
Abstract
While physical health can impact a variety of outcomes, little research has looked at health and delinquency. Through a lens of GST, this study examines whether health moderates the relationships between strain and delinquency and drug use. Data from the 2011 NSDUH were analyzed; results indicated that, for certain strains, very good and excellent health predicted lower risks of committing some types of delinquency and poor/fair health predicted the higher risk. For youth in “no parent” homes in very good health and from some youth with chronic illness, however, the risk of delinquency increased. The overall results dictate the expansion of health programming and the complex findings suggest increased research on the nexus of health and delinquency.
Physical health can impact a variety of outcomes from birth through adulthood (Centers for Disease Control and Prevention [CDC], 2020). For example, health in childhood is now thought to play a role in adult socioeconomic status (Palloni et al., 2009). Further highlighting the importance of health are current issues of socioeconomic and racial health disparities in the United States. Indeed, poverty is strongly tied to a host of health problems (Council on Community Pediatrics [CCP], 2016). Moreover, research indicates that health status tends to be best for non-Hispanic Whites and Asians and worst for Blacks and Native Americans (Lariscy et al., 2020). Unfortunately for many children, the only way they may come into contact with a health care provider is through contact with the justice system (Golzari et al., 2006; Hammett et al., 1998). Indeed, low income and minority children are more likely to be in this justice-involved group (Sickmund & Puzzanchera, 2014). While much health research focuses on health as an outcome variable, a few studies have discovered that health is a predictor of behavioral issues (Woods et al., 2013) and can impact interpersonal relationships (Larsen, 2019). Given the health disparities mentioned above, the connection between health and behavior, and the documented disproportionate minority contact with the justice system, the nexus of health and deviant behavior warrants much more research.
Literature Review
Human beings develop rapidly during childhood (Robinson et al., 2017) and poor health in the form of improper nutrition, chronic stress, and exposure to toxins and infections can impact the development of the young brain (American Academy of Pediatrics [AAP], 2014; CDC, 2020). As such, it is not unreasonable to suggest that poor health could influence youth behaviors in a negative way, and indeed, research does provide some support for this (Gortmaker et al., 1990; Woods et al., 2013). However, research regarding health and delinquency has been sparse and often looks at health as an outcome variable (see Junger et al., 2001). This paper posits that health is a moderating variable, with poor health acting to erode a youth’s ability to cope with strain and strong health bolstering coping ability.
General strain theory (GST) claims that negative relationships pressure adolescents into deviant behavior by creating “negative affective states” (Agnew, 1992). These negative relationships include parental fighting, parental rejection, neighborhood and work problems, working in the secondary labor market, and poor school performance (Agnew, 2001, 2006). Other sources of strain, such as the inability to obtain educational goals and unpopularity with peers, have received mixed empirical support (Agnew, 2001). According to GST, negative relationships can produce strain by preventing youth from achieving desired goals or by presenting youth with “noxious stimuli.” Strain then leads to “negative affective states” such as anger or depression. When a youth experiences a negative affective state, they can cope in a variety of ways to reduce their strain.
According to Agnew (1992), there are three types of coping strategies: cognitive, behavioral, and emotional. How a juvenile copes with strain depends upon a variety of individual constraints, including coping skills, social controls, and life circumstances (Agnew, 2001). Juveniles who do not have access to legitimate coping strategies will resort to deviant coping strategies. Deviant cognitive strategies would involve denial; deviant behavioral strategies include verbally or physically attacking the source of the strain (or a proxy). Indeed, anger and similar emotions are thought to be most closely tied to deviance (Agnew, 1992), and aggression can be a response to anger (Bushman, 2002; Parrott & Peterson, 2008; Parrott & Zeichner, 2002). Another example of illegitimate behavioral coping is stealing, particularly when the strain is an economic one (Agnew, 2001). Deviant emotional coping with a negative affective state includes avoidant strategies such as the use of illicit drugs to escape the negative emotions (Agnew, 1992).
Agnew and White (1992) discuss the difficulties of categorizing variables into strain or into constraint variables; their rule of thumb is that strain variables are those that clearly involve negative relations with others. Strains cause the adolescent to be treated adversely (such as being insulted, embarrassed, or fail to achieve a goal) or to feel negative emotions due to others (Agnew & White, 1992, p. 481). While Agnew and White placed “serious illness or injury” into the strain category, this paper argues health is not a source of negative relations but is better categorized as an individual factor that influences how one responds to strain. “Individual coping resources” affect one’s ability to engage in the three types of coping strategies; those with fewer resources are constrained to delinquent coping strategies and thus have a higher risk of delinquency (Agnew, 1992, p. 71). Poor health falls into the individual coping resources category because, as stated by Shepard and Franklin, poor health can aggravate stress by causing coping mechanisms to deteriorate (as cited in Larsen, 2019) resulting in those with poor health being more likely to engage in deviant responses to strain. Research suggests that poor health impairs cognition, reduces emotional well-being (Larsen, 2019; Woods et al. 2013), and is related to behavior problems (indicated in prior research), supporting an assertion that poor health constrains the available cognitive, behavioral, and emotional coping strategies.
Prior Research
One compelling argument for a relationship between health and delinquency is the high rates of health problems in the juvenile justice population. Physical health problems are overrepresented in this group (Golzari et al., 2006; Sedlak & McPherson, 2010). For instance, in their review of health surveys of youth in detention facilities, Golzari et al. (2006) found that the prevalence of “any” medical condition was 46% to 70%.
An alternative explanation for the overrepresentation of health problems in delinquent youth is poverty. Living in poverty is a significant source of stress as those in poverty are more likely to experience substandard housing, noise, family turmoil, work problems, and community violence than are middle class persons (Evans & English, 2002). The higher degree of stress in these communities is thought to contribute to poor health outcomes (Kaplan et al., 2013) such as “birth weight, infant mortality, language development, chronic illness, environmental exposure, nutrition, and injury” (CCP, 2016, p. 1). Not only does it impact health, but poverty is also related to delinquency (Jaggers et al., 2015; Jarjoura et al., 2002; Sampson & Laub, 2005).
However, prior research would suggest that this factor is not a sufficient explanation for the delinquency-health relationship. First, one study found that the stress from living in poverty resulted in increased difficulty with self-regulatory behavior (Evans & English, 2002), fitting with GST’s assertion that negative relationships (family turmoil and community violence from living in poverty) lead to strain (stress) and poor coping skills can lead to deviance (difficulty with self-regulatory behavior). Second, while poverty and food insecurity (a component of health) are correlated, Kimbro and Denney (2015) were able to find a relationship between food insecurity and behavior with a sample of subjects in poverty, effectively controlling for poverty. Most importantly, prior empirical research on health and delinquency has found a relationship even while controlling for socioeconomic variables (Gortmaker et al., 1990; Junger et al., 2001).
In addition, a small body of research has found that addressing physical health needs predicts reductions in recidivism. For example, Berman (1989) studied the relationship between vision problems, vision training, and delinquency; results indicated a reduction in delinquency for those who had gone through the program. Moreover, Sheu et al. (2002) found that continuity of care with a medical provider was related to a decreased likelihood of incarceration among a cohort of HIV+ females. Similarly, Kim et al. (1997) studied a prison release program for women which connected them with medical care, financial assistance, and substance abuse treatment; their results indicated significant reductions in recidivism for program participants. Finally, Hancock (2017) studied juvenile facilities in Florida and found that physical health care services were inversely related to facility recidivism. She proposed that addressing the physical health needs may allow youth to better cope with strain, engage in treatment, and deal with interpersonal issues (Hancock, 2017) which is in line with general strain theory.
Viewing prior research on health and behavior through GST, it is hypothesized that health moderates the relationship between strain and delinquent behavior. As stated, weak health has been found to be related to aggression and poor interpersonal relations, supporting an assertion that weak health may erode one’s ability to cope with anger and similar emotions. Therefore, it is believed that weak health will increase the risk of aggressive or avoidant deviance while strong health will reduce this risk. Because it is an economic strain, poverty and poor health will result in greater risk of committing property crimes.
Method
This study used data from the National Survey on Drug Use and Health (NSDUH) conducted in 2011 by the Substance Abuse and Mental Health Services Administration (SAMHSA). The NSDUH sample consists of non-institutionalized civilians over the age of 12 from all 50 states in the U.S. and DC. Using multistage probability sampling with stratification, NSDUH researchers created a national sample, oversampling from the eight most populous states, and also oversampling youths and young adults in order to equally represent the following three groups: 12 to 17 years old, 18 to 25 years old, and those over 26. 1
The computer-assisted survey was administered by about 700 field staff and consisted of both questionnaire and interview portions. Interviews were conducted using computer-assisted personal interviewing software, with sensitive questions being administered via audio computer-assisted self-interview software (RTI International, 2014). Questions covered topics such as drug use, delinquency, mental health, health care, social environment, and demographics. For questions involving things like family income, proxies answered on behalf of the younger respondents. In 2011, the NSDUH was administered to 70,109 persons (RTI International, 2014). The current study used only the data from the subjects who were 12 to 17 years old (19,264) and who attended a school that used a traditional letter grading system, 2 resulting in sample size of 18,877.
Variables
Health measures
This research will use two measures of health: overall health and chronic illnesses. Prior research has commonly used a self-assessment measure of overall health from youth (see Junger et al., 2001; Wade & Pevalin, 2005). Junger et al. (2001) point out that such health measures are predictive of long-term mortality; such measures are typically highly correlated with clinical assessments (Garrity et al., 1978). These measures ask respondents to answer about their health on a scale, typically ranging from “excellent” or “very good” to “poor.” Similarly, the NSDUH asked respondents to rate their general health on a 5-point scale ranging from “excellent” to “poor.” In addition, prior studies have also measure health through chronic illnesses (see Gortmaker et al., 1990; Junger et al., 2001; Woods et al., 2013); chronic illnesses have a longer duration and thus may have a special impact. The NSDUH asked respondents to indicate with which of 19 illnesses respondents had ever been diagnosed by a doctor or other medical professional. 3 This variable was measured as a scale variable and is substantively different from the overall health variable in that it requires a diagnosis from a medical professional, making it a less subjective measure. 4
Strain measures
While Agnew originally argued that strain was cumulative and should be measured as such, he later asserted that some strains might contribute to delinquency and some would not; he reasoned that the use of cumulative measures of strain in prior research may be why strain measures had achieved modest results (Agnew, 2001). Thus, this study will use five measures of strain related to the main ones identified in the literature review: poverty, two measures of parental relations, and two measures of school relations.
Poverty
Poverty was used as a proxy for the strains of poor physical and economic neighborhood conditions; indeed, as already stated, living in poverty is associated with a high degree of stress and a greater likelihood of neighborhood and work problems. Poverty was measured in the NSDUH using U.S. Census Bureau assignments based upon income, family size, and number of children in the family. Respondents were placed into one of three categories: living in poverty, income up to two times the federal poverty line (FPL), and income greater than two times FPL.
Parental relations
Parental relations were measured in two ways-the parents in the home and parental involvement. The absence of one or more parents is a strain on parental relations, so two parents was the reference. Parental involvement was measured through a series of questions about respondents’ relations with their parents in the past 12 months that they rated as “always,” “sometimes,” “seldom,” or “never.” These questions asked about whether their parents checked if they had done their homework, helped with homework, let the respondent know they had done a good job, let the respondent know they were proud of something they had done, made them do chores, limited television time, or limited time out with friends. Principle component analysis (PCA) (KMO = 0.718; significant Bartlett’s) indicated the first four variables be retained as their own factor (loadings 0.68 and above) 5 ; in addition, reliability analysis indicated a Cronbach’s alpha (CA) of 0.776 and that removal of any of the items would decrease the CA, suggesting a measure with strong internal consistency. These four responses were combined using the mean to create a single score for parental involvement. 6
School relations
School attitudes were used as one measure of relations with school. This measure utilized a series of question in the NSDUH regarding the respondents’ attitudes toward school and experience with teachers. PCA (KMO = 0.809; significant Bartlett’s) indicated a single factor be retained with all the variables (loadings 0.603 and above; CA = 0.769 with no increase by removing items). The mean of the responses was used to create a single school attitudes score. Similar to prior research, school performance was measured by asking respondents to report their grade average.
Delinquent measures
The NSDUH asked respondents to self-report whether they had engaged in various delinquent behaviors within the past 12 months using categorical scales ranging from “0 times” to “10 or more times.” Due to relatively low numbers engaging in the delinquency, the goal of assessing risk of delinquency, and prior strain research that used logistic regression, the variables were coded dichotomously. Included behaviors were attacking someone with the intent to seriously hurt them, engaging in a fight where a group had found against another group, getting into a fight at work or school, and stealing or trying to steal something worth more than $50. To measure substance use, one type of measure from the NSDUH was used: substance use in the past year. Substances included alcohol, marijuana, pain reliever not prescribed, or “hard drugs” (one or more of: cocaine, crack, heroin, ecstasy, LSD, methamphetamine, LSD, and/or PCP).
Other constraint variables
Risk taking behavior and peer drug use were included as constraints that could impact the coping mechanisms available to an adolescent. Youth with a greater proclivity for risk taking behavior may be less constrained from the use of risky deviant behavior. The NSDUH asked three questions about the propensity for risky behavior and seat belt usage and the mean of these responses were used to create a score for risk taking behavior. PCA (KMO = 0.518; significant Bartlett’s) indicated a single factor be retained with all the variables; however, the seat belt variable had a low loading (−0.323) and was conceptually different from the others so was removed; the remaining two were combined (loadings 0.9 and above; CA = 0.81). As above, the mean was used to create a single riskiness score.
Agnew and White (1992) included a measure of peer delinquency as a proxy for delinquent beliefs; they note that youth beliefs are usually consistent with that of their friends. The NSDUH asked questions about how many peers used alcohol, marijuana, cigarettes, or got drunk weekly; a measure of peer substance use was created to use in the substance use analyses. PCA (KMO = 0.835; significant Bartlett’s) indicated a single factor be retained with all the variables (loadings 0.835 and above; CA = 0.884 and no increase by removing items). The mean of the responses was used to create a peer substance use score.
Confounding variables
Age, gender, and race were included in the analysis. In addition, as mental health issues are predictive of delinquency (Barrett et al., 2013), a dichotomous measure of mental health was included: the presence of a major depressive episode (MDE) in the past 12 months. The NSDUH classified whether respondents had major depressive episodes by asking a series of adolescent appropriate questions relating to mood.
Analyses
Because the hypothesis regards risk of delinquency and drug use and dependence, moderation analyses were done through a series of logistic regression analyses. While tradition has dictated that moderating terms be mean centered, more recently it has become clear that mean centering is not necessary (Echambadi & Hess, 2007; Hayes, 2018; Iacobucci et al., 2017), impacts interpretation rather than tests of significance (Hayes, 2018) and yields results that are functionally equivalent to non-mean centered models (Kromrey & Foster-Johnson, 1998). Thus, variables in these analyses were not mean centered; results must be interpreted accordingly.
Analyses were done using PROCESS 3.5 developed by Hayes for use with SPSS to conduct moderation analyses. Each of the eight outcome variables (four delinquency and four drug use) were regressed 10 times-five times with overall health moderating each strain variable and five times with chronic illnesses moderating each strain variable. Constraint, confounding, and other strain variables were included in each model (only drug models included the drug using peers variable). The significant moderations were probed using the pick-a-point method for the overall health models as suits categorical moderators (Hayes, 2018). Pick-a-point was used for chronic illnesses as well using the 16th and 84th percentiles; standard deviations were not used as these values fell outside the realm of possible values for chronic illnesses and using such values is not recommended (Hayes, 2018). In addition, the Johnson-Neyman (JN) technique (inappropriate for categorical moderators and predictors (Hayes, 2018)) was used to probe the interactions between chronic illnesses and the continuous strain variables.
Results
Descriptive analyses indicated that gender and age for the 18,771 respondents were fairly equally distributed (51% male, 31% 12–13, 33% 14–15, 35% 16–17). The racial breakdown of the sample was 58.4% White, 18.2% Hispanic, and 13.7% Black. Only about 8% of respondents reported having symptoms in the past year that were consistent with MDE.
Table 1 is a breakdown of the constraint, strain, and outcome variables. Most of the youth in the sample seem to have been in good health. For example, nearly three-quarters had never been diagnosed with a chronic illness (mean = 0.34). Only about 4% reported their health to be either fair or poor and only 5% reported having been diagnosed with two or more chronic illnesses. Regarding risk taking and peer drug use, youth generally reported being more risk averse and were more likely to report having few peers who used substances.
Constraint, Strain, and Outcome Variables.
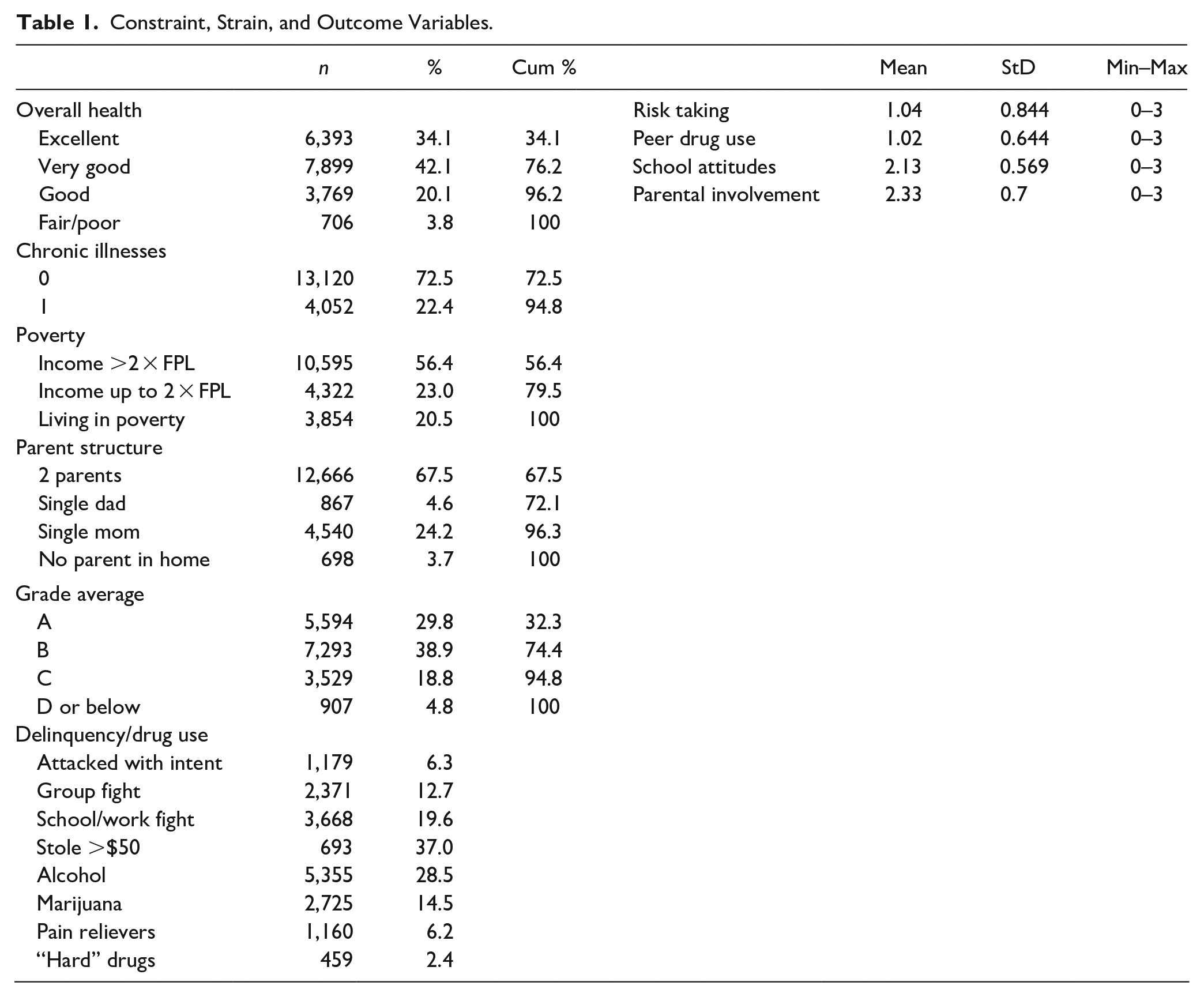
With regard to strain, about one in five subjects were living in poverty at the time of the survey. About two-thirds of the youth lived in two parent homes and youth tended to report higher levels of parental involvement. About 95% of respondents reported have a C average or better with a B average being the most common response. It is not surprising, then, that sample youth tended to report fairly positive attitudes toward school. Finally, given the low level of negative constraints and strains, it is not unexpected that the vast majority of the 18,877 youth in the sample reported no deviance in the past year. The most common deviant act reported in Table 1 was getting in a fight at school or work and the least common was stealing something worth more than $50. The most common substance used was alcohol, with just over a quarter having used alcohol in the past year, followed by marijuana. 7
Multivariate Analyses
Of the 40 health logistic regression models and the 40 chronic illness models (all statistically significant at the p < .001 level), five of the health models and four of the chronic illness models had significant moderations. These nine models explained at the lowest 4% to 15% of the variance and at the highest 25.5% to 36%. The variables that were significant in the most models were the confounding variables-age, gender, race, and major depressive episodes. Health by itself was significant in two models-those of work/school fighting regressed on parental involvement and regressed on parent structure. Surprisingly, good health (β = 0.39, p < .05), very good health (β = 0.66, p < 0.05) and excellent health (β = 0.71, p < .05) predicted a higher likelihood of reporting a work/school fight. Chronic illness by itself was only a significant predictor in one of the four models-that testing the relationship between parental involvement on alcohol use (β = 0.198, p < .001); more illnesses predicted greater risk of alcohol use.
Moderating relationships
Overall health
The analyses indicated five moderating relationships between overall health and strain for further exploration. These interactions were probed using the pick-a-point technique; the results can be found in Table 2.
Significant Moderating Relationships for Health.

p < .05. **p < .01. ***p < .001.
The second column in Table 2 shows the results of the chi square analyses testing the interaction between health and the strain variable. As indicated, health had at least one moderating relationship with all delinquency variables except for group fighting but had little moderating effect with regard to substance use. Health moderates the relationships between poverty and attacking with intent to harm and alcohol use. Youth in very good or excellent health in the highest income group had the lowest probabilities of having attacked somebody with intent; the same was true for youth in very good health in the middle-income group. Youth in the middle-income group with poor/fair health were more likely to report alcohol use, but those in very good health were less likely to report alcohol use. These relationships are also illustrated in Figure 1, which shows the changes in probability of attacking and probability of alcohol use as a function of poverty and defined by health.
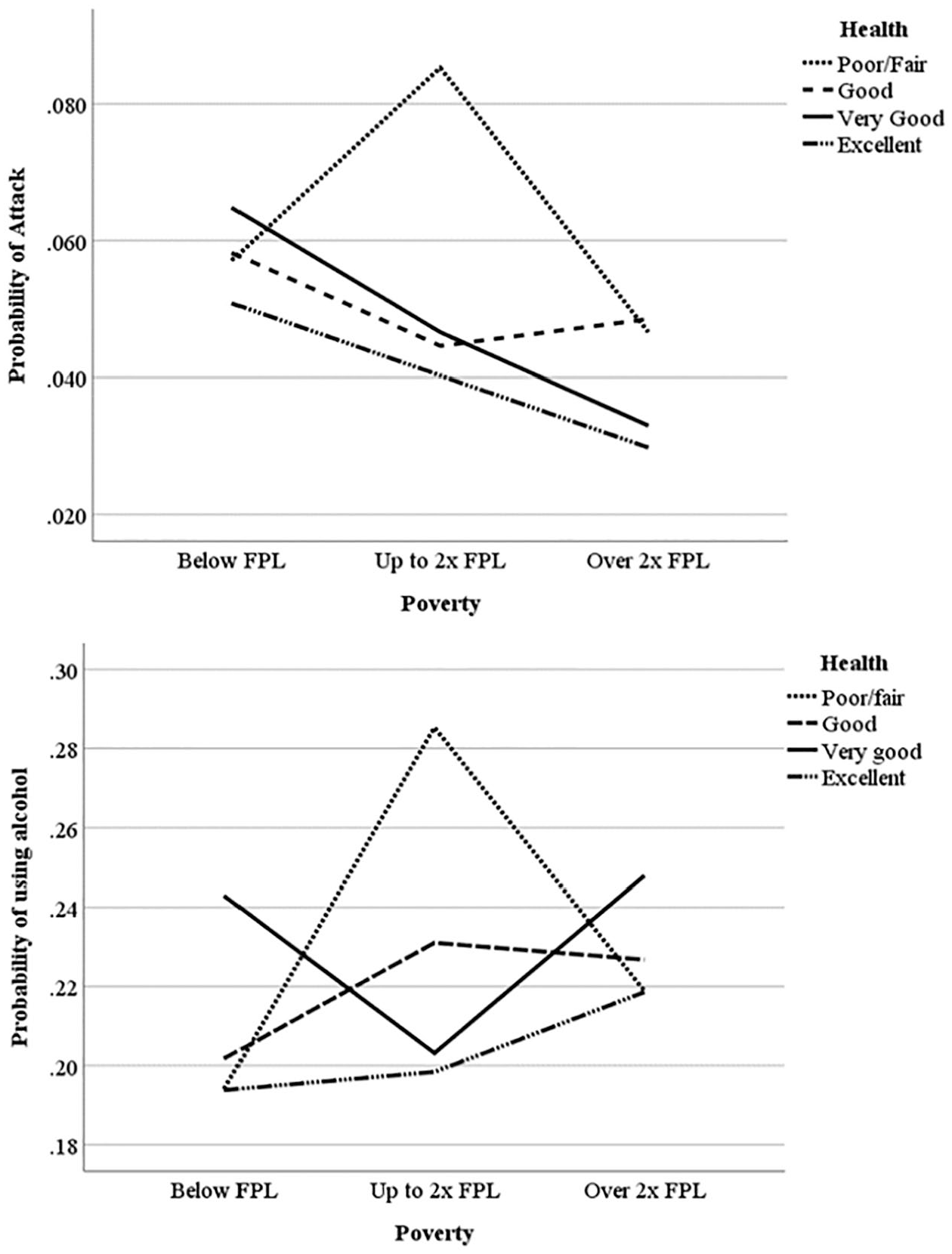
Probability of attack and probability of using alcohol by poverty.
Table 2 also suggests that health moderates the relationship between parent factors and work/school fighting. Health was an important variable for those in single mom or no parent homes. While good health was not significant, youth in single mom or no parent homes who were in poor/fair health, very good, or excellent health had a higher likelihood of reporting work/school fighting as compared to two parent homes, with those in no parent homes in very good health having the highest likelihood. For youth in very good or excellent health, their probability of reporting a work/school fight dropped as parental involvement increased. Interestingly, while not significant, those in poor/fair health showed greater risk of work/school fighting as parental involvement increased. These relationships are graphed in Figure 2.
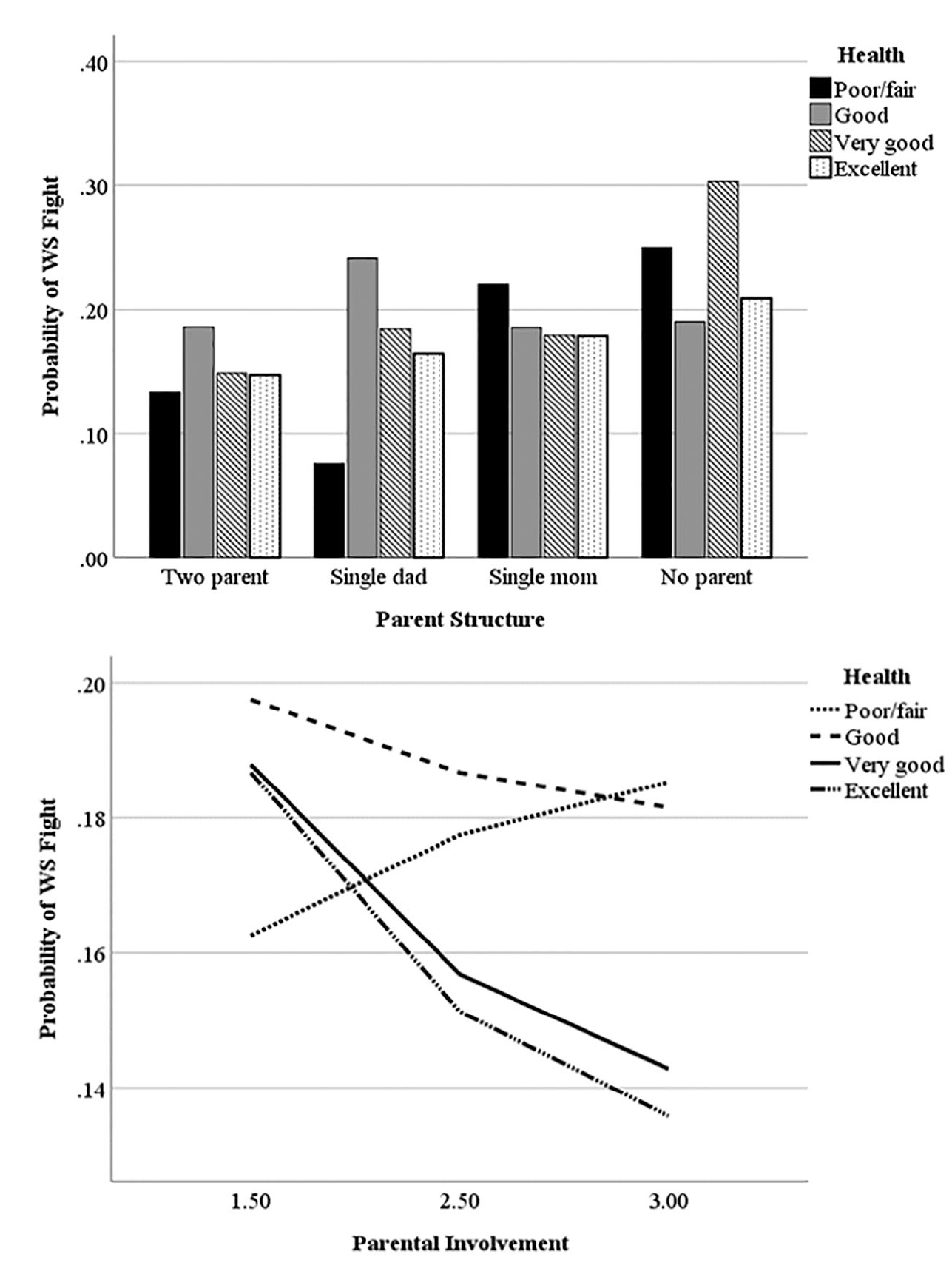
Probability of work/school fighting by parent strains.
Finally, Table 2 shows that health moderates the relationship between health and grades; those with good health and higher grades are less likely to report stealing. This relationship can be seen in Figure 3-the bars for very good and excellent health clearly descend from left to right; that of good health is fairly flat and that of poor/fair health is bimodal.
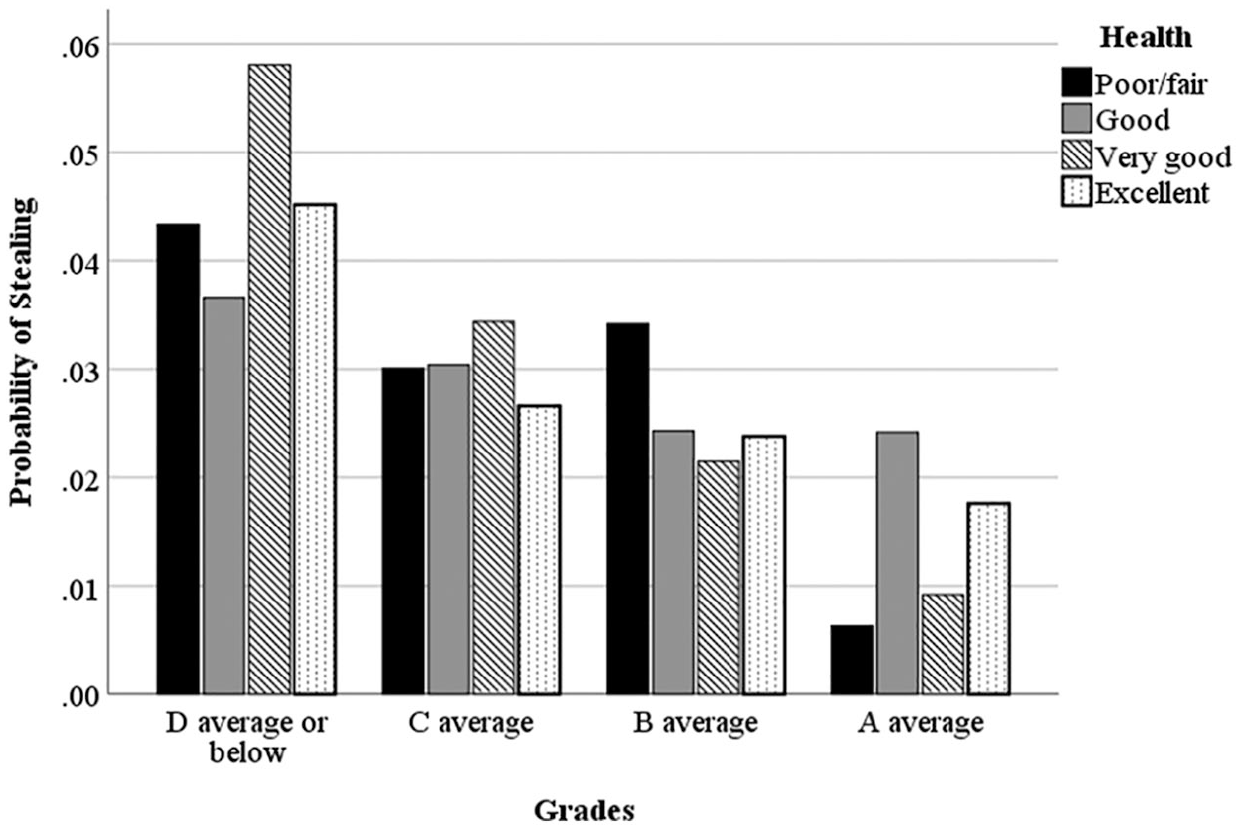
Probability of stealing something worth more than $50 by grades.
Chronic illness
The four moderating relationships were probed using the pick-a-point and JN techniques; the results can be found in Table 3. A higher p-value (0.1) was used for parent structure on work/school fighting and grades on stealing because those relationships were also identified with health and so allowed for comparison; the lower value was used with parental involvement on alcohol use as health also impacted alcohol use.
Significant Moderating Relationships for Chronic Illnesses.
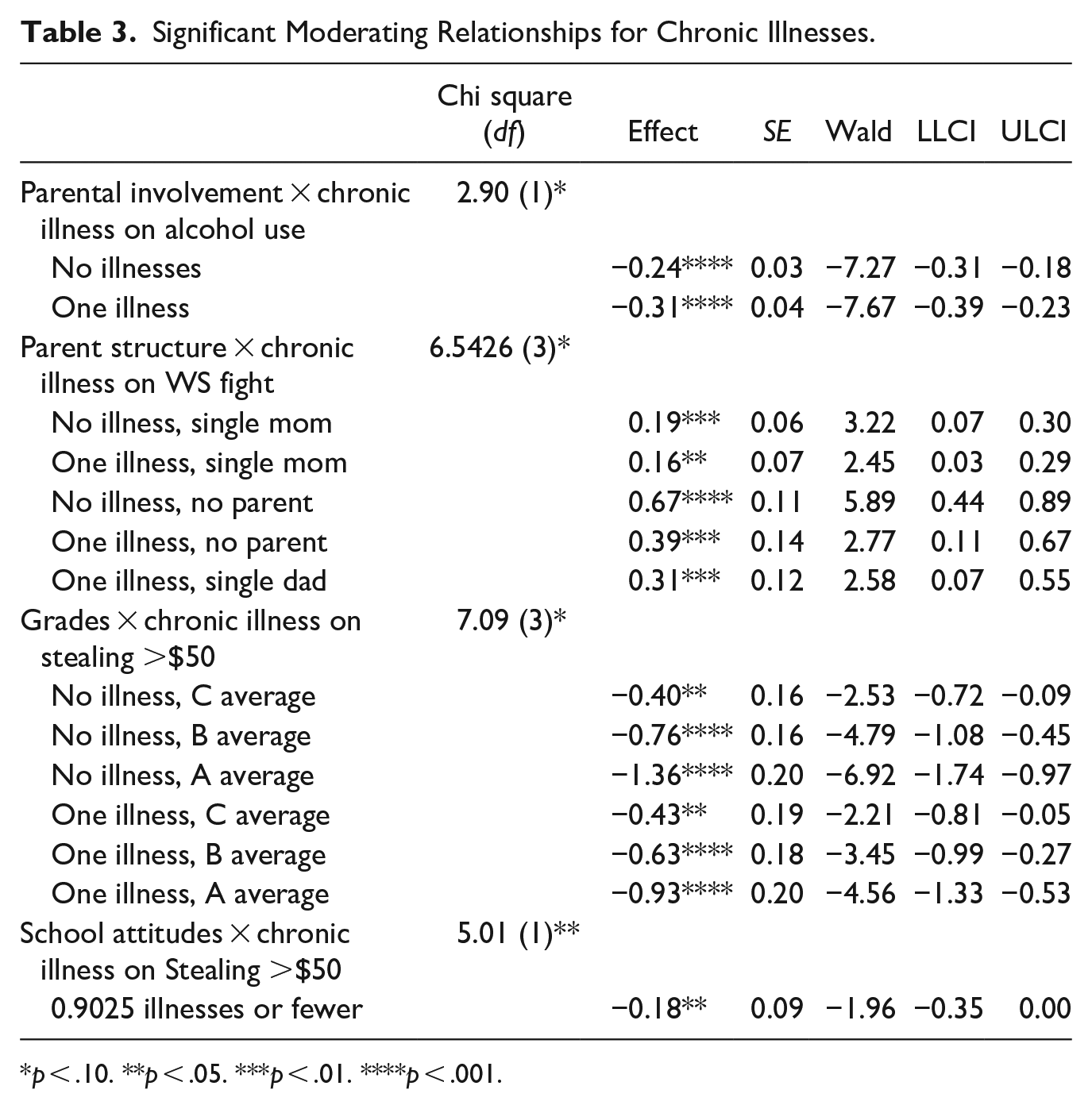
p < .10. **p < .05. ***p < .01. ****p < .001.
Because the JN technique did not find any statistically significant transition points, the pick-a-point method was used with chronic illness and parental involvement. As shown in Table 3, while youth with no diagnosed chronic illnesses (which is the vast majority of the sample) showed a decrease in alcohol use as parental involvement increased, this decrease was much steeper for those with one chronic illness (the next most common number, see Table 1). This relationship is graphed in Figure 4.
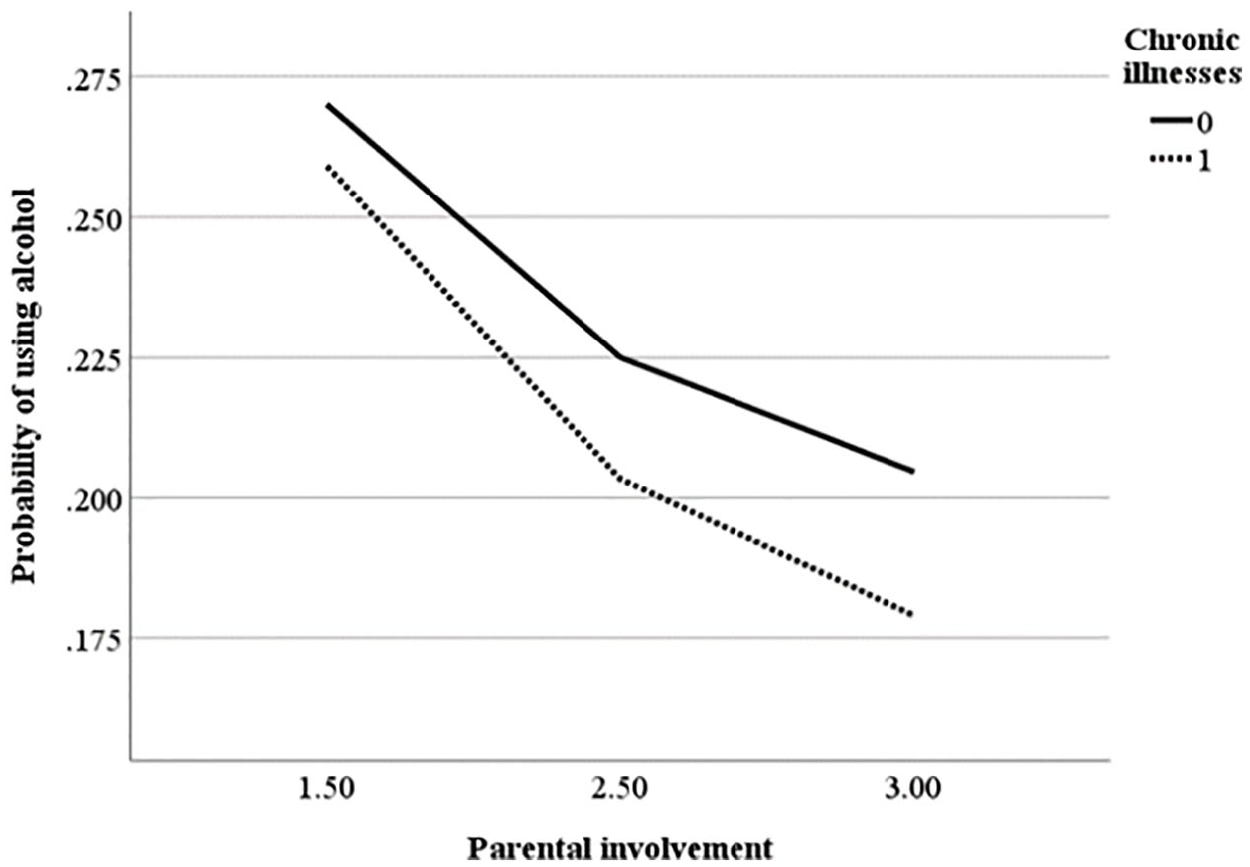
Probability of using alcohol by parental involvement.
As with health, chronic illnesses were important for youth in single mom and no parent homes. What is interesting is that these results somewhat go against what was found for health; youth with a chronic illness were more likely to report work/school fighting. What is also different here is that living in a single dad home and having a chronic illness was statistically significant and predicted a higher likelihood of work/school fighting. As with health, the no parent group had the highest rates of fighting. These relationships are shown in Figure 5.
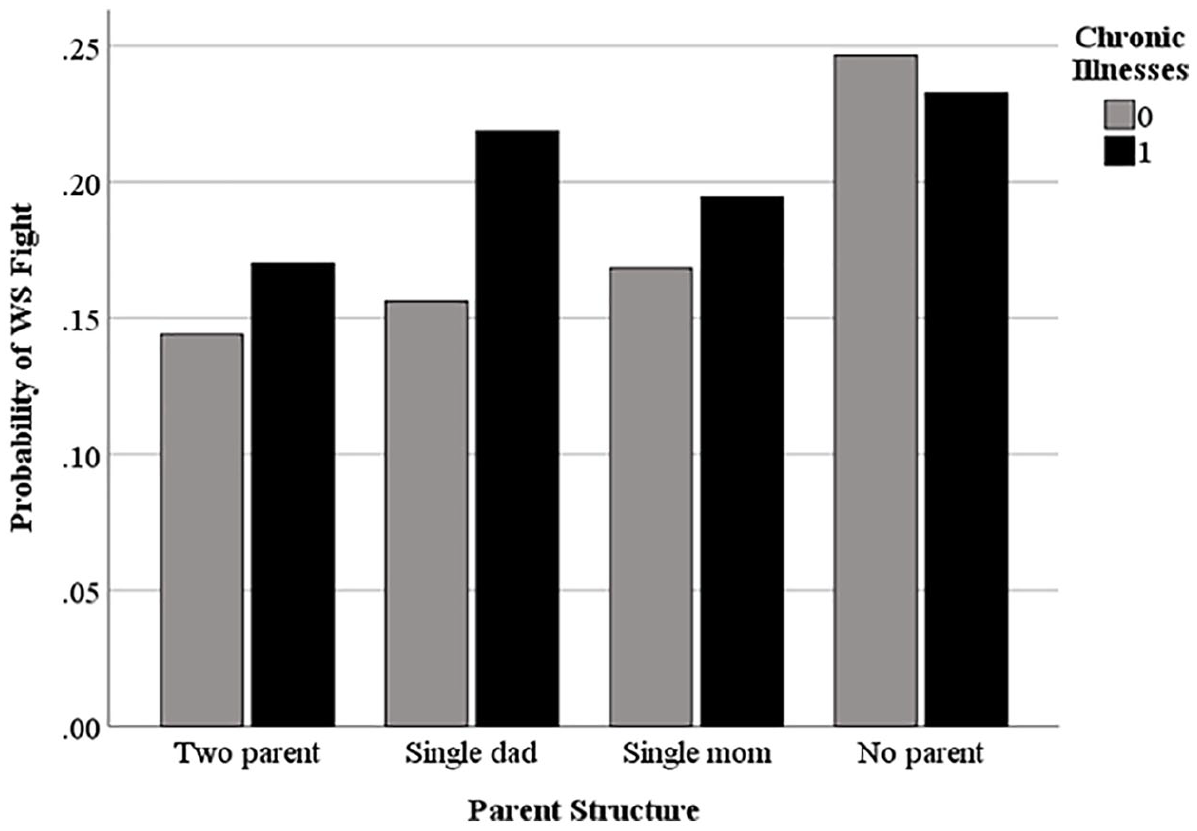
Probability of work/school fighting by parent structure.
Finally, chronic illnesses were important when it came to school variables and stealing. For school attitudes, the JN technique indicated the effect of chronic illness was only significant for those who had fewer than 0.9 illnesses. This suggests school attitudes impact the likelihood of stealing only for those students with no diagnosed chronic illnesses. The probability of stealing declines steadily as grades increase for both youth with no illnesses and with one illness; this decline is more dramatic for those with no illnesses, however. Chronic illness’s moderating effect on how these school strains influence the probability of stealing is graphed in Figure 6.
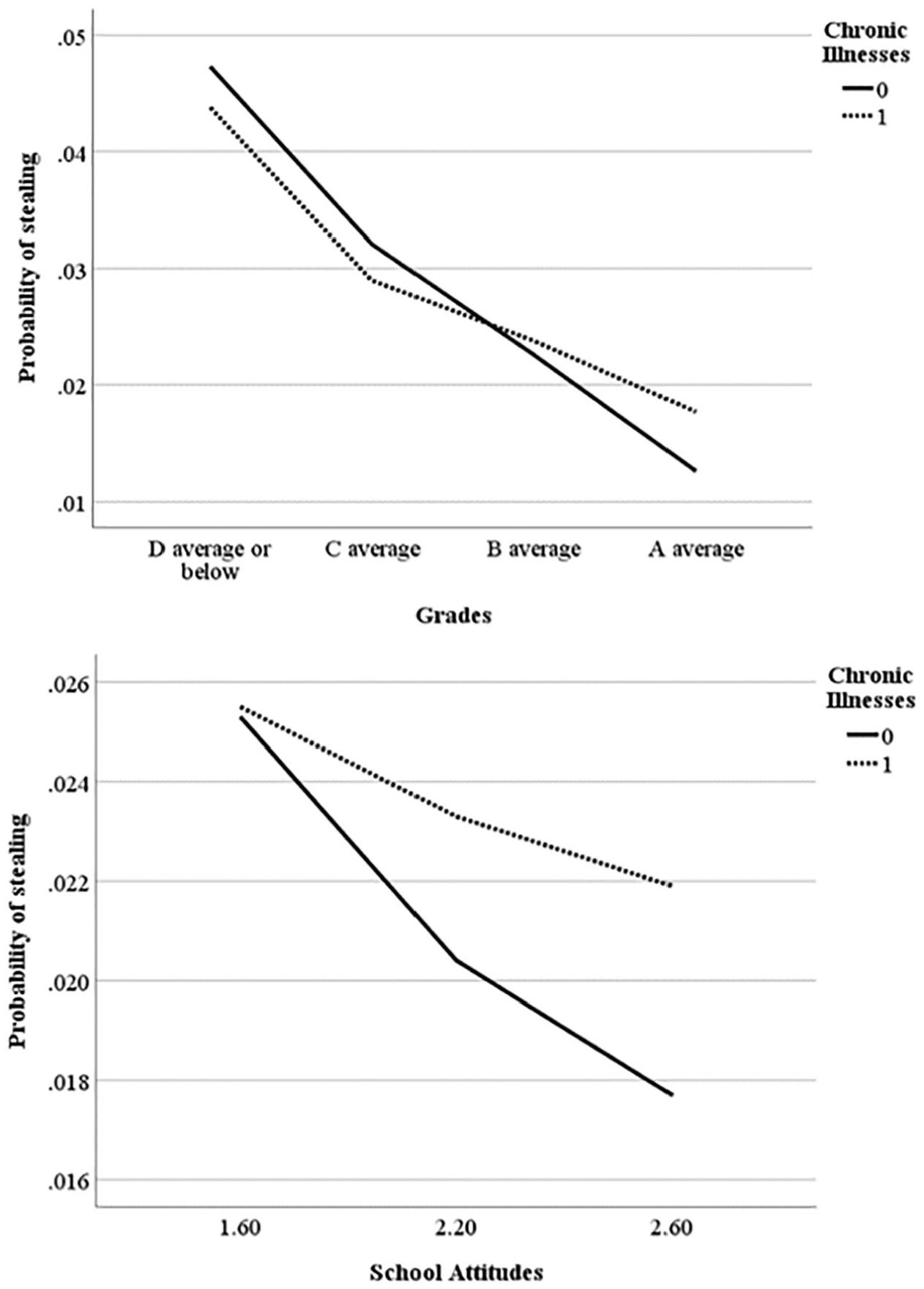
Probability of stealing by grades and school attitudes.
Discussion
The hypotheses were only partially supported. Weaker health did increase the risk of delinquency for a few types of strain. This was contradicted by (1) youth with no illnesses being more likely to use alcohol across the spectrum of parental involvement, (2) “no parent” youth with an illness who were less likely to fight and (3) students with an illness and a C average who were less likely to steal. However, those were the only relationships where weaker health significantly predicted less offending, all measured by chronic illness. “Good” health, the moderate health status, never emerged as significant. Conversely, very good and excellent health appear repeatedly in the analyses as significant, more often than did poor/fair health, and mostly in the expected direction (outside the no parent youth). In addition, chronic health only matters with regard to school attitudes and stealing if there is no chronic illness. Thus, viewing strong health as an individual protective factor for one’s coping skills may be a more accurate conceptualization than viewing poor health as a risk factor that erodes coping skills.
Another explanation for the few differences in the health and chronic illness models likely reflect underlying differences in what they are measuring and the social factors involved. The health measure is a self-assessment, and while used in prior research and highly correlated with clinical measures (including in this study), is a more subjective measure than that of chronic illness, which requires an official medical diagnosis. Self-assessments are influenced by a number of factors, including age, sex, socioeconomic status, employment status, stress, recent life changes, health history, and psychological health (Garrity et al., 1978). The assessment of one’s own health may even be wrapped up in one’s identity (“I’m a healthy person”). Indeed, the interactions with chronic illness were more straightforward than those with the more subjective health measure.
Further complicating these measures are issues of access to medical care-in order to be officially diagnosed with a chronic illness, youth need to have first visited a doctor, and that doctor needs to have diagnosed them. As stated already, many youth do not have access to medical care until they are brought into the justice system. If they do see a doctor, many may go undiagnosed. Indeed, prior research indicates that minorities and Whites are likely to receive different treatment with regard to diagnoses and therapeutic recommendations (Geiger, 2003). As such, there are surely youth in the sample with undiagnosed chronic illnesses; the youth with less access to health care and thus less likely to get diagnoses are those in the lower income groups who are also most likely to report more delinquency. Access to health care thus might explain the few odd results for chronic illness.
Relatedly, one interesting result was that those with poor/fair health had a spike in their likelihood of using alcohol and (though not significant) for probability of attack; these spikes occurred in “up to 2× FPL” group rather than the poverty group. The FPL (or percentages above it, such as 125 or 150) is used to determine eligibility for a variety of benefits, such as food stamps or Medicaid (O’Brien & Pedulla, 2010). A possibility is that some from the middle-income group may be youth from families that could use services but are not eligible due to having too large an income to receive benefits. Indeed, poverty thresholds have been criticized for decades as not accounting for factors such as transportation, housing, and the geographic differences in cost of living (O’Brien & Pedulla, 2010). Perhaps the youth in the “below FPL” group are getting extra help that the youth in middle income group do not get; as such, the middle-income youth may be experiencing more strain than the poverty group (or getting less assistance in coping with strain).
Health did not moderate the relationship between poverty and stealing, as predicted by GST, although $50 is admittedly a relatively high minimum value. That being said, the results did imply a relationship between health and school relations. Health moderated the relationships between school factors and stealing-health and chronic illness both moderated grades and stealing and chronic illness moderated school attitudes and stealing. In fact, school may represent youths’ primary opportunity for stealing, so their relations with school, moderated by health, naturally might influence their decision to steal. Better attitudes, higher grades, and healthier youth were less likely to steal things worth more than $50, again suggesting strong health is a protective factor rather than weak health being a risk factor. Youth with strong health may be able to more effectively engage with academic programming and thus have more positive attitudes toward school, reducing their likelihood of misbehavior.
The parent structure models indicated some complicated results. Youth in single mom homes (with strain on the dad relationship), were most likely to fight when in poor health. As single mom homes are likely to have lower incomes (Damaske et al., 2016), there may be strains tied up in this status that aren’t present in the single dad group. That being said, in the chronic illness model, the single dad youth with an illness were some of the most likely to fight. Those in no parent homes (with strains on both parent relationships) were also more likely to fight when in poor health, but were most likely to fight in very good health. This carried over to the chronic illness model, where those in no parent homes were more likely to fight with no illness. These relationships suggest the complexity behind parent relationships and health. Indeed, research suggests that the effect of parental absence on youth is dependent upon the reason for the absence (e.g., death, divorce, abandonment, etc.) (Fritsch & Burkhead, 1981), the amount of contact with the “absent” parent, and discipline of the remaining guardian (Trice & Brewster, 2004). Family structures and health deserve more research to tease these factors out.
As noted, there were a number of outcomes for which health did not moderate, namely group fighting and most substance use. There are two possible explanations. First, group fighting and, at least to some extent, substance use are group activities. It may be that health is a coping resource for individual activities, such as individual attacks, fighting, and stealing, but these skills succumb to other factors like peer pressure when it comes to group activities. Another explanation involves prescription drugs not prescribed-while youth may self-medicate with alcohol (Klee & Reid, 1998), youth who are sick may have drugs prescribed and so may not feel the need to misuse prescriptions. Although less likely, they may also fear drug interactions.
The main implication of these findings is to increase health programming, including a reconsideration of the cutoffs for public assistance, as has been noted for some decades (O’Brien & Pedulla, 2010). An increase in programming may also indirectly benefit single mom homes where stronger health had lower likelihood of deviance than poor/fair health. Health programming should include not only direct services but also education as to how youth and guardians can take care of youths’ health. Improving the overall health of the general youth population strengthens this protective factor, thus potentially reducing deviant behavior by improving youths’ ability to cope with inevitable strain.
Moreover, health programs should receive more funding in the school setting, both strengthening the health protective factor and also potentially improving school attitudes (i.e., reducing school strain). Offering quality health programs in school settings would also make it easier to provide care to youth regardless of income and minority status due to schools’ access to students. In fact, school-based health centers have been shown to increase healthcare service access and utilization (Anyon et al., 2013) as well as school engagement, satisfaction (Strolin-Goltzman et al., 2012), and performance (Strolin-Goltzman et al., 2014). It is also imperative to improve the health care services within the juvenile justice system; despite this being a primary health access point for many at-risk youth, many incarcerated youth receive inadequate health services (Hancock & Terry, 2019).
Future research needs to more fully investigate parent structure and health, getting more in-depth data about these structures and parent/youth relations. This need holds especially true for kinship and foster care and the relationship between health and deviance, as the “no parent” youth were the ones most likely to be deviant at higher levels of health for both measures of health. “No parent” youth likely have the most troubled backgrounds and in order to best address their needs, it is critical to understand how health plays a role with this group.
Given the complex findings, it is clearly possible that the relationship between health and delinquency is not linear. While health may erode one’s coping skills and lead to deviant coping behaviors, at some point, youth may be just too sick to engage in some of the extreme behaviors reported in this study, such as the fighting, or a potentially active behavior like stealing. Indeed, the study findings underscore the importance of more fully understanding health’s role in the tapestry of youth behavior and how it intersects with school, family, and the community.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.