
Abstract
Indigenous adolescents are overrepresented at multiple stages of the justice system, but we know very little about the role that mental health, particularly substance use disorder, plays in Indigenous pathways to arrest. This study examined the association between substance use disorder, its comorbidity with other disorders, and arrest using a longitudinal sample of Indigenous youth from the Northern Midwest and Canada. Of the 16% of youth who reported at least one arrest at Wave 5, half met criteria for substance abuse/dependence and slightly more for conduct disorder. Substance abuse/dependence and conduct disorder were each associated with an increased risk of arrest, although co-occurring disorders were not. The reciprocal effects of arrest and mental disorder are discussed.
Keywords
On any given day, 1 in 25 American Indians/Alaska Natives (AIAN) aged 18 years or older is under the jurisdiction of the criminal justice system. AIAN youths represent about 1% of the U.S. population, yet make up 2% to 3% of those arrested for offenses such as theft and alcohol violations, and when arrested, they are 18 times more likely to be committed to adult prisons than are European adolescents. Of all youths who are prosecuted in federal courts, 32% are placed in a secure facility; of these 74% are AIAN (Perry, 2004). Although Indigenous people make up less than 1% of the population in Minnesota, they are disproportionally stopped, arrested, and incarcerated. Indigenous young people accounted for 15.7% of juveniles in the Minnesota Red Wing Correctional Facility (American Indian Policy Center, 2005). Nationally, the average rate of new commitments of Indigenous youth to adult state prisons is almost twice that (1.84 times) of European American youth. These are enormous ethnic disparities, yet we know very little about AIAN young people in the juvenile justice system and their pathways to arrest and incarceration (Cross, 2008).
Linkages between alcohol abuse, arrests, and incarceration of AIAN people have been around for decades (e.g., Levy, Kunitz, & Everett, 1969; O. Stewart, 1964), and although the mechanisms at work have been refined, the associations largely still hold (Feldstein, Venner, & May, 2006). In a recent Bureau of Indian Affairs study of alcohol-related crime in five Western states and Alaska, alcohol use was involved in 60% of homicides, 58.6% of child abuse, 52.4% of sexual assaults, and 50% of assaults (Leonardson, 2006). Grobsmith (1989) reported that 100% of the American Indian (AI) inmates in a Great Plains prison told her they had a drug or alcohol dependency problem. Substance abuse disorders were the most common psychiatric disorders among AI adolescents in Northern Plains detention centers (Duclos et al., 1998). Although they do not take arrests into account, there have been several recent studies linking early alcohol and drug use to delinquent behaviors among AI adolescents (Barnes, Welte, & Hoffman, 2002; Whitbeck, Hoyt, Chen, & Stubben, 2002; Whitbeck, Hoyt, McMorris, Chen, & Stubben, 2001).
Over time, it has become apparent that the linkages between AIAN alcohol and drug use and arrests are more complicated than early research would make them seem. For example, it is imprudent to generalize about substance abuse among AIAN people because of the great diversity among cultures and even among individual communities within cultures (May, 1996). Recent research that indicates higher abstinence rates among some AI communities than in the general U.S. population challenge old stereotypes (Herman-Stahl, Spencer, & Duncan, 2003; Spicer et al., 2003). But other research indicates that in some communities, AIAN adolescents begin drinking earlier, progress more rapidly to regular use (Beauvais, 1998; Blum, Harmon, Harris, Bergeisen, & Resnick, 1992), and have earlier onset of substance use disorders (SUDs) than their counterparts in the general population (Costello, Farmer, Angold, Burns, & Erkanli, 1997; Whitbeck, Yu, Johnson, Hoyt, & Walls, 2008), behaviors that may place AIAN youth at particular risk for negative consequences.
May and Gossage (2001) have pointed out that the majority of adult alcohol-related crimes among Indigenous people are accounted for by a minority of heavy drinking individuals. This is likely the case with juvenile arrests. Young people whose lives are most affected by substance abuse, those who meet diagnostic criteria for SUD, are a minority of heavy users among many abstaining or casual users of alcohol and drugs.
In this article, we investigate the relationships between SUDs, comorbid SUD and other psychiatric disorders, and likelihood of arrest among Indigenous (AI and Canadian First Nations) adolescents. We focus on adolescents who meet criteria for SUD in that they represent the habitual users, those most at risk for alcohol- and drug-related contacts with the criminal justice system, and those in need of treatment on entry into the criminal justice system. We use multivariate analyses of longitudinal data to investigate the effects of meeting criteria for SUD, other psychiatric disorders, and comorbidity when controlling for other known risk factors to test the relative strength of SUD on risk of entering the criminal justice system.
SUDs, Comorbidity, and Juvenile Arrests
Mental disorders are increasingly common among adolescents in the juvenile justice system. Indeed, the criminal justice system has become the primary referral for mentally disordered adolescents (Grisso, 2004). Of particular concern is the disproportionate number of adolescents with SUDs in the juvenile justice system. For example, in their study of adolescents in a Cook County juvenile facility, Teplin, Abram, McClelland, Dulcan, and Mericle (2002) found that approximately half of male and female detainees had a SUD.
Psychiatric disorders rarely occur alone during adolescence (Kessler & Walters, 1998), and this is particularly true of SUDs (Hser et al., 2001). A history of conduct disorder (CD) doubles the risk of SUD (Sung, Erkanli, Angold, & Costello, 2004), and adolescents with externalizing disorders (e.g., CD, oppositional defiant disorder, attention deficit hyperactivity disorder [ADHD]) and co-occurring SUDs typically have worse developmental outcomes and poorer treatment prognoses (Clark & Scheid, 2001). Depressive disorders also often co-occur with adolescent-onset SUD (Clark, Kirisci, & Tarter, 1998), a combination that is associated with multiple negative outcomes (Bukstein, Brent, & Kaminer, 1989) and poor treatment outcomes (Grella, Hser, Joshi, & Rounds-Bryant, 2001). There is evidence among the general population that SUDs, co-occurring with any other psychiatric disorder, increase the likelihood that a person will be arrested (Swartz & Lurigio, 2007). In addition, there is some evidence that comorbidity of substance use and psychiatric disorders is more common among the AI children than majority of children (Costello et al., 1997; Federman, Costello, Angold, Farmer, & Erkanli, 1997), perhaps putting them at particular risk for negative outcomes such as arrest.
Theory and Hypotheses
Early-onset SUD may be an important factor in understanding the etiology and consequences of serious delinquent and criminal behavior among Indigenous adolescents and, along with comorbid psychiatric disorders, may differentiate those who persist in antisocial behaviors from those who engage in more normative adolescent-limited types of delinquency (Moffitt, 1993). SUDs, particularly in concert with externalizing disorders, increase the likelihood of antisocial behaviors by the disinhibiting effects of substance use on judgment and risk taking (Fromme, Katz, & D’Amico, 1997) and in the activities surrounding procurement and use of illegal substances (Arseneault, Moffitt, Caspi, Taylor, & Silva, 2000). Early-onset SUD is strongly associated with later criminality (Loeber, Burke, Lahey, Winters, & Zera, 2000). Co-occurring externalizing disorders and SUDs amplify disruptive, hyperactive, and oppositional problem behaviors that are “requisite for sustained and serious violent offending” (Tolan & Gorman-Smith, 1998, p. 75).
Alcohol dependence develops over 2 to 4 years (Martin, Langenbucher, Kaczynski, & Chung, 1996), and marijuana dependence may take up to 2 years or more to emerge (Rosenberg & Anthony, 2001). Such long-standing patterns of use and abuse are difficult to change. This is especially true for adolescents with co-occurring psychiatric disorders who are less likely to complete treatment programs and more likely to relapse after treatment (Brown, Gleghorn, Schuckit, Myers, & Mott, 1996). SUDs and co-occurring disorders together contribute to the momentum of maladaptive behaviors, establishing trajectories that may become more and more difficult to interrupt. The concept of “cumulative continuity” suggests delinquent adolescents may become ensnared in the consequences of their own behaviors, resulting in lifelong effects (Caspi, Bem, & Elder, 1989; Caspi, Elder, & Bem, 1987). We believe that SUDs and comorbid disorders play an important part of this process.
Based on prior research, we investigate three hypotheses. First, controlling for other risk factors, SUD would increase the odds of arrest among Indigenous adolescents. Second, externalizing disorders (e.g., CD and ADHD) would increase the likelihood of arrest when controlling for other risk factors. Third, given research findings that comorbidity is common among arrested adolescents, we hypothesize that comorbid disorders, specifically SUD and other disorders, would increase the likelihood of arrest over and above the direct effects of any single disorder (Dolamanta, Risser, Roberts, & Risser, 2003; Neighbors, Kempton, & Forehand, 1992; Swartz & Lurigio, 2007).
Method
Procedure
These data were collected as part of an ongoing longitudinal study designed in partnership with four U.S. reservations and four Canadian First Nations reserves and a university-based research team. The reservations share a common cultural tradition and language with minor regional variations in dialects. The sample represents one the most populous Indigenous cultures in the United States and Canada. Prior to the application’s funding, the research team was invited to work with the reservations/reserves, and tribal resolutions were obtained. As part of the partnership agreement, the researchers promised that culture and the names of the participating reservations/reserves would be kept anonymous in published reports.
On each participating reservation, an advisory board representing all reservation/reserve districts was appointed by the tribal council. The advisory boards are responsible for handling difficult personnel problems, advising on questionnaire development and reviewing reports for respectful writing and confidentiality. All participating staff on the reservations/reserves were approved by the advisory boards and were either tribal members or, in a few cases, nonmembers who were spouses of tribal members. To ensure quality of data collection, all the interviewers underwent special training at each wave of the study for conducting pencil-and-paper interviews and computer-assisted personal interviewing for the diagnostic measures. The training included in-class practice, feedback sessions, and homework practice assignments.
Each of the participating reservations and reserves provided a list of families of tribally enrolled children aged 10 to 12 years who lived on or proximate (within 50 miles) to the reservation or reserve. We attempted to contact all families with a target child within the specified age range. Families were recruited with a personal visit by an Indigenous interviewer at which time the project was explained to them. They were then presented with a traditional gift and invited to participate. The recruitment method was approved by advisory boards on each of the reservations and reserves. If the family members agreed to be interviewed, each family member (the target child and at least one parent or caretaker) received US$40 for their time when the interviews were completed. The recruitment procedure resulted in an overall response rate of 79.4%.
Sample
These analyses use data from the first five waves of the study. Overall, this study had very little attrition, with retention rates ranging from 88.1% to 94.6% across the five waves. We used two strategies to address missing data. For the descriptive analyses (bivariate correlations, Table 1; and prevalence of mental disorder, Table 2; and comorbidity, Table 3, among arrested youth), listwise deletion was used for any cases with missing values on any of the included variables. This resulted in a final sample size of 603 adolescents for the descriptive analyses. For the multivariate analyses predicting arrest at Wave 5 (Table 4), missing data were addressed by multiple imputation in Stata using a freeware command called “ice” (Royston, 2005; Royston, Carlin, & White, 2009). Multiple imputation allows parameter estimates to be pooled from a series of imputed data sets, using information from all the covariates included in an analysis, which provides improved parameter estimates and more accurate standard errors than in single imputation methods (Acock, 2005). The use of multiple imputation resulted in a final sample size of 689 adolescents.
Mean, Standard Deviation, and Correlation for All Study Variables (n = 603).
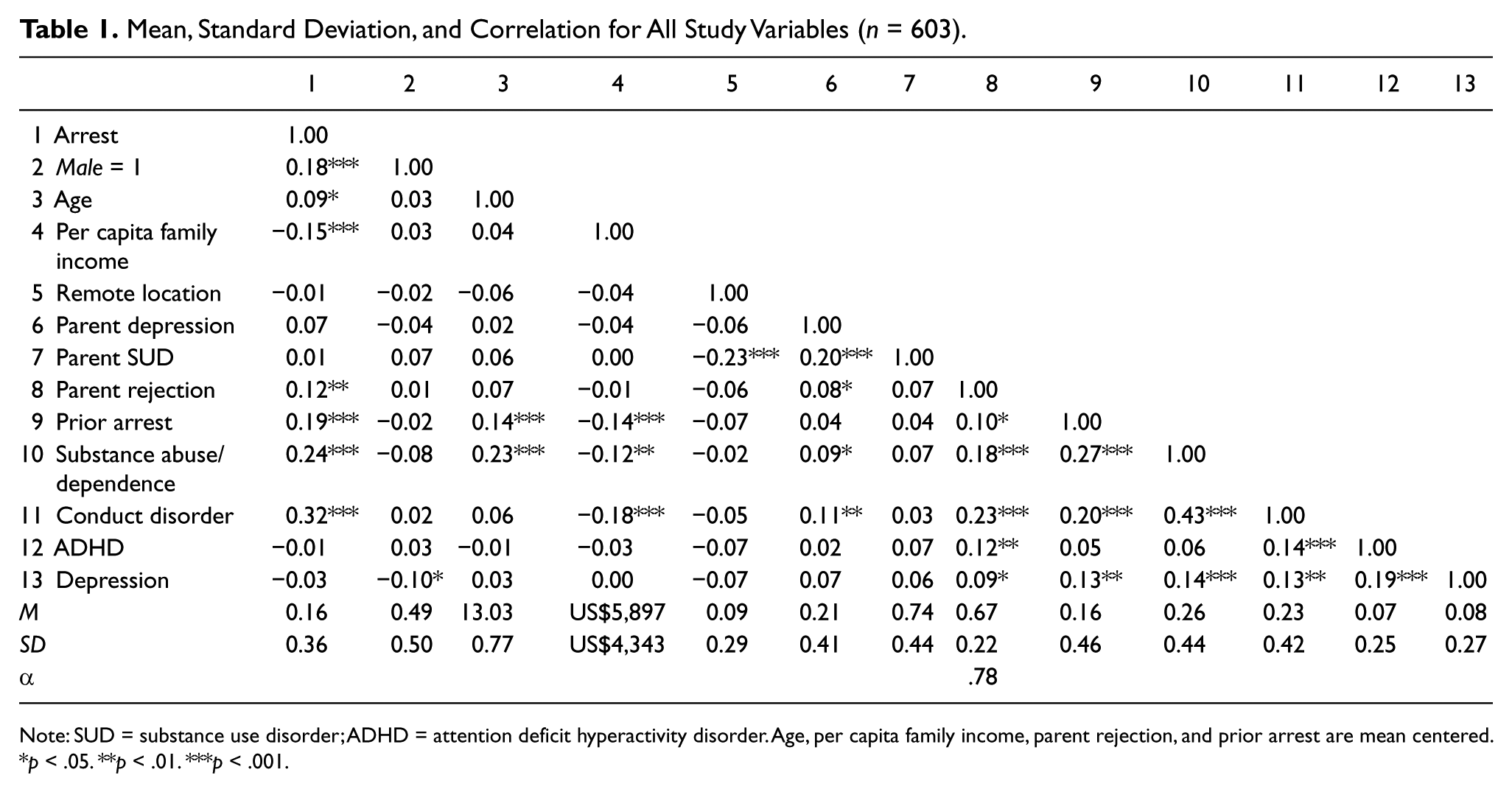
Note: SUD = substance use disorder; ADHD = attention deficit hyperactivity disorder. Age, per capita family income, parent rejection, and prior arrest are mean centered.
p < .05. **p < .01. ***p < .001.
Prevalence of Mental Disorders Among Indigenous Adolescents (n = 603).
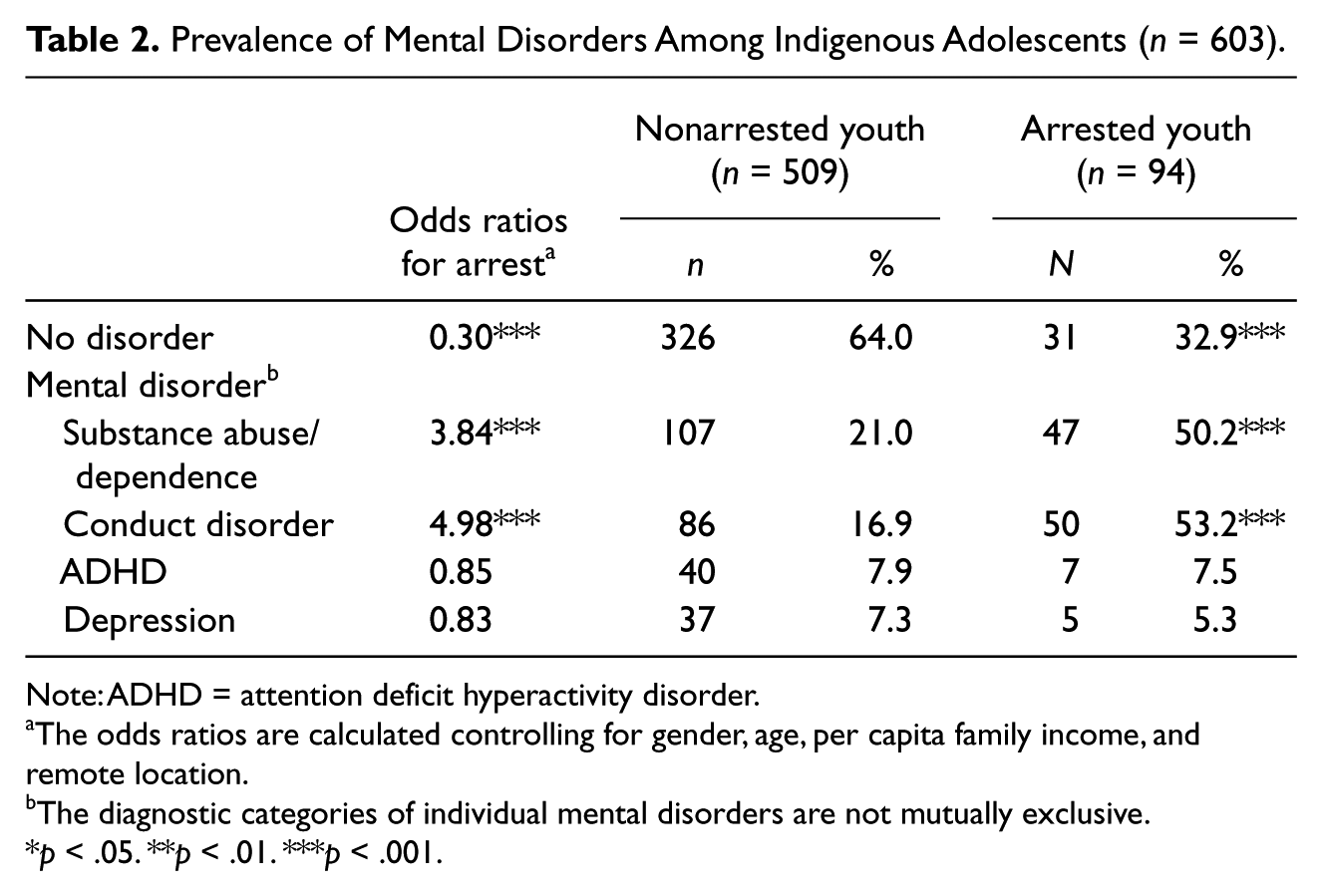
Note: ADHD = attention deficit hyperactivity disorder.
The odds ratios are calculated controlling for gender, age, per capita family income, and remote location.
The diagnostic categories of individual mental disorders are not mutually exclusive.
p < .05. **p < .01. ***p < .001.
Prevalence of Substance Abuse/Dependence and Comorbidity Among Indigenous Adolescents (n = 603).
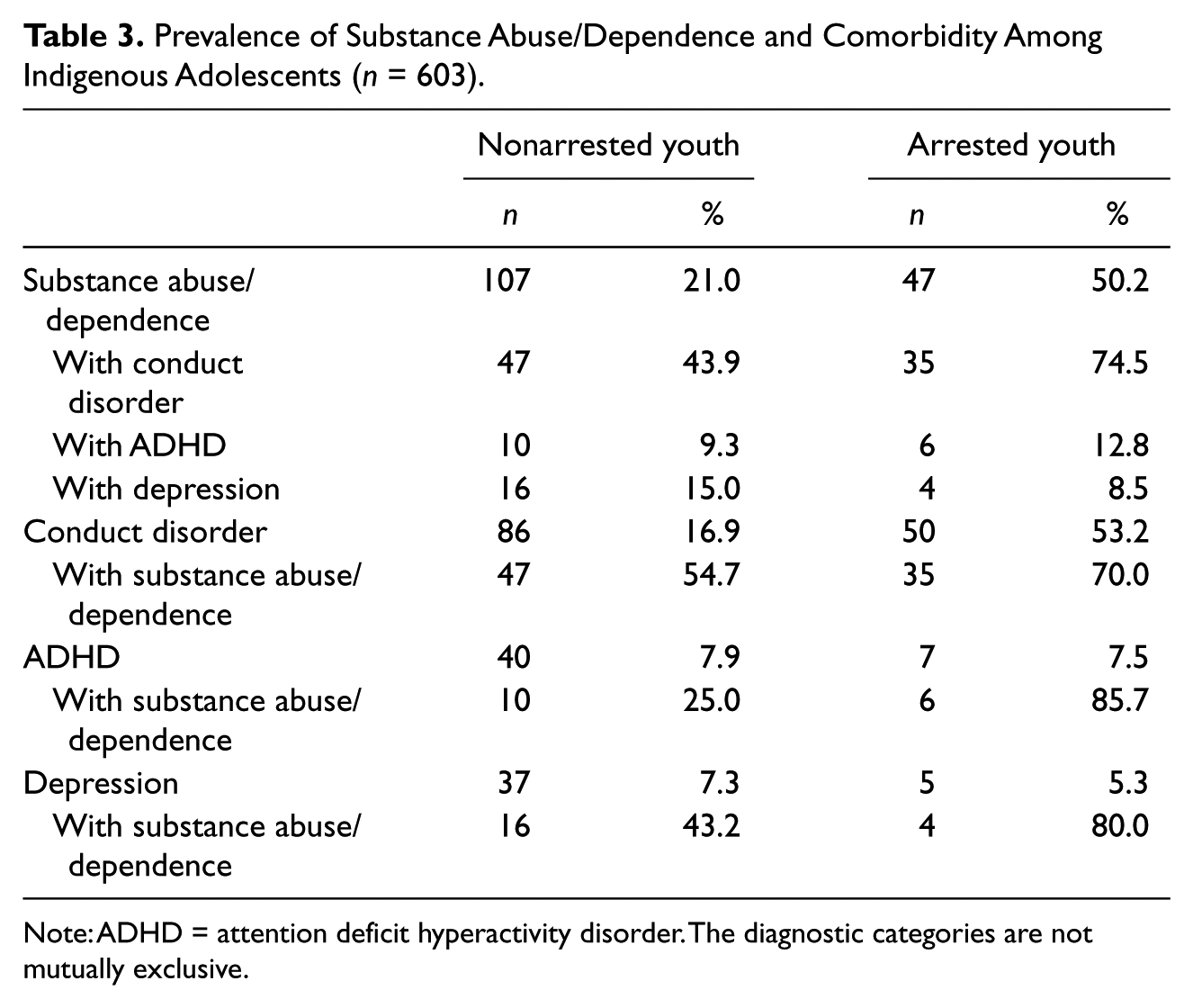
Note: ADHD = attention deficit hyperactivity disorder. The diagnostic categories are not mutually exclusive.
Logistic Regression Models Predicting Arrest (n = 689).
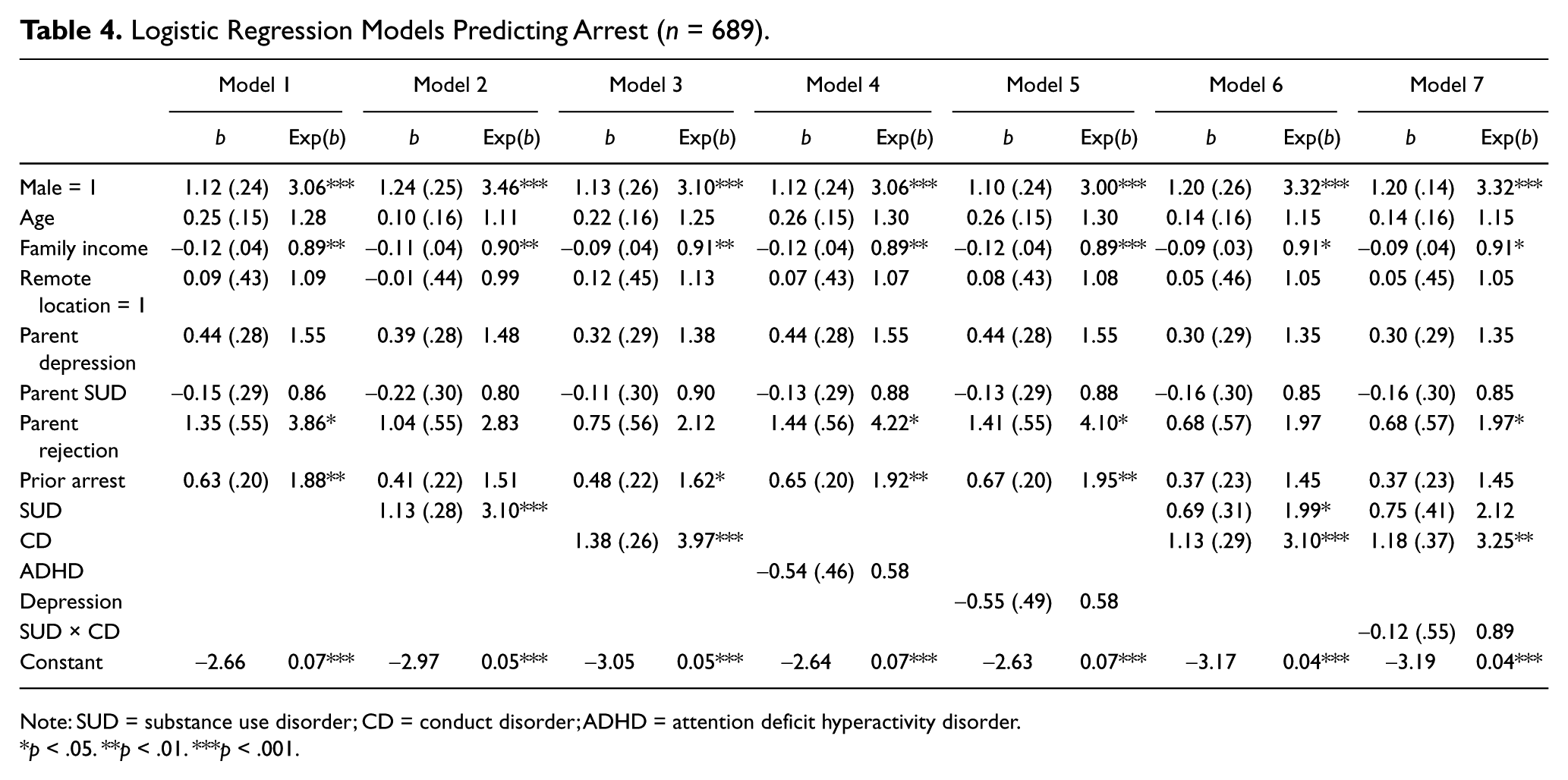
Note: SUD = substance use disorder; CD = conduct disorder; ADHD = attention deficit hyperactivity disorder.
p < .05. **p < .01. ***p < .001.
Measures
Not all variables used in the present article are drawn from the same waves. Although there is considerable consistency of measures used across waves, not all variables are available at every wave. Namely, only diagnostic information was collected in Wave 4, and thus only the mental disorder variables are drawn from that wave. The prior arrest variable comes from the first three waves for that same reason. In addition, our dependent variable is the only variable drawn from Wave 5.
The dependent variable, arrest, was assessed in Wave 5 of the study. The adolescents were asked, “Have you been arrested within the past 12 months?” Those who responded “yes” were coded as 1 and “no” were coded as 0. Approximately 15% of the youth responded that they had been arrested at least once in Wave 5.
To assess youth psychiatric disorders, the Diagnostic Interview Schedule for Children–Revised (DISC-R)Version II CD, ADHD, SUDs (alcohol abuse, alcohol dependence, marijuana abuse, and marijuana dependence), and major depression modules were used. The DISC-R is a highly regarded, structured interview intended for use with trained interviewers who are not clinicians. Computer algorithms were used to determine whether each behavior was present at clinically significant frequency/severity levels. We use the combined youth and parent/caretaker reports, which tend to be more reliable than child reports alone (Schwab-Stone et al., 1996; Shaffer et al., 1996).
Three family risk factors (parental depression, parental substance abuse/dependence, and parental rejection) were included in the study. The University of Michigan Composite International Diagnostic Interview (UM-CIDI), based on the Diagnostic and Statistical Manual of Mental Disorders (3rd ed., text rev.; DSM-III-R; American Psychiatric Association, 1987) criteria, was used to assess parental 12-month parental depression and parental lifetime substance abuse/dependence (parental SUD). Computer algorithms were used to determine whether each behavior was present at clinically significant frequency/severity levels. A single indicator of parental substance use was constructed from the individual substance-related diagnoses (alcohol abuse, alcohol dependence, marijuana abuse, marijuana dependence). Diagnoses were coded as “1” if at least one caretaker met diagnostic criteria and “0” if neither caretaker met criteria.
Parental rejection is a mean indicator of adolescent-reported rejection over the first three waves of the study. At each wave, respondents were asked how often someone in their family really trusts them, blames them when they do not deserve it, really cares for them, blames them for things that others have done, spends time doing things they enjoy, is unhappy with things they do, and gives them attention for things they do. Positively worded questions were reverse coded. A high value indicates higher levels of rejection. The measure had acceptable internal reliability, with a Cronbach’s alpha of .78.
Prior arrest was constructed from responses to the question, “Have you ever been arrested?” (Wave 1) and “Have you been arrested within the past 12 months?” (Waves 2-3). Only diagnostic questions were asked at Wave 4; thus, no youth report of arrest at that wave is included. Youth who responded that they had been arrested were coded as 1. A single index of prior arrest was constructed by summing the responses, with a range of 0 to 3.
Four control variables were included in the analyses, all drawn from Wave 3. Gender is dichotomized and coded as 1 = male. Age is a continuous measure of adolescent age in years. Location refers to the proximity to towns or other communities. There are two locations identified for this sample. A rural location refers to those reservations/reserves within somewhat close proximity to other towns, and remote refers to those far removed from other communities. The variable is coded so that 1 = remote. Per capita family income is measured by asking parents/caretakers to indicate their overall household incomes in the past year. Responses were divided by the number of people living within the household, which was then divided by 1,000 to set the metric of this measure in thousands of dollars.
Analytic Strategy
The analytic strategy of this article is twofold. First, we used bivariate analyses to explore the associations between arrest and SUD, CD, ADHD, major depressive episode, and comorbid SUD with these disorders. Second, we used stepwise logistic regression to test the hypotheses of the associations between mental disorder and arrest.
Results
Mental Disorders/Comorbidity and Arrest
Bivariate correlations, means, and standard deviations are presented in Table 1. Arrest was associated with gender, age, per capita family income, parent rejection, prior arrest, substance abuse/dependence (SUD), and CD. There was no significant association between arrest and depression, or arrest and ADHD.
Prior arrest was associated with SUD and CD; it was also associated with meeting criteria for depression. Parental depression was associated with parent SUD, parent rejection, adolescent SUD, and adolescent CD. Parental rejection was associated with all adolescent mental disorders. Parental SUD was not associated with any adolescent mental disorder.
Table 2 presents the prevalence of the disorders and comorbidity among arrested and nonarrested Indigenous adolescents. Almost two thirds of youth who were not arrested in Wave 5 (64%) had no mental disorder, compared with only one third of arrested youth (32.9%). Adolescents without a disorder had the lowest odds of arrest (odds ratio = 0.30). SUD, although fairly prevalent overall, was much more common among arrested youth: 50.2% of youth arrested in Wave 5 met criteria for SUD, compared with only 21% of nonarrested youth.
One half of adolescents who were arrested met criteria for CD (53.2%). There were no significant differences between arrested and nonarrested youth who met criteria for ADHD or depression.
In addition to the individual disorders, arrested youth were much more likely to have comorbid disorders (Table 3). Of the 47 adolescents with SUD who were arrested in Wave 5, 74.5% had co-occurring CD, 8.5% had co-occurring depression, and 12.8% had co-occurring ADHD. But perhaps more importantly, arrested adolescents with either depression or ADHD had very high rates of co-occurring SUD. Of the five arrested adolescents with depression, four of them also had comorbid SUD. Of the seven arrested adolescents with ADHD, six of them had comorbid SUD. This suggests that SUD is very common among adolescents with depression or ADHD who have been arrested, although neither depression nor ADHD is as prevalent among those with SUD.
SUD comorbidity was less common but still pervasive among adolescents who were not arrested at Wave 5. Of the 107 adolescents with SUD, 43.9% also had CD, 15% had depression, and 9.3% had ADHD. Slightly more adolescents meeting criteria for the other disorders had co-occurring SUD. Of the 86 adolescents with CD, more than half (54.7%) also had SUD, and fewer adolescents with either depression (43.2%) or ADHD (25%) had comorbid SUD.
Logistic Regression Models: SUDs, Comorbidity, and Arrest
Arrest risk factors and individual mental disorders affecting the probability of arrest were explored in a series of logistic regression models (Table 4). The four control variables (gender, age, per capita family income, and remote location), family risk factors (parental depression, parental SUD, and parental rejection), and prior arrest were entered simultaneously in the first model. Of the control variables, only income and gender were significant. Males, b = 1.12, exp(b) = 3.06, had significantly higher odds of arrest than females, but age of adolescent was unrelated to arrest. Of the family risk factors for arrest, only perceived parental rejection was associated with arrest. A 1-unit increase in parental rejection above the mean was associated with an almost fourfold increase in risk of arrest, b = 1.35, exp(b) = 3.86. As expected, prior arrest was associated with later arrest. For each additional prior arrest above no arrest, the odds of subsequent arrest increased by 88%, b = 0.63, exp(b) = 1.88.
To address the first two hypotheses that SUD and externalizing disorders, respectively, would increase the odds of arrest among Indigenous adolescents, each individual mental disorder was added separately into the logistic regression models. Similar to the bivariate analyses, SUD and CD were each significantly associated with arrest. The odds of arrest for adolescents who met criteria for SUD were 3 times higher than for adolescents without the disorder, Model 2, b = 1.13, exp(b) = 3.10. Adolescents with CD had odds of arrest almost 4 times higher than adolescents without CD, Model 3, b = 1.38, exp(b) = 3.97. As in the bivariate analyses, ADHD (Model 4) and depression (Model 5) were not associated with later arrest.
Because both SUD and CD were so strongly associated with arrest, and because there is considerable comorbidity of the two disorders, we tested a model with both disorders entered simultaneously (Model 6). SUD and CD remained significant when both were included, although the odds ratios were smaller than those in Models 2 and 3 with the disorders entered separately. Adolescents with SUD had odds of arrest that were twice as high as in adolescents without SUD, controlling for CD, b = 0.69, exp(b) = 1.99. Adolescents with CD had odds of arrest that were more than 3 times higher than in adolescents without CD, controlling for SUD, b = 1.13, exp(b) = 3.10. To address the third hypothesis that comorbidity of SUD with other disorders will increase the odds of arrest, we tested an interaction effect of SUD and CD (Model 7). The association was not significant, indicating that there is not a joint effect of the two disorders beyond the additive combinations of their individual effects. Because neither ADHD nor depression had significant direct effects, we did not test any interactions with those disorders and SUD.
Discussion
Consistent with prior research (Duclos et al., 1998; Hartney, 2008), Indigenous adolescents with SUD or CD reported high arrest rates. More than half of adolescents who were arrested met criteria for either SUD or CD. Comorbidity, particularly for adolescents who met criteria for SUD and CD, was very common among arrested adolescents. Importantly, adolescents who met criteria for ADHD and MDE were much more likely to have been arrested if they had concurrent SUD. Indeed, of the seven young people with ADHD who were arrested, six also met criteria for SUD. Similarly, of the five depressed adolescents who were arrested, four met criteria for SUD. Neither of these two disorders, however, increased the odds of arrest.
SUDs also were linked to arrests in the multivariate analyses. Meeting criteria for SUD in Wave 4 increased the likelihood of Wave 5 arrest 3 times, and meeting criteria for CD at Wave 4 increased the odds of Wave 5 arrest 4 times. We were surprised to find that the interaction between SUD and CD was not statistically significant. That is, both disorders exerted independent effects but did not have a joint effect on the likelihood of arrest. The lack of association between ADHD and arrest has been documented in other studies (Hirschfeld, Maschi, White, Traub, & Loeber, 2006; Satterfield & Schell, 1997). There is evidence that it is the hyperactivity/impulsivity subtype that is associated with delinquency rather than the attention deficit subtype (Babinski, Hartsough, & Lambert, 1999; Carroll et al., 2006; Lahey & Loeber, 1997), a distinction we could not make in the current study. Similar to ADHD, MDE was not related to Wave 5 arrests regardless of gender of adolescent. This could be due to the small number of adolescents who met criteria for MDE.
There were several interesting findings regarding control variables and family risk factors. First, adolescent age was unrelated to odds of arrest. Second, parental mental health was not associated with adolescent arrest. Of little surprise were the findings regarding gender, parental rejection, and prior arrest. Boys, adolescents who felt rejected by their caretakers prior to Wave 5, and adolescents who had been arrested in previous waves were more likely to be arrested in Wave 5. This is congruent with gendered arrest patterns (Federal Bureau of Investigation, 2009), a considerable body of research that shows family effects on delinquent behaviors (Blumstein, Cohen, Roth, & Visher, 1986; Chatterji & Markowitz, 2001; Farrington, Barnes, & Lambert, 1996; Rowe & Farrington, 1997; Rutter, Giller, & Hagell, 1998) as well as the stability of delinquent behavior across time (Nagin & Farrington, 1992; Nagin & Paternoster, 1991; Sampson & Laub, 2005).
Limitations
There are several important limitations to this study that deserve consideration. First, it was based on a single Indigenous culture and may not be generalizable to other Indigenous populations. However, because of the great diversity among cultures and the near impossibility of obtaining a random, representative sample across all of the more than 500 cultures, research such as this must proceed culture by culture and rely on cumulative information as it emerges. Second, the study adolescents lived either on or close to rural reservations, so these results may not reflect the experiences of urban Indigenous young people even if they share the same cultural background. Third, there is always the concern that European diagnostic measures do not take into account cultural differences. Our diagnostic measures, however, are the same as those used in major epidemiological studies of AI people. At this point, these are the best measures available. Fourth, our reliance on self-report data invites the criticism of potential social desirability bias, but we believe the most likely bias would be underreporting arrests and problem behaviors, making our findings conservative.
Conclusion
Our findings extend previous research linking substance abuse and arrests among Indigenous adolescents through the use of diagnostic measures to identify those most at risk for serious, perhaps lifelong consequences. Only about 5% of adolescents in the general population are likely to be life course persistent antisocial (Moffitt, 1993). Although it is difficult to accurately project the continuation of problem behaviors, we know that these are the young people most at risk for persistent problems with alcohol and drugs and involvement with the criminal justice system into adulthood (Loeber, Stouthamer-Loeber, & White, 1999; Moffitt, Caspi, Harrington, & Milne, 2002). By first arrest, adolescents with this combination of life experiences may already be on a trajectory of negative, self-reinforcing events that will become harder and harder to moderate as time goes by (Sampson & Laub, 2005; E. A. Stewart, Simons, Conger, & Scaramella, 2002). They are more likely to be rearrested (Gendreau, Little, & Goggin, 1996; Wierson & Forehand, 1995), they are less likely to complete treatment programs (Clark & Scheid, 2001; Kaminer, Tarter, Bukstein, & Kabene, 1992), and if treatment is mandated, they are more likely to relapse (Brown et al., 1996; Grella et al., 2001).
The key may be early identification and treatment of related SUD and mental disorders either prior to or at first contact with the criminal justice system. Diversionary programs that require psychological and substance abuse evaluations along with interventions and/or family-based interventions (Mmari, Blum, & Teufel-Stone, 2010; Pullmann et al., 2006) may reduce early and repeated arrests. Moreover, diversionary programs may be more cost-effective than incarceration for substance abusing offender (Mauser, Van Stelle, & Moberg, 1994). But first arrest already may be too late in a cumulative process. Very early assessments to identify and intervene with high-risk children may reduce the arrest rate in the long term. As we have pointed out, most substance-related crimes are committed by a very small group of heavy users (May & Gossage, 2001). These heavy users were likely early-onset substance abusers. Genuinely high-risk adolescents are a small group of early-onset substance abusers almost certainly with preexisting behavioral problems associated with CD, oppositional defiant disorder, and/or ADHD. Early identification and intervention with these relatively few children and their families would be extremely cost-effective in monetary and human terms. Without such interventions, we may be relegating some of these children to an adolescence ensnared in a sequence of disruptive behaviors, poor academic performance, affiliation with delinquent peers, substance use, and eventually involvement in the criminal justice system. If arrest is the point of first intervention, we already may be too late.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the National Institute on Drug Abuse (DA13580) and the National Institute of Mental Health (MH67281), and Les B. Whitbeck, principal investigator.