
Abstract
Objective:
The study aimed to design and evaluate a health behaviour change intervention for looked after young people, targeting sexual health, smoking, exercise, healthy eating and non-dependent alcohol and drug use.
Design:
A pre–post intervention evaluation was undertaken exploring health behaviours and wellbeing.
Methodology:
The one-to-one intervention was individually tailored to each person. Young people eligible for the intervention were aged 11 years and over and were ‘looked after’, meaning they were under a supervision order with a local authority in Scotland, or were a care leaver. A total of 144 young people referred to the intervention service between March 2009 and January 2014 were eligible for the evaluation. Evaluation data were analysed using standard statistical tests on SPSS.
Results:
Behaviour change techniques, including goal setting, action planning, barrier identification/problem solving and motivational interviewing contributed to improvements in all areas. Difficulties with consent and follow-up were highlighted as barriers to effective evaluation.
Conclusion:
Improving the current health of looked after young people with a view to prevent future ill health using a tailored intervention with behaviour change techniques enables this group to improve health behaviours, despite numerous challenges in working with these vulnerable clients.
Introduction
Looked after young people are under a supervision order with a local authority. In Scotland, they include those placed in residential care, foster care, kinship care and those remaining in their own homes. Research shows that looked after young people in higher income countries, including the UK, have poorer mental health, behavioural problems and poorer health behaviours around sexual health, alcohol and drug use and smoking, which represent key public health issues (Gramkowski et al., 2009; Meltzer, 2007; Meltzer and Lader, 2005; Sawyer et al., 2007; Scott and Hill, 2006; Tarren-Sweeney and Hazell, 2006).
While many different factors trigger and maintain behaviour across various settings, social and environmental influences tend to have the greatest negative impact on the health of vulnerable groups (Bywaters, 2007). As a group, looked after young people have multiple disadvantages and may have experienced abuse, neglect and family breakdown before entering care, and being subject to decisions out of their control. This all contributes to distrust of, and lack of engagement with, health-promoting services (Webb, 1998). In consequence, supporting behaviour change in looked after young people can be especially challenging. Similarly, there are considerable challenges in training professionals to enable them to deliver effective behaviour change interventions, such as motivational interviewing, to patients (Söderlund et al., 2008). Typically, health services offer a one-size-fits-all approach to health behaviour change, which has received some criticism (De Visser, 2005; Wise, 2009). Young people in care, upon receiving the same health education as other young people, may be less likely to have the motivation and skills to adopt healthy behaviours. They may also lack the resources (e.g. financial, transport), encouragement and support to implement any intentions to engage in healthier behaviours. Therefore, an approach that builds on the education they do receive is likely to be needed, along with providing support and solutions to resolve any practical barriers.
A theoretically derived intervention that both recognises and addresses the complexity of behaviour change in this disadvantaged group from an awareness of social and environmental influences is likely to be especially effective (Medical Research Council, 2008; Noar et al., 2007; Joint United Nations Programme on HIV/AIDS [UNAIDS], 1999). Such interventions, particularly at a high-intensity level, where more complex behavioural interventions are required, will necessitate additional training for health and social care staff, including carers, involved in supporting looked after young people. Furthermore, there are links between multiple risk behaviours; therefore, this may need to be a consideration in interventions (Jackson et al., 2012; Thompson and Auslander, 2010). Despite these clear health disparities for young people in care, there is a lack of reporting of interventions in the literature, internationally, to address risky health behaviours. Tailoring interventions to disadvantaged groups may be particularly important and require additional resources to affect behaviour change (Kelly et al., 2007).
We therefore aimed to develop a behaviour change intervention for looked after young people in Fife, Scotland. An important part of developing such an intervention was to include flexibility in tailoring the intervention components for each individual. The intervention for young people was part of a broader service, which included raising awareness with other services, and offering consultancy and training more widely to workers and carers. These other elements do not make up part of the evaluation reported here.
Methodology
Participants
Inclusion criteria for the service specified that young people were under a supervision order with a local council or be a care leaver, which means they were transitioning out of care services. Young people had to be aged 11 or over (range 11–21), and the focus of the presenting problem was on health behaviours, although wider factors such as mental and physical health problems may have been present. Young people entered into the service through referrals from workers, carers or self-referral. All young people engaging with the service were eligible to participate in the evaluation. These included all people who had completed a planned intervention between March 2009 and January 2014 (n = 125 of 144 referred; see Figure 1 for flow chart of participants through the evaluation).
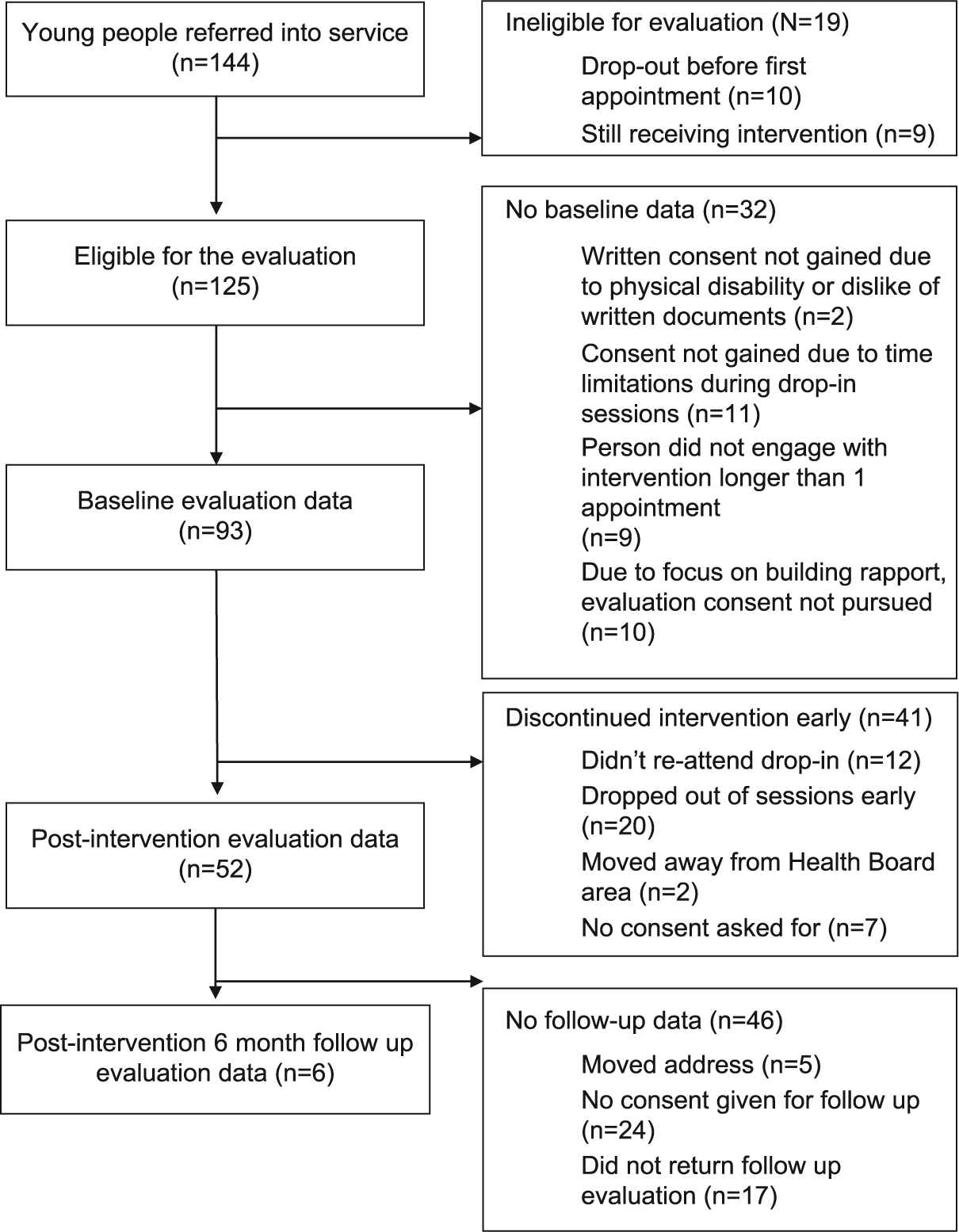
Flow diagram of the progress through the evaluation for young people referred into the service.
Intervention
The intervention was guided by a previous needs assessment of the chosen population (Dale et al., 2010), motivational interviewing and behaviour change theory and techniques. While an intervention mapping protocol was not strictly followed, the steps described by this model guided development (Bartholomew et al., 2001).
The intervention was delivered predominantly on an individual basis by a health psychologist, with occasional small group work (5 groups of 2–5 people were delivered as part of the intervention). Drop-ins were offered, to engage young people at their residential accommodation. Sessions followed a collaborative model of engagement, agenda setting and delivery of intervention. The first appointment focussed on building a rapport and shared understanding with the young person of why they had attended and formal assessment was conducted of their current health behaviours and desire for change. A combination of the assessment of health behaviours, intentions, behaviour change needs along with consideration of theories, the taxonomy of behaviour change and clinical judgement were utilised in developing a formulation and treatment plan (American Psychological Association [APA] Presidential Task Force on Evidence-Based Practice, 2006). Behaviour change theories drawn upon include the Theory of Planned Behaviour, Social Cognitive Theory and the Health Action Process Approach, which helped guide formulation and interventions, such as the inclusion of work around self-efficacy, attitude, risk perception, planning and environmental factors. The behaviour change intervention considered the broader complexities of social and environment factors within psychological formulations, which helped to inform the intervention. The interventions were tailored accordingly and ranged from low to high intensity depending on the needs of the young person. For example, a low-intensity intervention (level-2 psychological intervention; National Institute for Health and Care Excellence [NICE], 2011) may include education and information, guided self-help and development of social support for the young person in order to support change. A high-intensity intervention (level-3 psychological intervention; NICE, 2011) may involve a more complex formulation and intervention, including approaches such as motivational interviewing, techniques from cognitive-behaviour therapy and integrative therapies incorporating a range of behaviour change techniques.
The behaviour change content could broadly be considered in two phases: motivational and volitional. For example, if a young person came into the service lacking motivation, motivational techniques were utilised including motivational interviewing (‘a person-centred counselling style for addressing the common problem of ambivalence about change’; Miller and Rollnick, 2013: 24) designed to support clients in behaviour change through exploring and resolving ambivalence), eliciting/providing information about the consequences of behaviour and prompting anticipated regret. If a young person was motivated, volitional techniques (putting intentions into practice) were primarily used, including goal setting, coping planning, environmental restructuring and planning social support (Michie et al., 2011). To assist in delivering the volitional work, planning booklets were developed for all health behaviours, which were colourful, included pictures and had example plans to help guide young people. These facilitated the young person, together with the health psychologist, to develop a tailored, written action and coping plan, which incorporated implementation intentions, relating to the behaviour of choice (Martin et al., 2009). Young people were involved in their development. These plans aimed at bridging the intention–behaviour gap (Gollwitzer, 1999).
While the service was not specifically manualised, the fidelity of the service was maintained, as much as possible, to ensure a consistent service with flexibility. This was completed through regular clinical supervision from a senior health psychologist and through the recording of techniques, which allowed reflection of the techniques most commonly used (as represented in Supplementary Table 1). There was no set number or duration of sessions; this was decided on an individual basis in consultation with the young person. Typically sessions lasted 30–60 minutes, were delivered on a fortnightly basis and a mean of six sessions were given.
Measures
The evaluation used a range of outcome measures to assess behaviour, intention and wellbeing.
Behaviour
The following behaviours were measured using single-item questions: number of cigarettes smoked per week, number of hours of moderate–high intensity exercise per week, portions of fruit and vegetables per day, contraception use, frequency of condom use, number of units of alcohol consumed on an average week and drug use. For example, ‘How many units do you usually have per week (on average)?’
Intention
Intention to improve health for the above areas was also measured using questions such as ‘How much do you plan to increase the amount of exercise you are doing?’ with a 5-point Likert scale ranging from ‘strongly intend to’ to ‘strongly do not intend to’.
Wellbeing
Wellbeing was measured using the Warwick-Edinburgh Mental Well-Being Scale (WEMWBS) since it was one of the only wellbeing scales available and validated for use with young people and was brief enough to be used in appointments (Clarke et al., 2010; Tennant et al., 2007).
Behaviour change techniques
A 40-item taxonomy of recorded behaviour change techniques used in each session was documented in order to help inform future practice and research (Michie et al., 2011). Further techniques have been defined and were also included in the evaluation and are identified within Supplementary Table 1 (Dale et al., 2014).
Evaluation procedure
Data were collected at the first and last appointments, where possible, for all attendees. Young people who attended at least one appointment were invited to participate in the evaluation. A short information sheet and a consent form were given to young people. A National Health Service (NHS) Research Ethics Service was consulted, and since the project was a service evaluation, it was deemed that it did not require full ethical approval. Caldicott approval 1 was sought and granted from the local NHS board, which allowed patient information (age and sex) to be used in evaluations.
Analyses
Data were analysed using the Wilcoxon signed-rank test and McNemar’s test. Analyses were conducted using SPSS (PAWS) v18. Alpha was set to .05.
Results
Figure 1 shows the flow of young people through the service and evaluation. Unless otherwise stated, all data presented within the results are based on the 93 people for whom both evaluation consent and baseline data were available. Only six people returned the 6-month follow-up questionnaire; therefore, analyses cannot be computed for follow-up. Demographic details for these 93 individuals are presented in Table 1.
Demographic characteristics of the sample of looked after young people for whom there is baseline evaluation data (N = 93).
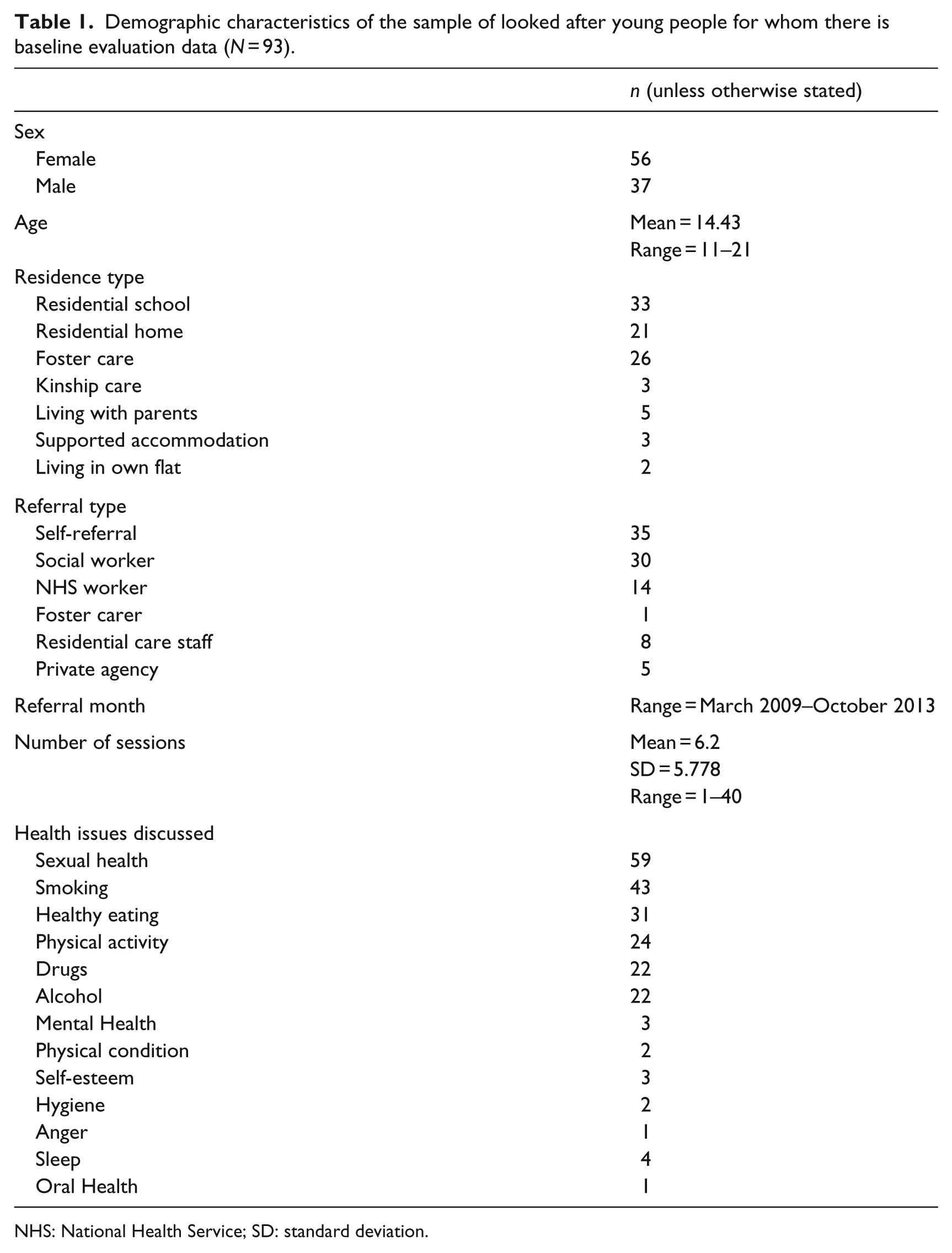
NHS: National Health Service; SD: standard deviation.
Table 2 shows self-reported behaviour change and wellbeing pre- and post-intervention. Data are only reported for those who had both pre- and post-data (n = 52). However, the numbers in each analysis are often less, since participants often just answered questions relating to the lifestyle area of focus for them.
Descriptive statistics and statistical test results for behaviours and wellbeing pre- and post-intervention.

STI: sexually transmitted infection; SD: standard deviation.
Change in smoking behaviour showed that for the 38 people whose outcome data were available, four quit and six cut down. Overall, young people smoked less cigarettes per week at follow-up (mean = 16, median = 0) than at baseline (mean = 26, median = 0), and this finding was significant (z = −2.58, p = .01 r = −.30).
Exercise was significantly increased (n = 25; z = −3.67, p ⩽ .000, r = −.52) from a mean of 3 (median = 2.5) to 6 (Median = 5) hours per week. Fruit and vegetable intake also significantly increased (n = 25, z = −3.36, p = .001, r = −.48) from a mean of almost 1 to around 2.5.
Intention to use condoms shifted from more people intending not to use them or being unsure to people intending or strongly intending to use them (n = 23; z = −2.98, p = .003, r = −.44). Condom use also moved towards more people reporting that they used condoms most of the time or always (n = 9; z = −2.23, p = .026, r = −.53). Using McNemar’s test, this showed that participants were significantly (n = 27; p = .006) more likely to be on a pregnancy contraceptive post-intervention (70%) than pre-intervention (33%). Similarly, taking a sexually transmitted infection (STI) test increased from 18% pre-intervention to 47%, however, it did not reach significance (n = 17; p = .219).
Reported changes in alcohol and drug use did not reach significance, due to floor effects in the data, suggesting that few people for whom outcome data were available reported engaging in drug or alcohol use.
Wellbeing scores increased from a mean of 40 (median = 39) to 50 (median = 53) out of 70 and was significant (n = 19; z = −3.03, p = .002, r = −.49).
Supplementary Table 1 details the total number of times each behaviour change technique was used. A total of 47 behaviour change techniques were used in total, 33 of which were from the 40-item taxonomy (Michie et al., 2011). The most frequently used behaviour change techniques from the 40-item taxonomy were as follows: providing information on consequences of behaviour in general, providing information on consequences of behaviour to the individual, motivational interviewing, providing normative information about others’ behaviour, goal setting (behaviour), action planning, barrier identification/problem solving, setting graded tasks, planning social support/social change, motivational interviewing. Out of the 40-item taxonomy, the following were frequently used: providing general encouragement, building self-esteem, building confidence to say ‘no’ to unwanted sex, discrepancy assessment (between their perceived ideal standard and own behaviour), providing general information about sex and relationships, including services, promoting positive values and attitudes towards sexual health and relationships.
Discussion
The intervention was successful in encouraging vulnerable young people in care to discuss health-related behaviours in a space that enabled them to explore the issues that were relevant to them. In spite of difficulties in gaining pre- and post-evaluation data, there were significant results for most health behaviours and wellbeing, showing that individuals have been supported to adopt a healthier lifestyle. Interestingly, providing information about sexual health and relationships was one of the most common behaviour change techniques. Sexual health and relationships were the most common lifestyle areas that young people chose to discuss, perhaps reflecting the relevance to this population and strong need for more information on this topic among looked after young people (Dale et al., 2010). Intention to use condoms and the shift in intention to use condoms were stronger than actual condom use, demonstrating that although action plans and implementation intentions can help to bridge the intention–behaviour gap, some individuals may still struggle to carry out their intentions (Gollwitzer, 1999). The evaluation of behaviour change techniques utilised in the intervention shows that a large range of both motivational and volitional techniques were used in sessions and perhaps indicates the type of techniques that may assist vulnerable young people to achieve behaviour change. The type of volitional techniques used with looked after young people in this intervention appears to be similar to that found in research targeting low income groups, which are considered to be another vulnerable group within higher income countries (Michie et al., 2008). Michie and colleagues’ review found that interventions were heterogeneous in content and the techniques most associated with effective interventions were providing information about the consequences of behaviour and goal setting. It was suggested that, particularly for disadvantaged groups, information about the consequences of behaviour may be more helpful due to more limited knowledge. This coupled with goal setting interventions may be especially facilitative of change. Motivational Interviewing may also be important for inclusion in such interventions, since young people were often engaged in the intervention reporting low levels of motivation. These approaches therefore supported young people to explore their ambivalence and build on their reasons for change.
This is the first intervention targeting health behaviour change in looked after young people to report outcome data. While numbers are small, findings reveal that positive changes can be made where collaborative, intensively tailored and engaging interventions are developed for this vulnerable group. This was made possible by using a range of referral routes and communication methods favoured by young people, for example, texts, flexibility and perseverance in engaging young people. The skills required by practitioners for behaviour change vary according to the complexity of the presenting problem, which can be influenced by social, environmental and psychological factors related to the individual; the type of behaviour; and the type of illness, if one exists. Social and environmental factors, for example, deprivation, isolation, ‘social disorganisation’ and family stability, can contribute to negative health behaviours (Yen and Syme, 1999). Interventions aimed at vulnerable groups in particular may therefore need to ensure they take into consideration the impact of the complex environmental and social issues (Kelly et al., 2007), and may need to include higher intensity interventions. There may also be some techniques that carers/professionals could use to support behaviour change with the right training and support from health professionals. This study describes relevant approaches and techniques which were used to achieve changes in behaviour, which include motivational interviewing, building self-esteem, building confidence to say ‘no’ to unwanted sex, goal setting, action planning, barrier identification/problem solving, setting graded tasks and planning social support/social change.
Limitations include the high attrition of the study sample and subsequent small sample available for analyses, unusable follow-up data, along with lack of control group. The lack of control group and associated limitations reflect the clinical need of this specific intervention to be service-based; however, it is unknown whether those not included in the evaluation changed their behaviours. Further research and/or evaluation of this approach in a greater number of participants and with longer follow-up would be beneficial. Research studies have had similar, if not greater, problems with recruitment and attrition (Mezey et al., 2015). Therefore, researchers should be mindful of the challenges of researching and evaluating this group and innovative ways to engage and retain participants may be required. Due to the flexibility offered in broad services such as this, there is greater adaptation of the interventions required compared to more manualised interventions, or the time frames that young people may be seen over. The flexibility offered in delivery of the intervention is a key strength given the mobile nature of this vulnerable group; however, this is problematic to capture due to evaluation limitations. The study also highlights the difficulties in evaluating interventions for vulnerable groups. Figure 1 demonstrates some of the added complications, including young people not returning to drop-ins, which can be a more fruitful way of engaging young people, people dropping out due to changed priorities and people moving away from the health board area.
Findings suggest that more controlled studies with this group, or other vulnerable groups, may be highly problematic, since the stage of engagement, building rapport and trust – which is critical for health promotion (St Leger, 2008) – would not be possible at the point of recruitment. Methods including social marketing, health system recruitment, physician referrals reimbursement and increased knowledge about the research have been found to be effective in recruiting hard-to-reach groups to research (Baquet et al., 2006; UyBico et al., 2007). N-of-1 studies may also prove to be an effective means of studying young people in care and other vulnerable groups since it offers a way to analyse in-depth the behaviour change process over time in individual participants (Sniehotta et al., 2012).
There may also be ways to increase the completion of research or evaluation questions. Generally, questions that can be asked informally and verbally, rather than a structured paper questionnaire, may assist in enabling more people to complete baseline data. Creative ways of gathering baseline data may be needed, such as the use of Internet or app-based methods, which may also engage young people in completion of evaluation questions. Problems also arise around evaluation consent; for service evaluations, written consent may not always be required, and would therefore allow for greater inclusion of results and a clearer picture of the interventions findings. However, ethical requirements for research and some evaluations may restrict this.
Conclusion
The development and evaluation of an intensively tailored one-to-one service for looked after young people around healthy lifestyle issues suggest that such an intervention can result in positive changes in key health risk areas. Further research, which includes a comparison or wait-list control group, would be beneficial to confirm findings. Due to the vulnerable nature of young people in care, the evaluation of the intervention is somewhat limited. This article highlights the complexities of evaluating services for disadvantaged groups in higher income countries and suggests some solutions, which include ensuring time is taken to build rapport and the use of more informal measurement tools. Evaluation is challenging; however, this should not detract from the aim of enabling vulnerable young people to improve health behaviours which will impact on their future health and life chances.
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the Fife Health and Wellbeing Alliance.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.