
Abstract
This study compared sociodemographic characteristics, adverse childhood experiences (ACEs), and substance use and psychiatric disorders between adolescent-limited (AL), adult-onset (AO), life-course-persistent (LP) and nonoffender (NO) groups using a large U.S. general population survey. The odds of experiencing several ACEs were greater among each offender group relative to NOs. LP offenders experience more ACEs than AL and AO offenders. Each offender group generally experienced greater substance use and psychopathology than NOs, whereas LP offenders experienced more substance use and psychopathology than AO and AL offenders. The results of this study identified several sociodemographic factors, ACEs, and types of psychopathology that differentiate AL, AO, LP, and NO offenders that can help inform prevention and intervention strategies designed to prevent offending and shorten criminal careers.
Introduction
Two of the most significant and recurring findings in the criminal behavior literature are that juvenile (Abram et al., 2003, 2004, 2015; Colins et al., 2010; Fazel et al., 2008; Gottfried & Christopher, 2017; McClelland et al., 2004; Ryan & Redding, 2004; Teplin et al., 2002; Teplin et al., 2012) and adult (Bronson et al., 2017; National Center on Addiction and Substance Abuse at Columbia University, 2010) offenders have high rates of substance use disorders and other psychiatric disorders and experience adverse childhood experiences (ACEs; e.g., sexual, physical abuse) (Aebi et al., 2015; Friestad et al., 2014; King et al., 2011; National Center on Addiction and Substance Abuse at Columbia University, 2010) disproportionately in relation to the general population. Furthermore, ACEs have been linked to substance use and psychiatric disorders (Li et al., 2016; Lindert et al., 2014; Maniglio, 2012; Varese et al., 2012) and these findings generalize across juvenile offenders (Baglivio et al., 2014; Fox et al., 2015; King et al., 2011; Underwood & Washington, 2016; Vahl et al., 2016), adult offenders (Friestad et al., 2014; Kim et al., 2016; Varese et al., 2012), psychiatric patients (Westermair et al., 2018), and general population samples (Björkenstam et al., 2017; McLaughlin et al., 2012).
Relative to individuals who did not experience ACEs, individuals with higher exposures to ACEs demonstrate detrimental effects on multiple domains later in life, including a broad array of psychiatric disorders, especially substance use and abuse and other psychiatric disorders (Craig et al., 2017; Dube et al., 2003). In addition, ACE exposure has been found to differentiate early-onset chronic and other offender patterns (Baglivio et al., 2014; Beckley et al., 2016). Among adjudicated juveniles, exposure to ACEs has been associated with increased risk of rearrest, decreased length of time to rearrest, increased risk of becoming seriously violent and chronic offenders, and increased likelihood of encountering the criminal justice system among those already at risk (e.g., those from disadvantaged backgrounds; Baglivio et al., 2014, 2017; Craig, 2019; Fox et al., 2015; Wolff et al., 2015).
The relationship between substance use, substance use disorders, other psychiatric disorders, ACEs, and sociodemographic factors and criminality has often been studied within a life-course taxonomic perspective. Many of these methods of classifying offenders are age based, with the most influential model proposed by Moffitt (1993). In this model, adolescent-limited (AL) offenders are hypothesized to restrict their antisocial behaviors to their teen years. In contrast, life-course-persistent (LP) offenders begin offending in childhood and early adolescence and do not desist, committing a range of offenses throughout their life course (Moffitt & Caspi, 2001; Odgers et al., 2008). In addition to Moffit’s AL and LP offenders, an important additional offender prototype has emerged, that is, the adult-onset (AO) offender, who initiates offending after adolescence (Carrington et al., 2005; Farrington et al., 2009; Kratzer & Hodgins, 1999; McGee & Farrington, 2010; Zara & Farrington, 2009).
Most studies to date that aim to differentiate the four offender types (AL, LP, AO, and nonoffender [NO]) have focused on comparisons between AL and LP offenders as a test of Moffit’s (1993) typology (Assink et al., 2015; Fairchild et al., 2013), whereas very few have assessed risk factors differentiating all four offender types (Jolliffe et al., 2017a). Furthermore, none of these studies examined detailed ACEs or diagnostically defined specific substance use, substance use disorders, and other psychiatric disorders.
Criminology research is increasingly focused on an epidemiological population-based understanding of offender prototypes where offender types are differentiated by a broad array of risk factors (DeLisi & Piquero, 2011; Vaughn et al., 2015). Consistent with the recent calls for the incorporation of large epidemiological datasets into the study of criminology (epidemiological criminology; Akers & Lanier, 2009; DeLisi et al., 2018), this study compares sociodemographic characteristics, substance use, substance use disorders, and other psychiatric disorders and ACEs among four groups defined by offender status (AL, AO, LP, and NO) in a large epidemiological survey of the United States. The National Epidemiologic Survey of Alcohol and Related Conditions-III (NESARC-III; Grant, 2014) is perfectly suited to this objective in terms of extensive information collected on sociodemographic factors, ACEs, substance use and substance use disorders, and other psychiatric disorders defined by the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; American Psychiatric Association, 2013).
Identifying sociodemographic, ACE, and mental health risk factors that differentiate offender groups can inform prevention and intervention efforts to target those factors with a view toward addressing sociodemographic, early trauma-related experiences and mental health needs of offender groups while enhancing public safety and reducing recidivism. Identifying those factors that differentiate offender groups can also lead to important insights about the etiology of criminal behavior and suggest more refined future hypotheses to examine its origins.
Sample
The 2012–2013 NESARC-III is a nationally representative, face-to-face interview survey of 36,309 adults aged 18 years and older (mean age = 45.6 years) residing in households and selected group quarters, with respondents selected through multistage probability sampling (Grant, 2014). Primary sampling units were counties or groups of contiguous counties, secondary sampling units were groups of U.S.-Census-defined blocks, and tertiary sampling units were households within sampled secondary sampling units within which each eligible adult respondent was selected. Black, Asian or Pacific Islander, and Hispanic individuals were oversampled. The household response rate was 72.0%, the person-level response rate was 84.0%, and the overall response rate was 60.0%, which were comparable with other current national surveys (Adams et al., 2013; Substance Abuse and Mental Health Services Administration, 2012). Data were adjusted for oversampling and nonresponse and weighted to represent the U.S. civilian population based on the 2012 American Community Survey (U.S. Census Bureau, 2013). Weighting adjustment compensated for nonresponse (Grant, 2014; Grant et al., 2015a); the National Institutes of Health and Westat Institutional Review Boards approved the protocol and informed consent procedures.
Offender Groups
NESARC-III respondents were asked whether they were (a) ever in a jail, prison, or juvenile detention center before the age of 18 and (b) ever in a jail, prison, or correctional facility since age 18 years. Four mutually exclusive offender groups were constructed: AL before the age of 18 only; AO since age 18 only; LP both before and after 18; and NOs with no jail or incarceration history.
ACEs
All questions about ACEs related to respondents’ first 17 years of life. Questions were adopted from the Adverse Childhood Events Study (M. Dong et al., 2003; Dube et al., 2003) and were originally part of an extensive battery of questions appearing on the Conflict Tactics Scale (CTS; Straus, 1979; Straus & Gelles, 1990) and the Childhood Trauma Questionnaire (CTQ; Bernstein et al., 1994; Wyatt, 1985).
There were seven ACE scales examined in this study with several items operationalizing each scale: emotional abuse, physical abuse, emotional neglect, physical neglect, sexual abuse, witnessing domestic violence, and other childhood trauma. Items in the other childhood trauma scale were coded as 1 = “yes” and 0 = “no.” Emotional abuse, physical abuse, emotional neglect, sexual abuse, and witnessing domestic violence ACE scale items were coded as 0 = “never,” 1 = “rarely,” 2 = “sometimes,” 3 = “often,” and 4 = “very often.” The emotional neglect scale was reverse coded to yield 0 = “never,” 1 = “rarely,” 2 = “sometimes,” 3 = “often,” and 4 = “very often” categories.
Items associated with each ACE scale were summed and any positive response to at least one item within each scale constituted a positive response for that scale for the purpose of this study, that is, at least one positive (1 = yes) response for the other childhood trauma scale, or at least one positive response (response categories 1–4) for all the other ACE scales. Test–retest reliabilities of each ACE scale as ascertained in a general population sample were excellent (kappa = 0.69–0.89; Ruan et al., 2008).
Emotional abuse and physical abuse were operationalized by three and two questions from the CTS, respectively. For emotional abuse, questions asked how often respondents’ parents or caregivers living in their home (a) swore at, insulted, or said very hurtful things to the respondent; (b) threatened to hit or throw something at the respondent but did not; and (c) acted in any way that made the respondent afraid that he or she would be physically hurt or injured. For physical abuse, the frequency of (a) pushing, grabbing, shoving, slapping, or hitting and (b) hitting so hard that the respondent had marks or bruises was ascertained.
For both emotional and physical neglect, sets of five CTQ items were used. Items assessing physical neglect included the frequency with which respondents (a) were made to do chores too difficult or dangerous for their age; (b) were left alone or unsupervised when they were too young to be alone; (c) went without things they needed like clothing, shoes, or school supplies; (d) went hungry or were not being provided with regular meals; and (e) had parents or caregivers fail to get them medical treatment when the respondent was sick or hurt. Items assessing emotional neglect included the following: (a) there was someone in the respondent’s family that wanted him or her to be a success; (b) there was someone in the family who helped the respondent feel important or special; (c) the respondent’s family was a source of strength and support; (d) the respondent felt that he or she was part of a close-knit family; and (e) someone in the respondent’s family believed in him or her.
Childhood sexual abuse was defined by four questions developed by Wyatt (1985). All sexual abuse questions asked about sexual experiences with an adult or any other person and were restricted to behaviors that respondents did not want and were experienced when respondents were too young to know what was happening. The sexual abuse questions included (a) touching and fondling; (b) touching in a sexual way; (c) attempting to have sexual intercourse; and (d) actually having sexual intercourse.
Having a battered mother or female caregiver was defined by four questions from the CTS that assessed the frequency with which each respondent’s father, stepfather, foster or adoptive father, or mother’s boyfriend engaged in any of the following ways toward the respondent’s mother: (a) pushing, grabbing, slapping, or throwing something at her; (b) kicking, biting, hitting her with a fist, or hitting her with something hard; (c) repeatedly hitting her for at least a few minutes; and (d) threatening her with a knife or gun, or using a knife or gun to hurt her.
The other childhood trauma scale consisted of six items that measured general household dysfunction. The items included the following experiences occurring before the respondent was 18 years to a parent or other adult with whom they lived with: (a) have an alcohol problem; (b) have a drug problem; (c) went to jail or prison; (d) treated or hospitalized for a mental illness; (e) attempted suicide; or (f) actually committed suicide.
Substance Use and Psychiatric Disorders
The Alcohol Use Disorders and Associated Disabilities Interview Schedule—Fifth Edition (AUDADIS-5) separately assessed alcohol, cannabis, nicotine, and any other drug use (cannabis, cocaine, sedative/tranquilizer, opioid, inhalant/solvent, hallucinogen, stimulant, club drug, heroin, and other) on a lifetime basis. Test–retest reliabilities of these drug use measures were excellent (kappa = 0.70–0.73) in general population samples (Grant et al., 2003, 1995).
The AUDADIS-5 assessed DSM-5 past-year and prior-to-the-past-year diagnoses of alcohol, cannabis, nicotine, and other drug use disorders. The DSM-5 criteria for all drug use disorders required at least two of 11 criteria in a 12-month period. Twelve-month and at any time prior-to-the-last-12-month diagnoses were aggregated to form lifetime diagnoses for each drug. Test–retest reliabilities of these substance use disorders were good to excellent (kappa = 0.41–0.72) in a general population sample (Grant et al., 2015b). Validity of substance use disorders, as ascertained through clinical reappraisals using the clinically administered Psychiatric Research Interview for Substance and Mental Disorders (PRISM-5; Hasin et al., 2011), was good to excellent (kappa = 0.44–0.72; Hasin et al., 2015a).
Lifetime DSM-5 psychiatric disorders assessed in the AUDADIS-5 included major depressive disorder (MDD), bipolar I disorder, persistent depression, panic disorder, agoraphobia, generalized anxiety disorder (GAD), and social and specific phobias. Consistent with the DSM-5, all mood and anxiety disorders were independent diagnoses, that is, substance-induced or medically induced diagnoses were excluded. Posttraumatic stress disorder (PTSD), antisocial personality disorder (ASPD), and borderline and schizotypal personality disorders were also assessed. Test–retest reliabilities and validities of these diagnoses were fair to good as ascertained in general population samples (Grant et al., 2015b; Hasin et al., 2015b).
Statistical Analyses
Weighted cross-tabulations were used to derive the prevalences of sociodemographic characteristics (sex, age, race–ethnicity, family income, education, marital status, urbanicity, region of country), ACEs and substance use, substance use disorders, and other psychiatric disorders for each offender group. Chi-square tests compared these characteristics across offender groups. Multivariate logistic regression analyses were used to compare each offender group with all others across the various ACEs, controlling for sociodemographic factors. A final series of multivariable logistic regression analyses compared each offender group with all others across substance use, substance use disorders, and other psychiatric disorders, controlling for sociodemographic factors and ACEs. The Stata software was used to account for the complex survey design of the NESARC-III (StataCorp, 2019). 1
Results
Sociodemographic Characteristics
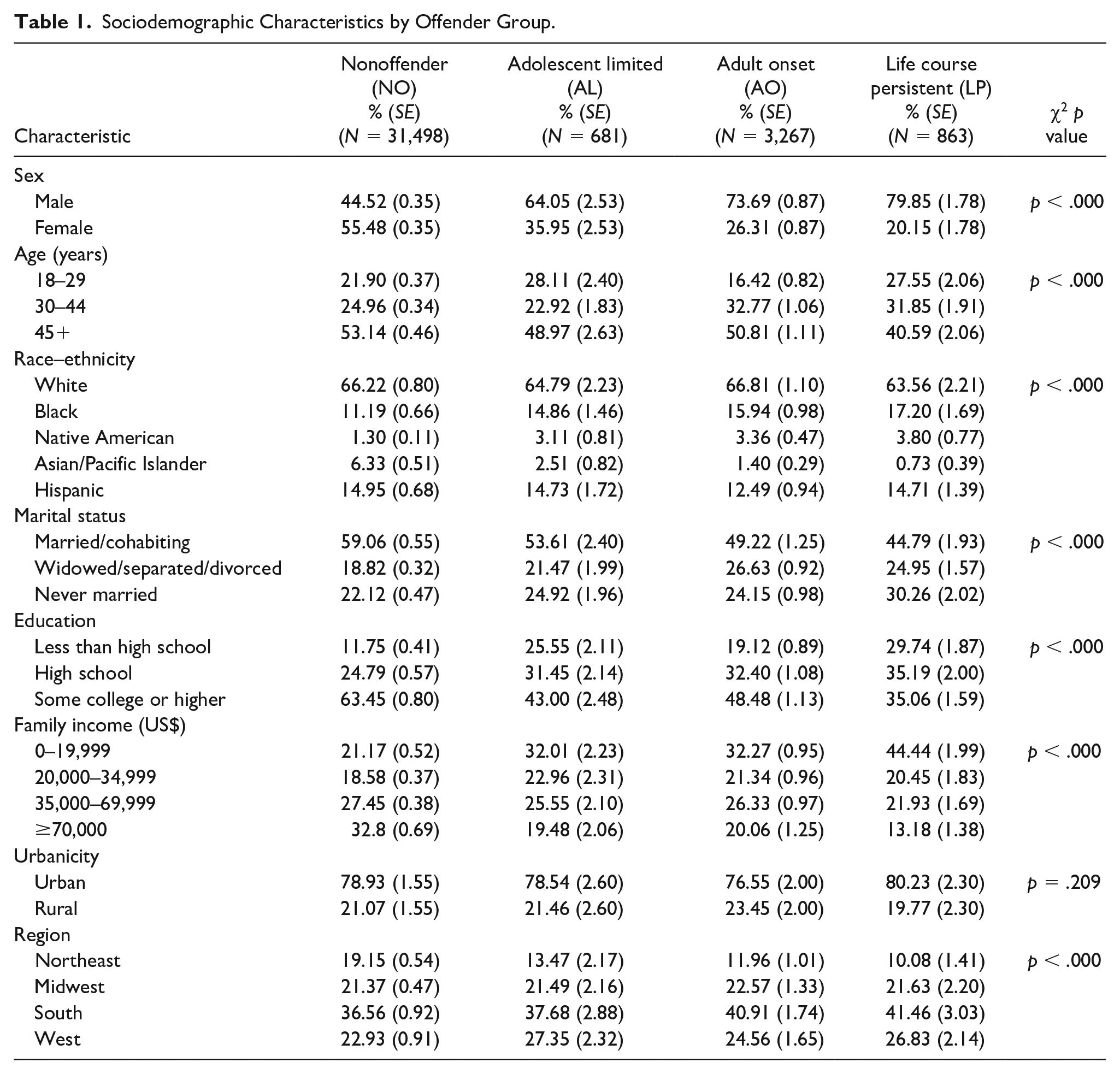
The prevalences of AL, AO, and LP offenders were 1.8%, 8.4%, and 2.2%, respectively. AL, AO, and LP offenders were more likely to be male relative to NOs. AO offenders were less likely to be 18 to 29 years old relative to AL, LP, and NO offenders and LP offenders were less likely to be older (45+ years old) relative to all other offender groups. Compared with NOs, AL, AO, and LP offenders were more likely to be Black or Native American, but less likely to be Asian/Pacific Islander. LP offenders were more likely to never be married/cohabitating compared with the other three offender groups. AL, AO, and LP offenders were more likely to have high school/less than high school education and lower income (<US$0–US$19,999) relative to NOs, whereas NOs were more likely to have some college or higher education and incomes of ≥US$70,000 relative to the three offender groups. Little differentiation between NOs and AL, AO, and LP offenders was observed for urbanicity or region of the country (Table 1).
Sociodemographic Characteristics by Offender Group.
ACEs
Table 2 shows the prevalences and odds ratios (ORs; adjusted for sociodemographic characteristics) of ACEs by offender group. Without exception, the prevalence of each ACE was greater among AL, AO, and LP offenders than NOs and greater among AL and LP offenders than AO offenders. The odds of each ACE was greater among LP than AO offenders (ORs = 1.5–2.2), whereas the odds of physical abuse, witnessing domestic violence, and other childhood trauma were greater among LP relative to AL offenders (ORs = 1.5–1.7). The odds of all ACEs except physical abuse and neglect and emotional abuse were lower among AO compared with AL offenders (ORs = 0.6–0.8).
Prevalences and Adjusted Odds Ratios (AORs) a of Adverse Childhood Experiences by Offender Group.
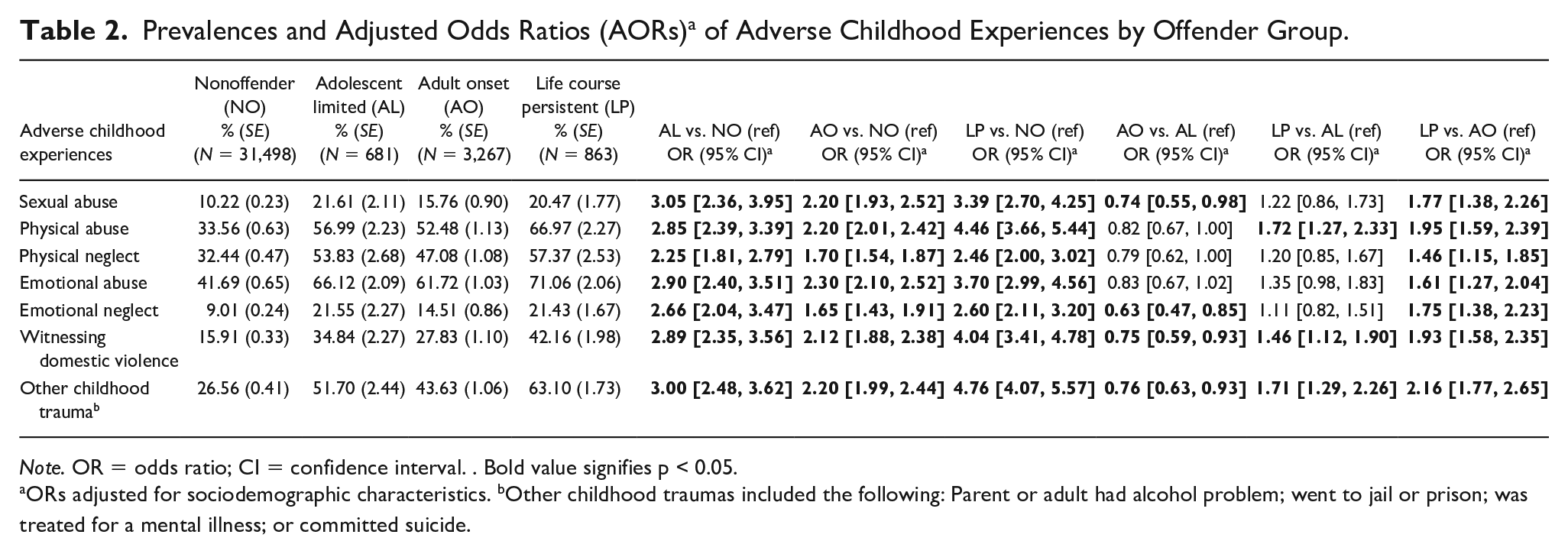
Note. OR = odds ratio; CI = confidence interval. . Bold value signifies p < 0.05.
ORs adjusted for sociodemographic characteristics. bOther childhood traumas included the following: Parent or adult had alcohol problem; went to jail or prison; was treated for a mental illness; or committed suicide.
Substance Use and Psychiatric Disorders
Tables 3 and 4 show the prevalences and adjusted ORs of substance use and substance use and psychiatric disorders by offender group. In general, prevalences of all substance abuse, substance use, and psychiatric disorders were greater among all offender groups relative to NOs and greater among AL and LP offenders compared with AO offenders.
Lifetime Prevalences of Substance Use and DSM-5 Substance Use and Psychiatric Disorders by Offender Group.
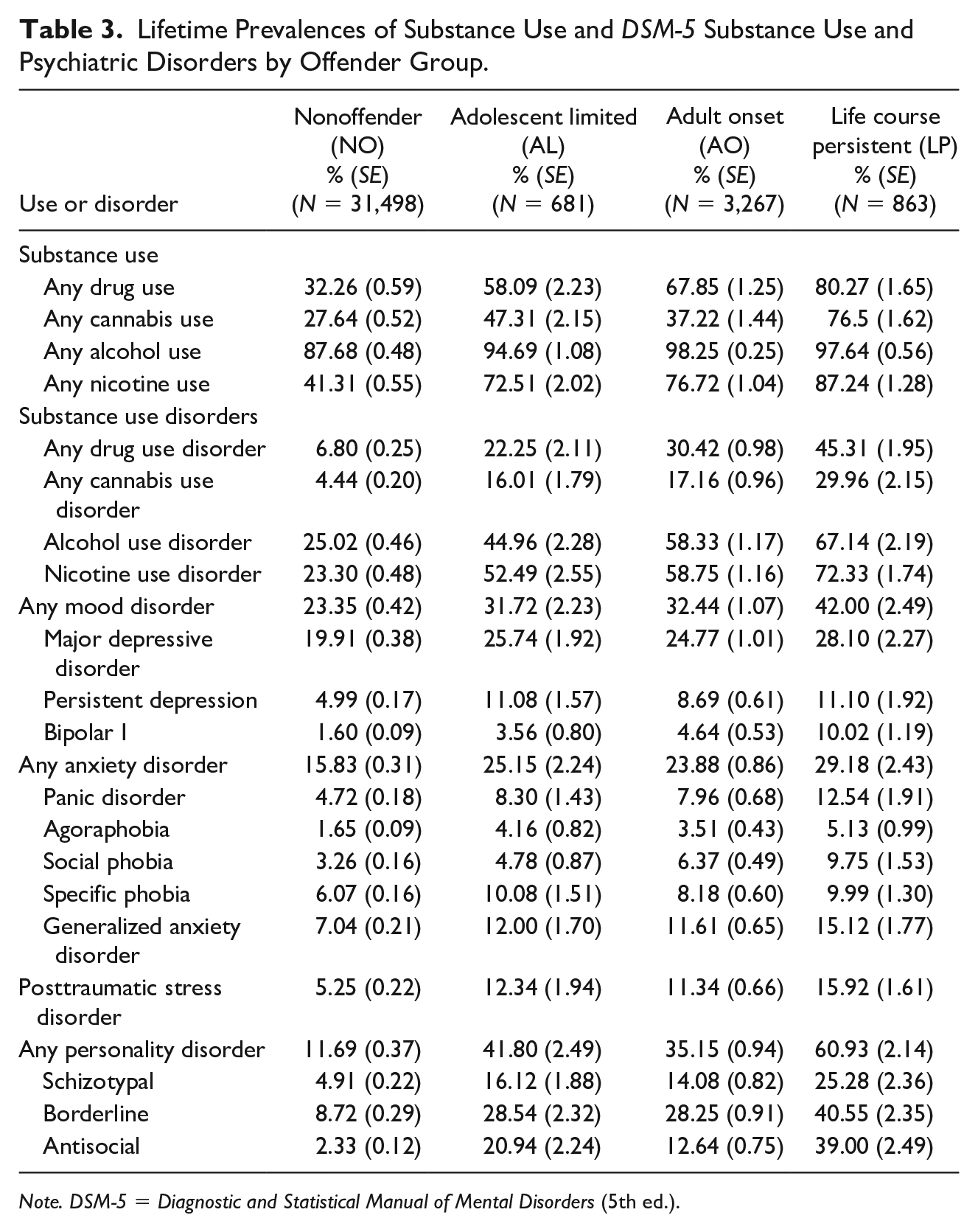
Note. DSM-5 = Diagnostic and Statistical Manual of Mental Disorders (5th ed.).
Adjusted Odds Ratios (AORs) a of Lifetime Substance Use and DSM-5 Substance Use Disorders and Psychiatric Disorders by Offender Group.
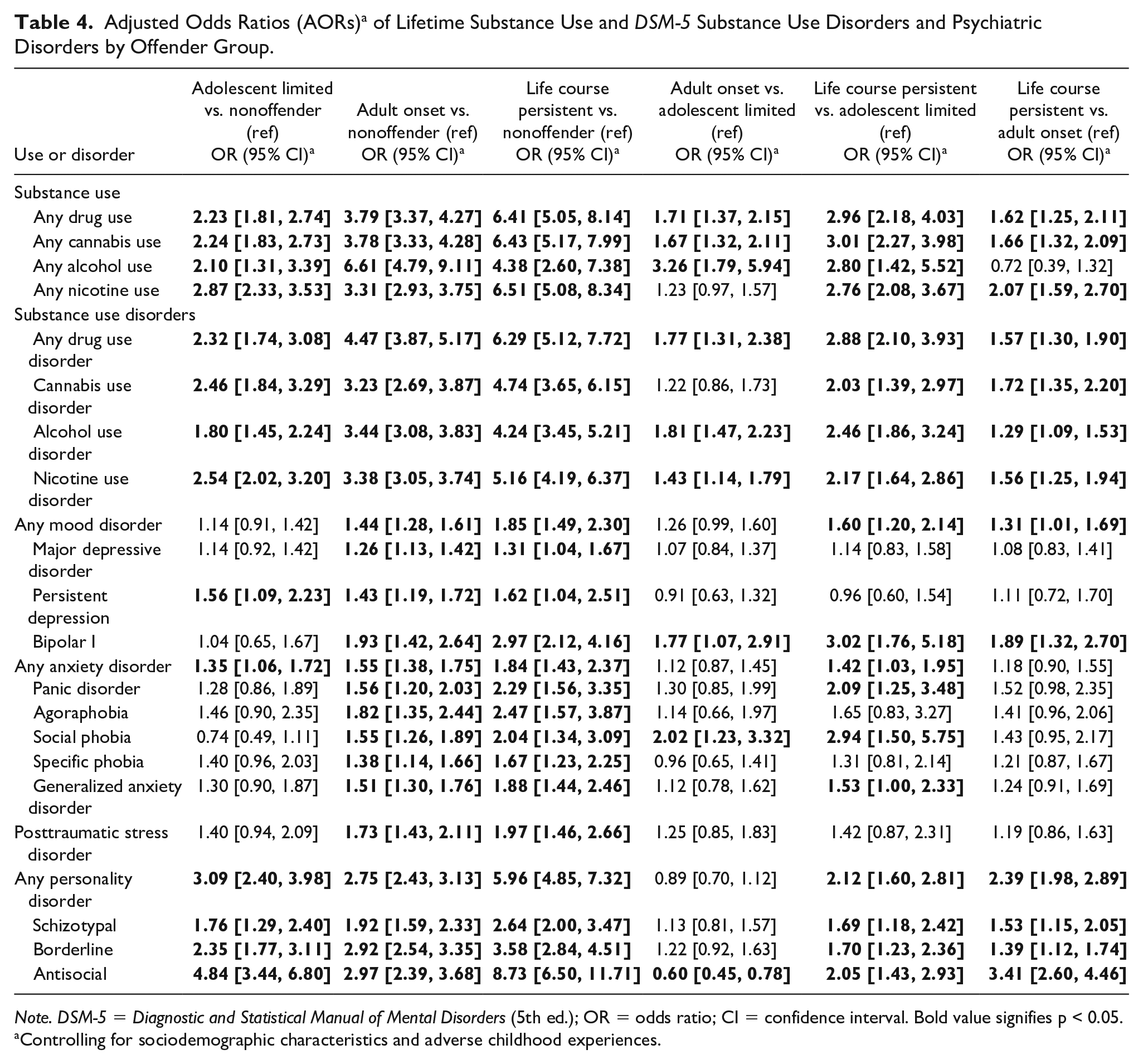
Note. DSM-5 = Diagnostic and Statistical Manual of Mental Disorders (5th ed.); OR = odds ratio; CI = confidence interval. Bold value signifies p < 0.05.
Controlling for sociodemographic characteristics and adverse childhood experiences.
The odds of all substance use and substance use and psychiatric disorders were greater among AO and LP offenders relative to NOs (ORs = 1.3–8.7). The odds of all substance use and substance use disorders, persistent depression, ASPD, and borderline and schizotypal PDs were greater among AL offenders relative to NOs (ORs = 1.3–4.8). The odds of most substance use, bipolar I disorder, ASPD, and borderline and schizotypal PDs were greater among LP offenders than AL and AO offenders. In addition, the odds of panic disorder, social phobia, and GAD were greater among LP offenders compared with AL offenders. The odds of most substance use (except nicotine use), most substance use disorders (except cannabis and nicotine use disorder), bipolar I disorder, and social phobia were greater among AO offenders relative to AL offenders, whereas the odds of ASPD were lower among AO offenders compared with AL offenders.
Discussion
The prevalences of AL, AO, and LP offenders were 1.8%, 8.4%, and 2.2%, respectively, in this nationally representative survey. Prevalence estimates of offender types are rarely available in general population surveys. Only one study (Vaughn et al., 2015) using two earlier NESARC surveys combined reported the prevalence of AL offending as 3.6%. A recent review of offender types derived from prospective studies based on self-report and/or official crime statistics yielded wide variation in the overall prevalences of AL (6.7%–16.1%), AO (2.0%–11.3%), and LP (3.7%–13.1%) offenders (Jolliffe et al., 2017b), with variation primarily attributed to differences in offender group definitions, sample selection, and other methodological aspects of the study designs.
The prevalence of AO offenders in this general population survey was 8.4%, exceeding the rates of AL (1.8%) and LP (2.2%) combined. The existence of AO offenders remains controversial in the literature, with some authors viewing AO offending as an artifact of prior offending that has simply gone undetected or not serious to warrant a criminal justice system response (DeLisi & Piquero, 2011; McGee & Farrington, 2010; Wiecko, 2014) or a product of overly strict definitions of adulthood (Sohoni et al., 2014). Recently, DeLisi et al. (2018) have argued that the existence of AO offending has been mixed largely due to the narrow focus on early adulthood (Krohn et al., 2013; Sohoni et al., 2014) and is primarily based on official data lacking triangulation with self-report data (Zara & Farrington, 2010). The results of this study suggest that AO offending may exist and deserves further study as suggested by several authors (DeLisi & Piquero, 2011; Eggleston & Laub, 2002; Sapouna, 2017).
With regard to sociodemographic characteristics, AL, AO, and LP offenders were more likely to be male, Black, or Native American, have lower education and income, but are less likely to be married/cohabitating or Asian/Pacific Islander. Those classified as LP offenders were also more likely than AL, AO, and NO offenders to be never married and of lower socioeconomic status in terms of education and income. These results are consistent with Vaughn et al.’s (2015) study of former juvenile detainees using two earlier NESARC surveys and one long-term prospective cohort study (Bergman & Andershed, 2009). Our findings of lower socioeconomic status among offender groups relative to NOs, and among LP offenders compared with other offender groups, are also consistent with lower educational achievement identified as an early risk factor of AL, AO, and LP offending in many prospective studies (Jolliffe et al., 2017a). Unlike many unmodifiable sociodemographic factors identified here (e.g., male sex), many successful interventions have been designed to address low academic achievement and associated socioeconomic disadvantage, interventions shown to be cost-effective methods of preventing offending or shortening criminal careers regardless of offender type.
The odds of experiencing each ACE prior to the age of 18 were greater among each offender group relative to NOs. The odds of experiencing each ACE were also greater among LP than AO offenders. The odds of experiencing physical abuse, witnessing domestic violence, and other childhood trauma were greater among LP compared with AL offenders, whereas the odds of sexual abuse, physical abuse, emotional neglect, witnessing domestic violence, and other childhood trauma were lower among AO relative to AL offenders. That offender groups experience a greater odds of all ACEs than NOs is consistent with a large body of literature on juvenile and adult offenders (Aebi et al., 2015; Basto-Pereira et al., 2016; Friestad et al., 2014; King et al., 2011; National Center on Addiction and Substance Abuse at Columbia University, 2010). This study further showed that ACEs disproportionately affect LP offenders. Several studies on other early risk factors of offender types (e.g., impulsivity, lack of guilt, low socioeconomic status, witnessing/being a victim of violence, convicted parent, low educational attainment) reported limited evidence on specific risk factors that differentiate AL, AO, and LP offenders (Bergman & Andershed, 2009; Dubow et al., 2014; Pulkkinen et al., 2009). Furthermore, LP offenders were shown to have a greater number of early risk factors than AL offenders, who in turn tended to have a greater number of early risk factors than AO offenders. It appears that, in terms of exposure to adverse childhood trauma examined in this study, LP, AL, and AO offenders may differ more in degree (magnitude) than in kind.
Among offenders, AO and LP offenders had a greater odds of experiencing each substance use, substance use disorder, and mood, anxiety, and PD assessed in this study relative to NOs during their lifetimes even after controlling for sociodemographic factors and ACEs. In contrast, AL offenders had a greater odds of each specific substance use, substance use disorder, persistent depression, and each PD compared with NOs. More importantly, the magnitudes of these associations were consistently greater among LP offenders relative to AL and AO offenders. LP offenders also had a greater odds of experiencing all substance use and substance use disorders, all PDs, and bipolar I disorder than AL and AO offenders, whereas LP offenders had greater odds of panic disorder, social phobia, and GAD compared with AL offenders. Taken together, these results suggest that LP offenders experience more lifetime psychopathology than AO offenders, who in turn experience more psychopathology than AL offenders. These findings are consistent with a review of early risk factors among juveniles that identified alcohol and drug abuse and behavioral problems as risk factors among LP relative to AL offenders (Assink et al., 2015). These findings are also consistent with Beckley et al. (2016) who found that, compared with NOs, AO offenders are more likely to have bipolar I disorder and be dependent on alcohol or other substances. It appears that LP offenders can be differentiated from AL and AO offenders not only in the degree of psychopathology but also in the kind of psychopathology. Although LP offenders had greater rates of substance use, substance use disorders, bipolar I disorder, and each PD assessed in this study relative to AL and AO offenders, LP offenders could be differentiated from AL offenders by greater rates of anxiety disorders (panic disorder, social phobia, and GAD), whereas AO offenders could be differentiated from AL offenders in terms of greater rates of substance use, substance use disorders, bipolar I disorder, and social phobia but lower rates of ASPD.
The finding that LP offenders had greater rates of ASPD than either AL or AO (and NO) offenders suggests that early antisocial behavior may be a stronger predictor of LP offending relative to AL or AO offending. This result is consistent with Moffitt’s (1993) characterization of adolescence-limited antisocial behavior with onset during adolescence that usually stops before adulthood and LP antisocial behavior with onset in childhood persisting into adulthood. Moffitt’s theorizing, however, did not consider all patterns of antisocial behaviors, especially AO offending. Interestingly, the lower odds of ASPD among AO relative to AL and LP offenders suggests that antisocial behaviors may not be initiated until adulthood among AO offenders. As DSM-5 ASPD diagnoses used in this study required evidence of conduct disorder in childhood prior to the age of 15 years and adult antisocial behaviors since the age of 15 years, future research should differentiate between three antisocial syndromes: ASPD (requiring evidence of conduct disorder and adult antisocial behaviors), child conduct disorder (without adult antisocial behaviors), and adult antisocial behaviors (without evidence of conduct disorder). This disaggregation of antisocial syndromes may help differentiate AO, AL, and LP offenders not only in the degree of antisocial behavior, but also in the kind of antisocial behavioral syndromes.
Limitations are noted. Classification of offender groups based on respondents’ self-report of criminal behavioral may have resulted in an underestimation of prevalences and classification of offender groups. Memory of events occurring prior to age 18 (e.g., ACEs, incarceration) may induce recall bias in this study. However, both exposure to ACEs and incarceration prior to age 18 are significant traumatic events not likely to be forgotten. The NESARC-III is a cross-sectional survey and longitudinal survey designs are needed to assess the stability of estimates and associations found in this study over time and the temporal ordering of risk factors and incarceration (e.g., temporality between ACEs and incarceration prior to age 18). Although the NESARC-III and its scope, especially the inclusion of numerous DSM-5 substance abuse and psychiatric disorders, are perhaps unsurpassed, it does not include some important environmental and contextual information that might help further refine offender classifications and allow for differentiating risk factors between them. NESARC-III did not include measures of type of crime and frequency of criminal incarceration, and further research on specific crimes and their intensity is warranted. The NESARC-III sample did not include incarcerated individuals similar to other large epidemiological surveys of the U.S. general population. These limitations are counterbalanced by the strengths of the survey that included its large sample size, rigorous methodology, and generalizability of its results to the U.S. population.
Conclusion
In summary, this study provided important information on the sociodemographic characteristics, experiences with ACEs, and psychopathology across offender types. The results of this study supported further research on AO offending and identified several sociodemographic characteristics (e.g., lower socioeconomic status), experiences with ACEs, and various types of psychopathology that differentiated AO from AL from LP offenders, differences in both degree or magnitude and kind. Further research using the NESARC-III data to explore the heterogeneity of specific types of offenders in terms of sociodemographic characteristics, ACEs, and substance use and psychiatric disorders and other putative risk factors can help inform prevention and intervention strategies designed to prevent offending and shorten criminal careers and elucidate the origins of criminal behaviors. Increasing our understanding of offender types and their risk factor profiles using large epidemiological surveys of the U.S. population holds great promise in generating refined hypotheses to address an array of questions relating to criminal populations, especially those relating to validation of existing and identifying new prototypes of offenders. Importantly, the NESARC-III included the collection of DNA information on a large subsample of the survey, substantially increasing its value in terms of genetic variants and their environmental interactions with the rich phenotypic data relating to offender type and their risk profiles.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Disclaimer
The views and opinions expressed in this article are those of the authors and should not be construed to represent views of the sponsoring organizations or the US government.