
Abstract
Objective:
The objective of this study was to assess knowledge of metabolic syndrome (MS) among Chinese adults and provide directions for designing healthcare promotion schemes for improving MS awareness in the community.
Design:
The study adopted a cross-sectional design and a convenience sampling method.
Method:
Chinese adults aged 18–65 years and living in the community completed a self-administered questionnaire, providing socio-demographic information and indicating their knowledge of MS using a validated knowledge of MS (K-MS) scale comprising 10 multiple-choice questions. The scores of K-MS can range from 0 to 100.
Results:
A total of 297 participants were recruited (mean age = 51.3 ± 8.9 years), 66.7% of whom were women. More than half of all participants (n = 154) were identified as having MS and numerous participants were obese (n = 158). The mean K-MS score was 44.9 out of 100; most participants (61%) scored below 50, indicating a poor level of MS knowledge. Participants who were older, had a lower level of education or were unemployed scored the lowest.
Conclusion:
Acquiring knowledge of MS is crucial for preventing the development of type 2 diabetes and cardiovascular diseases. However, Chinese adults in a community setting exhibited poor understanding of MS. Public health efforts regarding primary prevention of cardiovascular diseases should be targeted at improving MS knowledge. Additional measures are needed to assist people in the low socioeconomic classes.
Keywords
Introduction
Metabolic syndrome (MS) has gained increasing attention due to its association with type 2 diabetes development and cardiovascular events. In the USA, age-adjusted prevalence reveals that those between 40 and 59 years of age have at least twofolds higher prevalence compared with those between 20 and 39 years of age. By the age of 60 and above, the prevalence of MS is approximately 50% for both men and women (Mozumdar and Liguori, 2011). Meanwhile in Asia, the prevalence of MS is beginning to resemble that in the Western countries. For example, the age-adjusted prevalence of MS in Korea increased significantly from 24.9% in 1998 to 31.3% in 2007 (Lim et al., 2011). In China, using the latest harmonised criteria of defining MS, the prevalence among urban community residents was approximately 33.5%. Furthermore, regardless of which definition of MS applied, the presence of MS was associated with a relative risk from 3.5 to 5.2 for diabetes development (Ford et al., 2008).
MS is characterised by a cluster of metabolic risk factors, including impaired glucose tolerance, elevated fasting triglycerides, decreased fasting high-density lipoprotein cholesterol, elevated blood pressure and central obesity (Alberti et al., 2009; Grundy et al., 2005). The presence of MS contributes to an increased risk for cardiovascular events as well as all-cause mortality (Lakka et al., 2002; Mottillo et al., 2010). In addition to physical detriments, MS also affects an individual’s quality of life because of its association with various depressive symptoms (Akbaraly et al., 2009; Huang et al., 2011a).
As suggested by the American Heart Association (AHA), individuals with MS at their pre-morbid state should be first recommended to lifestyle modifications including changes in diet and increase in physical activity (Grundy et al., 2005). Healthcare professionals may encourage such lifestyle changes through health education to modify individuals’ perception of their own health in line with the theoretical model of behaviour change (Janz and Becker, 1984). However, poor knowledge level of MS may result in reduced risk perception and subsequent poor health management (Hollman et al., 2006; Wan et al., 2014). For example, in the USA, a study has found that less than 15% of the respondents had recognised MS or had adequate knowledge about MS (Lewis et al., 2008). In Greece, a multi-centre study has reported that one-third of their respondents were unaware of their MS conditions (Athyros et al., 2005).
Against this background, the management of MS at primary level requires the involvement of both public health and healthcare professionals. This study aimed to assess knowledge of MS among Chinese adults, a topic which has not been not studied previously. Our findings aimed to assist in the review of existing health promotion curricula and the development of better programmes for the primary prevention of MS in a fast-growing population.
Methods
Design and sampling
This study was approved by the ethical committee of The Chinese University of Hong Kong. All participants were briefed on the study purpose, consented to be involved, and were assured of the anonymity and confidentiality of study results. A cross-sectional survey design was employed to examine knowledge of MS among Chinese adults in the community setting of Hong Kong. Participants were recruited from a convenience sample obtained during a community health assessment programme. The inclusion criteria were Chinese, aged 18– 64 years, who could comprehend Cantonese-Chinese. Those with known cardiovascular diseases (CVD) or who were enrolled in other cardiovascular health promotion programme were excluded.
Measurements and instruments
Basic health assessments were first conducted by a registered nurse. They included the measurement of height, weight, body fat composition, waist circumference (WC), blood pressure and fasting capillary glucose level. All participants were then invited to complete a self-administered questionnaire to assess their knowledge of MS and to collect socio-demographic data. Information on medical history and current prescriptions were assessed by the nurse based on participant-provided data. In this study, participants with three or more risk factors as specified by the AHA-harmonised criteria 1 (Table 1) were identified as positive for MS (Alberti et al., 2009).
American Heart Association (AHA)-harmonised criteria for the clinical diagnosis of metabolic syndrome.

AHA: American Heart Association.
The knowledge of MS (K-MS) scale, developed by See et al. (2010), was used in this study. It has three subscales embedded in 10 multiple-choice questions: (1) Definition of MS, (2) Relationship between MS and CVD and (3) Prevention of MS. There are five answer options for each question, including the option ‘I do not know’. Scoring was based on the number of correct answers and each correct answer will be given a score of 10. Thus, the total score of K-MS can ranged from 0 to 100, with a higher score indicating a better knowledge of MS. In this study, the face and content validity of the questionnaire was established by a panel of experts including an endocrinologist, nurses and cardiovascular health researchers. For the K-MS scale, a Cronbach’s alpha of .77 was achieved indicating good internal consistency. The K-MS scale was also pre-tested and achieved an intraclass correlation coefficient of .78 between day 1 and day 14, indicating good test-retest reliability.
Statistical analysis
All data were analysed using IBM SPSS for Windows version 20.0. Participants’ characteristics and the scoring of K-MS were reported by descriptive statistics. Socio-demographic information, health history and anthropometric data were presented as means and standard deviations for continuous variables, and frequencies and percentages for categorical variables. Performance on K-MS and socio-demographic characteristics between those with and without MS were tested for using independent samples t-test and Chi-square test according to their level of measurement. In addition, K-MS scoring was compared across different socioeconomic statuses using one-way analysis of variance (ANOVA). The level of significance of all statistical testing was set at alpha = .05.
Results
Characteristics of participants
Table 2 provides the summary of participants’ socio-demographic data. A total of 297 Chinese adults were recruited of which 66.7% were women. The mean age was 51.3 ± 8.9 years, with 43% being aged 55 or above. Forty percent of the participants had their highest education level below secondary school and 52.2% had a monthly family income less than the local median (HKD $22,000). Despite this diverse socioeconomic background, there were no statistically significant characteristics differentiating between participants with MS and those without.
Socio-demographics of participants.
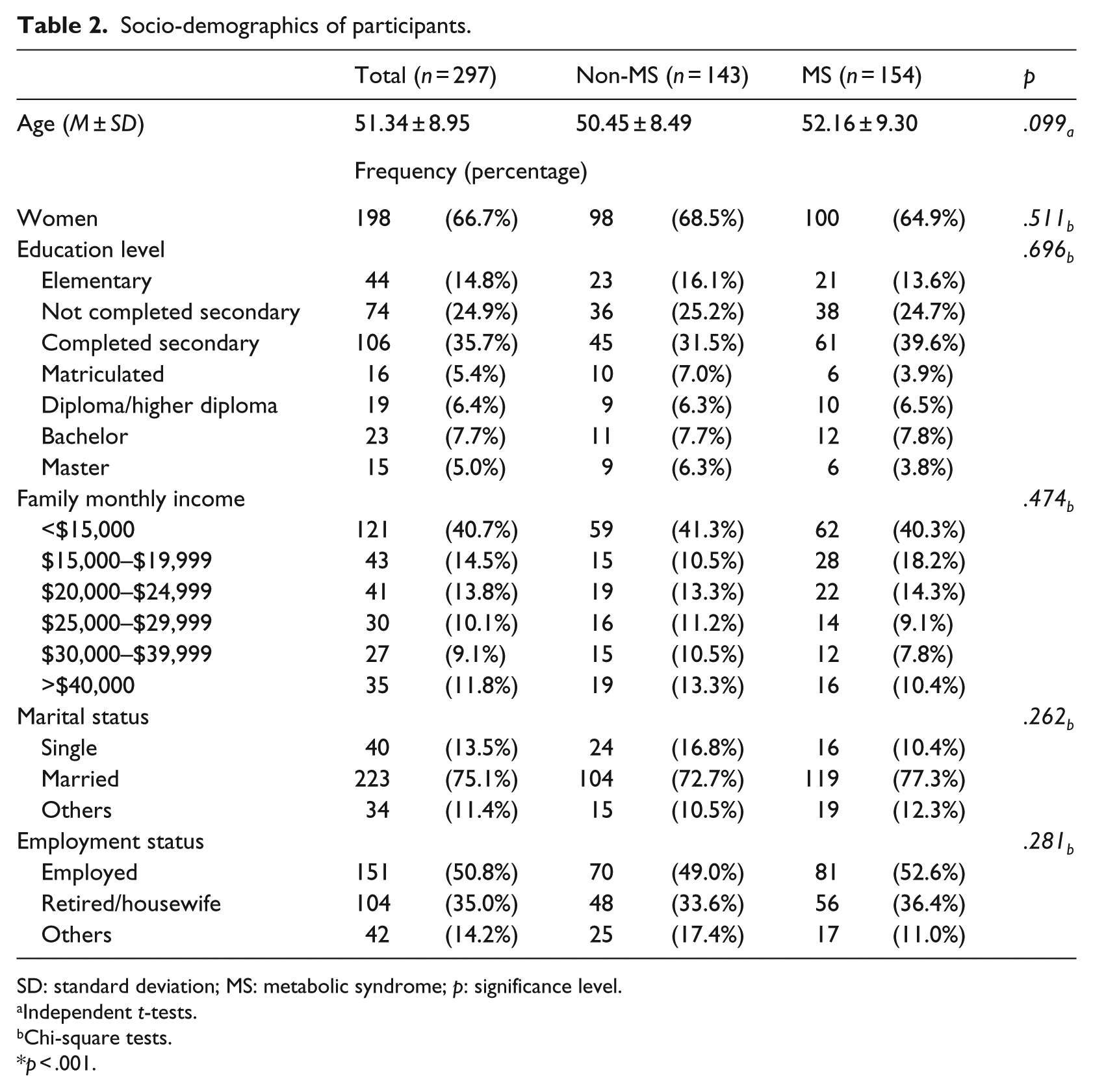
SD: standard deviation; MS: metabolic syndrome; p: significance level.
Independent t-tests.
Chi-square tests.
p < .001.
Table 3 illustrates the cardiometabolic risk profile of participants. Over half of the participants were obese (53.2%), and many of them were overweight (21.2%). For clinical indicators of MS, the mean WC for men was 88.2 cm (SD = 9.9 cm) and for women it was 93.9 cm (SD = 9.3). The mean systolic blood pressure (SBP) was 128.3 mmHg (SD = 17.0 mmHg), while the mean diastolic blood pressure (DBP) was 83.1 mmHg (SD = 11.3 mmHg). The mean fasting capillary glucose level was 5.1 mmol/L (SD = 8.6 mmol/L). Regarding their chronic disease status, 36% had been diagnosed with one or more chronic diseases such as hypertension, diabetes mellitus and hypercholesterolaemia. Despite the fact that this study did not support the detection of dyslipidaemia with clinical data, more than half (51.9%) of the participants were identified as having three or more cardiometabolic risk factors, indicating the presence of MS.
Cardiometabolic risk profile of participants.

MS: metabolic syndrome; SD: standard deviation; BMI: body mass index; WC: waist circumference; SBP: systolic blood pressure; DBP: diastolic blood pressure; Capillary-FG: capillary fasting glucose; DM: Diabetes Mellitus; MS: metabolic syndrome; p: significance level.
Independent t-tests.
Chi-square tests.
p < .001.
Scoring of K-MS
The scoring of K-MS was shown in Table 4. With a total score of 100, the mean total score of K-MS in all participants was 44.92 ± 24.65. Over 60% of participants scored below 50.00, indicating a poor knowledge level of MS. Scoring was the lowest in the subscale that assessed participants’ knowledge of the correct definition criteria of MS (scoring from 0 to 50, M = 14.81 ± 12.89), and was followed by knowledge of ways to prevent MS (scoring from 0 to 30, M = 16.94 ± 10.86). Performance was best on the subscale that assessed knowledge of the relationship between MS and CVD (scoring from 0 to 20, M = 13.17 ± 7.58). Although the total and subscale score of K-MS were generally higher among the MS group, a statistically significant difference was only found on the subscale that assesses knowledge of the relationship between MS and CVD (p = .03). It was also found that the number of ‘I do not know’ answers were significantly lower among the MS group (p = .02).
Scoring of K-MS.

SD: standard deviation; MS: metabolic syndrome; CVD: cardiovascular diseases; p: significance level.
Independent t-tests.
p < .001.
Table 5 depicts the difference in K-MS score between participants of different socioeconomic statuses. Age, education level and employment status were found to influence the scoring of K-MS significantly. In particular, participants above the age of 55 had a significantly lower K-MS score (p = .019) while those who were less educated also generally obtained a significantly lower K-MS score (p < .001). Participants in unemployment also had a significantly lower mean K-MS score than employed participants (p = .027). However, K-MS scores were not significantly influenced by family income (p = .225) nor by marital status (p = .299).
Difference of K-MS score.

MS: metabolic syndrome; SD: standard deviation; p: significance level.
Independent t-tests.
One-way analysis of variance (ANOVA).
p < .001, **p < .05.
Item-level analysis of K-MS
Figure 1 gives the breakdown of the percentage of correct answers and most frequent incorrect answer for each item in the K-MS. The overall percentage of correct answers ranged from 13.5% to 68.7%. The percentages of ‘I do not know’ answers were above 20% for nearly all items. For items that assessed knowledge of MS definition, almost half of the participants can correctly define central obesity using gender-specific WC. In contrast, the correct values for elevated blood pressure and elevated blood glucose were only known by less than one-fifth of the participants. For items that assessed the relationship between MS and CVD, over 60% of participants knew that MS was associated with CVD, but not with cancer. For items that assessed knowledge of MS prevention, about half (49.2%) of the participants believed smoking might precipitate MS occurrence.
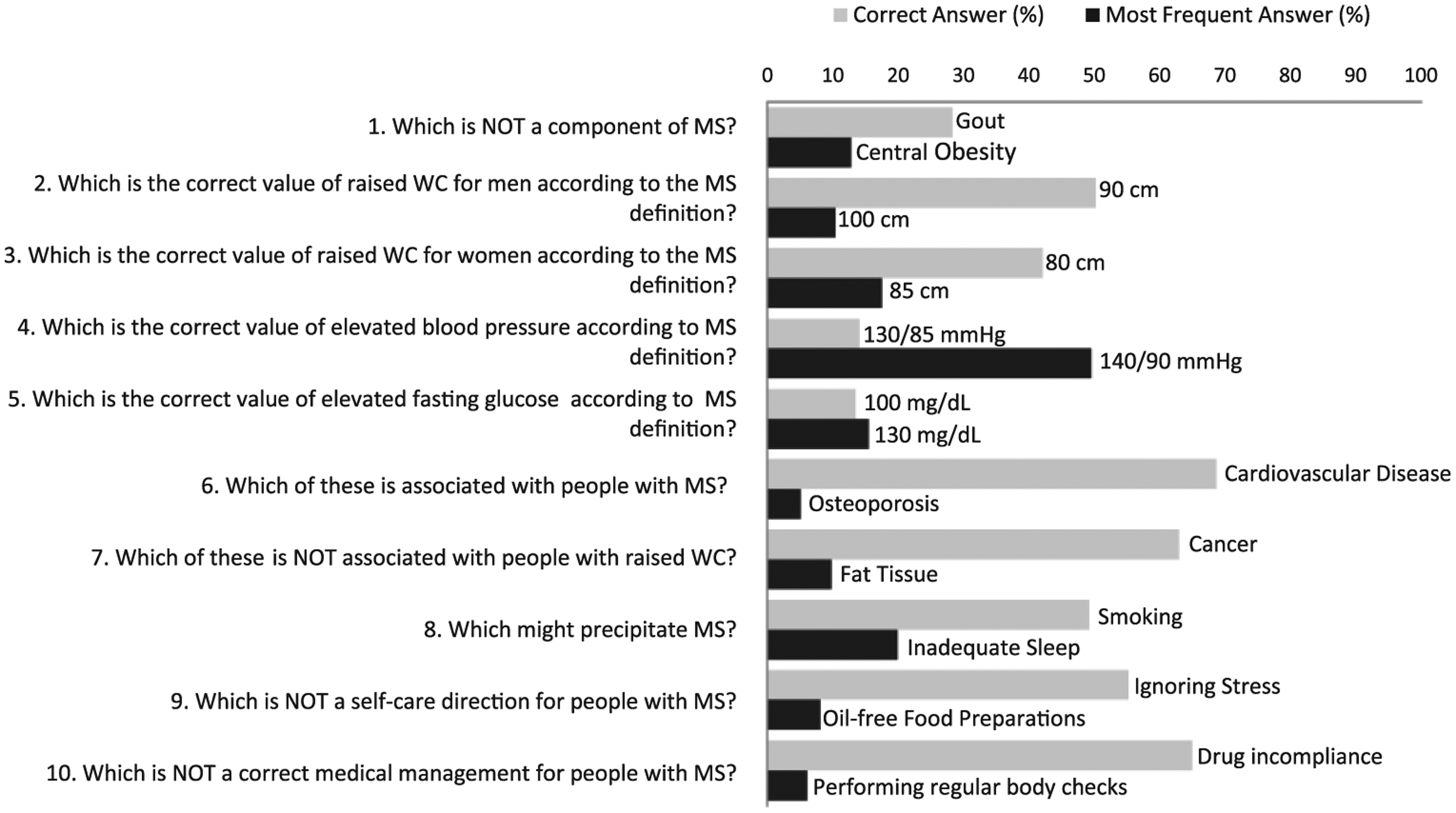
K-MS item analysis.
On the other hand, several incorrect answers were frequently selected by participants. For example, almost half (49.5%) of the participants incorrectly stated that the cut-off value for elevated blood pressure in MS is equivalent to the cut-off value for a medical diagnosis of essential hypertension. Besides, 12.8% of the participants wrongly indicated that central obesity is not a component of MS. Furthermore, ‘inadequate sleep’ was regarded as a precipitator to MS by one-fifth of our participants.
Discussion
MS is a global public health problem and its prevalence is high and increasing (Lim et al., 2011; Mozumdar and Liguori, 2011). The presence of MS has been associated with increased risk for developing CVD and type 2 diabetes (Cassells and Haffner, 2006; Mottillo et al., 2010). The recommended management of MS is primarily based on behavioural changes including the increase in physical activity, diet management and, if necessary, pharmacological intervention (Dunkley et al., 2012; Grundy et al., 2005). This study reported the characteristics and poor level of MS knowledge among Chinese adults in Hong Kong.
The poor knowledge level of MS identified in our results is consistent with findings from studies conducted in Western countries. For example in USA, The Study to Help Improve Early evaluation and management of risk factors Leading to Diabetes (SHIELD) found that less than 15% of respondents knew about MS or had an adequate knowledge about MS (Lewis et al., 2008). Meanwhile, a European multi-centre study, which evaluated the awareness, treatment and control of MS among 9,669 participants, reported that one-third of their participants were unaware of their MS condition, and only 5% of them had considered MS to be a clinical condition (Athyros et al., 2005).
Although currently there is limited evidence on the correlation between knowledge of MS and health-promoting behaviour, a positive linear relationship is apparent for other chronic illnesses such as hypertension and diabetes (Huang et al., 2011b; Norris et al., 2001). Theoretical models have suggested that health-promoting behaviour may be influenced by an individual’s perceived susceptibility to disease, together with other modifiable factors such as the perceived barriers/benefits of practising a health-promoting behaviour (Janz and Becker, 1984). Thus, it may be supposed an improved knowledge of MS will enhance health-promoting behaviour to prevent CVD and facilitate disease management. Because of this, primary healthcare professionals should consider educating clients at risk of MS in addition to their standard health education protocol.
Teachable moments for the prevention of MS may include health visits by at-risk individuals. In the case of diabetes, a culturally appropriate structured health education during health visits can increase patient’s knowledge on diabetes management and may lead to a better glycemic control (Hawthorne, 2001). Moreover, researchers have found significant associations between diabetes knowledge, self-care activities and health visits (Bruce et al., 2003). For people with obesity, Swift et al. (2009) found that health education focussed on weight management helps to facilitate informed choices about health-promoting behaviour. However, consideration must be given to individuals’ perceptions of obesity-related risks. It was well established that obesity is as an independent risk factor for CVD (Hubert et al., 1983). The fact that over half of our participants were obese individuals, and 60% of them had MS, makes this population particularly susceptible to the development of diabetes and CVD. Results from previous studies highlight the importance of self-awareness in disease management, suggesting those who are more knowledgeable about disease are more likely to take up recommended self-care activities. Based on our findings, healthcare professionals in primary care should consider enriching current diabetes and obesity prevention programmes by adding health education of MS knowledge.
Apart from the primary prevention, early disease detection requires recognition by both individuals and healthcare professionals. In some ways, it is not surprising that this population was relatively uninformed about the epidemic of MS. As relatively new terminology even to healthcare professionals, MS is still often undiagnosed and unattended to. Although many primary care practitioners had reported the use of MS diagnosis in evaluating patients for cardiometabolic risk management, previous studies had found that 43.7% of practitioners miss the diagnosis for MS and 12.9% wrongly diagnose it (Barrios et al., 2007; Gohdes et al., 2009). These findings align with a survey study of 194 healthcare workers, which reported that less than one-fifth can correctly identify MS criteria (Alam et al., 2011).
From a public health perspective, this study was conducted in an urban city that has recently launched large-scale campaigns targeting central obesity and hypertension (Department of Health HKSAR, 2012, 2013). Although the effectiveness of these campaigns is unknown, the results of this study suggest that the majority of participants continued to underestimate the WC threshold for central obesity. Participants were also confused with the value of elevated blood pressure between MS and essential hypertension. Participants in this study tend to consider that MS occurs at a state where health indicators are far beyond the normal range, and such misinterpretation of health indicators might disguise individuals’ risks for CVD.
In addition, the number of ‘I do not know’ answers was significantly lower among the MS group, suggesting their perception of an adequate knowledge for MS. Yet, the poor performance of the K-MS among the MS group revealed that their perceived knowledge of MS was indeed inadequate. This overconfidence may in turn hinder individual’s health-seeking behaviour and leads to subsequent health risks (Khan et al., 2013). In this study, although participants have a fair knowledge about MS prevention and the relationship between MS and CVD, it appeared that they lacked the knowledge to determine whether they are at risk. Therefore, health promotion programmes targeting to increase MS awareness may strengthen public’s knowledge about MS and hopefully delay the development of CVD.
Furthermore, K-MS score was found to be lowered among participants who were older in age, with lower education level and not in employment. Post-hoc comparisons indicated that the total K-MS score was significantly higher among those who had completed secondary education (M = 49.2 ± 23.3) than those education level was below secondary (M = 40.7 ± 24.2) and elementary (M = 29.1 ± 24.2). In addition, participants from lower socioeconomic classes also had poorer K-MS score. Healthcare professionals may find it valuable to make extra effort, such as through the use of creative teaching aids and case finding within the community, to increase awareness and knowledge of MS in this population.
To the best of our knowledge, this is the first study to explore levels of knowledge about MS among Chinese adults. However, the results of this study had limitations because of the convenient sampling method and relatively small sample size. The use of self-report may create recall bias during data collection, although self-report data are also considered to be less influenced by social desirability effects (Groves et al., 2013). The study did not support the detection of dyslipidaemia with clinical data and therefore it was anticipated that prevalence of MS were underestimated in this study. Another potential limitation is the high percentage of ‘do not know’ answers in the K-MS. Although this option was formulated in an attempt to enhance the reliability of the scale, this study cannot distinguish whether the participants were poor in knowledge of any particular K-MS item or generally unfamiliar with the term ‘metabolic syndrome’. Future study should assess participant’s awareness of the term ‘metabolic syndrome’ at baseline.
Conclusion
The results of this study were consistent with previous research but unique to the Chinese population. Lack of MS knowledge combined with socioeconomic status makes this group of population more susceptible to CVD. Primary care health professionals need to promote awareness of MS by providing necessary information for clients at high risk for MS. Public health programmes should improve education about MS in the community as a preventive measure against the development of diabetes and CVD.
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Professional Development Fund of the Association of Hong Kong Nursing Staff.