
Abstract
Background:
Factors affecting the delivery of sexuality education to school students include government policy, school leadership and teacher confidence.
Objective:
The aim of this paper was to understand, from the perspective of regional education, health and welfare sector professionals, what is needed to support good sexual health for secondary school students.
Methods:
A qualitative study that took place in ‘Fairview’, a regional location in Victoria, Australia. Five focus groups, totalling 37 participants, were conducted in 2015. An inductive analysis was used to identify key themes.
Findings:
The main theme was the inconsistent presence and delivery of sexuality education curriculum in Fairview schools. This was attributed to factors such as perceived lack of commitment at government level to sexuality education, lack of importance in comparison with other subjects and variation in inclusion across year levels. Teachers and the delivery of sexuality education and the role of school leadership in supporting sexuality education were the two sub-themes present within the broader narrative. Teacher capacity to deliver sexuality education was ascribed to lack of training. Perceptions concerning the use of external providers to deliver sexuality education differed, as did opinions about the role of school leadership in supporting sexuality education.
Conclusion:
Sexuality education in schools could be improved through clearer government policy direction. This would signal the importance of sexuality education to school leaders and, if supported via resources such as training for teachers, could assist in achieving the aim of improving students’ sexual health and well-being.
Introduction
Young people’s understandings of sexual health and well-being are influenced through sexuality education delivered in school settings. Key aspects of what could be considered comprehensive and equitable sexuality education include teaching that goes beyond biological and reproductive information to being a critical and theory-driven approach (Sanjakdar et al., 2015) that includes discussion and debate around ethics, communication and relationship negotiation, integrated across curriculum subjects (Goldman, 2008). However, the delivery of sexuality education can be dependent on structural interpretations (e.g. within school policies or curriculum outlines) and/or based on the knowledge of teachers, which can differ according to confidence, experience and beliefs about sexuality (Preston, 2013; Smith et al., 2013).
The international context regarding sexuality education varies. In the USA, it is characterised by a long history of debate around the delivery of one of the three approaches: abstinence-only, abstinence-based and comprehensive sexuality education (Barr et al., 2014; Dunn et al., 2014). In contrast, in many Western European countries, comprehensive sexuality education programmes are the most prevalent, informed by standards that advocate for a positive, health-promoting, rights-based, holistic approach (World Health Organization [WHO], 2010). The strengths-based approach to sexuality and relationships education contained in the Australian National Curriculum indicates a move towards a more comprehensive approach (Johnson et al., 2016) in this country, in contrast to previous disease prevention-focused curricula (Sanjakdar et al., 2015).
Sexuality education in Australia is a state and territory responsibility. As such, there is a lack of coordination and consistency nationwide (Dyson and Mitchell, 2005), with distinct differences between state and territory sexuality education curriculum and policy (Shannon and Smith, 2015). Sexuality education has been present in State of Victoria government schools for nearly 30 years (Johnson et al., 2016). However, the weight of importance placed upon it has varied, but leaned towards being low relative to other subjects (Helmer et al., 2015). This was evident findings from the First National Survey of Australian Secondary Teachers of Sexuality Education, which results noted that many teachers only spend between one and five hours in a school year on sexuality education (Smith et al., 2011). The location of sexuality education in the health and physical education domain, commonly delivered by female health or physical education teachers (Smith et al., 2011), has served to further marginalise its standing and separate its connection from other subjects throughout the curriculum. Marginalisation has also occurred through the narrow content focus on disease prevention and risk minimisation (Sanjakdar et al., 2015).
The State of Victoria government is currently implementing a new secondary school curriculum. Expert teachers will provide specialist programmes for other teachers that will cover professional learning strategies across a range of areas including health education and personal and social capability, including respectful relationships (Victorian Department of Education and Training, 2015). This is timely, given that barriers to sexuality education delivery, such as sexuality topics not being in the curriculum, lack of school policy support and a lack of teacher training, have been identified in Australian secondary schools (Smith et al., 2011).
Impediments upon teachers’ confidence to deliver sexuality education have been widely documented. These include time constraints (Smith et al., 2011), lack of guidance regarding topics and depth of content (Johnson et al., 2014; Smith et al., 2013) and feeling as though other teachers did not value the work (Ollis and Harrison, 2016). A key component of teacher confidence is the extent to which teachers feel prepared to deliver content (Barr et al., 2014; Goldman and Coleman, 2013). Teachers are reluctant to teach aspects of sexuality education when they do not feel adequately equipped (Barr et al., 2014; Fisher and Cummings, 2015; Johnson et al., 2014). Some studies have found that teachers without formal sexuality education training may narrowly define sexuality education as combating risk (Preston, 2013). Teachers are aware of their limitations in relation to preparedness; many studies have noted that when asked what resources are needed to improve their confidence to deliver sexuality education, many ask for professional development on teaching strategies and engaging learners (Fisher and Cummings, 2015; Preston, 2013).
Very little literature exists about sexuality education in regional and rural Australia. What does exist (e.g. Duffy et al., 2013; Smith et al., 2013) does not specifically discuss rurality as a factor in the delivery of sexuality education. Well-being in a rural geographical context can be defined as the outcome of a complexity of relationships, dependent on the values of who is applying the term (Winterton et al., 2014). It is conceivable, then, that rural and regional young people’s sexual health and well-being will have a relationship not only to the type, quality and amount of sexuality education they receive but also to who is delivering it.
Data for this study were collected in a regional location with a population of 37,345 in Victoria, Australia. This location, which has been given the pseudonym ‘Fairview’, was established in the 1860s. The median resident age is approximately 35 years. Two percent of the population identify as Aboriginal or Torres Strait Islander Australians. The three largest industry sectors in Fairview are manufacturing, public administration and health care. In all, 17% of employed persons in Fairview are technicians and trade workers, compared to the Victorian average of 14% (Australian Bureau of Statistics, 2011). There are 11 primary schools and two government and four independent secondary schools. The Technical and Further Education (TAFE) college also offers secondary school curriculum. All schools service students from Fairview as well as surrounding rural locations.
Fairview has a historical narrative of social disadvantage and notoriety in relation to sexual health. This is due in part to the location’s socio-cultural characteristics. For example, among other indicators of disadvantage, the town has a significant percentage of social housing in relation to total dwellings, a high percentage of families headed by one parent, a suicide rate higher than the Victorian average and a history of sexually transmissible infection notifications for Chlamydia higher than the Victorian average (Victorian Department of Health and Human Services, 2013). Sexual health–related stories in the local newspaper over the last five years have further added to stigma with headlines, including ‘Chlamydia rates high for Fairview’s young people’, ‘Teenage pregnancies doubling’ and ‘I’m having a baby at 18, get over it’.
In this paper, we aim to contribute to the existing literature by discussing the results of a qualitative descriptive study which aimed to understand the perspectives of professionals from the education, health and welfare sectors about what was needed to support Fairview secondary school students to experience good sexual health. In doing so, we hope to improve understanding of sexuality education delivery in the regional context that results in positive, supportive and pragmatic changes for schools, teachers and their students.
Methods
This was a qualitative descriptive case study that was part of a larger action research project. The project was focused on understanding and improving the systems, stakeholders and contexts that contribute to the sexual health and well-being of regional and rural secondary school students.
Ethical approval was obtained from The University of Melbourne (approval number 1545164). Sampling was purposeful with education, health, welfare and local government professionals in the study location invited to participate via an email invitation and/or being approached personally by the research team.
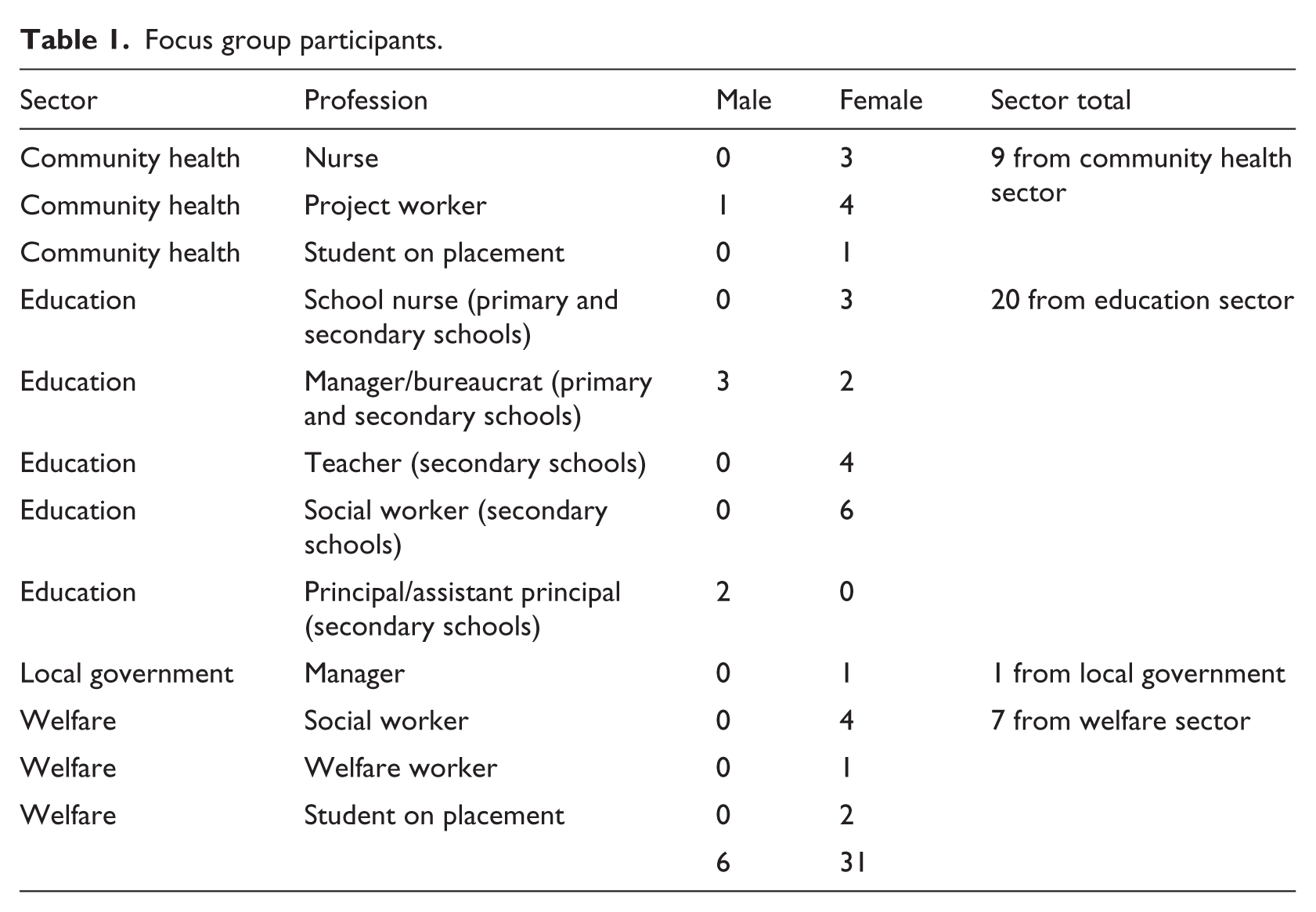
Five focus groups, with a total of 37 participants, were conducted between August and September 2015. Focus group composition was mixed according to convenience for participant attendance. There were three sectors represented across the focus groups, with a range of professionals from each sector (see Table 1). Each focus group was facilitated by authors A.H.C. and S.R., who were professionally known to some but not all of the participants. A semi-structured interview schedule (see Online Appendix 1) was used to guide discussion around participants’ knowledge and perceptions of local sexual health services, determinants of health, previous and current sexual health interventions, school roles and student support needs. Focus groups lasted approximately 90 minutes, were digitally recorded and later transcribed.
Focus group participants.
Inductive analysis was used to identify patterns and themes as they emerged from the data (Patton, 2002; Thomas, 2006). QSR NVivo (version 10) qualitative software was used to code, create categories and identify themes. A number of techniques were used to ensure that data analysis was conducted rigorously (Morse, 2015). Coding and categorisation were undertaken individually by A.H.C., S.C. and S.R., and the results were then compared. For each transcript, any data that had not been coded were discussed to determine whether new codes needed to be created. J.T. acted as a peer reviewer, helping the authorship team to further conceptualise and clarify research themes, which assisted with internal validity (Morse, 2015). This process meant some codes were collapsed into a broader theme, while others remained intact. All the authors contributed to manuscript preparation, with A.H.C. and J.T. leading this process.
Findings
The inconsistent presence and delivery of sexuality education curriculum within Fairview schools was the major theme that emerged from the focus group discussions in response to what was needed to support Fairview secondary school students to experience good sexual health. The delivery of sexuality education in the classroom and the role of school leadership in supporting sexuality education presence and delivery were the two sub-themes present within the broader narrative.
Although there were three sectors involved in the focus group discussions, the most vocal was the education sector. Within this sector, there were five distinct groups of professionals: teachers, social workers, school nurses, managers/bureaucrats and school principals. All professionals worked in the government-funded education system except for one teacher who taught at an independent school. Apart from a school nurse and the education managers and bureaucrats, the rest of the education professionals worked in secondary school settings. Discussion around the major theme and sub-themes was almost solely confined to professionals from the education sector, with a very small amount of input from community health sector professionals. The following section outlines the findings associated with the main theme and sub-themes and discusses the implications for school-based sexuality education.
Inconsistent sexuality education presence in school curricula
Inconsistency in the presence of sexuality education in Fairview schools’ curricula was discussed in equal measure by teachers, school nurses, managers and principals, with some input from community health sector professionals. Three issues were associated with inconsistent presence of sexuality education: lack of governmental mandate for delivering sexuality education, importance ascribed to sexuality education and when sexuality education is delivered.
Lack of government mandate for delivering sexuality education
Professionals from the education sector perceived a lack of commitment from the Victorian Department of Education and Training to sexuality education. This was reflected in comments about a lack of funding for teacher training and no clear direction on when and where in the curriculum sexuality education should be delivered. One school principal felt that teacher confidence was linked to training and a more comprehensive sexuality education plan:
… I reckon teachers will be confident to deliver something if they’ve got some training, and it was a departmental policy or departmental programme or something like that. But it’s all bits of isolation … (Education sector, school principal, male, P2H)
Two different teachers commented on limited government financial commitment to teacher training for sexuality education:
We have to increase teachers’ capacities and that’s hard, and that costs money and is time consuming. So that’s where the department sits, they haven’t got the money for that … It can be really difficult and the department doesn’t push it. (Education sector, teacher, female, T5R) I think it would be great if the Department of Education said you have to spend X amount of minutes teaching kids sexuality in schools and to make sure that your staff are up-skilled, here’s some training … (Education sector, teacher, female, T3R)
Importance ascribed to sexuality education
Teachers and principals discussed sexuality education as not being seen as important within the school setting in comparison with other subjects and that this contributed to inconsistency in delivery. This was discussed in the focus groups that included more teachers and education sector managers. Conversation focused on the ‘crowded curriculum’ and the pressure on teachers to meet a range of obligations:
… as schools we have other things [besides sexuality education] we need to fulfil from a departmental level and a system level. I know our teachers feel really overwhelmed with, oh, it’s just another thing we have to do. (Education sector, teacher, female, T5L)
In order to meet these obligations, teachers discussed having to focus on subjects for which outcomes are measureable, such as literacy and numeracy:
… because there’s so much pressure for schools to perform literacy and numeracy and be able to show to parents that if you come to whatever school it is in the area, that your child will achieve, there’s no way to measure sexual health … (Education sector, teacher, female, T3R)
Because sexuality education is not measured, it appeared to be easier to drop from the curriculum, as observed by a community health nurse:
… I think sexual health and wellbeing gets dropped off over lots of other things, and schools are busy, their curriculums are too full … (Community health sector, nurse, female, N4L)
Some education sector staff noted that the importance of sexuality education also seemed to be linked to particular school staff who championed for the presence of it in the curriculum. This meant that changes in school staffing posed a threat to delivery:
I used to work at Fairview secondary college and that [sexuality education] programme was driven by me and I created all the resources and pushed that programme. But then once someone leaves … then it doesn’t get picked up again. (Education sector, teacher, female, T3R)
Delivery
When sexuality education is delivered
Inconsistency in when sexuality education is delivered across primary and secondary schools in Fairview was identified by education sector professionals. Teachers employed in Fairview schools for a number of years described a scenario of constant change in when and how sexuality education was incorporated into different year-level curricula and a need for education to be delivered in primary schools from the earliest years:
… in the past, some of the nurses have been going into particularly grade fives and sixes and doing puberty education. But they need the stuff from prep … As we know young people at 12 are presenting and having positive Chlamydia tests. So if we start then, it’s too late. (Education sector, manager, female, M3J)
It was clear from comments from the education sector that continual variations in schools as to when sexuality education was being delivered was causing some students to miss out on any sexuality education at all. One school principal described a situation where not all students in years 10, 11 and 12 were undertaking the elective subjects in which sexuality education was being taught, which had resulted in:
… a big hole [in sexuality education] for most of our kids. That might be the same at most schools where once they get up in the upper levels, they’re not doing health and human development subjects [where sexuality education had been positioned for delivery]. (Education sector, school principal, male, P4M)
A school nurse remarked that inconsistent delivery was linked to a lack of monitoring at a school or government level:
… it is meant to be in the curriculum right from prep, but it’s really hit and miss as to whether schools do it. No one actually checks that they do it … (Education sector, school nurse, female, N2A)
Teachers and the delivery of sexuality education
The first sub-theme linked to the main theme of inconsistent presence and delivery of sexuality education curriculum in schools is the delivery of sexuality education by teachers. This narrative came from education sector managers, principals, social workers and school nurses, while teachers’ voices were silent in this regard. Some education sector professionals talked about teacher reluctance to even discuss sexual health topics with students. Others spoke about teachers selectively delivering only information they felt comfortable with:
Teachers will chose the ones [sexuality education units] that are the easiest or most comfortable – not the more confronting units … they will just do historically what they have done … (Education sector, manager, male, M1J) … there is a lot of good people out there that want to do the right thing but in a panic we jump in and just teach them about sex … and Catching On [sexuality education resource] doesn’t do that, it starts with that sense of self … (Education sector, school nurse, female, N2F)
The capacity to deliver sexuality education, however, was attributed by education sector managers, principals and social workers to a lack of teacher training rather than lack of interest in the topic:
… If they’re [teachers] not exposed to it [sexuality education curriculum] or haven’t received that training, they’re not going to know [how to deliver content] … (Education sector, social worker, female, S2B)
Using external providers to deliver content was raised as an alternative to training teachers. Some participants, including school principals, education sector managers and education sector social workers, felt that external facilitators had more expertise in sexual health and so were better suited to delivering this content:
We’re [teachers] not a sexual health expert … I reckon we’re better off leaving it to the professionals … so what we deliver should be some basic stuff, some understanding, and then tapping into the professionals. (Education sector, school principal, male, P2H)
However, other education sector professionals were uneasy about using external providers, seeing this as a compromise in how and when information was delivered and limiting teachers’ capacity to respond to student questions arising from externally delivered sessions. Furthermore, using external providers to deliver sexuality education was viewed as an impediment to teachers being able to develop their own skills. Well-intentioned health professionals could potentially usurp the teacher role, the benefits of confident teachers and the sustainability of sexuality education in the school by stepping into the delivery role:
The schools have requested it [sexuality education] again this year, so I have been to speak to them. We are really not supposed to be doing it but we would love to do it … it was very successful, and then hopefully the teachers would take over.
That is the problem though, is it not? We think we are increasing capacity …
But you are not …
School leadership
Discussion on the role of school leadership in supporting sexuality education was the second sub-theme linked to the inconsistent presence and delivery of sexuality education curriculum in schools. School leadership was perceived as playing a key role in the uptake of sexuality education curriculum, as well as providing opportunities for teachers to attend relevant professional development. Education sector professionals, in particular teachers and education managers, were the most vocal about school leaders being the gatekeepers to sexuality education in schools. As one teacher surmised,
It comes down to each school, so if you’ve got a leadership there … someone on there is going, we need this and we need to do something about it … (Education sector, teacher, female, T5L)
An education sector manager described her thoughts on school leadership. Using a somewhat exasperated tone of voice, she noted that despite the presence of policy and resources, school leaders had the final say on the presence of sexuality education:
Sexual and reproductive health is part of the curriculum. The department has provided evidence-based resources to support schools to implement that curriculum. It’s up to the school. (Education sector, manager, female, M3N)
Another education sector manager was quite blunt when reflecting on the power of principals to confine school nurses’ scope of practice:
Some of the dis-enablers can be the leadership in the school if they have particular strong views [about sexuality education] … (Education sector, manager, male, M5J)
However, a school principal endeavoured to explain things from a leadership perspective, discussing in particular the pressures upon school leaders to meet particular education outcomes associated with school performance and respond to parental priorities:
‘The success of a school is not around sexual health, it’s around other things …’ and ‘I don’t have parents with placards … saying we want a greater sexual health programme … they’re not marching with their feet from school to school because it’s got a greater sexual health programme …’ (Education sector, principal, male, P2H)
In contrast, an education sector manager in the same focus group countered this argument by explaining some of the broader context in which the local school leaders were operating – one aspect of which was concern around unplanned pregnancy rates within the Fairview government secondary school student cohort and the high rates of critical incidents relating to unwanted sexual contact between students occurring in these same schools. This participant spoke with a sense of urgency about the need for sexuality education to be a school priority as a means of helping address the identified concerns.
Discussion
Inconsistent sexuality education presence in school curricula
The Victorian Department of Education and Training policy on sexuality education states it is a compulsory part of the health education curriculum and that it is taught and assessed by teachers. The policy also notes that sexuality education is more effective when developed in consultation with parents and community, suggesting that there will be content variance among schools (Victorian Department of Education and Training, 2014). In relation to the involvement of school nurses, government policy notes that a team approach to health education delivery by teachers and nurses needs to be endorsed by principals. This broad direction, however, leaves scope for interpretation in when sexuality education is delivered and by whom, as evidenced by some school principals and teachers reporting using nurses from the community health sector and social workers noting they had also delivered content in the classroom. It was unclear as to whether these professionals had been approved by principals.
From this study, it is evident that direction about sexuality education delivery needs to be clearer than what is stated in the current, approximately 100 word-long Victorian Department of Education and Training sexuality education policy statement. To encourage school principals to pay greater attention to sexuality education, government guidance needs to be better articulated in relation to what schools are expected to provide, including when sexuality education should be taught and where in the curriculum (with a whole-school approach being mentioned in the Victorian Department of Education and Training sexuality education policy only once), and greater clarity around the roles of teachers and others in curriculum delivery. It is timely that this be considered immediately, as the Victorian curriculum is in a state of change, including around the content and delivery of relationships and sexuality education at secondary school level.
The need for state and nationwide consistency in the delivery of sexuality education has been identified in other studies. Smith et al.’s (2011) study of sexuality education in Australian schools recommended ‘the development of national standards and detailed unambiguous guidelines for the delivery of sexuality education from primary through to secondary school year 12 …’ (p. 49). Teachers in a US study by Eisenberg et al. (2012) discussed the need for mandatory sexuality education and state standards for health education, feeling that it was not appropriate for this decision to be made at the school level. In turn, this would support a more consistent approach to sexuality education delivery. A top-down demonstration of commitment to sexuality education would help teachers to feel supported in delivering curricula, promote consistency across schools and indicate to parents and other community stakeholders that young people’s health and well-being are fundamental to consider alongside effective education outcomes (Shannon and Smith, 2015).
Delivery of sexuality education
In the current study, there was no consistency regarding who was best placed to deliver sexuality education. Teachers were seen by some participants as appropriate but perhaps not appropriately skilled, while others felt that external providers with sexual health expertise were better suited to curriculum delivery. School nurses and social workers indicated that they had delivered sexuality education in the school setting, but this was done to ensure that students received some education, rather than provided as a prescribed element of their job roles.
Despite studies highlighting the long-standing need for teachers to be appropriately skilled (Iyer and Aggleton, 2015) and the importance of this to effective sexuality education (Carmody, 2015; Goldman, 2011; Milton et al., 2001), delivery by teachers who are not adequately trained appears to persist. This was evident in the current study, with education sector managers, school principals, social workers and school nurses critiquing teachers’ capacities to deliver sexuality education. These comments were made in support of teachers’ need for professional development, not as a criticism of their lack of care about or commitment to sexuality education.
Clearer direction about who should participate in sexuality education delivery has been raised in previous studies (Baraitser and Wood, 2001; Klein et al., 2012). This need appears to remain salient, particularly in relation to understanding the roles that can be played by different providers (e.g. school nurses, teachers, social workers) and the attributes, aside from content knowledge, required of these providers. Such attributes include trustworthiness, willingness to listen, having a sense of humour, being comfortable with one’s own sexuality, being approachable and being flexible (Milton et al., 2001).
School leadership
School leadership is important in supporting the delivery of sexuality education and appears to be the link between the role of government in establishing sexuality education policy and teachers in delivering sexuality education. School leaders in the government school system, in essence, have a role (and potentially are caught between) fulfilling government requirements while also remaining sensitive to local demands around sexuality education. The findings from this study demonstrate the power that school leadership has in directing time and resources regarding sexuality education. However, it was also raised by study participants that school leaders experience multiple competing pressures that can divert attention from curriculum issues.
Rural school leaders have been noted as facing a range of unique challenges. These include being expected to be available to attend numerous community events; being able to quickly resolve administrative, managerial, staffing and teaching issues; managing constrained budgets; and negotiating complex policy, pedagogical and outcome reporting changes with limited support (Preston et al., 2013). In the light of these constraints, it is perhaps not surprising that sexuality education was not foremost in the minds of Fairview school leaders. Given the socio-cultural characteristics of Fairview, it is reasonable to assume that a proportion of students attending Fairview government secondary schools may experience challenging family, social and economic circumstances. However, this does not mean that school leaders are absolved from responsibility; rather, it indicates that there needs to be a greater focus on supporting school leadership in relation to the effective delivery of sexuality education.
Study limitations
Although this study does provide important insights, some limitations exist. The findings of this study cannot be generalised due to a small sample that was purposefully chosen and the undertaking of the study in a regional location. Furthermore, sampling targeted those interested in and working with young people in the health, education and welfare sectors. The inclusion of participants from different backgrounds in focus groups may have limited the openness of some professionals to discuss the work of their own or another sector. Some participants also held positions of power that could have limited responses from others. Finally, many participants knew each other in a professional or personal capacity, and this may have influenced responses given in a focus group situation.
Conclusion
This paper has sought to understand what is needed to support regional secondary school students to experience good sexual health. Findings highlight that sexuality education is valued by professionals in the education sector as a means for improving students’ sexual health and well-being. However, inconsistencies in the presence and delivery of sexuality education appear to be thwarting the potential of this subject to make a positive difference in the lives of young people.
More specific government direction about the inclusion and delivery of sexuality education within schools may encourage school leaders to invest more attention and effort towards this important aspect of student learning and development. While this paper makes a contribution to the literature around sexuality education delivery in the regional context, further research is warranted regarding other issues affecting regional and rural sexuality education delivery, particularly from the perspectives of primary school and independent school leaders and teachers. Such information would assist in planning a community-wide systematic approach to sexuality education, which would ultimately benefit students’ sexual health and well-being.
Footnotes
Acknowledgements
The authors thank all participants who kindly donated their time to the study as well as Kylie Stephens who assisted with project work related to the study.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Centre for Excellence in Rural Sexual Health is funded by the Victorian Department of Health and Human Services through a service agreement with The University of Melbourne.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.