
Abstract
This study aimed to investigate the effects of Person-Environment Fit on trajectories of cognitive function. Data came from the Health Retirement Study (1998-2010), focusing on those aged 65 and above who had at least one limitation in activities of daily living. Using longitudinal mixed-effect modeling, we analyzed the effects of living in supportive home environments on trajectories of cognitive function over time. Disabled older individuals living alone were likely to experience a decline in cognitive function over time. However, the detrimental effects of living alone were moderated when the home was equipped with supportive features and accessibility. The findings reveal the importance of home modifications for socially and physically vulnerable elders.
According to the U.S. Census Bureau, in 2016, 35% of older adults aged 65 and above had some type of disability such as difficulties with ambulation, independent living, hearing, vision, cognition, or self-care (U.S. Census Bureau, 2016). In 2014, nearly one half of older adults, or 18 million people, had difficulty or received help in the last month with daily activities (Freedman, & Spillman, 2014). Aging in place (in one’s own home) has become central to social policies and programs as an effective strategy for meeting older adults’ strong preference for staying in their homes as long as possible and addressing the high costs of long-term care (Farber, Shinkle, Lynott, Fox-Grage, & Harrell, 2011; Koss & Almeida, 2016). Existing evidence shows that physical features adapted in homes to reduce environmental barriers (home modifications) have a positive effect on health outcomes for people with functional disabilities including reduced risk of falls (Stark, Keglovits, Arbesman, & Lieberman, 2017) and slower functional decline (Szanton et al., 2011).
This study aims to expand current knowledge on the role of home modifications by focusing on long-term trajectories of cognitive function among older adults with functional disabilities. Cognitive impairment has been demonstrated to be the most powerful risk factor for institutionalization. Because functional limitations could cause reduced physical activity and social interactions, older adults with functional limitations who do not receive physical and social support are more likely to experience declining cognitive function (Sofi et al., 2011). Specifically, we focus on two areas that have been understudied. First, most studies on home modification have not examined to what extent the living arrangements of older adults (e.g., living alone) affect their health. The physical home environment (e.g., in-home features and accessibility) are more important to older individuals with limited functional ability, but the degree to which these elders can adapt may depend on their living arrangement. This is especially relevant as social factors are known to be important for later year cognitive health and are affected by living arrangements. Second, most existing studies are cross-sectional or followed up for a short period (6 months to 2 years) and are, thus, limited in their ability to make causal arguments about the benefits of home modifications. From a policy-planning perspective, our limited knowledge of changes in health outcomes for vulnerable subgroups of older adults hinders efforts to design effective and efficient policies.
Conceptual Framework
The Person-Environment Fit (P-E Fit) perspective (Lawton & Nahemow, 1973) was used as a framework to investigate different aspects of aging in place for older adults with functional limitations. Specific contexts of environment include physical features of the home (e.g., grab bars in bathrooms, wheelchair ramps), home technology (e.g., universal design), retirement living facilities, or, more broadly, natural or designed neighborhoods and communities that attend to the increasing and varying health and social support needs of older adults. Although they differ, these various contexts promote independence and autonomy for older adults for as long as possible. A central proposition of the P-E Fit perspective is the environmental docility hypothesis, which suggests that individuals with limited resources are affected to a greater extent by environmental demands than are individuals with more resources. Guided by this proposition, this study focuses not only on the independent effects of home environment (i.e., home modifications and accessibility), but also on how they interplay with older person’s living arrangement (living alone) and their home environment. Trajectories of cognitive function are examined as an outcome of “fit” between personal characteristics and their physical environment.
Living Alone and Cognitive Function
The number of older individuals living alone has increased in most countries around the world (Suzman & Beard, 2011). In the United States, more than 12 million people above age 65—30% of the entire older population—currently live alone (Administration on Aging, 2016). This proportion is expected to increase and become a normative part of the aging process (Lichtenberg, MacNeill, & Mast, 2000) due to a structural shift in family formation in the modern era such as an increase in those who never married and/or divorced in middle or old age. Research suggests that living alone is associated with more limitations in activities of daily living (ADL) and instrumental activities of daily living (IADL), worse physical and mental health (Gaymu & Springer, 2010), and a lack of social integration (S. T. Cheng, Fung, & Chan, 2008). An increased understanding of aging in place among live-alone adults is timely given the demographic imperatives and associated policy challenges of providing more care and support.
Recently, a growing body of research has focused on a subset of at-risk older adults who live alone with little-to-no support (Carney, Fujiwara, Emmert, Liberman, & Paris, 2016). Studies have shown that a small social network and loneliness are associated with a higher risk of cognitive decline and dementia (Boss, Kang, & Branson, 2015; DiNapoli, Wu, & Scogin, 2014; Wang, He, & Dong, 2015) and that older people who live alone have fewer social contacts, and many are lonely (S. T. Cheng et al., 2008; Gow, Corley, Starr, & Deary, 2013). Most prior studies on social relations and cognitive health have been cross-sectional or based on a short-term follow-up. A longitudinal study by Josefsson, Luna, Daniels, and Nyberg (2016) with a small sample found that over the 15-year study period, older people who lived alone exhibited lower performance on episodic memory than those who co-resided, although the difference was not statistically significant, probably because of the small sample size.
Home Environment and Cognitive Function
Home modifications are adaptations to the living environment intended to increase safety, security, and independence (Pynoos, Steinman, & Nguyen, 2010). Modifications may include changes in or additions to the structure (e.g., widening doorways or adding a first-floor bathroom or a ramp) and/or installing specialized equipment (e.g., grab bars and handrails; Maggie et al., 2018). There is strong evidence that home modifications protect older people from falling (Gillespie et al., 2012) and have a positive impact on self-rated abilities for everyday life (Stark et al., 2017). The evidence that home modifications can improve the performance and safety of people with functional limitations is growing; however, evidence for dementia-related conditions is limited (Wahl, Fange, Oswald, Gitlin, & Iwarsson, 2009).
A Joint Center for Housing Studies (2014) report indicated only 1% of U.S. housing units have key supportive features (e.g., no-step entry, single-floor living, extra-wide doorways, lever-style door knobs). The Fair Housing Amendments Act (FHAA) of 1988 is the only national policy that encourages home modifications rather than incurring the expense of building or buying a new accessible home. The effects have been limited because the policy applies only to new or renovated multifamily housing of four units or more. Currently, less than 5% of housing units are accessible to those with moderate mobility impairments and only 0.15% to those utilizing mobility devices (Semeah et al., 2017).
The impact of home modifications may depend on individual needs and situations; some subgroups may accrue more benefits than others. Disabled older adults living alone are one of the groups needing supportive housing environments because they tend to have limited physical and social support for their daily activities. Gilderbloom and Markham (1996) found that older men who live alone had a greater need for home modifications. Safran-Norton (2010) found that home modifications were a predictor of continued residence in their own homes for those who live alone, but no such relationship was found among those living with others. Older adults with functional limitations are at a greater risk for declining physical and mental health and limited physical activity (Gaymu & Springer, 2010) and a lack of social integration (S. T. Cheng et al., 2008), especially when they live alone. All these factors may contribute to declining cognitive function in old age.
The environmental docility hypothesis suggests disabled older adults who live alone may be less likely to experience cognitive decline when they live in supportive home environments. Among disabled older people, living alone may aggravate social isolation and/or loneliness; home modifications may serve as a supportive feature to enhance sense of competence, which may help reduce this isolation. Existing evidence has consistently shown that social isolation and/or lack of social engagement are strong predictors of cognitive decline (Beller & Wagner, 2018; Poey, Burr, & Roberts, 2017).
Existing empirical P-E Fit research has tended to examine housing environments as they relate to older adults’ functional health. German and Swedish studies have demonstrated that greater limitations in older adults’ daily activities were significantly related to lower accessibility within the home, a construct used to examine the fit between functional limitations and barriers in the home environment (Iwarsson, Horstmann, & Slaug, 2007). Another study showed that home modifications had a positive impact on the performance of daily activities among older adults (Stark et al., 2017), finding that activity performance and functional independence improved and were maintained over 2 years. Eshkoor, Hamid, Hassan Nudin, and Mun (2014) examined how environmental conditions affected the likelihood of falls in older people with dementia and found that increased environmental quality (e.g., lighting, ventilation, and others) significantly decreased the risk.
Surprisingly little attention has been paid to the potential direct relationship between home modifications and cognitive function. More importantly, no known study has examined the relationship between home environment and changes in cognitive function over a long period of time.
Present Study
The current study investigated long-term trajectories of cognitive function among older adults with functional limitations. Guided by the P-E Fit perspective, we hypothesized that trajectories of cognitive function differ depending on personal needs and physical environment. Specifically, we suggest two hypotheses:
Method
Data and sample
Data used in this study came from seven waves of the Health and Retirement Study (HRS), between 1998 and 2010. The HRS is a nationally representative panel survey of older adults in the United States aged 51 and older. The HRS oversamples African Americans, Hispanics, and residents of Florida. Details of multistage sample design, selection criteria, implementation, and response rates are available elsewhere (Servais, 2010). The HRS is a publicly available dataset; collection of the HRS data complies with the requirements of the University of Michigan’s Institutional Review Board (IRB).
To examine the P-E Fit, the effects of home modifications (Environment) on cognitive health (Fit) among older adults living alone with functional limitations (Person), we restricted our sample to respondents who were 65 years or older and had at least one impairment in ADL (i.e., bathing, eating, dressing, walking across rooms, or entering or leaving bed). Because proxy interviews in HRS did not provide information on the cognitive health condition of respondents, observations from proxy interviews were not included. To examine the trajectories of cognitive function over time, respondents who were already cognitively impaired (i.e., dementia) at the baseline were excluded in our sample. HRS assessed respondents’ cognitive function using a modified version of the standardized measure of the Telephone Interview for Cognitive Status (TICS; Brandt, Spencer, & Folstein, 1988), a multidimensional screening instrument modeled after the Mini-Mental State Exam (MMSE; Folstein, Folstein, & McHugh, 1975), with scores ranging from 0 to 35. Although there is no strong norm for the cutoff indicating dementia in this measure, the cutoff value of 8 has been used in multiple studies using HRS data (Crimmins, Kim, Langa, & Weir, 2011; Herzog & Wallace, 1997). Therefore, respondents whose cognitive score was less than 8 were excluded in our sample. Furthermore, because data with multiple imputation are not technically feasible for testing nested models in Stata, we dropped observations missing covariates (n = 97 observations). The final sample included 6,043 respondents with 12,086 observations over the 12-year period. Because our sample included frail older adults who had at least one ADL, attrition rate due to death or other reasons was high. During the study period, 643 respondents (10.64%) died, and 26.18% of the sample participated in three or more waves of surveys. The final sample included 6,043 respondents with 12,086 observations over the 12-year period.
Measures
Dependent variable
The outcome variable of this study was cognitive function. Scores for cognitive function included measures of memory, working memory, speed of mental processing, knowledge, and language (Freund & Szinovacz, 2002; Herzog & Wallace, 1997; Ofstedal, Fisher, & Herzog, 2005). Specifically, the total cognition score sums the word recall and mental status summary scores, which range between 0 and 35 with higher scores indicating better cognitive function. The total word recall summary variables sum the immediate and delayed word recall scores (range = 0-20). The mental status summary sums the scores for serial 7’s, backwards counting from 20, and object, date, and president/vice-president naming tasks (score range = 0-15; Ofstedal et al., 2005). Herzog and Wallace (1997) evaluated these cognitive tests and indicated that they have reasonable response rates, psychometric properties, and construct validity. Also, these measures have been used extensively in studies examining changes in cognitive function among older adults, and their validity and reliability have been demonstrated (Alley, Suthers, & Crimmins, 2007; Freedman, Aykan, & Martin, 2001; Langa et al., 2009; Lièvre, Alley, & Crimmins, 2008; Masel & Peek, 2009; Zivin, Kabeto, Kales, & Langa, 2009). In our analyses, the MMSE score was reverse-coded to show a higher value refers to a worse cognitive condition.
Key independent variables
Guided by the P-E Fit perspective, we focused on living alone as a personal characteristic and home modification and accessible home environments as environmental factors. Living alone was measured as a binary variable. Home modification was measured as a binary variable (1 = at least one home modification feature, 0 = no features at all) and was assessed based on the following two questions: “Sometimes buildings have special features to help older persons or someone with a disability get around. Does your home have features such as a ramp, railings, or modifications for a wheelchair?” and “How about special features to safeguard older persons or someone with a disability—Does your home have features such as grab bars, a shower seat, or a call device or another system to get help when needed?” Accessible home environment was determined based on three questions: “Is all your living space on one floor?” (1 = yes, 0 = no); “Is your house [or the building your home is in] one story, two stories, or more than two stories?” (1 = one story, 0 = two or more stories); and “Does your house [or the building your home is in] have an elevator or stair lift?” (1 = yes, 0 = no). Houses with at least one accessible characteristic out of three were considered as accessible home environments.
Covariates
We included a series of covariates that have been demonstrated to be significantly associated with cognitive function in old age (G. Cheng, Huang, Deng, & Wang, 2012; Hertzog, Kramer, Wilson, & Lindenberger, 2008; Lindsay et al., 2002; Sharp & Gatz, 2011). Age, years of education, and household-adjusted income (in thousands) were measured as continuous variables. Gender (female = 1, male = 0) was included as a binary variable. Race/ethnicity was categorized into White, African American, Hispanic, and others. Residential region was also included in the analyses (urban areas with a population of one million or more, suburban areas with a population of 250,000 to one million, and rural areas with a population of less than 250,000). Social relations was coded 1 if a respondent met their friends at least once per week. We also controlled for self-rated health (excellent = 1, very good = 2, good = 3, fair = 4, poor = 5) and the number of chronic conditions such as high blood pressure, diabetes, cancer, chronic lung disease, heart attack, stroke, psychiatric problems, and arthritis. To address potential bias from respondents who died during our study period and those who did not continuously participate in the survey, death (1 = dropped from survey due to death; 0 = survived throughout the study period) and ever attrited (1 = ever not responded to survey during the study period; 0 = continuously participated in the survey) were also controlled in the analyses.
Analytical strategy
We performed analyses for this study in two steps. First, bivariate analyses were done using chi-square and one-way analysis of variance (ANOVA) tests to determine differences in sociodemographic covariates and health conditions between respondents living alone and those living with others, and between respondents who had home modification features and those who did not. Second, to analyze the independent and joint associations among living alone, home modifications, and trajectories of cognitive impairment in repeated measures of panel data (Bollen, Christ, & Hipp, 2004), we conducted multilevel growth modeling. Based on person-specific baseline values (intercepts) and rates of change (slope) of cognitive impairment, multilevel growth models describe intra-individual change patterns of cognitive function over time. In our analyses, Model 1 was conducted as an unconditional model including only attrition, death, and time. Model 2 examined the main effects of living alone and home modifications on cognitive impairments without any covariates, both for initial level and linear change. In Model 3, we added a series of sociodemographic and health variables to Model 2 to control for these covariates. Finally, Model 4 examined the moderating effects of living alone and home modification on cognitive function over time. Interaction terms between living alone and home modifications were added for the initial level (intercept) and linear change (slope), and all the covariates used in Model 3 remained in the analyses.
Results
Descriptive and bivariate analyses
Table 1 shows the descriptive characteristics of our sample at the baseline and their bivariate associations with living alone and home modification. Among older adults with functional limitations, 35.03% lived alone and 29.59% had at least one home modification feature. We found that respondents who lived alone were less likely to have home modification features (27.26%) than those who lived with others (30.85%). The average age of our sample was 75.81 (SD = 8.11); 61.96% were women; 74.93% were White; and 56.69% met friends at least once a week. The average education was 11.32 years (SD = 3.47), and 44.89% lived in an urban area. Average scores of self-reported health were 3.70 (range = 1-5, SD = 1.02; a higher number is worse self-rated health), and respondents had an average of 2.82 (range = 0-8, SD = 1.44) chronic conditions. Regarding cognitive status, the average score at the baseline was 15.06 (range = 0-26, SD = 5.02; a higher number is worse cognitive function), which is considered normal (Crimmins et al., 2011; Herzog & Wallace, 1997). As mentioned above, respondents who were cognitively impaired at the baseline were dropped from our sample. As seen in Table 1, there were no significant differences in cognitive scores between living alone versus living with others and between home modification versus non-home modifications. However, compared with older adults living with others, those living alone were older, more likely to be female and White, and tended to have lower incomes and to meet their friends more often. Compared with older adults whose homes did not have any modification features, those who lived in a house with some features of home modification were younger, White, had more education, higher incomes, and a greater number of chronic conditions.
Characteristics of Sample at the Baseline, by Living Arrangement and Home Modification Status (% or Mean [SD]).
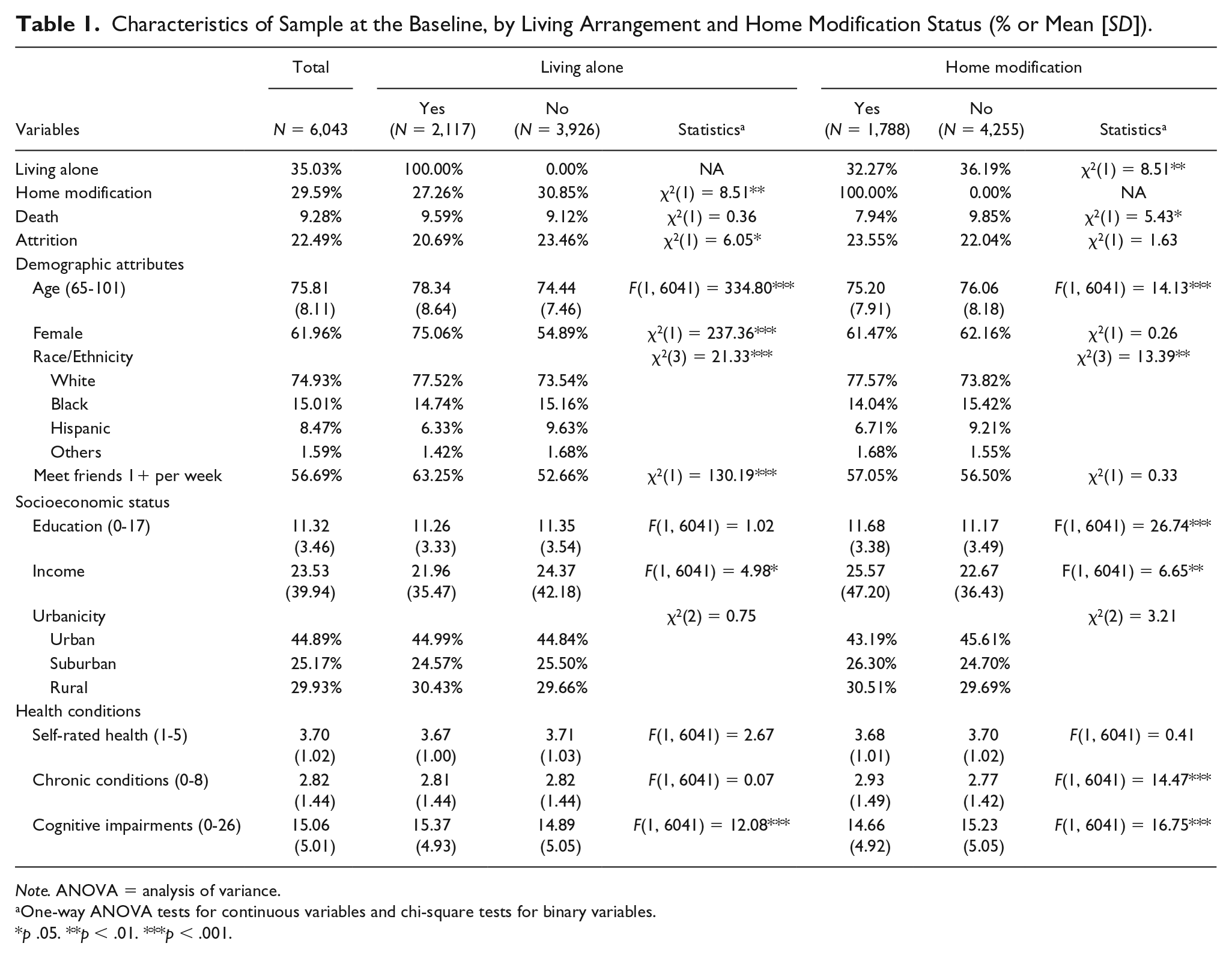
Note. ANOVA = analysis of variance.
One-way ANOVA tests for continuous variables and chi-square tests for binary variables.
p .05. **p < .01. ***p < .001.
Trajectory of cognitive functioning
Tables 2 and 3 present the hierarchical models that examined trajectories of cognitive functioning over 12 years. Home modifications and accessible home were used as environmental protective factors for cognitive function in old age. The cognitive functioning score at the mean time of follow-up was 15.954 out of a possible 35 (Coef. = 15.895, p < .001), which is considered normal, but increased (equaling decreased functioning) over time (for linear change, time, Coef. = 0.491, p < .001; Model 1). Time was significantly associated with cognitive function across all models, which illustrates that cognitive function declines over time among older adults with some disabilities. Random effects were found to be significant in between- and within-person variations in cognitive function, showing that respondents had different levels of cognitive functioning that changed over time (Singer & Willett, 2003).
Living Alone, Home Modification, and Trajectories of Cognitive Functions (N = 6,043; Obs. = 12,086).
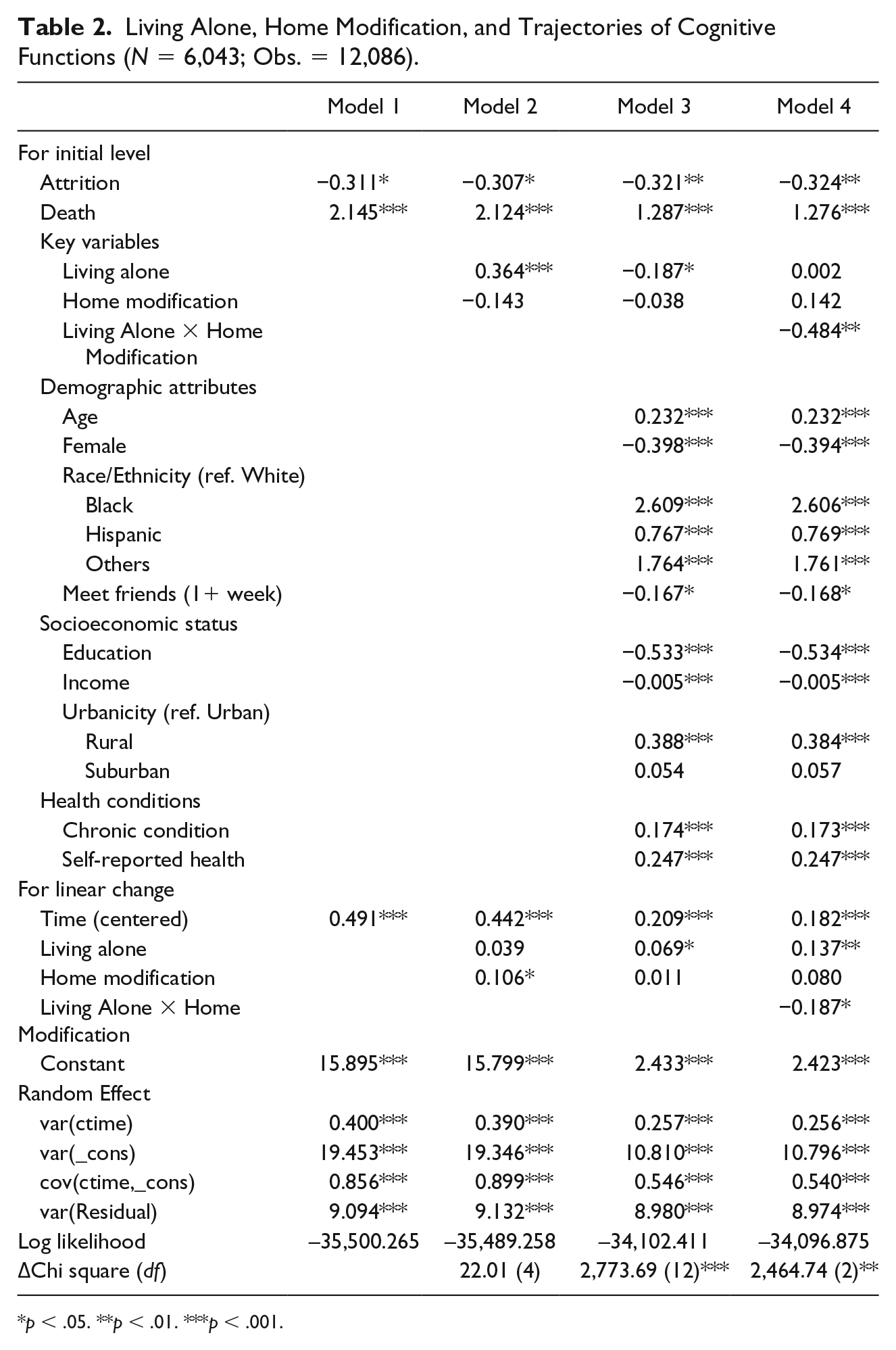
p < .05. **p < .01. ***p < .001.
Living Alone, Accessible Home, and Trajectories of Cognitive Functions (N = 6,043; Obs. = 12,086).
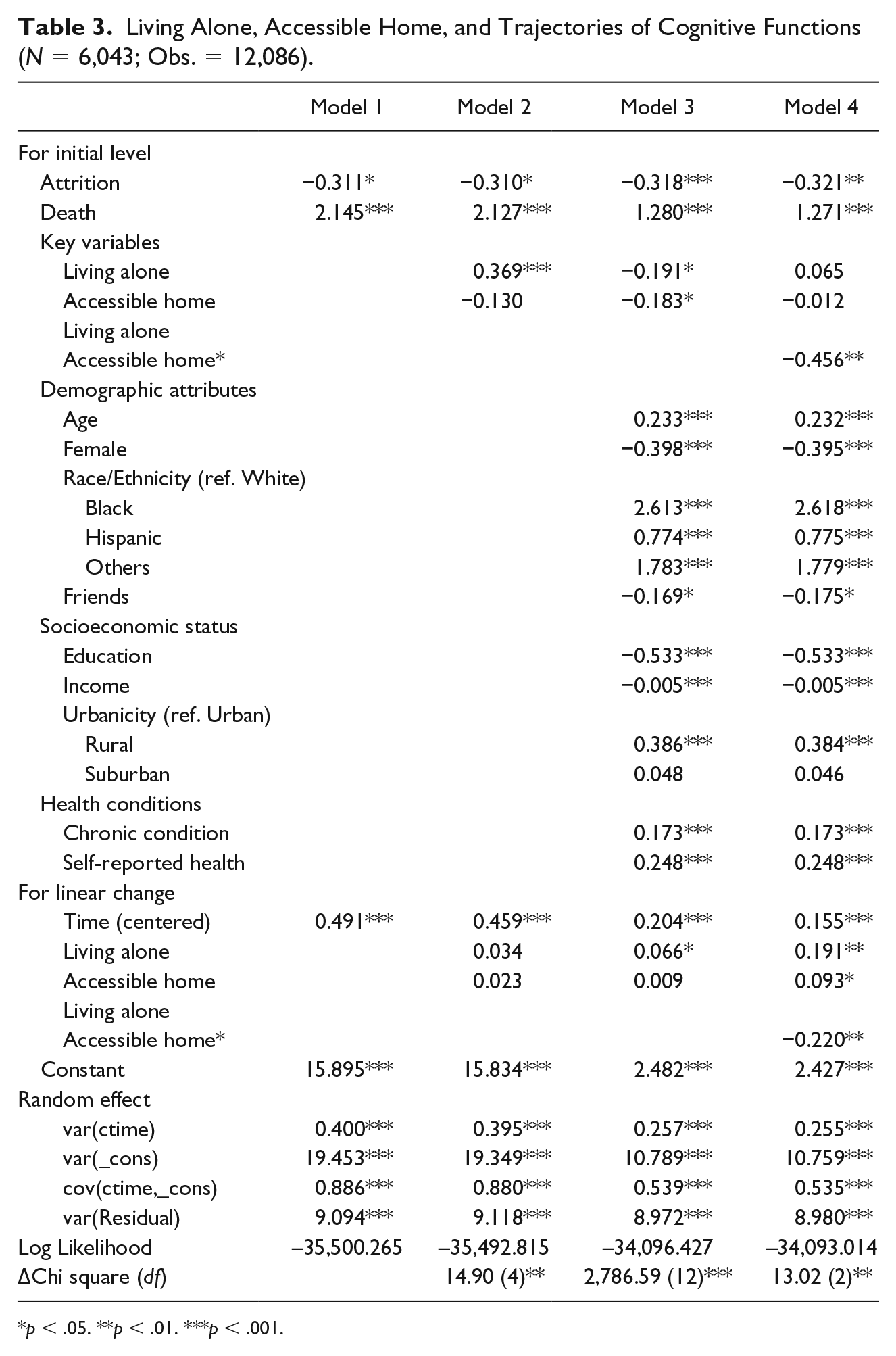
p < .05. **p < .01. ***p < .001.
Living alone, home modifications, and trajectories of cognitive functioning
In Table 2, Models 2 and 3 show the results from the analyses that examined the effects of living alone and home modifications on cognitive functioning over time. Model 2 did not include any covariates, but a series of sociodemographic and health conditions were added in Model 3 to ascertain the independent influences of living alone and home modification on cognitive functioning. Model 2 shows that respondents living alone tended to have poorer cognitive functioning (Coef. = 0.364, p < .001; Model 2), which did not significantly change over time. Home modifications were not significantly associated with cognitive functioning at the baseline, but cognitive function among respondents who lived in a home with modification features got worse much faster than among those who lived in a home without any modifications (Coef. = 0.106, p < .05; Model 2). After adjusting for sociodemographic and health covariates, the results in Model 3 turned out significantly different from those in Model 2. After controlling for all the covariates, we found that respondents living alone were significantly more likely to have better cognitive health at baseline (Coef. = −0.187, p < .05; Model 3), but, as in Model 2, their cognitive conditions got worse much faster than those living with others (Coef. = 0.069, p < .05; Model 3). We did not find any significant independent effects of home modifications on initial level or linear changes of cognitive functioning over time.
In Model 4, interaction terms between living alone and home modification were included both for initial level and linear change to investigate whether there are differences in the associations between living alone and cognitive functioning depending on home modifications. Respondents living alone and living with some home modifications tended to have better cognitive status at the baseline (Coef. = −0.484, p < .01; Model 4). Home modifications positively moderated the main effect of living alone on cognitive function over time (Coef. = −0.180, p < .05; Model 4).
Living alone, accessible home, and trajectories of cognitive functioning
Table 3 shows the results from the analyses using Accessible Home as an environmental factor and Living Alone as an individual factor. The effects of living alone and accessible home on cognitive functioning over time were examined in Models 2 and 3. In Model 2, without any covariates controlled, living alone was significantly associated with poorer cognitive functioning (Coef. = 0.369, p < .001; Model 2) but not with changes in cognitive function over time. An accessible home was not significantly associated with cognitive functioning at the baseline or change over time. After adjusting for covariates in Model 3, respondents who lived alone were more likely to have better cognitive function at the baseline (Coef. = −0.191, p < .05; Model 3), but their cognitive function declined much faster (Coef. = 0.066, p < .05; Model 3) compared with those who did not live alone. We also found that cognitive function among those living in accessible home environments was better than those living in homes without accessible features (Coef. = −0.183, p < .05; Model 3), but we did not find any significant independent effects of accessible home on linear changes of cognitive functioning over time. Model 4 examined whether an accessible home significantly matters for respondents who lived alone over time. We found that those living alone and living in an accessible home were more likely to have better cognitive function at the baseline (Coef. = −0.456, p < .01; Model 4), and an accessible home environment reduced the speed of cognition decline over time (Coef. = −0.220, p < .01; Model 4).
Discussion
For the past several decades, achieving and maintaining independence in the community, generally referred to as aging in place, has been a stated goal of many policies and programs for older adults. Home modification has been widely considered a protective factor for loss of independence, particularly for older adults with functional limitations. Drawing from an environmental gerontological perspective (P-E Fit), this study examined the trajectories of cognitive function over time among older adults with functional limitations and their associations with social (living alone) and physical (home modifications) environments. This study makes several contributions not only to home modification literature specifically, but also to aging research in general. To our knowledge, this study is the first to examine P-E Fit between older adults with functional limitations considering both the social and physical environments. Our findings demonstrate the importance of considering individuals’ needs and available resources when examining the effects of environmental support.
From health and social policy perspectives, identifying a compensating role of home environment for socio-physically vulnerable older people has important implications for both gerontology research and aging-related policy and program development. Findings of the descriptive and bivariate analysis were consistent with past studies, showing that older adults living alone tended to be older, female, White, and have lower income and worse health conditions (West, Cole, Goodkind, & He, 2014). Also, older adults living alone were more likely to have functional limitations, suggesting they have a higher need for home modification (Gilderbloom & Markham, 1996). The concentration of risk factors among the disabled who live alone suggests that a focused research and policy development effort should be made for this subgroup to identify what features of the environment may compensate for vulnerable health status and other living conditions.
For our first research hypothesis, we examined to what extent home modifications interact with living alone status as related to changes in cognitive function. The P-E Fit perspective suggests that the fit for successful adaptation in old age is determined by the degree to which environmental characteristics compensate for an individual’s restricted personal resources. An interesting finding was that home modifications were negatively associated with changes in cognitive function (older adults living in a modified home were more likely to experience rapid cognitive decline over time) when we did not control for covariates (Model 2). However, when we controlled for all the covariates, this significant effect disappeared, which means that the negative association could be explained by the socioeconomic and health characteristics of older adults living in a house with home modification rather than home modifications alone. In the final model, interaction terms between living alone and home modification were included both initially and for linear changes. Although it was found that home modifications did not significantly affect cognitive function trajectories in Model 3, in Model 4, we found that older adults living alone with home modifications tended to experience slower cognitive decline over time than those living with others.
For our second hypothesis, we examined to what extent home accessibility interacts with living alone status as related to changes in cognitive function. As in the case of home modification, the results indicate older adults living alone in an accessible home environment were less likely to experience cognitive decline over time. The consistently postive role of home environment supports the environmental docility hypothesis by demonstrating that a specific population whose needs (living alone and functional limitations) fit environmental support (home modifications or accessible home) had better outcomes (better cognitive functioning over time).
Existing empirical P-E Fit research has tended to examine housing environments as they relate to older adults’ functional health (Iwarsson et al., 2007; Stark et al., 2017) or risk of fall (Eshkoor et al., 2014). Petersson, Kottorp, Bergström, and Lilja (2009), in a quasi-experimental longitudinal study, found that physically disabled respondents with home modifications experienced less difficulty in performing daily life tasks compared with their peers who did not have such modifications. A more recent longitudinal study examined the effect of home modifications on the risk of falls (Maggi et al., 2018). However, most existing studies are cross-sectional, limiting their ability to make causal arguments about the benefits of home modifications. Surprisingly little attention has been paid to the potential direct relationship between home modifications and cognitive function. More importantly, no known study has examined the relationship between home environment and changes in cognitive function over a long period of time. From a policy-planning perspective, limited knowledge of the health benefits of home environment for vulnerable subgroups of older adults hinders efforts to design effective and efficient policies.
Our study is one of the first to examine trajectories of cognitive health among functionally vulnerable older adults in the context of the compensating role of home environment. Future research should pursue an empirical examination of the different functions of environmental contexts to better allocate resources for and meet the needs of older adults who live alone who have various health impairments. We discuss several important implications for future research.
Theoretically, environmental perspectives on aging (Lawton, 1985) have conceptualized the diverse needs of an older adult’s environment including maintenance, support, and stimulation. Rarely examined empirically to date, it is feasible to apply the three conceptual categories of function of residential environment embedded in the P-E Fit perspective. The perspective suggests that no matter what level of loss or decline in health characterizes the older person, there are acceptable ranges of each of the three functions that allow them to continue to be capable of affording personal satisfaction and enhanced well-being.
More relevant to current and future study is the “support” function of the home environment. Briefly, maintenance refers to the basic functions of the environment that help older persons with normal activities such as getting out of bed, going to the bathroom, and other basic functional behaviors. Compared with “maintenance,” the “support” function becomes more directly relevant for successful adaptation as an aging individual’s health declines. Support is an extended process characterized, on one hand, by relative lack of variation in terms of vulnerability and, on the other, by the easy availability of the resources necessary to maintain life. Findings of our study suggest that accessibility and safety-related features in home modifications serve as support functions for disabled older people who live alone. From a clinical intervention perspective, this suggests that resources for environmental support may be most effectively directed toward people with functional disability, whereas resources for environmental maintenance would be most effective for those with less severe impairments.
In this study, the support function was examined in two physical aspects of home environment; modification feature and accessibility. Home modification features examined in this study were largely those to ensure the safety of disabled older adults in moving around their homes. Accessibility is also closely related to safety function, but it may be more directly relevant as a way to facilitate or encourage getting out of the home for disabled people. The importance of “accessibility” is grounded in the realization that social engagement or community participation for individuals with disabilities is nearly impossible without overcoming attitudinal and environmental barriers preventing full participation (DeJong, 1979). One study investigated both physical accessibility and loneliness as related to mobility among older people (Rantakokko et al., 2014). Another study examined both physical and social environment for quality of life (Rantanen et al., 2012). Considering the well-established link between social engagement and cognitive function, an important future study should empirically examine to what extent the physical environmental fit (degree of fit between disabled older adults living alone and home accessibility) leads to changes in the social environment (i.e., isolation and/or loneliness), which ultimately affects change in cognitive health.
Last, “stimulation” functions of the home environment are characterized by the pleasurable experience of novelty, the learning of new responses, and the affirmation of the experiencer’s sense of competence (Lawton, 1985). This function is postulated to be relevant to the least competent as well as to the most competent, which may explain the independent effect in the main effect model, and more importantly, may argue that for socio-physically vulnerable people, coordinator-initiated programs and activities serve as stimulation. Home modifications promote stabilization when a functional recovery does not seem to be possible; therefore, home modifications may be the best alternative for frail older persons for whom physical exercise programs do not seem useful in terms of reduction of the risk of falls (Maggi et al., 2018). Our study provides important initial evidence about the protective role of home modifications against cognitive decline. For example, for people with lower levels of cognitive function and/or higher levels of physical disability, the degree to which home modification features moderate would vary as would which specific feature is supportive. A future study could incorporate a life space concept (Stalvey, Owsley, Sloane, & Ball, 1999). Older adults’ ability to move across different living spaces in and outside of the home (i.e., within the home area like the bedroom, immediately outside the home like the porch, and outside the home like the parking lot) could be measured. Most previous research on the home environment has focused on the number of barriers/facilitators or used a global score of environmental misfit. To what extent various functions of home modification can compensate for loss in function and/or health (e.g., degree of disability or cognitive function) for a specific clinical population (e.g., those discharged from hospitalization after a fall among those living alone) are important for future inquiries.
Another important direction for future research regards how to examine “fit” in the P-E relation. By following the majority of empirical P-E research, this study employed an interactional approach, which conceives the statistical interaction between personal (living alone) and home environmental characteristics. Contemporary research from a P-E perspective focuses on evaluating the available physically supportive features in and around the residences of older adults. European studies develop conceptual models of variations in in-home features design and accessibility (e.g., Granbom, Slaug, Löfqvist, Oswald, & Iwarsson, 2016) and propose a typology of problematic P-E Fit constellations for people with different types of functional limitations (Slaug, Schilling, Iwarsson, & Carlsson, 2015). With data permitting, it will be a promising future research to directly measure P-E Fit constellations between an individual’s health and home environment.
Certain limitations of this study should be acknowledged. First, we focused on objective aspects of physical features in the home environment. Other studies have examined objective and subjective indicators of housing quality (Oswald, Hieber, Wahl, & Mollenkopf, 2005) and multidimensional indicators such as adequacy, quality, and use of housing (Christensen, Carp, Cranz, & Wiley, 1992). Future research efforts should include a more refined set of indicators when examining the long-term effects of the physical environment. Second, a dynamic association between living arrangement and the environment underlies the P-E Fit perspective. In our study, we did not examine transition patterns of living arrangements, such as starting to live alone due to the death of a spouse or always living alone. The way older people adapt to their changing personal resources such as declining health and reduced income may be different depending on the changes in their living arrangement over time.
Despite these limitations, our study is an important contribution to the research on aging in place by demonstrating the long-term effects of home modifications for those living alone. Findings regarding health profiles and the associations between P-E Fit highlight the importance of understanding the effects of different contexts on aging in place and have important policy and intervention implications.
Footnotes
Authors’ Note
Takashi Amano is now affiliated with Rutgers University, Newark.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.