
Abstract
Objective:
Recent federal legislation in the USA highlights the role schools play in student health by requiring the utilisation of wellness councils for policy development and oversight. One barrier to developing good-quality wellness policies and wellness culture is limited knowledge of resources among school professionals. This article describes an approach to webinar delivery to improve school wellness efforts.
Design:
Eight webinars, 30–60 minutes in length, were delivered on topics designed to enhance school wellness environments.
Setting:
Webinars were delivered using an online meeting software platform to school professionals, who participated from their respective school buildings remotely.
Method:
Webinars featured content experts for the selected topics and were promoted to school professionals and wellness organisations. Attendees were invited to participate in a post-webinar questionnaire regarding satisfaction with the session and intent to act on knowledge gained from participation.
Results:
Webinars reached 280 school and wellness professionals (teachers, administrators, nurses, etc.). Participants who completed post-webinar surveys (n = 78) rated the webinar’s ability to enhance their knowledge in the respective topic area with an average score of 4.3 out of 5.0 (1 = poor, 5 = excellent). Most respondents (n = 69) intended to share the information gained with a colleague.
Conclusion:
Webinars provide a viable method of instruction and education for school personnel interested in strategies for improving a school’s wellness environment. Further investigation is necessary to determine the best strategies for promoting webinar engagement. Future research should also explore the link between webinar participation and positive changes in school wellness environments.
Keywords
Background
Children in the USA spend more than half of their waking hours in school, creating an appropriate environment for addressing student health and wellness (Centers for Disease Control and Prevention, 2014d; Institute of Medicine, 2012). Research emphasises the link between health and academic achievement, suggesting that school-based initiatives which support physical health (i.e. nutrition, physical activity) and social and emotional health (i.e. bullying prevention, mental health) are critical within the school setting (Basch, 2011; Centers for Disease Control and Prevention, 2011).
Federal legislation in 2006 and 2010 brought major changes to the landscape of school wellness efforts, particularly in local school wellness policy (United States Department of Agriculture, 2016). Unfortunately, several studies report that the school environment and policy changes that took place as a result of this legislation were less effective than originally hoped, resulting in a need for strategies to improve the development and implementation of stronger, healthier school wellness policy (Kim, 2012; Metos and Murtaugh, 2011; Smith et al., 2012).
The Whole School, Whole Community, Whole Child (WSCC) model seeks to integrate the traditional coordinated school health model into an expanded framework, supporting health and academic success through a collaborative environment (Centers for Disease Control and Prevention, 2014d). Most importantly, the model also supports professional development as a key factor in improving school wellness environments (Lewallen et al., 2015). The availability of continuing education opportunities for school professionals, such as health and physical education teachers, has increased over the last 10 years, but is often limited to the content of the subjects they teach, not school wellness overall (Brener et al., 2013). When it comes to improving wellness culture, significant barriers exist to implementing and sustaining quality wellness policies and programmes, including staff buy-in, lack of programme leadership and integration of policy and programming into current school culture (Bennett et al., 2016; Inchley et al., 2007). In addition, limited knowledge among school professionals about the most appropriate strategies to employ can also hinder implementation (Agron et al., 2010; Budd et al., 2009). This is compounded by limits to the time and financial resources available for these individuals to participate in professional development (Anderson and Enge, 2012; Vought-O’Sullivan et al., 2006).
Web-based education in the form of short, topic-centred webinars can be used to offer information about effective strategies for improving school wellness policies and environments. In addition, this format of professional development can be accessed at low or even no cost to the participant and their school employer. In this article, we describe our approach to webinar delivery as a means to improving knowledge about effective strategies for increasing school wellness efforts.
Methods
Webinar development
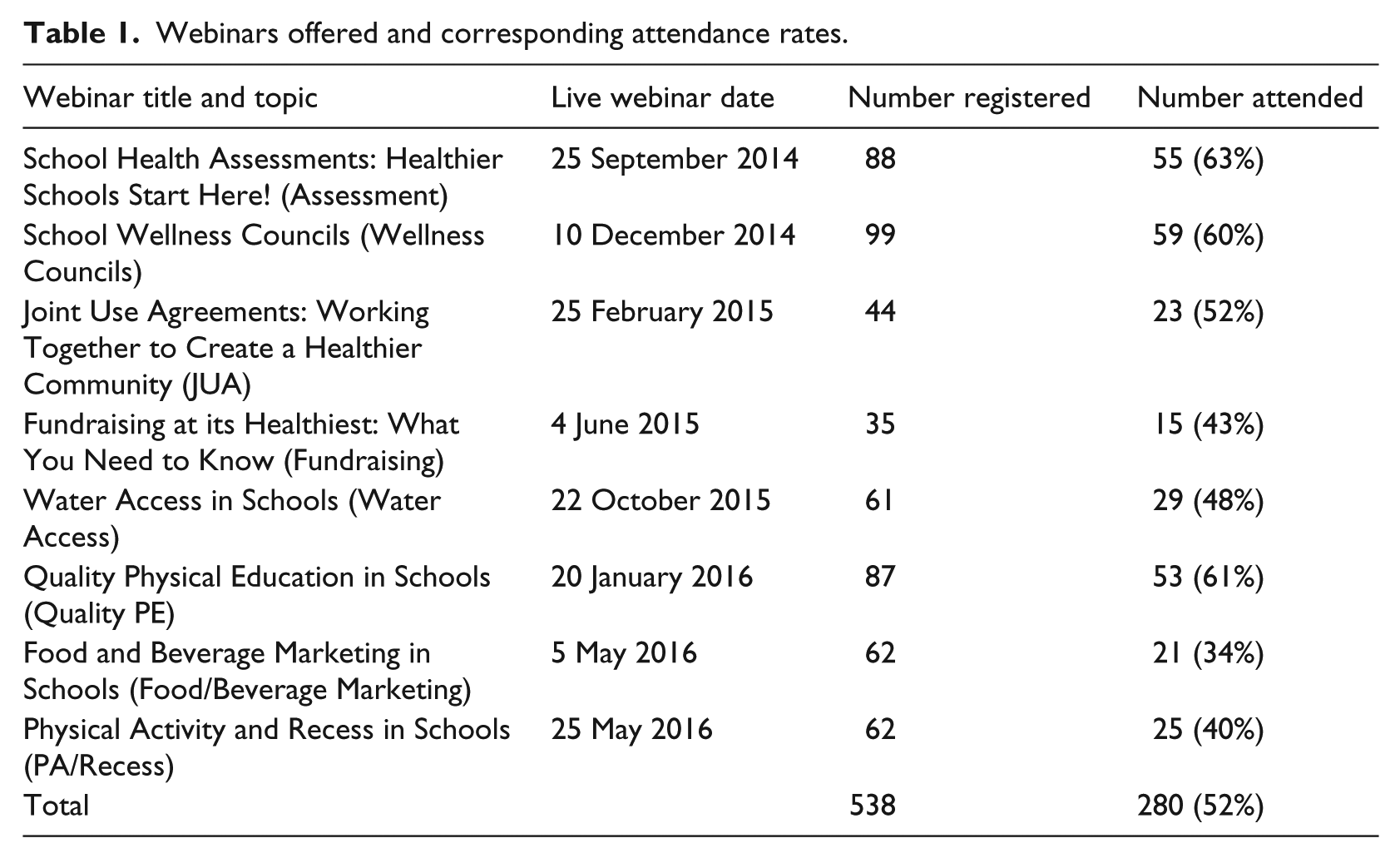
A series of eight webinars, defined for our purposes as informational sessions utilising expert speakers and engaging audience members through a web-based platform, were developed and offered to school personnel and stakeholders (i.e. parents, non-profit representatives) during the 2014–2015 and 2015–2016 school years. The webinars were designed to increase knowledge around strategies for enhancing school wellness environments (Table 1). Topics were selected based on the reported interests of school district professionals (data not published) and guidance provided through the Centers for Disease Control and Prevention (CDC) (Centers for Disease Control and Prevention, 2011) and the WSCC model (Lewallen et al., 2015). Each webinar began at 3:30 p.m. EST (after the school day) and was 30–60 minutes in length. Webinars featured content experts for the selected topics and were delivered using an online meeting software platform (GoToWebinar), selected for its wide array of available features.
Webinars offered and corresponding attendance rates.
Webinars were promoted to a Listserv comprising school professionals, community organisations, government agencies and private industry. In addition, an email Listserv, developed through the Pennsylvania Department of Education (2016) to deliver email messages to every school district, charter school, intermediate unit, vocational technical school/career and technology center in Pennsylvania, was utilised. Webinars were also promoted through the Penn State PRO Wellness social media pages and website. Promotion for each event began several weeks prior to the delivery date.
Participants were engaged throughout each webinar with polling questions, as well as a question and answer session at the end. Polls served a variety of purposes, including the opportunity for the webinar speakers to gain information about the audience’s prior knowledge of the topic, specific demographic information and current practices or policies in the participant’s school.
After each webinar, both attendees and registrants who did not attend received a follow-up email. Attendees were thanked for their participation, provided a certificate of completion and invited to participate in a post-webinar survey. Registrants who did not join the live webinar were provided a link to a recorded archived version of the webinar posted on the Penn State PRO Wellness website. Relevant resources were stored with the archived webinar and remain fully accessible to the public. 1
Data collection and analysis
Data on registrants and attendees were collected at several points. During registration, interested participants reported their name, email, school/organisation, school district and professional role in a school. Following webinar delivery, the webinar software generated registration-to-attendance conversion rates and attendee interest ratings, calculated by the average time a participant had the webinar application open as the primary window on their computer or device.
A post-webinar survey, distributed to all webinar attendees, captured (1) self-reported participant satisfaction with the webinar, (2) knowledge gained from participation, (3) intention to share information gained with a colleague and (4) intention to make wellness environment changes (i.e. conduct an assessment or create a wellness council). Attendee satisfaction was based on an average rating of the pace of delivery, content provided, adherence to objectives and application to the profession of the participant. Responses were rated using a 5-point Likert scale from poor (1) to excellent (5). Attendee knowledge increase was measured by asking respondents whether the webinar enhanced their understanding of the topic and was rated using a 5-point Likert scale from strongly disagree (1) to strongly agree (5). Both intent to share the information gained with a colleague and intent to make wellness environment changes were indicated using ‘yes’, ‘no’ or ‘not applicable’. The data on webinar attendance and engagement were analysed and presented descriptively using frequencies and associated percentages. Normally distributed data from the post-webinar survey were presented using the mean and standard deviation.
Results
Participation
Out of 538 individuals registered across the eight webinars, 280 attended the live event (52%). Overall, school nurses represented the largest group of attendees (25%), with teachers and administrators representing the next two largest groups of school professionals (21% and 18%, respectively). However, over the course of the series, webinar attendees represented a variety of professions (Figure 1).

Webinar attendees by profession (n = 280).
Individuals affiliated with a school made up the majority of webinar attendees (79%). However, participation among individuals not affiliated with a school included wide representation of community-based organisations (recreation authorities, YMCA), national professional public health organisations (CDC, American Academy of Pediatrics) and state departments of health (Idaho, California, Wisconsin, Pennsylvania, South Dakota).
Webinar attendee interest and attention
Overall, 52% of those who registered for a webinar attended the live event (highest 63%; lowest 34%) (Table 1). Attendees remained attentive 59% of the time (highest 68%; lowest 46% – data only available for seven of eight webinars). In addition, participation in live webinar polls ranged from 57% to 80% (data only available for seven of eight webinars).
Post-webinar survey
Of the 280 attendees who participated in the live webinar, 28% (n = 78) completed the post-webinar survey (Table 2). Respondents reported an average satisfaction of 3.9 out of 5.0 with the webinars. Webinars were also rated on their ability to increase knowledge in their respective topic area, with an average score of 4.3 out of 5.0 (Table 2).
Post-webinar evaluation: respondent’s satisfaction and knowledge change.
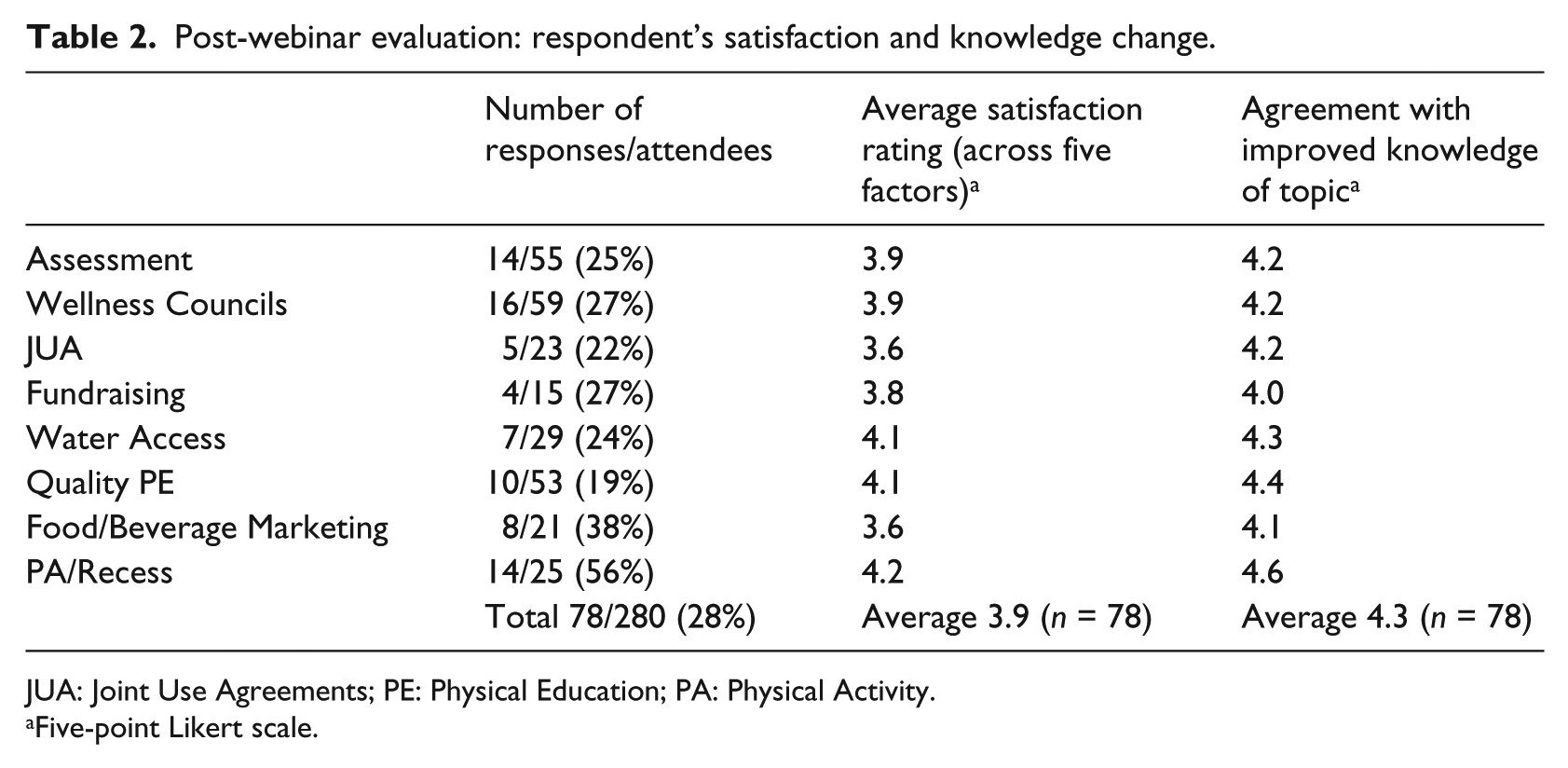
JUA: Joint Use Agreements; PE: Physical Education; PA: Physical Activity.
Five-point Likert scale.
Of the 78 (28%) post-webinar survey respondents, 73 (94%) indicated that sharing information with a colleague would be applicable to them (i.e. affiliated with a school). Of those 73 respondents, 95% (n = 69) indicated that they planned to do so. In addition, 59 (76%) post-webinar survey respondents indicated that creating wellness environment change (i.e. conducting an assessment, creating a wellness council) would be applicable to them (i.e. affiliated with a school). Of these 59 respondents, 83% (n = 49) intended to do so (Table 3).
Post-webinar evaluation: respondent’s intention to act on information gained.
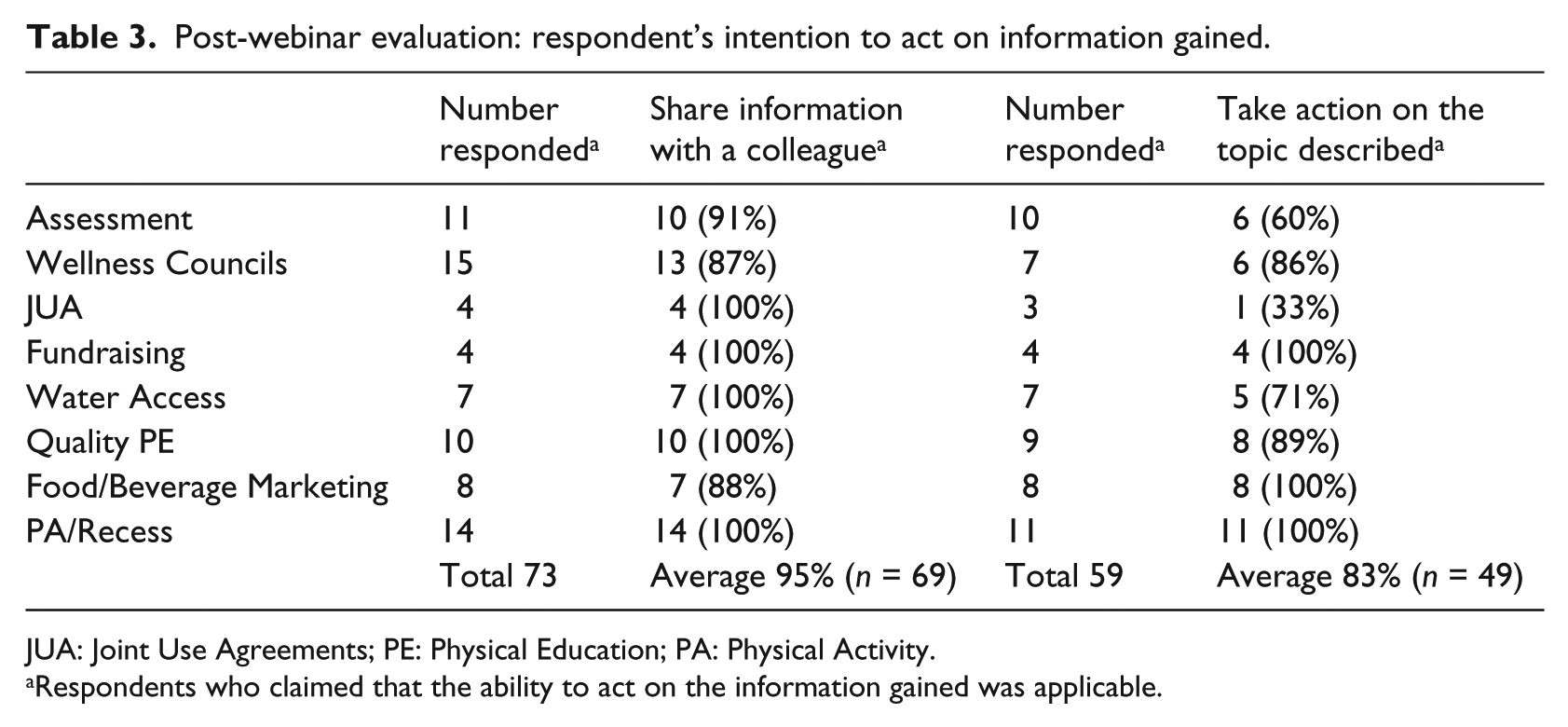
JUA: Joint Use Agreements; PE: Physical Education; PA: Physical Activity.
Respondents who claimed that the ability to act on the information gained was applicable.
Discussion
Data from the post-webinar evaluation survey indicate that this model of professional development is valuable for both increasing knowledge around school wellness topics and inciting motivation among participants, who may take action to improve wellness efforts in their respective school settings. On average, survey respondents agreed that the webinars were effective at increasing participant knowledge of the webinar topic area (4.3 out of 5.0), suggesting that webinars are a useful tool for increasing awareness of these important school health topics and strategies. In addition, 95% (n = 69) of the surveyed individuals who found it applicable indicated that they plan to share the information gained with a colleague, thereby increasing the reach of the initial live webinar. Most importantly, in the subgroup of participants that described it as applicable, 83% (n = 49) of respondents reported that they plan to take action through conducting an assessment, creating a wellness council, developing a joint use agreement, suggesting healthier food and beverage marketing or fundraising options, increasing water access in schools or improving physical education and physical activity opportunities. These findings demonstrate that short, informational training opportunities, like this webinar model, can serve as a catalyst for positive change in school wellness environments.
The need for professional development opportunities in areas of school wellness strategy is persistent in the literature (Agron et al., 2010; Centers for Disease Control and Prevention, 2011, 2014a, 2014b, 2014c; Murray et al., 2015). The WSCC model calls on higher education, philanthropic organisations and government agencies to utilise the framework to develop professional development opportunities for improving school health within the WSCC constructs (Lewallen et al., 2015). In addition, the CDC cites the need for continuing education across school professionals in a variety of health-related topics in the School Health Guidelines to Promote Healthy Eating and Physical Activity and their Bridging the Gap research briefs (Centers for Disease Control and Prevention, 2011, 2014a, 2014b, 2014c). With these calls to action, however, come barriers to implementation. The literature suggests that schools face many barriers to ensuring school professionals receive the training and education needed, including available time, cost of participation (i.e. substitutes, travel and registration) and competition for resources with other academic subjects (Agron et al., 2010; Anderson and Enge, 2012; Budd et al., 2009). Webinars are a useful model for meeting the education needs while overcoming many of the barriers that prohibit schools from meeting these recommendations. In support of this concept, our method of web-based professional development utilises a live, concise (30–60 minutes) and participant-engaging delivery, along with offering a publicly accessible archived version of the webinar on our organisation’s website1. In addition, relevant resources, guides, templates and contact information of content experts accompany each archived webinar. All webinars were offered free of charge to participants, eliminating the barrier of cost, both in terms of event registration and travel.
The literature reporting on the industry standard for webinar attendance suggests that it ranges from 30% to 45% (Britton, 2014; ON24 Inc., 2016). As evidenced by our webinar registration-to-attendance conversion rate of 52%, attentiveness and variety of school and wellness professionals that attended these webinars, it is clear that the topics offered are of interest to school wellness advocates, both inside and outside of the school walls. In addition, the attendance data suggest that different topics attract a different majority of these staff types. The school health assessment webinar, which described the importance of school wellness assessment along with how to conduct the assessment and use the resulting information, attracted a large proportion of school nurses. These data suggest that school nurses may be an audience that could serve as leaders within schools in the area of wellness assessment and may benefit from additional training opportunities in this respect (Kubik et al., 2007; Maughan et al., 2015; Schroeder et al., 2016). In addition, the school wellness council webinar, which described the purpose of a wellness council along with how to develop and sustain a council, had the largest number of participants. Interest in this topic is timely, due to the federal requirement of all schools that participate in the National School Lunch Program to develop or revise their Local Wellness Policy and implement a wellness council to ensure its implementation and regular revision (United States Department of Agriculture, 2016). These data suggest that everyone in the school setting should be considered for the role of wellness leader and call for school wellness resources that speak to the differing perspectives of teachers, school nurses and administrators, among others. This aligns with the body of literature that supports a coordinated approach to school wellness (Centers for Disease Control and Prevention, 2011; Lewallen et al., 2015).
The work outlined in this article is important in that (1) to our knowledge, it is the first study addressing a gap in the literature around the use of webinars as a professional development method for school health topics and (2) it is a response to the call to action for the use of professional development in making positive changes to the school wellness environment. In addition, the varied group of attendees, both school and community-based, indicates that this model and topics selected are valuable to a general audience. However, several limitations exist. First, the data collected on participants is limited and does not include standard demographic information, such as age, gender and race. Second, because the participant intention and knowledge data are only collected through the post-webinar survey with no baseline comparison, our ability to draw certain conclusions is limited. In the future, we plan to facilitate the collection of more post-programme surveys by only offering the certificate of completion to individuals who complete the survey. Finally, webinars as a mechanism for professional development are largely informational and therefore require motivation on the part of the participant to make change as a result of the information they acquire. However, our webinar methodology aims to encourage interaction both during the webinar, through polling and question and answer sessions, and after the webinar, through archiving each webinar recording on our website and accompanying it with applicable resources for taking the next step. A consideration for future web-based professional development offerings may be to incorporate technical assistance support as follow-up to participants, but this would need to be explored more fully.
Implications
The proposed model of developing and delivering webinars is a feasible option for increasing knowledge around school wellness improvement strategies and for motivating school professionals to initiate positive change in wellness environments by overcoming many of the barriers normally faced with professional development. Through this mechanism, we reached a variety of school professionals, suggesting that many different members within a school can be interested and motivated to learn and take initiative with strategies to improve the wellness environment, including areas such as wellness councils, assessing the school wellness environment and creating a healthier school and community culture through improving opportunities for nutrition, physical education and physical activity.
Footnotes
Acknowledgements
We thank the content experts who provided their time to speak throughout the webinar series. The authors also thank the Pennsylvania Department of Health for their support of Penn State PRO Wellness in the development and delivery of professional development opportunities for school-based personnel.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the State Public Health Actions to Prevent and Control Diabetes, Heart Disease, Obesity and Associated Risk Factors and Promote School Health cooperative agreement from the US Centers for Disease Control and Prevention. Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the US Centers for Disease Control and Prevention or the US Department of Health and Human Services.