
Abstract
In a preliminary exploration of atheists using a concealable stigmatized identity framework, we investigated outness, identity magnitude, anticipated stigma, and psychological and physical well-being. Atheists (N = 1,024) in the United States, completed measures of outness, atheist identity magnitude, anticipated stigma, and psychological and physical well-being online. Consistent with predictions, we found small but significant associations between (a) anticipated stigma and well-being, (b) social components of atheist identity magnitude and outness as well as well-being, and (c) outness and well-being. A significant and moderate association was found between anticipated stigma and outness. There were significant, small indirect effects of ingroup ties, a social component of atheist identity magnitude, on psychological and physical well-being via outness; and of ingroup affect, another social component of magnitude, on psychological well-being via disclosure of atheist identity. Implications for research, practice, and training are offered.
Christianity is the majority, privileged religion in the United States (U.S.; Blumenfield, 2006; Schlosser, 2003), and identifying as religious in general and as Christian, specifically, is perceived as closely associated with U.S. American culture (Edgell, Hartmann, Stewart, & Gerteis, 2016; Pew Research Center, 2017). The term atheist describes an individual without belief in the existence of a god or gods (Bullivant, 2013) and, for the purposes of this study and consistent with other researchers, we defined atheists as those who “deny the existence of any sort of divine being” (Hunsberger & Altemeyer, 2006, p. 37). Researchers have found that atheists are among the least favorably viewed groups in the United States (Edgell, Gerteis, & Hartmann, 2006; Jones, 2012), often experiencing discrimination (Hammer, Cragun, Hwang, & Smith, 2012). In addition, atheists are perceived as untrustworthy (Franks & Scherr, 2014; Gervais, Shariff, & Norenzayan, 2011), immoral (Cook, Cottrell, & Webster, 2015; Wright & Nichols, 2014), and angry (Meier, Fetterman, Robinson, & Lappas, 2015). Further, atheists are generally underrepresented in the scientific literature and in psychology scholarship in particular (Brewster, Robinson, Sandil, Esposito, & Geiger, 2014).
Given their stigmatization in U.S. culture, atheists may experience adverse health consequences. Little is known about the effects of anti-atheist perceptions on atheists’ health, although experiencing anti-atheist discrimination has been associated with psychological distress (Brewster, Hammer, Sawyer, Eklund, & Palamar, 2016). Similarly, people with concealable stigmatized identities (CSIs), especially those who identify strongly with their marginalized identities (Quinn & Chaudoir, 2009), are negatively affected, mentally and physically, by discrimination (Cole, Kemeny, Taylor, & Visscher, 1996; Major & Gramzow, 1999; Schmitt, Branscombe, Postmes, & Garcia, 2014). Concealment of an identity has been associated with poor health and well-being (Meidlinger & Hope, 2014; Newheiser & Barreto, 2014). As an atheist identity is concealable and stigmatized, the well-being of atheists may be negatively associated with stigma and concealment. Thus, in this study we explored the association among atheist identity, outness, stigma, and psychological and physical well-being.
Atheism as a CSI
A CSI refers to being part of a marginalized group in which there is an opportunity to hide membership (Quinn & Earnshaw, 2011). A CSI has two major components, namely valenced content and magnitude, that influence the manner in which persons are affected by their CSI (Quinn & Earnshaw, 2011). Valenced content refers to the complex array of positive and negative emotions associated with a CSI and includes internalized stigma, experienced stigma, anticipated stigma, others’ responses to one’s disclosure, and how individuals defend themselves against stigma. Magnitude refers to the degree to which CSIs are incorporated into one’s overall sense of self, as determined by the centrality and salience of the CSI. Greater importance of the CSI to one’s overall identity and higher frequency of thoughts about the identity indicate greater magnitude of the CSI. Both valenced content and magnitude have implications for the psychological and physical distress of people with CSIs (Quinn & Earnshaw, 2011). Specifically, the various stigmas that comprise valenced content may predict greater distress and, although magnitude may protect those with conspicuous stigmatized identities from the effects of stigma on distress, greater centrality and salience of a CSI may be associated with greater distress as a result of decreased social support from similar others (Quinn & Chaudoir, 2009).
Several researchers have examined the relations among magnitude, distress, and the degree to which people anticipate being stigmatized as a result of their CSI, one component of valenced content. Among people with CSIs, including those with mental illness, a history of rape, and who identify with a minority sexual orientation, higher anticipated stigma and magnitude have been associated with higher psychological and physical distress (Chaudoir & Quinn, 2016; Quinn et al., 2014; Quinn & Chaudoir, 2009). Anticipated stigma directly affected psychological distress and worked indirectly through magnitude, particularly centrality, such that higher anticipated stigma was associated with higher magnitude, and higher magnitude was associated with more distress (Quinn & Chaudoir, 2009).
Doane and Elliott (2015) explored a similar model in a sample of atheists, although they measured psychological and physical well-being rather than distress. They found similar paths between well-being and perceived discrimination, including personal and group discrimination, directly and indirectly through magnitude. Perceived discrimination was associated with lower well-being; however, contrary to other studies of CSIs, they found a positive relationship between magnitude and well-being such that higher atheist identification was associated with higher well-being (Doane & Elliott, 2015). Therefore, for atheists, magnitude may protect against, rather than exacerbate, the negative association between stigma and well-being.
Coming Out as Atheist
Coming out refers to self-disclosure of a concealable identity to others (Chaudoir & Fisher, 2010) and is typically associated with stigmatized identities (Zimmerman, Smith, Simonson, & Myers, 2015). Outness refers to the degree to which one’s identity is known to others, and is generally defined by the number of contexts within which one is open regarding the stigmatized identity (e.g., family, work; Mohr & Fassinger, 2000). Atheists’ qualitative reports suggest they are hesitant about coming out, encounter resistance to their atheist identity from religious communities, and do not always describe their initial coming out experiences as affirming (Brewster, 2014). However, ultimately, many atheists connect with similar others (Brewster, 2014) and consider coming out as a positive experience, if only in retrospect (Christina, 2014; Smith, 2011). Coming out as an atheist to one’s family, for example, appears to be positive when accompanied by healthy communication, family cohesion, adaptability, and the ability to remain close despite differences (Zimmerman et al., 2015).
To our knowledge, only one study has explored the relationship between outness and stigma in an atheist population. The researchers found that atheists reporting more outness also reported more experiences of discrimination (Hammer et al., 2012). Similarly, Quinn et al. (2014) found a significant, positive association between outness and anticipated stigma among people with other CSIs. Conversely, Newheiser and Barreto (2014) found that people with CSIs who perceived more bias toward their identity were more likely to conceal that identity than those who perceived lower levels of bias. Although outness may facilitate increased opportunities to experience discrimination, explaining the positive relationship found between outness and stigma in previous studies, the anticipation of stigma may deter atheists from being out, given the strength of anti-atheist bias in the United States (Edgell et al., 2016).
Likewise, atheist identity magnitude may be associated with outness among atheists. In a qualitative exploration of atheist identity formation, the development of an atheist identity including rejecting faith and reinterpreting worldview, preceded the final stage of atheist identity development—coming out. As participants’ atheist identity became more central and salient and they saw themselves as part of an atheist community, they felt a stronger desire to claim their identity via disclosure (Smith, 2011). By contrast, in a study of CSIs that did not include atheists, no significant associations were found between centrality or salience of identity and outness (Quinn et al., 2014). Strongly identifying as atheist may make outness more likely as compared to other CSIs, given that public disaffiliation from religion may serve as a political or symbolic statement (Hout & Fischer, 2002).
Extant literature on outness in marginalized groups other than atheists generally suggests outness is beneficial to well-being (Chaudoir & Quinn, 2010; Corrigan, Kosyluk, & Rusch, 2013; Morris, Waldo, & Rothblum, 2001), although significantly greater benefits are demonstrated when coming out takes place in a supportive environment (Legate, Ryan, & Weinstein, 2012). Low outness and concealment of an identity may compromise psychological well-being (Major & Gramzow, 1999; Meidlinger & Hope, 2014), increase physical health risks (Cole et al., 1996), and reduce sense of belonging and authenticity (Newheiser & Barreto, 2014). Risks of outness include social isolation, harassment, and psychological stress (Ragins, 2008) and are reflected in the concerns atheists express about disclosure of their identity (Brewster, 2014; Hammer et al., 2012).
CSI theory posits that distress resulting from identification with a CSI may be a function of low social support (Quinn & Chaudoir, 2009). As outness may facilitate contact with other group members, there may be an indirect path between atheist identity magnitude, particularly social aspects of group identification, and well-being, through outness of atheist identity. In a CSI study that included outness in addition to stigma, magnitude, and psychological distress, higher magnitude, specifically salience, as well as anticipated stigma, independently predicted more distress whereas outness appeared to serve as a protective factor, predicting less distress. However, contrary to prediction, outness did not moderate the relationship between anticipated stigma and distress (Quinn et al., 2014). In another study of CSIs, increases in anticipated stigma worsened depressive symptoms over time; however, openness about CSI, or outness, did not appear to be significantly associated with depressive symptoms (Chaudoir & Quinn, 2016). Therefore, despite studies suggesting that outness is beneficial to well-being, CSI studies have not replicated those findings. Of note, studies of CSIs exploring relationships between outness and other CSI variables have, to date, primarily included participants with mental illness, history of abuse and/or trauma, substance abuse, or appearance concerns, and have excluded atheists.
The Present Study
Considering prior CSI research and limited existing literature studying atheists, we hypothesized that among atheists higher anticipated stigma would be associated with less disclosure and more concealment and, conversely, higher atheist identity magnitude would be associated with more disclosure and less concealment. We also expected that higher anticipated stigma would be associated with lower psychological and physical well-being, higher atheist identity magnitude would be associated with higher psychological and physical well-being, and more disclosure and less concealment would be associated with higher psychological and physical well-being. Our additional hypotheses tested patterns of mediation. Building upon previous research, we also expected that outness would mediate the relationship between magnitude and psychological and physical well-being such that greater magnitude would be associated with more disclosure and less concealment and, in turn, higher psychological and physical well-being.
Method
Participants
Participants were recruited electronically through listservs and social media associated with atheist organizations, and via snowball sampling. A total of 1,362 people began the study, but 71 were agnostic and 7 were theists and were, therefore, ineligible for participation. An additional 222 discontinued the survey after completing none or some of the demographic questionnaire, or completed fewer than 80% of the measures; these participants were excluded from the analyses as well. Finally, as we were particularly interested in the experiences of U.S. atheists, and because the experience of atheists can vary considerably transnationally, non-U.S. participants (n = 38) were excluded, resulting in a final sample of 1,024.
Participants ranged in age from 18 to 92 years (Mage = 54.38, SD = 16.99) and identified as men (62%), women (38%), and intersex (<1%). Most (92%) were White/European American with the remaining consisting of Latino (3%), other (2%), bi-multiracial (2%), Asian/Asian American/Pacific Islander (1%), Black/African/African American (<1%), and Native American (<1%) participants. Most participants resided in the Western (35%) or Southern (32%) United States, 21% were from the Midwest, and 12% from the Northeast. Most (87%) participants identified as heterosexual, 6% as bisexual, 6% as gay or lesbian, and 2% as other, the most common of which was pansexual. Most participants were financially independent (96%) and earned at least $33,000 annually (84%). Years of formal education ranged from less than a high school degree to 30 years; 74% reported having earned a bachelor’s degree or more education. Although some participants were raised without a focus on religion (atheism, agnosticism, or no religion; 12%), most (73%) were raised in Christian families. The number of years that participants had identified as an atheist ranged from 1 to 80 (M = 29.17, SD = 20.05, Mdn = 25.00).
Procedure
Data were collected via PsychData, an online survey platform. Participants answered one criterion question adapted from Hunsberger and Altemeyer (2006) to confirm atheist identity. Following the definition of a traditional god(s), participants chose one of the following statements: “I am an agnostic. I do not believe in the existence of this ‘traditional’ god, nor do I disbelieve in it,” “I am a theist. I believe in the existence of this traditional god,” or “I am an atheist. I do not believe in the existence of this ‘traditional’ god. I believe it does not exist.” Those who chose the final statement were invited to continue in the study. Participants completed five scales in the order in which they are presented in the next section.
Measures
Outness
Because no measures of atheist outness exist, we adapted a measure designed for use with LGB populations with permission from the authors. The Nebraska Outness Scale (NOS; Meidlinger & Hope, 2014) is a 10-item measure consisting of two subscales measuring concealment (NOS-C) and disclosure (NOS-D). The scale was adapted for an atheist population by replacing “sexual orientation” with “atheist identity.” Participants indicate the percentage of people aware of their identity and the frequency with which they avoid talking about their identity within various contexts such as “Members of your immediate family” and “People you socialize with.” Items are scored on an 11-point Likert-type scale; higher scores indicate more outness and more disclosure. The NOS has been correlated positively with other measures of outness, suggesting strong evidence of convergent validity. In initial testing, the NOS-C and NOS-D demonstrated Cronbach’s alphas of .80 and .82, respectively. In the current study, the NOS-C and NOS-D demonstrated Cronbach’s alphas of .82 and .75, respectively.
Atheist identity magnitude
Atheist identity magnitude was measured via the 12-item Three-Dimensional Strength of Group Identification Scale (SGIS; Cameron, 2004). The SGIS includes items capturing the two constructs of magnitude, centrality and salience, such as “being an (ingroup member) is an important part of my self-image,” and “I often think about being an (ingroup member).” The SGIS also includes items related to emotions associated with group membership (ingroup affect) and the degree to which individuals consider themselves a part of a group (ingroup ties). Items are scored on a 7-point Likert-type scale; higher scores indicate greater agreement with the statement (Cameron, 2004). Researchers have found positive correlations between the SGIS subscales and other social identity measures, as well as with measures of related constructs such as collective self-esteem, suggesting good construct and convergent evidence of validity (Obst & White, 2005, 2007). In initial testing across five studies, the subscales demonstrated the following Cronbach’s alphas: .67 to .78 (centrality), .77 to .82 (ingroup affect), and .76 to .84 (ingroup ties). The current study demonstrated Cronbach’s alphas of .72 for the centrality subscale, .76 for the ingroup affect subscale, and .82 for the ingroup ties subscale.
Anticipated stigma
Quinn and Chaudoir (2009) adapted the day-to-day discrimination scale from Kessler, Michelson, and Williams (1999) to measure anticipated stigma in a study of the psychological and physical health of individuals with CSIs. Participants were asked how likely various forms of discrimination were to occur if others were made aware of their CSI. Items include, “People act as if they are afraid of you” and “Treated with less respect than others.” The adapted measure demonstrated strong internal consistency (α = .95; Quinn & Chaudoir, 2009). We slightly modified Quinn and Chaudoir’s (2009)’s scale by eliminating four of the six items because they were specific to a college population and irrelevant to atheists. We then added an item to reflect the social devaluation atheists anticipate based on the literature, which suggests atheists are perceived as immoral (Gervais, 2014; Wright & Nichols, 2014). The resulting measure was comprised of 12 items scored on a 7-point Likert-type scale with higher scores indicating greater anticipated stigma. Internal reliability was excellent; α = .95. A parallel analysis-guided promax, principal axis factoring exploratory factor analysis revealed a one-factor solution accounting for approximately 62% of variance; therefore, a total score was calculated.
Psychological well-being
Psychological well-being was measured using Ryff’s (1989) Psychological Well-Being Scale (PWBS). The PWBS measures psychological well-being through various dimensions including self-acceptance, purpose in life, environmental mastery, positive relationships, personal growth, and autonomy. Using a 6-point Likert-type scale, participants indicate their level of agreement with 18 statements, including “The demands of everyday life often get me down” and “Some people wander aimlessly through life, but I am not one of them.” Higher scores reflect greater psychological well-being (Ryff, 1989; Ryff & Keyes, 1995; Springer, Hauser, & Freese, 2006). Among prior studies of conspicuous (e.g., racial and/or ethnic minorities) and concealable (sexual minorities) stigmatized identities, the PWBS has demonstrated good reliability (Brewster, Velez, Foster, Esposito, & Robinson, 2016; Frost & Meyer, 2012). In the current study, α = .83.
Physical well-being
Physical well-being was measured using the Pennebaker Inventory of Limbic Languidness (The PILL; Pennebaker, 1982). The PILL measures the frequency of 54 common physical symptoms and sensations associated with illness including “choking sensations” and “stiff or sore muscles.” Participants indicate how often they experience each symptom on a 5-point Likert-type scale, with high scores indicating more frequent symptoms. The PILL is a valid measure, evidenced by positive correlations between reports of symptoms and physician visits as well as health problems. Scores are moderately correlated with those of other symptom inventories. Initial testing demonstrated Cronbach’s alphas ranging from .88 to .91 in a sample of college students (Pennebaker, 1982). In the current study, α = .92.
Results
Descriptive statistics were calculated for all demographic variables. Distributions of all measures met the assumption of normality, with the exception of ingroup affect with skewness of -3.53 (SE = .08) and kurtosis of 17.71 (SE = .15), as many participants reported very strong positive feelings about their atheist identity. Generally, participants reported moderately strong to strong atheist identity magnitude, physical well-being, and psychological well-being; anticipated stigma, disclosure, and concealment were midrange (see Table 1). Missing data ranged from 0% for the NOS to 3% for the PILL. Little’s MCAR, χ2 = 743.42, df = 645, p = .004, suggested data were not missing at random, possibly due to ordering effects, as the PILL was administered last. Therefore, multiple imputation was used to estimate missing data for those who did not complete all surveys. As missing data were well below 30% for all variables, we performed five imputations (Schafer & Graham, 2002). Descriptive analyses suggested the distributions of the imputed datasets did not significantly differ from the original dataset. Analyses were run on the original dataset as well as all imputed datasets. As results were consistent across datasets, the results of the original data are presented. Mediation analyses were conducted using the PROCESS macros for SPSS developed by Hayes (2013).
Correlations

p < .05. **p < .01.
Correlations
Correlational analyses were conducted to test Hypotheses 1 through 5 (see Table 1). Hypothesis 1 predicted that higher anticipated stigma would be associated with less disclosure and more concealment of atheist identity. Hypothesis 1 was supported as significant, moderate associations were found between anticipated stigma and disclosure, and between anticipated stigma and concealment. We predicted higher magnitude would be associated with more disclosure and less concealment of atheist identity in Hypothesis 2. Hypothesis 2 was partially supported as ingroup ties and ingroup affect, two of the three subscales measuring magnitude, had small but significant associations with disclosure and concealment of atheist identity. Higher ingroup ties and ingroup affect were related to more disclosure and less concealment. The centrality subscale was not significantly associated with disclosure or concealment.
Hypothesis 3 was supported as there were significant, small to moderate associations between anticipated stigma and psychological well-being and anticipated stigma and physical well-being. Thus, higher anticipated stigma was related to lower psychological well-being and higher reporting of physical illness symptoms. We also predicted that higher magnitude would be associated with higher psychological and physical well-being. Hypothesis 4 was partially supported as, like Hypothesis 2, small, significant associations were only found between ingroup ties and well-being, and ingroup affect and well-being. Specifically, higher ingroup ties and ingroup affect were associated with higher psychological well-being and fewer reported physical illness symptoms. Centrality was not significantly associated with psychological or physical well-being. Finally, Hypothesis 5 predicted that more outness would be related to higher well-being. Hypothesis 5 was supported as small, significant relationships were found between both disclosure and concealment of atheist identity and well-being. Higher rates of disclosure were related to higher psychological well-being and fewer reported physical illness symptoms and, conversely, higher concealment was associated with lower psychological well-being and a higher number of physical illness symptoms.
Mediation Analyses
To explore Hypothesis 6, we conducted simple mediation analyses (Model 4; Hayes, 2013) to test for the indirect effects of atheist identity magnitude (ingroup ties, ingroup affect, and centrality) on psychological and physical well-being via atheist identity disclosure and concealment (bootstrap resamples = 10,000). Two models were explored. Both models’ consisted of three predictors—ingroup ties, ingroup affect, and centrality (atheist identity magnitude)—and two mediators—disclosure and concealment of atheist identity (outness). The first model’s outcome variable was psychological well-being, and the second model’s outcome variable was physical well-being. Mediation analyses were conducted for each possible combination of predictor, mediator, and outcome variables. Hayes’ PROCESS macros removes cases without complete data for the variables included in the analysis, resulting in a sample of 969 for the mediation analyses involving psychological well-being and 952 for analyses involving physical well-being.
Results for the tests of the indirect effect of ingroup ties on psychological well-being via disclosure and concealment, respectively, are presented in Table 2. Small, significant indirect effects of ingroup ties on psychological well-being through disclosure and concealment, independently, were found (see Figure 1). Ingroup ties was associated with .007 higher psychological well-being scores as mediated by disclosure and .007 higher psychological well-being scores as mediated by concealment.
Testing Mediation Model for Indirect Effects of Ingroup Ties on Psychological Well-Being via Disclosure and Concealment

Note. β = standardized beta coefficients; CI = confidence interval.
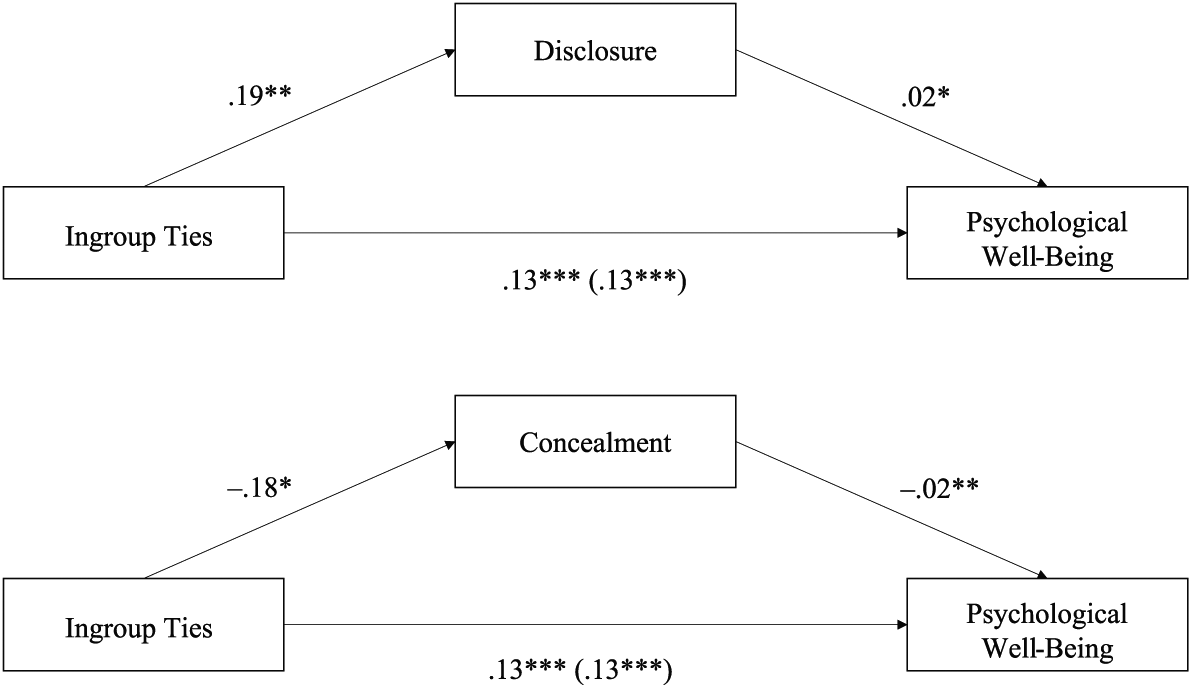
Standardized regression coefficients for the relationships between ingroup ties and psychological well-being as mediated by disclosure and concealment, respectively. The standardized regression coefficients between ingroup ties and psychological well-being, controlling for disclosure and concealment, are in parentheses.
Results for the tests of the indirect effect of ingroup ties on physical well-being via disclosure and concealment are presented in Table 3. Similar to findings for psychological well-being, small, significant indirect effects of ingroup ties on physical well-being through disclosure and concealment, independently, were found (see Figure 2). Ingroup ties was associated with .007 lower reported physical symptoms as mediated by disclosure, and .006 lower reported physical symptoms as mediated by concealment.
Testing Mediation Model for Indirect Effects of Ingroup Ties on Physical Well-Being via Disclosure and Concealment
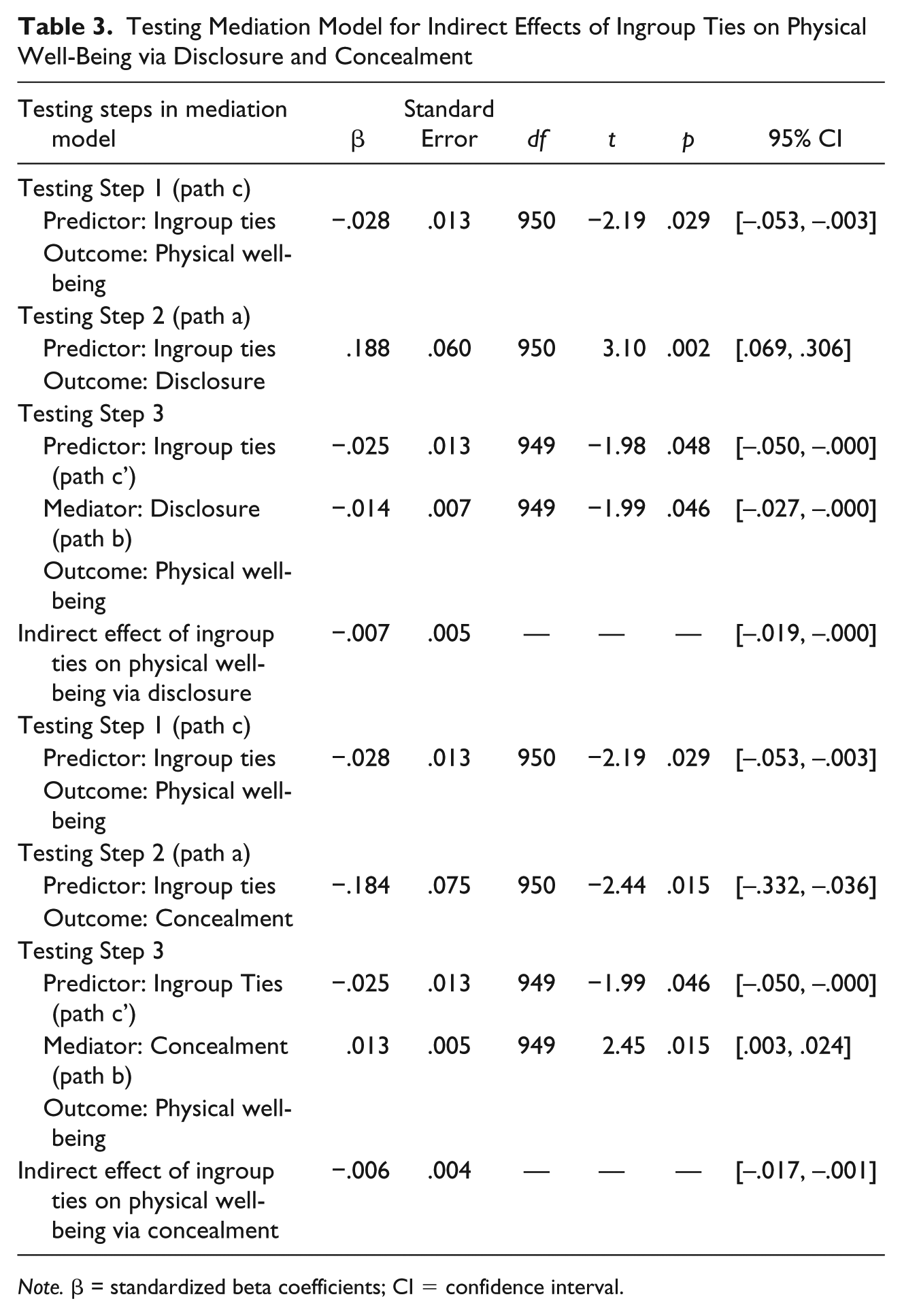
Note. β = standardized beta coefficients; CI = confidence interval.
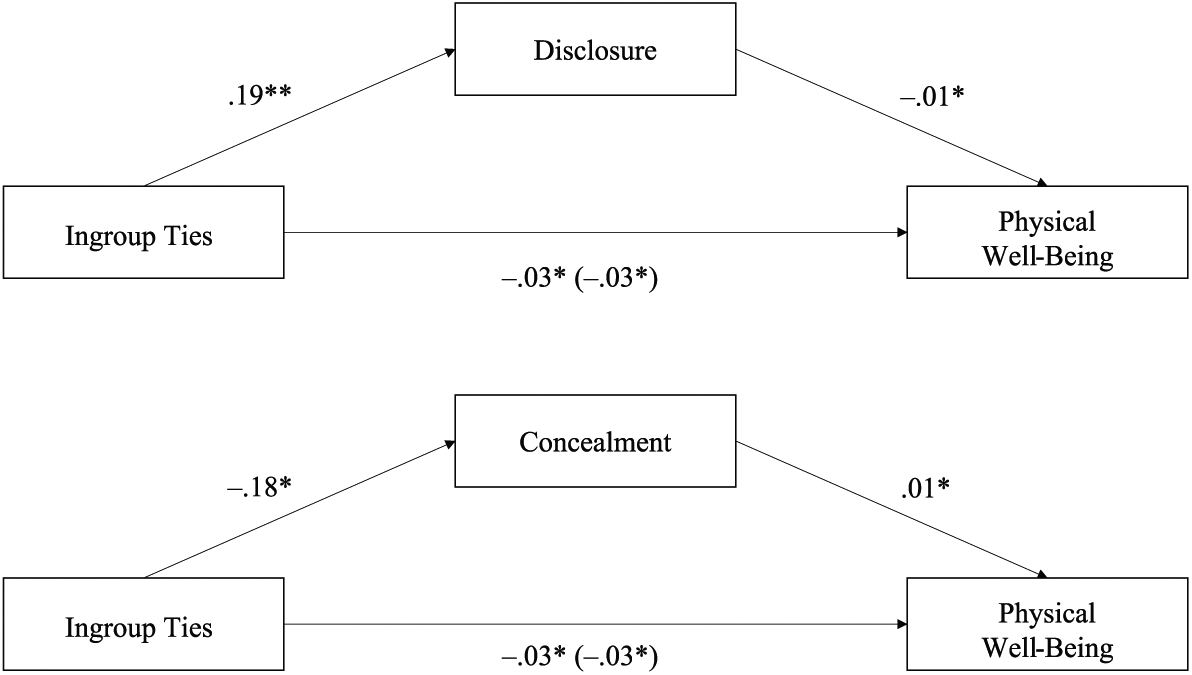
Standardized regression coefficients for the relationships between ingroup ties and physical well-being as mediated by disclosure and concealment, respectively. The standardized regression coefficients between ingroup ties and physical well-being, controlling for disclosure and concealment, are in parentheses.
In a similar exploration of the indirect effect of ingroup affect on psychological and physical well-being through disclosure and concealment, the mediation hypothesis was only supported for the role of disclosure as a mediator of the relationship between ingroup affect and psychological well-being. The indirect effect of ingroup affect on psychological well-being via disclosure, β = .01, SE = .01, CI included 0, 95% CI [.001, .019], was significant. Ingroup affect was associated with .007 higher psychological well-being scores as mediated by disclosure. No significant indirect effects of centrality on well-being via disclosure or concealment were found.
Therefore, both disclosure and concealment mediated the relationship between ingroup ties and psychological well-being. Specifically, a stronger sense of connection with other atheists was associated with more disclosure and less concealment of atheist identity which, in turn, were associated with a small increase in psychological well-being as compared to the direct effect of ingroup ties on psychological well-being alone. Likewise, higher disclosure and lower concealment associated with higher ingroup ties were, in turn, associated with lower physical illness symptom reporting as compared to the direct effect of ingroup ties on physical well-being alone. Finally, more positive emotions related to one’s atheist identity was associated with greater disclosure of atheist identity and, in turn, higher psychological well-being.
Discussion
Our study adds to the growing literature on atheists, as we investigated previously unexplored questions about the relationships among anticipated stigma, outness, atheist identity magnitude, and physical and psychological well-being. The results provide preliminary data regarding how atheism fits within a CSI framework. Results were in some ways consistent with, but in other ways diverged from, studies of other CSIs. Higher levels of anticipated stigma were associated with less disclosure of atheist identity, more concealment of atheist identity, and lower psychological and physical well-being. Two components of atheist identity magnitude, as measured in our study, were associated with outness and well-being. Specifically, higher ingroup ties, or a sense of connectedness with other atheists, and higher ingroup affect, or positive emotions associated with one’s atheist identity, were related to more disclosure, less concealment, and higher psychological and physical well-being. Likewise, more disclosure and less concealment of atheist identity were associated with higher psychological and physical well-being. Additionally, indirect effects were found from ingroup ties to psychological and physical well-being through disclosure and concealment, such that higher ingroup ties was associated with more disclosure and less concealment of atheist identity and, in turn, higher psychological and physical well-being. A similar indirect path was found from ingroup affect to psychological well-being through disclosure such that higher ingroup affect was associated with more disclosure and, in turn, higher psychological well-being.
Integration with Previous Research
CSI
Consistent with previous studies of CSIs (Brewster et al., 2016; Doane & Elliott, 2015; Hatzenbuehler, Phelan, & Link, 2013; Meyer, 2003; Quinn & Chaudoir, 2009; Schmitt et al., 2014), atheists’ physical and psychological well-being were negatively influenced by discrimination, particularly by the anticipation of stigmatization. Previous studies of CSIs have commonly investigated the influence of discrimination on psychological distress (Hatzenbuehler et al., 2013; Meyer, 1995; Quinn & Chaudoir, 2009) rather than on psychological well-being. Our study is among the first to explore how stigma influences psychological well-being. Therefore, although effect sizes were small, our findings begin to provide support for the relationship between anticipated stigma and well-being among those with CSIs.
We used a measure of magnitude to assess group identification that included centrality and salience as well as ingroup ties and ingroup affect. Interestingly, in our study, centrality and salience were not associated with well-being or outness, as predicted, although higher centrality was associated with higher anticipated stigma. However, consistent with the theory that finding similar others promotes well-being among those with CSIs (Quinn & Earnshaw, 2013), we found that higher ingroup ties and ingroup affect, social components of group identification, were significantly associated with higher psychological and physical well-being. Additionally, identity magnitude’s association with less distress among atheists in the present study is consistent with Doane and Elliott’s (2015) findings in which atheist identity and atheist well-being were significantly associated. In their study, however, they measured atheist identification via centrality, importance, and commitment.
Outness
The strongest association found in the present study was between anticipated stigma and outness, such that higher anticipation of stigmatization was related to less disclosure and more concealment of atheist identity. This finding is consistent with those of previous studies, suggesting that people with CSIs are more out in environments in which there is lower risk of discrimination (Legate et al., 2012; Moradi et al., 2010). Atheists, too, may assess risk of stigmatization in determining whether to disclose or conceal their atheist identity. Also consistent with other studies and theories of CSIs (Legate et al., 2012; Meidlinger & Hope, 2014), disclosure was positively associated, and concealment was negatively associated, with physical and psychological well-being. Although there are risks associated with outness, and some atheists experience challenging disclosure experiences (Brewster, 2014), outness may be beneficial. In particular, outness may facilitate social connection, as evidenced by the significant association between ingroup ties and outness, resulting in benefits to well-being. However, effect sizes were small; it is possible that outness plays a less vital role in the health of atheists than is true for individuals with other CSIs.
Implications for Training and Practice
Brewster et al. (2014) noted that atheism should be integrated into training so students can explore their biases and learn to work responsibly and ethically with atheist clients. Similarly, Sahker (2016) recently noted the importance of developing clinical and ethical guidelines for psychologists working with nonreligious clients. The current study provides preliminary data to guide the development of such guidelines and to determine which aspects of an atheist identity may be relevant to psychological treatment. Specifically, our findings support Sahker’s (2016) suggestion that psychologists incorporate clients’ potential fear of discrimination in case conceptualization, particularly among atheist clients. Atheist clients may also benefit from exploring disclosure and concealment of their atheist identity and identifying environments in which they are able to be out in the interest of improved well-being.
Implications for Research
Participants in the present study, consistent with past research, were privileged regarding ethnicity, gender, sexual orientation, and class. Individuals from marginalized groups including people of color and sexual minorities were underrepresented despite our attempts to recruit a more diverse sample. Future researchers should intentionally draw from more diverse samples including participants with intersecting marginalized identities, particularly those who are non-White, queer, and of less privileged social classes. In addition, exploring the differences between atheists raised with and without faith could be a valuable area of study. Researchers may also choose to replicate previous studies of CSIs and minority stress by using measures of psychological distress, including anxiety and depression scales, to assess well-being. In addition to exploring anticipated, experienced, and internalized discrimination, exploring the consequences of microaggressions on the physical and mental health of atheists (Pagano et al., 2013; Sue et al., 2007) would be useful. Regarding outness, the mechanisms by which outness may facilitate health were not assessed in our study; however, greater outness may allow for social support which, in turn, would influence health positively (Weisz, Quinn, & Williams, 2016). Thus, in future studies, researchers could assess the degree of support of atheists’ environments to explore this possibility.
Limitations
Although significant relationships were found, the effect sizes in the present study were generally small; therefore, other variables such as internalized stigma and personal discrimination experiences may more strongly influence atheist well-being than the variables we explored. Additionally, the homogeneity of our sample limits generalizability. Although the demographic characteristics of our sample are generally consistent with national estimates (Pew Research Center, 2015), marginalized groups—including atheists of color, gender and sexual minorities, and working class atheists—are underrepresented. Because cultural factors may exacerbate or attenuate the impact of anticipated stigma on psychological distress (Ikizer, Ramírez-Esparza, & Quinn, 2018), effect sizes may be larger among a more diverse group with greater marginalized intersecting identities. Additionally, the cross-sectional nature of the data is a limitation, and future longitudinal studies are necessary to support the directionality of the associations reported.
Also, even though the demographics of our study mirror those in other recent studies of atheists (Doane & Elliott, 2015; Hammer et al., 2012), Gervais and Najle’s (2018) finding that there may be far more atheists than previously thought suggests we may know very little about atheists who are not out or members of atheist organizations. Considering that participants in our study self-identified as atheists and were primarily recruited from atheist and secular organizations, the findings may not generalize to other atheists. Further, definitions of atheism vary, and atheists without a belief in god(s) who do not actively deny the existence of god(s) may have chosen not to continue.
As few measures developed specifically for atheists exist, the scales chosen for the present study were normed on individuals whose identities were similar to atheists in their stigmatized and concealable nature. Because the Measure of Atheist Discrimination Experiences (MADE; Brewster et al., 2016) and the Scale of Atheist Microaggressions (SAM; Pagano et al., 2013), are in early development, they were not used in the present study. Additionally, measures were not counterbalanced to control for order effects, and analyses were correlational; therefore, causation cannot be inferred.
Conclusion
Atheists are a highly stigmatized population in the United States. Anticipating stigma is associated with higher outness and higher psychological and physical well-being. Magnitude, particularly higher connectedness to other atheists and positive emotions about atheist group identification, is associated with higher outness and, in turn, higher psychological and physical well-being. The current investigation is among the first to assess outness by applying CSI theory to a sample of atheists and, in particular, to the relationship between outness and psychological and physical well-being. Additional research is necessary to extend the present study’s findings; explore additional contextual factors that contribute to atheists’ outness, magnitude, and overall well-being; and broaden our general understanding of the experience of living as an atheist in the United States.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.