (Broadbear et al., 2022).
People with a BPD diagnosis are also likely to represent to hospital at higher rates than people with other psychiatric disorders (Broadbear et al., 2025). For example, people with BPD were found to represent to ED at almost twice the rate of people with depression (i.e. 73% vs 42%, respectively) (Broadbear et al., 2022). Smith et al.’s (2024) study showed people diagnosed with BPD experience more frequent, short-term (e.g. < 2 days) hospital admissions; and are more likely to have an episode, relapse and represent to the hospital sooner than other diagnoses. Interestingly, males with BPD represented to the hospital following an episode sooner than females with BPD. In addition, people who self-harmed were at greater risk of representing to the hospital than people with adjustment disorder who also self-harm (Smith et al., 2024). Furthermore, people diagnosed with BPD often present to ED with higher rates of chronic suicidality (i.e. repetitive patterns of self-harm, suicide ideation and overdose) than people with other psychiatric diagnoses (Broadbear et al., 2022). Moreover, many people with BPD suffer co-occurring anxiety disorder/s, which may potentially influence the frequency of crisis presentations to ED (Broadbear et al., 2022). Co-occurring anxiety disorders are present in up to 85% of people with BPD (Pascual et al., 2023; Tedesco et al., 2023), are linked to the clinical severity of BPD (Qadeer Shah et al., 2023) and exacerbations in emotional distress and anxiety during ED presentations involving suicidal crises (Pascual et al., 2023).
When experiencing a suicidal crisis, people with BPD seeking treatment from overstretched emergency services pose challenges for health providers working within the constraints of the dominant biomedical model, typically oriented towards tertiary-level care and often not responsive to meeting the complex treatment needs of this patient group (Broadbear et al.,2022, 2025; De-la-Morena-Perez et al., 2023). This lack of capacity is evidenced by some health providers’ problematic interactions with people with BPD, including refusing hospital admission (Lawn and McMahon, 2015; Shaikh et al., 2017), despite evidence supporting the value of providing short-term hospital stays (of up to 3 days) for people with BPD at risk of suicide (National Health and Medical Research Council, 2012). The practice of refusing hospital admission to people with BPD seeking help from clinical services is concerning, given that this patient group is at high risk of dying by suicide (10%) (Paris, 2019). Broadbear et al.’s (2020) study undertook a retrospective analysis of reports on suicides from the Coroners Court of Victoria and Victorian Suicide Register between 2009 and 2013, and found that 25% of patients with a BPD diagnosis died by suicide within 6 weeks of attending an ED. This finding highlights the importance of people with BPD accessing responsive services and treatment at times of high need (Broadbear et al., 2020).
Further challenges to accessing responsive MHS for BPD are perpetuated by stigmatising narratives of service providers labelling this patient group with negative connotations, such as attention seeking and non-compliant (Proctor et al., 2021); the corollary of which is sub-optimal care of people with BPD (Klein et al.,2022a, 2022b). Unsurprisingly, people with BPD report experiencing anxiety in response to stigma and discrimination in health services, and express concerns about the quality of care provided by some health providers (Lawn and McMahon, 2015). Despite these anxiety-provoking encounters, ED continues to be the first point of contact people with BPD and carers utilise during a suicidal crisis (Acres et al., 2019). The frequency of visits to ED by this patient group reflects the limited access to long-term treatment and supports in the community to meet demand for BPD-related health services (Broadbear et al., 2022).
Historically, people living with BPD have been misunderstood and misrepresented (Gallop et al., 1989; Nehls, 1998; Nehls and Diamond, 1993). Extensive empirical research has been undertaken on the structural stigma linked to the BPD diagnosis in health systems to highlight this important public health concern and improve health service delivery (Davidson, 2008; Pigot et al., 2019). Yet, BPD-related stigma remains embedded in health systems. Further research is needed to help understand people with BPD experiences of health service access, and to determine the system-level processes and practices contributing to the pervasive stigma and discrimination in healthcare. Significant knowledge gaps continue to impede our understanding of the structural mechanisms impacting people with BPD experiences of health service access.
The aim of the present investigation was to identify associations between people with BPD experiences of MHS and structural stigma in Australian health systems. Specifically, this study examined (1) the influence of co-occurring anxiety disorder/s or having been refused public hospital admission, on anxiety (feeling anxious or very anxious) in relation to MHS access and stigma and (2) the influence of demographics including, sex, age and residential location on MHS access among respondents who identify as having co-occurring anxiety disorder diagnoses, or experienced being refused public hospital admission.
Methods
Study design
A retrospective cohort study investigated the 2017 National BPD Consumer Survey data (Lawn et al., 2017) with permission from Lived Experience Australia, formerly known as the Private Mental Health Consumer Carer Network before 2016. Research ethics approval was granted from the Social and Behavioural Research Ethics Committee, Flinders University, South Australia (no. 8608) on 4 March 2020.
Data sources and participants
Data were extracted from the 2017 National Consumer Survey (Lawn et al., 2017) spanning Australian States and Territories between June and July 2017. Globally, this survey represents some of the first data collected specific to the population of people with BPD undertaken with national coverage. Participants were recruited online using SurveyMonkey. Adult consumers self-identifying as having BPD were eligible to participate in the survey. Respondents’ informed consent to participate was obtained at the commencement of the Consumer survey. A total of 423 participants with BPD completed the survey. Comprehensive reports on the 2017 National Consumer Survey are detailed elsewhere (Lawn et al., 2017; Proctor et al., 2021). Survey questions relating to stigma and discrimination underpin the current study.
Participant data
Participant demographics comprised sex (male = 0, female = 1); age (18–24 years = 1, 25–39 years = 2, 40–49 years = 3, 50 years and above = 4); residential location (capital city = 1, regional and remote towns = 2). Clinical characteristics constituted co-occurring anxiety disorder diagnoses (No = 0; Yes = 1); time since respondents’ were diagnosed with BPD: time since diagnosis (⩽1 year = 1, 1–5 years = 2, >5 years = 3); time since respondents’ commenced treatment for BPD: time since treatment (<1 year = 1, 1–5 years = 2, >5 years = 3); and type of MHS service access (accesses public MHS = 1, accesses private MHS = 2). Hospital service characteristics included refused public hospital admission (No = 0; Yes = 1).
Stigma items taken from the Consumer survey were BPD-related discrimination; not being taken seriously; being treated badly; not being treated respectfully; unable to access services; lack of choice of services; cost of services; local services not available; and long wait list for services (Lawn et al., 2017). All stigma items were scored on the same scale (neutral/no affect = 1, anxious = 2, very anxious = 3).
Exposure and outcome measures
BPD and anxiety disorder diagnoses and refused public hospital admission
Respondents with BPD were categorised into two groups according to clinical characteristics, with the exposure comprising the presence or absence of co-occurring anxiety disorder/s (people with BPD and anxiety disorder/s or people with BPD and no anxiety disorder/s). The outcome measure was level of anxiety (neutral/no affect, anxious or very anxious) for both comparison groups. Participants with BPD were also categorised into two groups according to hospital service characteristics with the exposure being hospital admission (people with BPD and refused public hospital admission or people with BPD and not refused public hospital admission) and the outcome measure being level of anxiety (neutral/no affect, anxious or very anxious).
Statistical analysis
All statistical analyses were conducted using R version 4.3.3 (R Core Team, 2024). Participant characteristics were expressed as frequencies and percentages of the respective denominator. Pearson’s chi-square test of association with continuity correction, where appropriate, was used to explore the significant differences between people with BPD and demographics, clinical or hospital characteristics. Fisher’s exact test was also utilised when dealing with small sample sizes or when the assumptions of the chi-square test were not met. A logistic regression model was employed to investigate the outcome in relation to participant exposures. Initial analyses involved univariable models, followed by multivariable models that included participant characteristics to adjust for potential confounding. Age, sex, residential location, MHS access, time of treatment and time of BPD diagnosis were included in the multivariate models. Model fit was assessed using the Hosmer–Lemeshow goodness-of-fit, with p-values greater than 0.05 indicating adequate fit. The receiver operating characteristic curve and area under the curve (AUC) were also used to evaluate model performance, with AUC values of 0.70 or higher indicating a good fit. All analyses were two-sided, with a significance level set at α = 0.05.
Results
Participant characteristics
The 2017 Consumer survey (N = 423) largely constituted female respondents (93.7%), who were aged 25–39 years (43.3%), and who lived in capital cities (64.2%) (Table 1). Nearly two-thirds of respondents reported they had accessed public MHS. A significant interaction was found for people with BPD by sex and stigma characteristic not being taken seriously (p = 0.014), with males with BPD more commonly reporting feeling anxious (58.8%) about not being taken seriously when accessing health services, than females (anxious 26.7%). A significant interaction was also found for people with BPD by residential location for stigma characteristic local services not available, (p = 0.024), with more respondents residing in regional and remote areas reporting feeling very anxious (40.2%) about access to health services not being available locally, relative to respondents living in capital cities (very anxious, 25.6%).
Participant demographics, hospital and clinical characteristics.
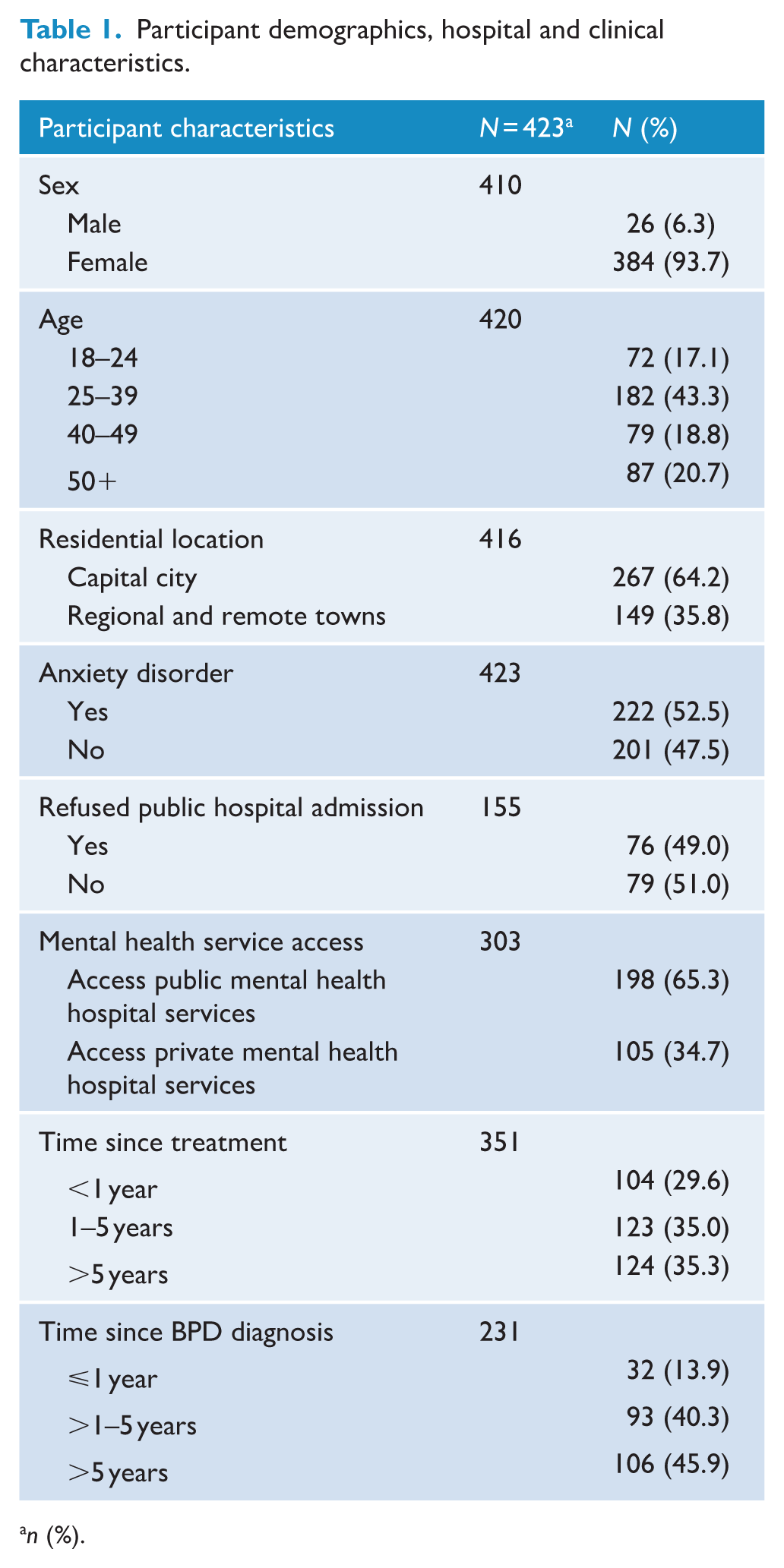
n (%).
BPD in relation to anxiety disorder diagnoses and refused public hospital admission
Slightly over half of participants with BPD self-identified as having anxiety disorder/s, compared to participants with BPD and no anxiety disorder/s (Table 1). Of these 198 respondents, 66.2% reported feeling very anxious (vs anxious 30.8%) about not being taken seriously when accessing MHS, compared to participants with BPD and no anxiety disorder/s (very anxious, 64.4%; anxious, 24.6%) (Table 2). A significant difference was found for people with BPD and anxiety disorder/s and stigma characteristic not being taken seriously (p = 0.012). Further investigations were undertaken to assess any significant interactions between BPD, anxiety disorder and sex, aside from the main effects. An absence of cells with very low counts or missing data for female and male groups suggested sufficient cases to detect the presence of sex-related differences between participant-reported anxiety in relation to MHS access and stigma.
Stigma characteristics and participants with BPD by hospital characteristics.
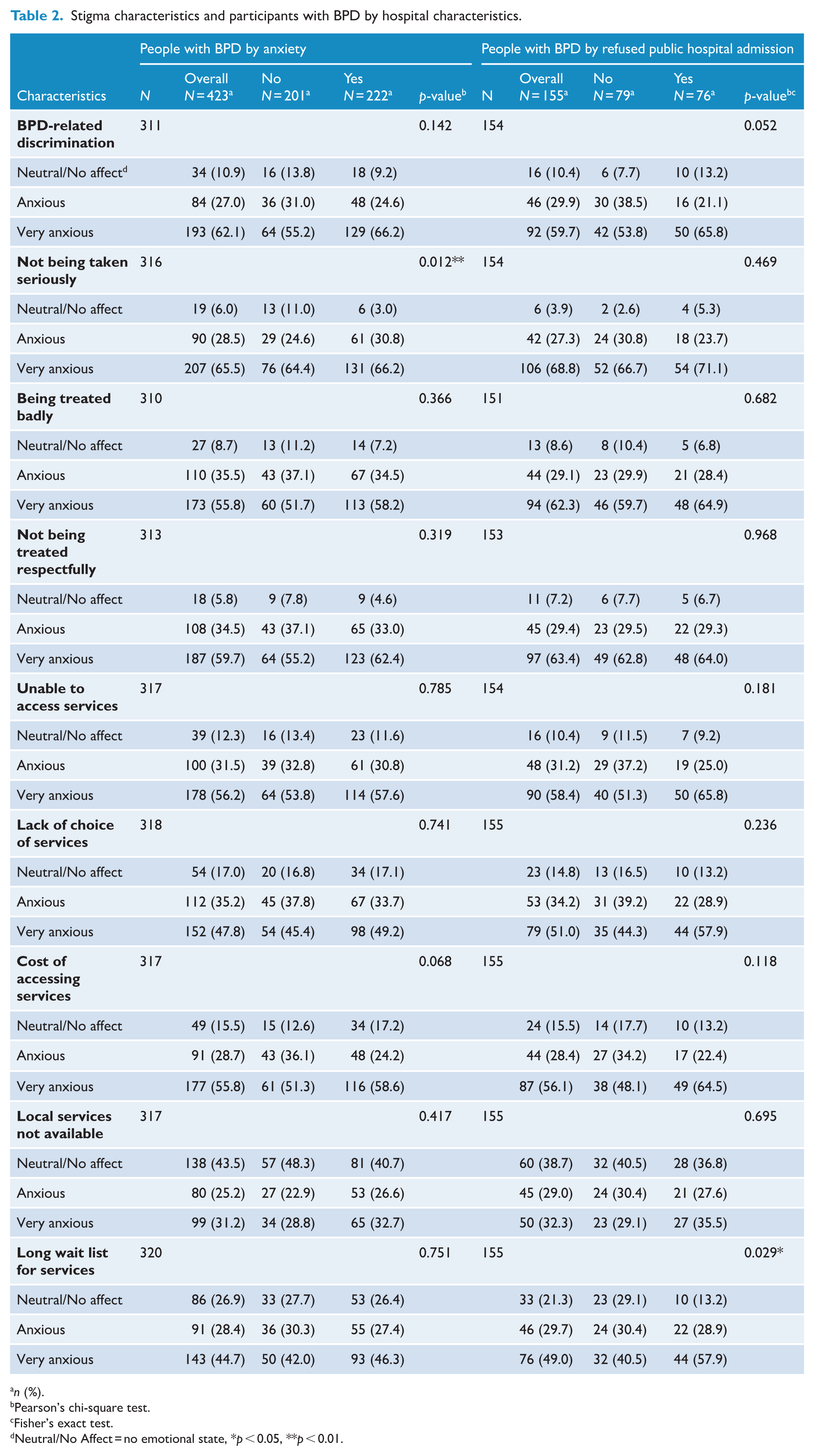
n (%).
Pearson’s chi-square test.
Fisher’s exact test.
Neutral/No Affect = no emotional state, *p < 0.05, **p < 0.01.
In relation to hospital admission, almost half of the respondents (49%) disclosed that they had been refused public hospital admission (Table 1). Of these 76 participants, 57.9% reported feeling very anxious (vs 28.9%, anxious) about long wait list for services, compared to respondents who reported not having been refused public hospital admission (very anxious, 40.5%; anxious, 30.4%) (Table 2). A significant difference was found for people with BPD by refused public hospital admission and stigma characteristic long wait list for services (p = 0.029).
Factors associated with hospital characteristics and stigma outcomes
The relationship of BPD with anxiety disorder diagnoses and stigma
The adjusted (A) models found significant associations for people with BPD and anxiety disorder/s, and not being taken seriously, very anxious (adjusted odds ratio [AOR] = 9.89, 95% confidence interval [CI]: [2.25, 55.6], p = 0.004) and anxious (AOR = 8.20, 95% CI: [1.72, 48.8], p = 0.012) (Supplementary Table 1). Furthermore, respondents with BPD significantly differed by anxiety disorder diagnoses and cost of services, anxious (AOR = 0.21, 95% CI: [0.05, 0.69], p = 0.015), compared to people with BPD and no anxiety disorder diagnoses. However, as cost of services are a protective exposure (with AORs below 1), people with BPD and anxiety disorder/s, were approximately 79% (AOR = 0.21, 95% CI: [0.05, 0.69], p = 0.015) less likely to feel anxious about the cost associated with accessing MHS, than respondents with BPD and no anxiety disorder/s. No other exposures were found to be significantly associated with anxiety disorder.
The relationship between BPD with refused public hospital admission and stigma
The adjusted models show significant associations for people with BPD who were refused public hospital admission and cost of services (AOR = 8.70, 95% CI: [1.68, 69.3], p = 0.018), with respondents being 8.7 times more likely to feel very anxious about the costs associated with MHS, relative to respondents with BPD who had not been refused public hospital admission (Supplementary Table 2). Significant associations were also evident among people with BPD who were refused public hospital admission and long wait lists for services, for very anxious (AOR = 5.39, 95% CI: [1.34, 26.1], p = 0.024), and anxious (AOR = 7.21, 95% CI: [1.55, 41.1], p = 0.017), than participants with BPD not refused public hospital admission.
Discussion
This study investigated associations between people with BPD and reported experiences of anxiety in relation to MHS access and stigma in Australian health systems. Significant associations were found for people with BPD and co-occurring anxiety disorder/s and stigma characteristics, not being taken seriously and cost of services, relative to people with BPD and no anxiety disorder/s. Strikingly, regardless of the presence or absence of co-occurring anxiety disorder diagnoses, our results show that the majority of respondents reported experiencing anxiety (n = 316; 65.5%, very anxious; 28.5%, anxious; vs 6%, neutral/no affect) about not being taken seriously in health services. This finding suggests that the anxiety endured by people with BPD relates to the stigma experienced in health services regarding not being taken seriously by health providers, rather than this fear being a product of anxiety disorder/s. The anxiety associated with MHS reflects the extent of the BPD-related stigma in health systems and alludes to the importance of de-pathologising anxiety in relation to stigma, as the anxiety experienced by people with BPD accessing MHS was present irrespective of co-occurring anxiety disorder diagnoses.
Findings from the descriptive analyses show significant differences for males with BPD and stigma characteristic, not being taken seriously; however, no other significant sex-related differences were found across all other characteristics, regardless of whether models were adjusted. Interestingly, despite the sample size of males (n = 26) in the descriptive analyses being disproportionately smaller than females (n = 384), comparisons of the rates revealed that males were more likely to feel anxious about MHS access in relation to stigma, than females. This sex-related trend was contrary to expectations, particularly given the literature on BPD being historically a highly stigmatised, female-oriented diagnosis (Bozzatello et al., 2024; Skodol and Bender, 2003). It is possible that this BPD-related sex-stereotype contributes to levels of stigma, elevating males’ anxiety and, consequently, resulting in barriers to seeking access to healthcare (Rice et al., 2021).
When confronted by stigma, it is challenging for both males and females with BPD to access adequate MHS, despite using their agency to seek help following suicidal crises (Proctor et al., 2021). This is partly due to the biomedical model’s approach to treating people with severe, complex needs being ill-equipped to deliver effective long-term therapeutic treatments, and address the social factors impacting people with BPD, such as gender bias, stigma and trauma (Sulzer et al., 2016).
In addition, an accumulative component to the anxiety expressed by people with BPD may be indicative of the continued attempts to use their agency to access support from health services, despite knowing that from past experiences the services received may re-traumatise and exacerbate chronic symptoms. This is particularly evident among people with BPD who perceive the risk of suicidality is not taken seriously or are refused public hospital admission when feeling unsafe and seeking help from health services (Lawn and McMahon, 2015; Proctor et al., 2021). Help-seeking behaviours of people with BPD provide a decisive moment where health providers can intervene with responsive treatment and care, and potentially save lives (Broadbear et al., 2020).
Analyses investigating responses to public hospital admission found significant associations between people with BPD being refused public hospital admission and being more likely to experience anxiety about the long wait list for services and cost of services, compared to people with BPD who had not been refused public hospital admission. In situations where the options for navigating public MHS including accessing in-hospital services are blocked by service providers, people with BPD are effectively hindered from obtaining affordable and appropriate treatment (National Institute for Health and Care Excellence, 2009). The cost of accessing private MHS may not be a financially viable option for some people living with BPD, while people who do preserve private health cover and pay the gap for hospital and specialist services experience further financial burden to an already stressful situation. People with BPD who are refused public hospital services in addition to struggling with the increasing cost of living, experience elevated stress levels associated with the unpredictability of receiving the appropriate treatment and care needed to support mental health recovery. In contrast, the finding that people with BPD and anxiety disorder/s were less likely to feel anxious about the cost of services, than people with no anxiety disorder/s may reflect the value that participants with co-occurring anxiety disorder/s place on accessing health services when needed (Fallon, 2003), despite the associated costs.
Respondents with BPD previously refused public hospital admission also reported feeling very anxious about the long wait lists for services, compared to people with BPD not refused public hospital admission. These findings reflect the lengthy wait lists for public and private MHS in response to the limited availability of health services for BPD in community (Broadbear et al., 2022; Lawn and McMahon, 2015). It also reflects the lack of trained and certified health providers and staff shortages in BPD-related generalist and specialist services unable to meet treatment demand (Iliakis et al., 2019). In countries like Australia with more resources available to treat people with BPD, stigma in relation to the BPD diagnosis combined with limited access to BPD-related education, training and supervision for health providers create structural barriers to the provision of quality health services (Iliakis et al., 2019; Klein et al., 2022b). Furthermore, research shows inadequate access to community-based services contributes to increases in rates of emergency service utilisation in Australian hospitals (Broadbear et al.,2022, 2025; Vecchio et al., 2018), as people with BPD and carers often perceive ED as the only immediate treatment option available when experiencing suicidal crises (Acres et al., 2019).
Overall, our findings support previous evidence on the extent of system-level problems persisting in MHS in response to the BPD diagnosis (Klein et al., 2022a), and advance our knowledge about people with BPD lived experiences of structural stigma and its impact on MHS access, and related mental health outcomes. People with BPD experiences of anxiety associated with MHS need to be considered within the broader structural processes and mechanisms that are driving BPD-related stigma in health systems to improve the quality of healthcare (Australian Commission on Safety and Quality in Health Care, 2021), rather than being dismissed as individuals’ experience of BPD and co-occurring anxiety disorder/s. Specifically, this relates to addressing the status quo that reproduces stigmatising practices and narratives in relation to the BPD diagnosis in MHS. These processes seek to distract from the structural problems that lie within the health system by shifting responsibility onto people with BPD, consequently limiting access to adequate BPD-related treatments required to meet the complex needs of this patient group and support mental health recovery. Results from this study are consistent with extensive literature on the pervasiveness of BPD-related stigma embedded in health systems (Corrigan et al., 2004; Klein et al., 2022a, 2022b; Ring and Lawn, 2019).
Policy and practice implications
Findings from this study can further drive change by informing long-term system-wide mental health reforms to develop policies and integrated health systems to improve MHS (Australian Government Department of Health, 2021), leading to better mental health outcomes for people living with BPD. This includes activities that prioritise prevention and the treatment of people with severe and complex mental illness (Australian Government Department of Health, 2022). Investing in stigma reduction approaches to shift the culture embedded in health systems (National Mental Health Commission, 2021; Stangl et al., 2019) is critical to addressing BPD-related stigma and discrimination, and normalising help-seeking behaviours when people with BPD access health services for suicidal crises (Proctor et al., 2021). Improving service delivery by making better use of current resources, such as integrated and coordinated care for mental health and suicide prevention (National Mental Health Commission, 2022), translates to relieving pressure on emergency services by linking more people to available community-based services and supports (Productivity Commission, 2019). Studies evaluating whole of service models evidenced reduced relapse and crises, ED re-presentations, shorter inpatient bed stays (Grenyer et al., 2018), and reduced hospital admissions (Graham et al., 2024); yielding direct cost savings and decreased demands on clinical services.
Limitations
While the survey used to gather data for this study was disseminated via existing local health networks and community-based organisations to consumers provides assurance on the respondents being representative of the population; these online surveys introduced some limitations. These included the short duration of the survey administration, limiting the number of respondents (N = 423) participating in the study (Lawn et al., 2017). One corollary of the small study sample size was reduced power to detect statistically significant associations; and, recognising that the nature of self-report surveys is reliant on recall of people with BPD lived experiences of MHS access and stigma. Also, there were variable response rates for each question in the survey. In addition, the results of this current study may not be generalisable across the broader BPD populations. The scope of the study is focused on people with BPD in Australian health systems; thus, findings from this study may also not be generalisable to other mental illnesses and/or countries. Moreover, the retrospective study design means causal inferences cannot be established regarding people with BPD anxiety levels in relation to MHS access and stigma-related outcomes.
Conclusion
Overall, structural stigma in healthcare has a significant impact on responsive health service delivery and care for BPD. This study provides a more nuanced understanding of the structural mechanisms and broader health system drivers and challenges affecting BPD-related services. The findings encapsulate the extent of the system-level problems embedded in MHS in relation to BPD and advance our knowledge on the impact of structural stigma and discrimination on people with BPD lived experiences of MHS access in the context of Australian health systems. Action is needed to address the dominant stigmatising discourse by improving the culture and quality of MHS for BPD.
Supplemental Material
sj-pdf-1-anp-10.1177_00048674261452046 – Supplemental material for People with borderline personality disorder experiences of mental health services in an Australian context: Associated anxiety and structural stigma
Supplemental material, sj-pdf-1-anp-10.1177_00048674261452046 for People with borderline personality disorder experiences of mental health services in an Australian context: Associated anxiety and structural stigma by Pauline Klein, Shahid Ullah, Sharon Lawn and A Kate Fairweather in Australian & New Zealand Journal of Psychiatry
Supplemental Material
sj-pdf-2-anp-10.1177_00048674261452046 – Supplemental material for People with borderline personality disorder experiences of mental health services in an Australian context: Associated anxiety and structural stigma
Supplemental material, sj-pdf-2-anp-10.1177_00048674261452046 for People with borderline personality disorder experiences of mental health services in an Australian context: Associated anxiety and structural stigma by Pauline Klein, Shahid Ullah, Sharon Lawn and A Kate Fairweather in Australian & New Zealand Journal of Psychiatry
Footnotes
Acknowledgements
The authors thank Janne McMahon, former Founder and Executive Director of Lived Experience Australia (previously known as the Private Mental Health Consumer Carer Network) for the significant contributions to the co-design and development of the 2011 and 2017 surveys, data collection, and permission to use existing data accessed from the 2017 National Consumer and Carer Survey in the current study. We would also like to thank and extend our gratitude to consumers with BPD who participated in the 2017 survey and shared their lived experience of MHS access. Thank you also to Dr Pawel Skuza, Statistical Consultant, Flinders University for their contribution to data extraction and cleaning the existing data file.
Author contributions
The research team (PK, SU, SL and AKF) contributed to the research design. PK contributed to the initial coding of the data in SPSS, under the supervision of SU. SU undertook the statistical analyses. SU, PK, AKF and SL contributed to the review of statistical analyses and interpretation of the findings. PK wrote the initial article, and PK, AKF, SL and SU edited the article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The research was supported by the Australian Government Department of Health-funded National Suicide Prevention Research Fund managed by Suicide Prevention Australia (grant number CNTR0011509).
Data availability statement
Data have not been made publicly available.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.