
Abstract
Background and context:
Healthy school communities aim to optimise student health and educational achievement. Various models, terms and resources have been used to describe healthy school communities. Policy makers and practitioners have reported confusion around many of the key concepts involved because of the varying models and terms. Importantly, practitioners have reported that the lack of clarity impedes progress related to advancing healthy school work. To address these issues and work towards a common understanding of healthy school communities within the Canadian context, a collaborative process involving practitioners, policy makers and researchers culminated in the production of a concept paper.
Objective:
Here, we describe the process used to develop the concept paper and summarise what is known about healthy school communities and the effectiveness of the approach.
Method:
Guided by a steering committee and expert panel, we identified, reviewed and summarised key resources to identify common components and principles necessary for a healthy school communities approach.
Results:
Core components of healthy school communities that emerged include the presence of education, social and physical environments, policy, community partnerships and the use of evidence. Fundamental principles for creating healthy school communities include the adoption of a whole school approach, education and health service synergy, planning and assessment, leadership and sustainability. Here, we describe the iterative and collaborative process to identify these key components and principles.
Conclusion:
Beyond the Canadian context, this discussion paper describes a process for enhancing communication among organisations and stakeholders invested in healthy school communities internationally.
Compared to their less healthy counterparts, healthy children have increased capacity to learn and develop the values, attitudes and skills necessary to be competent, effective and resilient adults. Children’s health status affects their ability to learn (Basch, 2011), and, in turn, education affects lifelong health status (Ever Active Schools, 2009; Stewart-Brown, 2006). Research has established a consistent, positive relationship between health and education across the lifespan (Furnee et al., 2008). A higher level of overall child and youth health status positively affects educational performance and attainment (Pathammavong et al., 2011; Suhrcke and De Paz Nieves, 2011). Interventions that promote health within a school community can result in improved academic and social achievement (Berlot and James, 2011; Florence et al., 2008; King et al., 2014; Murray et al., 2007; Ontario Physical and Health Education Association (Ophea), 2012; Suhrcke and De Paz Nieves, 2011).
Healthy school communities are necessary in order to optimise the health and educational attainment of students. A healthy school community is one that acknowledges the joint responsibility on the school and broader community for the health of students, staff and families who are part of a school. The socio-ecological model has been used to understand such complex systems as a school community (Colucci-Gray et al., 2006; Green et al., 1996; Kaai et al., 2013; Langille and Rodgers, 2010; Townsend and Foster, 2013) and underpins the Ottawa Charter for Health Promotion (Kickbush, 1989). The socio-ecological model suggests that individuals are affected by multiple levels of influence (Bronfenbrenner, 1977; Townsend and Foster, 2013). Schools are diverse in both their student populations and their settings that vary dramatically with regard to physical and social environment, policies, teaching and connections to communities (Veugelers and Schwartz, 2010). The complexity of school communities means that solutions to create healthy school environments require consideration of the individual school community context (Veugelers and Schwartz, 2010).
In Canada, efforts to optimise children’s health and learning outcomes have been impeded by a lack of clarity around the key concepts of healthy school communities (Strachan-Tomlinson et al., 2010). There are a number of different models, terms and resources that relate to healthy school communities. Knowledge users (e.g. healthy school community advocates and organisations, principals, teachers and public health units) have reported confusion around the key concepts involved because jurisdictions and organisations use varying terms and models to describe similar ideas. Importantly, practitioners (e.g. principals, teachers) have reported that the lack of clarity impedes progress related to advancing healthy school communities. For example, lack of clarity and confusion impedes communication and scaling up of healthy school initiatives across jurisdictions. Gaining consensus on a common understanding about what defines a healthy school community may facilitate greater efficacy and achievement of goals (Strachan-Tomlinson et al., 2010). Furthermore, developing a common understanding will improve coherence of efforts among partners engaged in healthy school community initiatives. For example, if educators, health practitioners and policy makers can agree on terminology and essential conditions for healthy school communities, they will be better able to align their efforts and consider similarities of their work across sectors and jurisdictions. Likewise, researchers will have a greater opportunity to evaluate outcomes and processes to achieve a healthy school community, and to determine appropriate measurement tools with greater consistency across projects.
To develop a common understanding of healthy school communities in Canada, individuals representing different organisations, jurisdictions and sectors were asked to participate in the process of developing a discussion paper with the purpose of better understanding the core elements involved. Our aim was to inform knowledge users from research, policy and practice such that improved understanding and communication can be facilitated for promoting healthy school community initiatives. Specifically, our intent is to begin building a common understanding regarding healthy school communities. This paper summarises what is known about healthy school communities, including common components and principles of pan-Canadian frameworks, and the effectiveness of the approach. Furthermore, we describe a process for enhancing communication among organisations and stakeholders invested in healthy school communities, which can be applied both within and beyond the Canadian context.
Method
Development of concept paper content
The need to develop a concept paper was identified at the National Health Promoting Schools (HPS) conference held in Alberta, Canada, in 2011. The meeting brought together stakeholders from research, policy and practice with a shared interest in healthy school communities. Among delegates, there was consensus that a concept paper which laid out the history, issues, core components and implementation principles that emerged in common from analysis of different models may serve to improve understanding and communication among delegates and other knowledge users to facilitate healthy community initiatives across the country.
Formation of steering committee and expert group
We invited individuals and organisations engaged in healthy school communities to guide and provide direction on the development of the paper. Representatives from all provinces and from health and education sectors of research, policy and practice were invited to join a Steering Committee. Additional individuals or organisations with experience and expertise in the area of healthy school communities were invited to participate on an expert panel to further refine and build the paper based on suggestions from the Steering Committee. Inclusion criteria for selecting additional members for the expert panel were diversity in geography (representing and located in different provinces), perspectives (research, policy, practice), jurisdictions (local/regional, provincial and national representation) and sectors (education and health). The final Steering Committee and expert group included individuals from six academic research institutions, and 14 organisations engaged in healthy school community policy and practice (e.g. Physical and Health Education [PHE] Canada, the Pan-Canadian Joint Consortium for School Health [JCSH], Provincial Ministries of Education, Regional Health Units).
Interviews about the historical context of healthy school communities in Canada
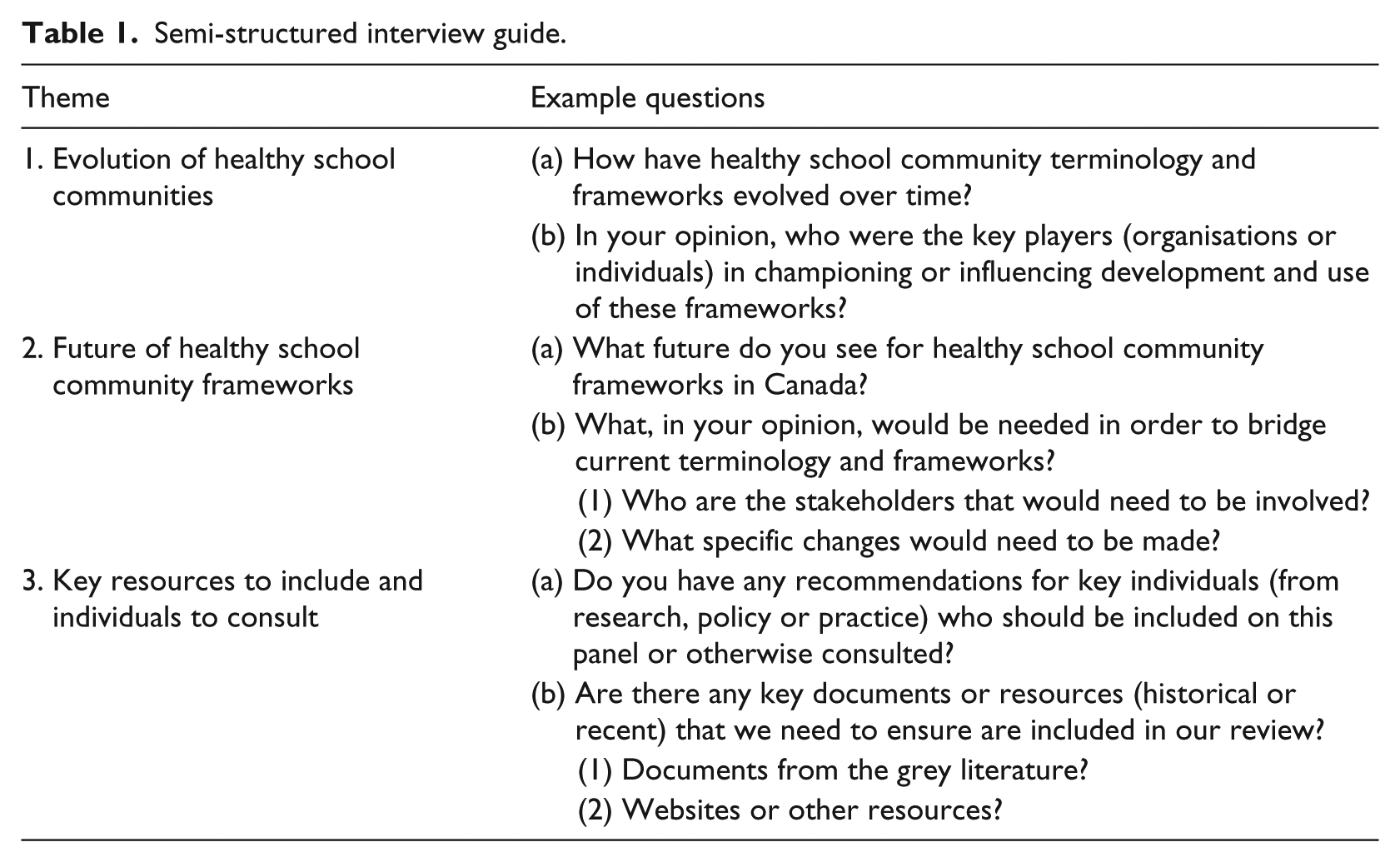
Interviews were conducted with four members of the expert panel who had relevant background and expertise regarding healthy school community research, policy and practice. Interview participants were familiar with the history and evolution of healthy school community frameworks. The purpose of the interviews was to ensure that authors had the appropriate context surrounding decisions made about the two main healthy school community frameworks currently operating in Canada (i.e. Comprehensive School Health [CSH] and HPS). Specifically, these interviews informed the authors and steering committee regarding the process of healthy school community framework development and evolution in several Canadian jurisdictions. Table 1 outlines the semi-structured interview guide.
Semi-structured interview guide.
Creating a list of key sources 1
A list of key sources was developed after an initial scan of scientific literature and Canadian and international websites related to concepts of HPS, CSH and Coordinated School Health. Steering Committee and expert panel members added to the initial list of resources and subsequently culled the list to include only the most relevant documents. Criteria for inclusion of documents were (1) relevance to healthy school communities in the current Canadian context and (2) a reflection of a framework used for healthy school communities, including those used in different areas of the world (e.g. HPS, CSH).
Concept paper process and meeting of expert group
After a small group had prepared an initial draft of the paper, 15 experts from 9 Canadian provinces, representing education and health sectors, and research, policy and practice perspectives, reviewed and provided feedback on this document prior to and during a 1-day meeting. Specifically, members of the expert group read the initial draft and participated in discussion regarding each section of the paper. Next, participants broke into small groups of individuals from research, policy and practice and discussed (1) recommendations for the paper, (2) implications of the findings and (3) strategies for dissemination, respectively. Their ideas and feedback contributed to subsequent drafts, which were further reviewed by the Steering Committee and Expert Group.
Findings
Our review yielded insightful information in three main areas: (1) the core components of a healthy school community approach, (2) the fundamental implementation principles to support a successful healthy school community approach and (3) the effectiveness of the healthy school community approach.
The core components of a healthy school community
Healthy school communities have been addressed internationally by the International Union for Health Promotion and Education (IUHPE, 2009) and the World Health Organization (WHO, 2008). Both organisations recommend a multifaceted, whole school approach to healthy school communities including a focus on instruction in and out of the classroom, the social and physical environment of the school, and the wider community (Guertin, 2007). The main purposes of this approach to healthy school communities include enhancing educational outcomes and building health knowledge and skills and behaviours in the cognitive, emotional, social and behavioural domains (IUHPE).
In Canada, the terms HPS and CSH reflect healthy school community frameworks that follow the WHO guidelines (WHO, 1996, 2008) and the IUHPE framework (IUHPE, 2005) and have been used to address school health and well-being. Many provinces/territories use these or other similar but tailored frameworks to conceptualise HPS and CSH. For the purpose of this paper, we will discuss HPS and CSH using the two frameworks as conceptualised by two pan-Canadian organisations: the Pan-Canadian JCSH and PHE Canada. JCSH (www.jcsh-cces.ca) was established in 2005 by the federal, provincial and territorial Deputy Ministers and Ministers of Health and the provincial and territorial Deputy Ministers and Ministers of Education. The purpose of the JCSH is to provide leadership and facilitate a comprehensive and coordinated approach to school health by building the capacity of the education and health systems to work together. The JCSH (2008) helped move towards some unity of understanding when they conceptualised healthy school communities using the CSH framework. PHE Canada (www.phecanada.ca/) also has a pan-Canadian mandate earned over its 75-year history. PHE Canada strives towards their vision to see ‘all children and youth in Canada living healthy, physically active lives’ through their conceptualisation of healthy school communities using the HPS framework for advocating and advancing quality physical education and health education programmes offered in Canadian schools (www.phecanada.ca). These frameworks describe the same basic concepts and processes, using slightly different language, and are often used interchangeably in research reports (Gleddie, 2011; McKenna, 2010; Veugelers and Schwartz, 2010). Each framework parallels the rationale of the IUHPE (2009) and WHO (2008) and indicates that promoting health and well-being (and thus optimal educational outcomes) in school communities requires more than classroom-based learning.
Comprehensive school health
The CSH framework aims to address school health in a planned, integrated and holistic way (Canadian Association for School Health [CASH], 2007). CSH, as conceptualised by the JCSH, is built on actions in four distinct but related pillars. When actions in all four pillars are harmonised, students are supported to realise their full potential as learners and as healthy, productive members of society. As of 2012, the CSH framework as conceptualised by JCSH has been endorsed by all provincial and territorial governments of health and education (with the exception of Quebec), as well as the Public Health Agency of Canada (JCSH).
The four pillars of CSH include the following: 2
Teaching and learning – curricular and non-curricular education of students and training of teachers in resources, activities and provincial/territorial curriculum where students gain age-appropriate knowledge and experiences, helping to build the skills to improve their health, well-being and academic outcomes.
Social and physical environment – the quality of relationships, and emotional well-being of students and staff, in addition to the buildings, grounds, spaces around the school and essential requirements such as air and water quality.
Healthy school policy – management practices, decision-making processes, rules, procedures and policies at all levels that promote health and well-being and shape a respectful, welcoming and caring school environment.
Partnerships and services – supportive working relationships within schools (staff and students), between schools and between schools and other community organisations and representative groups. Health, education and other sectors work together to advance school health. Community- and school-based services that support and promote student and staff health and well-being (JCSH, 2008: http://www.jcsh-cces.ca/index.php/about/comprehensive-school-health/4-pillars-explained).
Health Promoting School
The concept of the HPS has been described in detail by the World Health Organization (WHO, 1996). PHE Canada conceptualises the HPS framework as the ‘4Es’ – Everyone, Education, Environment and Evidence. This conceptualisation was initiated and developed by Ever Active Schools and subsequently adopted (with permission) by PHE Canada as a framework that resonates with practitioners to conceptualise the HPS concept (see Ever Active Schools, 2009). Research and practice leaders have indicated that these components are critical aspects in implementing a HPS approach.
The four components of HPS include the following:
Education: supporting a culture of learning for all school community members including wellness-related programmes for students and health promotion learning opportunities for teachers, staff and parents.
Environment: fostering a safe social and physical environment in the school, home and community, implementing policies that enable healthy active lifestyles and cultivating a place where everyone knows they belong.
Everyone: collaborating in a meaningful way with the people involved in the everyday life of the school and equal and inclusive opportunities for everyone to make healthy choices.
Evidence: collaboratively identifying goals, planning for action and gathering information to indicate the effectiveness of actions to support healthy active lifestyles throughout the school community (PHE Canada, 2012: http://www.phecanada.ca/programs/health-promoting-schools).
Essential components of health school communities frameworks
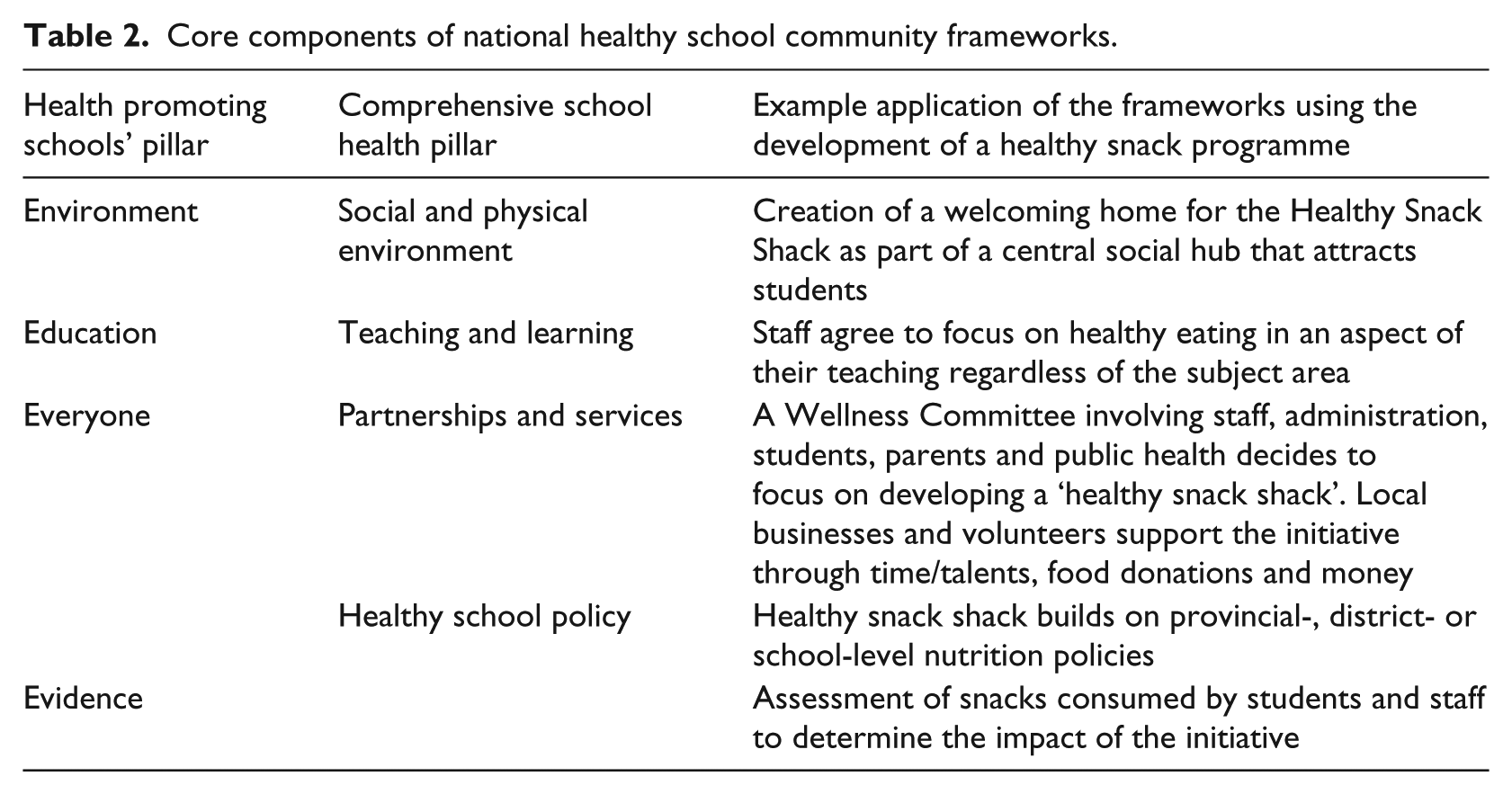
Different groups or jurisdictions use different frameworks and terminology. This has led to confusion among practitioners who may receive information, literature or support materials using unfamiliar terminology. Our review of healthy school community frameworks indicates that each framework describes essentially the same components using slightly different language and emphasis (Table 2). Both HPS and CSH emphasise the importance of healthy and supportive environments and policies along with education and partnerships. CSH as conceptualised by the JCSH draws attention to the importance of Healthy School Policy by pulling it out as a separate pillar, in addition to the social and physical environment pillar. The HPS framework, as conceptualised by PHE Canada, highlights a unique component called evidence, which for the purpose of this paper refers to gathering information systematically for planning and evaluation. Although evidence (or continuous learning, planning and evaluation) is not identified as a separate pillar in the CSH framework, it is a core principle underlying CSH to determine whether the strategies implemented are successful and to help guide improvements over time (JCSH, 2008). To move the healthy schools agenda forward in Canada, it is important, especially for stakeholders, to realise that we are all seeking the same end result, and it can be achieved regardless of which framework or vocabulary is used. For example, Table 2 illustrates a healthy school community approach through the application of the frameworks’ components in the development of a ‘healthy snack shack’ within a school.
Core components of national healthy school community frameworks.
Fundamental principles of the healthy school community approach
Given the complexity of school communities (Keshavarz et al., 2010; Veugelers and Schwartz, 2010), the process of creating healthy school communities must be looked at through a broad lens and tailored to the particular context. In addition to understanding the core components, one must consider the fundamental principles of a healthy school community approach and deem these principles as necessary conditions for successful implementation. From our targeted review of the literature and input from expert panels/steering committee, the following fundamental principles of a healthy school community approach emerged.
Whole school approach
One striking consistency in the discussion surrounding implementation of any healthy school community framework is the need to employ a whole school approach. The whole school approach refers to the interdependence of the school, its teaching and learning, its physical and social environment and partnerships with the community. This approach incorporates a healthy culture through structures, policies and procedures for staff, students and community to model and promote health and well-being (Guertin, 2007; McIsaac et al., 2013). Involvement and cohesion among school principals, teachers, students, parents and other members of the school community are imperative and an essential part of a whole school approach (Gottlieb et al., 1999; Mullen et al., 1995). Successful implementation demands integrated and holistic strategies (IUHPE, 2009; JCSH, 2008). Indeed, healthy school community initiatives must reach every part of the school community within and outside the classroom including its environment and policies (Beaudoin, 2011).
Education and health synergy
Education and health are integrated within the Pan-Canadian frameworks examined (JCSH, 2008; PHE Canada, 2012). Both are integral in the implementation of policies and actions to support healthy school communities (Gleddie, 2012). Cooperation and collaboration between health and education sectors often facilitate forward movement in the implementation of healthy school communities (Gleddie, 2011). However, incongruent priorities may exist between health and education, which inevitably contribute to tensions and a lack of cooperation (Saab et al., 2009). Effective efforts to implement a comprehensive approach in schools seek buy-in from education and health stakeholders. That is, by working together, both health and education can achieve optimal outcomes in their respective spheres (JCSH, 2008; PHE Canada, 2012). Joint planning and coordinating policies and resources (e.g. funding, time) across the health and education sectors can reduce duplication of efforts to enhance student well-being and decrease gaps in existing policies and practices (Gleddie, 2012).
Leadership team/committed champion
An individual leader or champion who strongly values a healthy school community approach and healthy living is key to successful implementation (Baugh Littlejohns, 2006; Deschesnes et al., 2010; Gleddie, 2011; Rowling and Jeffreys, 2006; Saab et al., 2009). While the positive effect of a school leader may be strongest when the principal acts as champion (Rowling and Samdal, 2011; Saab et al., 2009), some provinces and jurisdictions employ dedicated staff within schools to act as key champions for healthy school communities (Card and Doyle, 2008). A dedicated position to help guide and develop capacity for healthy school community initiatives has been linked with successful implementation (Austin et al., 2006; Card and Doyle, 2008; Ebbesen et al., 2004; Fung et al., 2012; Guertin, 2007; Vander Ploeg et al., 2014; Winnail et al., 2005). However, one individual alone is not sufficient for successful implementation; engaging a team of individuals with strong commitment, relationships (JCSH, 2008), communication and management practices will aid in facilitating healthy school community actions (Rowling and Samdal, 2011). Team members should include teaching and non-teaching staff, students, parents and community partners from stakeholder groups including at least one member from the health sector. Parents and students should be involved in all stages of a healthy school community approach (Macnab, 2013).
Assessment, planning and evaluation
The effective implementation of healthy school community approaches requires thoughtful planning, careful assessment of impacts and meaningful learning from actions. Evidence should inform planning in order to create healthy school communities and accelerate progress. In turn, evidence should be gathered based on the actions of healthy school communities, and this evidence should feed back into the system to inform future efforts and decision-making (Riley et al., 2011).
Consistent with planning literature, school communities should assess (1) existing resources including their current healthy school community actions, policies, goals, structures, resources (Rowling and Samdal, 2011), processes and personnel (Gleddie, 2011; Saab et al., 2009) and (b) needs of the students and staff (Beaudoin, 2011; IUHPE, 2009; Rowling and Jeffreys, 2006). The development of a specific and strategic implementation strategy is critical (Gleddie, 2011; Scottish Health Promoting Schools Unit, 2004). An effective implementation strategy involves all stakeholders including administration, teachers, staff, students and the broader community (Rowling and Jeffreys, 2006; Saab et al., 2009; Scottish Health Promoting Schools Unit, 2004).
Planning for sustainability
The process to establish healthy school communities requires strategies beyond limited-time ‘projects’ or ‘interventions’ (Rowling and Samdal, 2011). A healthy school community approach requires implementation over a long period of time (Guertin, 2007). Many studies have focused on how to achieve this sustainability. For example, there must be long-term anchoring of the healthy school community initiatives into policy at the school and district levels (Rowling and Samdal, 2011). Sponsoring agencies can contribute to sustainability through long-term commitment to healthy school community initiatives. Healthy school communities should approach change in an incremental, gradual and sustained manner (Saab et al., 2009) as such change requires intense and long-duration programmes, which inherently take time to implement (Baugh Littlejohns, 2006; Rowling and Samdal, 2011). It is important to allow for adequate time for changes to occur and for schools to see progress towards their specific healthy school community goals and targets (Gleddie, 2011; IUHPE, 2009).
Summary of core components and fundamental principles
The two nationally endorsed frameworks considered, the Comprehensive School Health framework (JCSH) and the HPS framework (PHE Canada), differ in emphasis not substance. They share their origins in international frameworks (IUHPE, 2009; WHO, 2008) and have the same goal of promoting healthy school communities that improve both health and academic success. The synthesis of evidence and consultation with experts related to the two frameworks points to fundamental principles that support development of healthy school communities. These include employing a whole school approach led by a strong champion backed by a team representing various perspectives; using effective planning, assessment and continuous improvement strategies to achieve synergy of education and health outcomes and incorporating sustained effort and sustainability planning. These components are described in Figure 1.
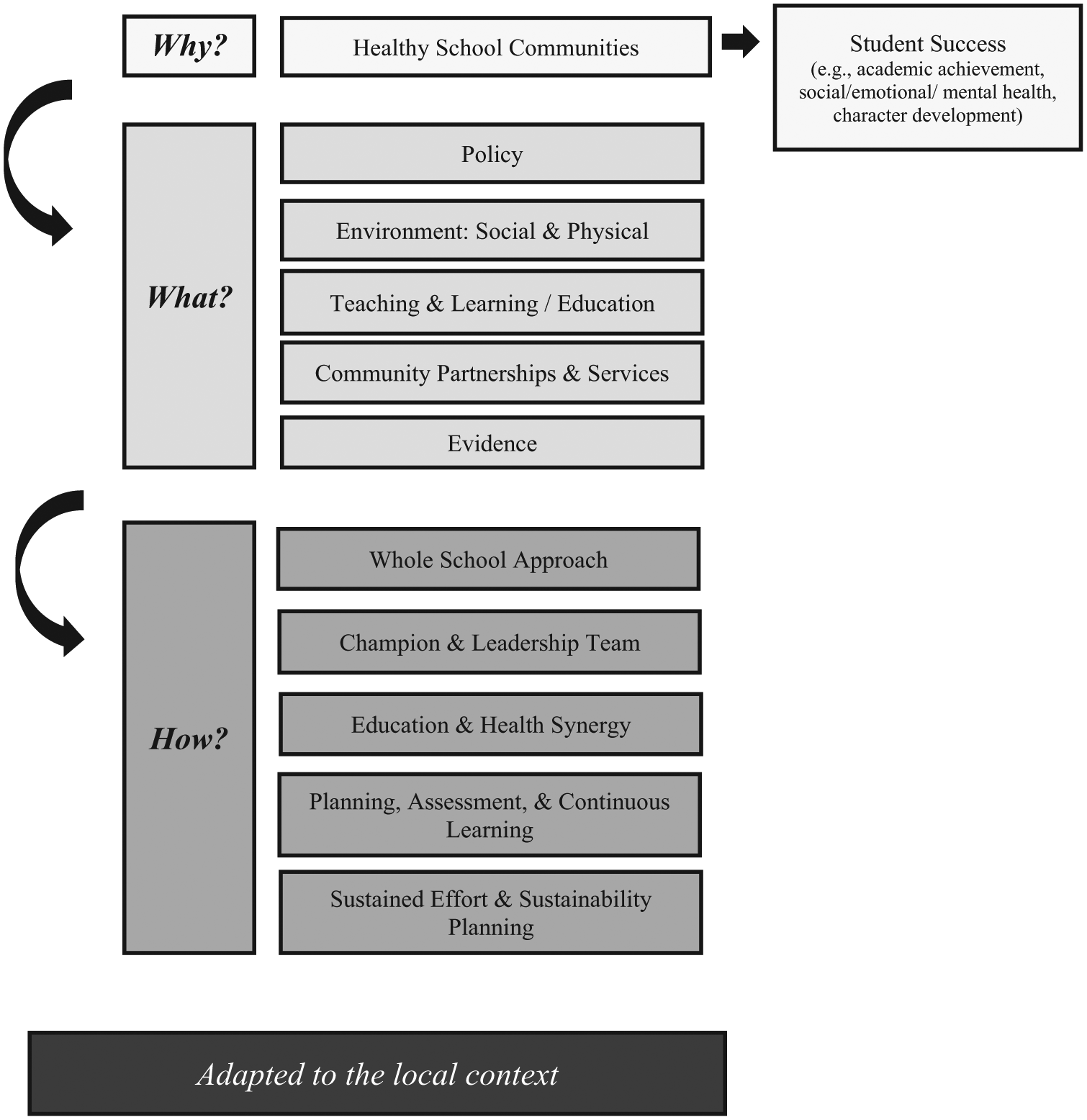
Healthy school community frameworks and implementation processes.
The effectiveness of the healthy school community approach
Evaluating the effectiveness of a particular healthy school community framework can be a challenging endeavour. While longitudinal studies have established the positive effect of targeted interventions, less well understood is how broader, comprehensive approaches to creating healthy school communities impact on health and academic outcomes. Specifically, few studies have examined initiatives that incorporate all the different components of a healthy school community framework (Fung et al., 2012; Guertin, 2007; Mukoma and Flisher, 2004; Stewart-Brown, 2006; St. Leger, 1999; Veugelers and Schwartz, 2010). However, there is evidence to support the notion that healthy school communities (or components of healthy school community frameworks) have a positive impact on health and academic and education outcomes (Guertin, 2007; King et al., 2014; Murray et al., 2007; Reed et al., 2008; Veugelers and Schwartz, 2010). When schools reported using some aspects of a healthy school community framework, there was a positive impact on the social and physical environment of the school, staff development, opportunities for healthy food at lunch and physical activity programmes (see Murray et al., 2007 for a review). Changes to behaviour were found in some (but not all) of the studies reported in the review. For example, schools that have used healthy school community interventions to focus on the health issue of physical inactivity have found a positive impact on students’ physical activity levels (Ophea, 2012). Another study showed that a healthy school community approach resulted in greater self-esteem in students and reduced bullying in the schools involved (Guertin, 2007). An evaluation of 33 Living Schools (an intervention that uses a CSH framework) showed evidence of significant improvements in standardised education test scores (Ophea, 2012) suggesting academic benefits to the comprehensive approach. A CSH approach was also used in the Alberta Project Promoting active Living and Healthy Eating (APPLE) Schools. Students attending APPLE schools were more physically active, had a lower likelihood of obesity, consumed more fruits and vegetables and consumed fewer overall calories after 2 years of programme implementation (Fung et al., 2012; Vander Ploeg et al., 2014). As well, students in CSH schools (APPLE) were more active not only during the school day, but also on weekends (Fung et al., 2012; Vander Ploeg et al., 2014). Overall, the existing research provides strong evidence for the positive effect of a healthy school community approach on health and academic outcomes. A more recent review (Basch, 2011) supports the claim that comprehensive healthy school community approaches can enhance academic achievement and reduce both education and health disparities.
Conclusion and future directions
This paper details the current state of approaches and evidence for healthy school communities. The purpose is to contribute to the development of a common understanding and enhanced communication regarding core components and implementation principles for creating healthy school communities. We have contributed to this objective through (1) the development of this paper itself, (2) presentations at national academic and practice conferences, (3) the development of a Healthy School Communities brochure for dissemination in school communities, and (4) broader communication initiatives such as teleconferences, social media and key website dissemination (e.g. PHE Canada). Furthermore, the process of developing the concept paper was beneficial in contributing to this objective; representatives from all provinces, and from health and education sectors of research, policy and practice, were engaged in communication and knowledge mobilisation activities. This process has been informative in identifying barriers to a common understanding and communication, as well as facilitators and strategies to enhance communication.
Despite our best efforts, however, improved understanding and communication around core components and implementation principles of healthy school communities is an on-going process, and we are in the beginning stages. Advancement of both research and practice in this area requires further evidence of the effectiveness of healthy school community frameworks for impacting health and academic achievement. Very few sources included in this review examined the full scope of healthy school community frameworks. In part, this is due to the complexity of the task. One challenge in gathering evidence for the concept paper was to compare outcomes of extant literature, which use various terms to describe healthy school communities and various indicators and measures to assess outcomes. A common language and common assessment indicators would permit greater comparison of outcomes and advance our understanding of the impact of healthy school community approaches (Riley et al., 2009). Future research must focus on the following areas: (1) evaluation of the implementation and outcomes of comprehensive approaches to healthy school communities at multiple levels including school community and individual student levels, (2) development of research methods and programmes of research that effectively test implementation of comprehensive healthy school community approaches at multiple levels, (3) identification of contextual factors (e.g. who, where, how) related to the implementation and effectiveness of healthy school community initiatives, and (4) assessment of essential ingredients for scaling up comprehensive healthy school community initiatives in a widespread way. Tools that assess the pillars and fundamental principles underlying healthy school community approaches, such as the JCSH Healthy School Planner (www.healthyschoolplanner.uwaterloo.ca), may contribute to this advancement. Greater collaboration between health and education in research, policy and practice is likely to move forward healthy school community approaches.
Footnotes
Acknowledgements
The authors would like to acknowledge Pratik Nair for his contributions to the literature search conducted for this project.
Funding
PHE Canada received funding from Lawson Foundation as part of an initiative to address healthy school community work. The funding from Lawson Foundation became the vehicle to drive forward the work on this paper.