
Abstract
Background:
The development of adolescent health literacy through school-based programmes is attracting international interest. However, there exist competing definitions, models and understandings of how these programmes should be conceptualised, implemented and evaluated. Australian Curriculum documents such as those relating to health and physical education currently focus on health literacy both in terms of learning outcomes and subject matter.
Objective:
This paper presents an evidence-informed framework for planning, implementing and evaluating health literacy school-based programmes and determining whether current Australian school-based health literacy programmes meet these guidelines.
Methods:
A systematic review was undertaken of PubMed, MEDLINE, PsycINFO, ERIC, ScienceDirect and the A+ Education databases. We included articles that had been published online or in print between 2010 and February 2017. We set limits on the earliest publication date to ensure we included those programmes designed to align with the health and physical education component of the Australian Curriculum and focused on health literacy outcomes.
Results:
Three studies were identified from a pool of 623 records. Two of the three studies had mental health literacy as the primary outcome. The third study more qualitatively assessed teachers’ and students’ perceptions of health literacy learning and whether these might have an impact on further health behaviour. Only one of the studies met the evidence-informed criteria.
Conclusion:
Recommendations are made for future school-based adolescent health literacy programmes. Producing an evidence-informed framework for enhancing adolescent health literacy through school-based programmes may enhance the future planning, implementation and assessment of adolescent health literacy in Australian secondary schools.
Introduction
In Australia, there is growing interest in adolescent health literacy and schooling, which intensified recently when health literacy was selected to underpin the recently developed Australian Curriculum for Health and Physical Education (Australian Curriculum Assessment and Reporting Authority [ACARA], 2013). Becoming so central to the recent shift from state- and territory-based health and physical education curriculum to a national curriculum requires us to consider how adolescent health literacy and schooling research has evolved over the previous three decades (Alfrey and Brown, 2013; Kilgour et al., 2015).
Macdonald (2013), the lead writer for the Australian Curriculum for Health and Physical Education, has argued that health literacy needs to be embedded in the new curriculum because of the limitations of the more uncritical approaches that have underpinned school health education in the past. She acknowledges, however, that a refocusing towards more socio-critical pedagogies will be challenging but important, citing the work of Kickbusch et al. (2005) who argue that health literacy provides a strategy for critical empowerment to increase people’s control over their health, their ability to seek out information and their ability to take responsibility.
The role of schools in promoting health is highlighted in the World Health Organization’s (WHO) (1999) Health Promoting Schools (HPS) framework. Through the opportunities they provide for contact with children and young people, schools provide a means of diffusing health information and fostering healthy lifestyles (International Union of Health Promotion & Education [IUHPE], 2009). Despite schools’ potential to enhance health literacy, there exists much debate about what this term means. Sørensen et al. (2012), for example, have identified 17 definitions of health literacy and 12 conceptual models. Given the burgeoning body of research on health literacy and schools, there is a need to review previous literature to identify a definition, conceptualisation and approach to promoting adolescent health literacy that is acceptable in Australian educational settings.
Definition and reconceptualisation of adolescent health literacy
Nutbeam (2000) argues that the aim of health literacy is to promote greater independence and empowerment rather than simply to convey information. As a construct, this implies that knowledge empowers young people to take responsibility for their health and supports their ability to seek help. This is especially important in adolescence when children transition into secondary school, often becoming more autonomous and requiring information about how to recognise health issues and where to go for health services (Blum and Nelson-Mmari, 2004).
Nutbeam (2000) suggests that health literacy can be organised into a three-level hierarchy, starting with basic elements (functional health literacy), progressing to skills (interactive health literacy), and then to capabilities to selectively access the broader health-related material critical for a community-focused level of understanding (critical health literacy). Recent research, however, has found that most school-based health literacy programmes focus on specific health risk behaviours and few provide learning opportunities for young peoples to develop a critical level of understanding (Benham-Deal and Hodges, 2009; Chinn, 2011; McCuaig et al., 2012, 2014; Sykes et al., 2013).
One approach to the development of critical health literacy is through an approach in which skills or capabilities are viewed as assets to be achieved (Nutbeam, 2008). In recent writing, Nutbeam’s (2008) describes health literacy as a learning outcome in the following terms: (1) it comprises a broad range of knowledge and competencies that people seek to encompass, evaluate, construct and use; and (2) through health literacy capabilities people become able to understand themselves, others and the world in a way that will enable them to make sound health decisions and to work on and change the factors that constitute their own and others’ health chances. Such action needs to be supported by the environment, the policies and processes in place, as well as people.
Within this framework, researchers and teachers are encouraged to recognise that health literacy learning takes place within the broader school context, rather than focusing solely on the health education classroom (Langford et al., 2015; Paakkari, 2015). In support of this, a framework for adolescent health literacy in schools has recently been developed from a critical analysis of health literacy practice, current health, health literacy and education theories and empirical research (Peralta et al., 2017). Three areas of focus emerged from the literature: namely, the importance of there being: (1) a focus on adolescent learning; (2) a commitment to building a health literate organisation informed by the HPS framework and/or by organisational school change, capacity and implementation theory; and (3) a concern to promote critical health literacy. These ideas have been elaborated to form a new conceptual framework (see Figure 1).
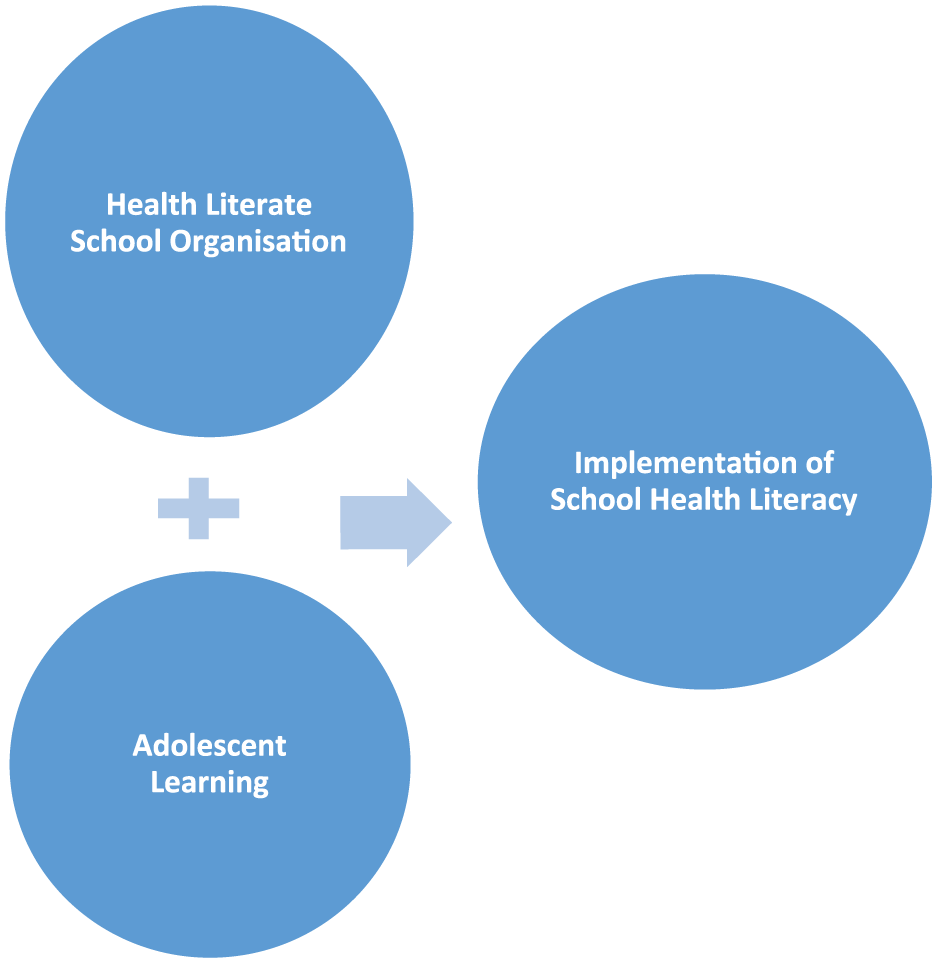
A framework for adolescent health literacy in schools.
During the process of conceptualising adolescent health literacy, it has become clear that there exists a major gap between the current implementation of health programmes in schools and the original HPS framework as a foundation for school health promotion and education (Langford et al., 2014, 2015).
Langford et al. (2014, 2015), for example, conducted a systematic review of 67 cluster randomised controlled trials, which targeted children and young people aged 4–18 years attending schools implementing health programmes which had made changes in all three domains of the HPS framework: (1) input to the curriculum; (2) changes to the school’s ethos or environment or both; and (3) engagement with families or communities or both. The review provided evidence that holistic school-based interventions such as those developed using the HPS framework can be effective in improving a number of health outcomes in students, especially body mass index (BMI), physical activity, physical fitness, fruit and vegetable intake, tobacco use and bullying. However, the review was unable to determine the impact of a holistic approach on other health outcomes such as alcohol and drug use, sexual health, violence and mental health.
In all, 56 of the studies included in Langford et al. (2015) review did not detail any educational or health literacy-related outcomes, or what we term the adolescent learning components of critical health literacy, capabilities and motivation in the conceptualisation of adolescent health literacy represented in Figure 1. Langford et al.’s (2014, 2015) review highlighted that within otherwise robust evaluations conducted using the HPS framework, educational impacts are rarely if ever described. It seems that research to date has largely been driven by health concerns, rather than those of schools, teachers and education researchers (Mohammadi et al., 2010; St Leger and Nutbeam, 2000). This is concerning as it underplays the importance of educational outcomes, including critical thinking, the development of capabilities and motivation for health behaviour change.
To be included in the review, interventions had to demonstrate effects in all three HPS domains. Langford et al. (2014, 2015) found that the family/community element of interventions appeared to be the weakest of the three domains. In almost half of the studies, activities to engage families were minimal, often involving newsletters, one-off meetings or family homework assignments. Only about one quarter of interventions attempted to involve local communities through, for example, media campaigns, neighbourhood health action teams or lobbying councils to improve neighbourhoods. Few studies provided details on what (if any) changes these family and community components brought about (Langford et al., 2014, 2015). This was unfortunate given that the influence of families (and the wider community, including media) on health-related knowledge, attitudes and behaviours can be profound (Garcia-Dominic et al., 2010; Hornby and Lafaele, 2011).
A whole-school approach requires commitment from schools in order to be effective (Langford et al., 2014, 2015). Several studies have highlighted the centrality of teachers and the importance of their knowledge and skills in ensuring that a whole-school approach is implemented appropriately (Midford et al., 2002; Mũkoma and Flisher, 2004; St Leger, 1998). This is more likely to occur if teachers can see the direct benefit to students and if teachers are supported to integrate health literacy efforts into the curriculum and whole-school efforts to improve health literacy outcomes. Support, resources and continuing professional development for teachers are important for this to occur. Health literacy outcomes can be further enhanced if schools work to become a health literate organisation (i.e. a system and organisation that provides the conditions for its members to be able to act upon newly developed health understandings; Kickbusch et al., 2013). Brach et al. (2012) have identified a number of attributes of health literate organisations. Most often, they are characterised by the following:
Leadership which makes health literacy integral to their mission, structure and operations;
Health literacy development which is integrated into planning, evaluation measures, service users’ safety and quality improvement;
Preparing the workforce to be health literate and monitoring progress;
Including populations served in the design, implementation and evaluation of health and related information and services;
Meeting the needs of populations with a range of health literacy skills while avoiding stigmatisation.
Knowing how schools function as health literate organisations and how school personnel can bring about change is essential for improving health literacy. Knowledge concerning implementation can help explain similarities and differences in health outcomes.
Attention to contextual factors has been stressed by Samdal and Rowling (2013) who articulate eight components for effective HPS implementation practice: (1) preparing and planning for school development; (2) policy and institutional anchoring; (3) professional development and learning; (4) leadership and management practices; (5) relational and organisational support context; (6) student participation; (7) partnerships and networking; and (8) sustainability. Overarching these eight components are three cross-cutting categories: (1) school leadership; (2) readiness for change; and (3) organisational facilitation of the change process (Samdal and Rowling, 2013).
Research argues for both structural and emotional support to achieve change, as well as the allocation of time and financial resources. These components need to guide practice in programmes and interventions to promote adolescent health literacy practice in schools.
Using the insights detailed above, we turn now to review Australian adolescent health literacy interventions and programmes to determine whether they are evidence-informed, demonstrating good practice, and aligned with Australian Curriculum for Health and Physical Education outcomes. To do this, we developed a checklist based on the research findings detailed above (Figure 2).
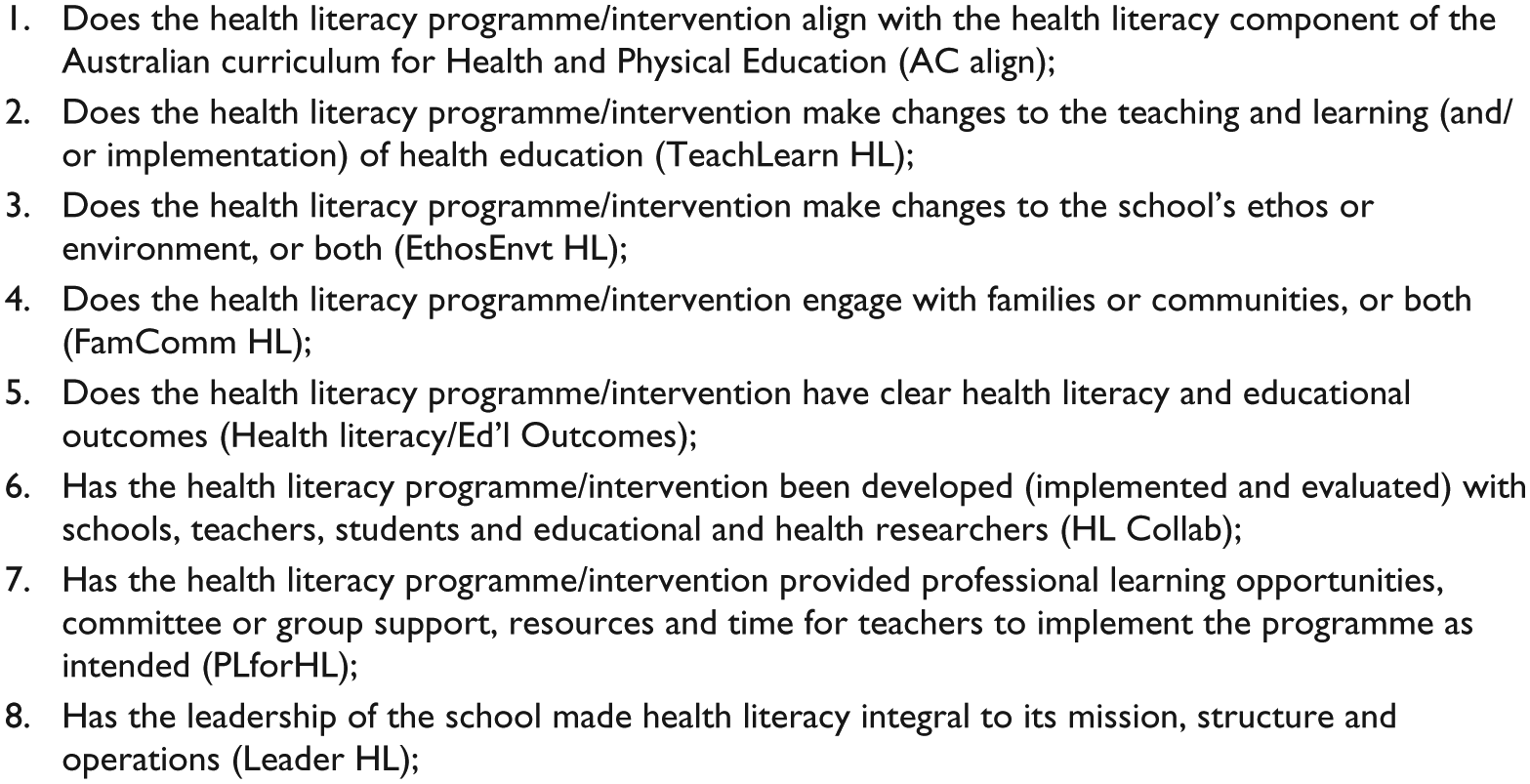
Checklist for adolescent health literacy.
Interestingly, four of the seven items in the checklist (items 4, 5, 6 and 7) concern implementation (i.e. the capabilities and motivation components of adolescent health literacy within our framework). These are critical elements of focus for intervention or programme designers and implementers.
Methods
Eligibility criteria
A systematic review was conducted to determine whether adolescent health literacy programmes/interventions in Australia align with the evidence-informed checklist (presented above). As the focus was on adolescent health literacy, studies that sampled students from classes in secondary schools (i.e. high school) were only included. Pre-school, primary school or post-secondary institution samples were excluded.
Included studies must have tested efforts to change usual teaching practices to improve adolescents’ health literacy, and therefore also needed to include a measure or assessment of health literacy. This could be a specific measure of health literacy assessed using questionnaire items (e.g. food literacy measured by a food literacy questionnaire) or qualitatively (e.g. by interviewing participants about their health literacy understandings), but could not be a health outcome measure (e.g. a measure of physical activity, sedentary behaviour).
We included English language, peer-reviewed articles (not abstracts) that reported on primary data and which had been published online or in print between 2010 and February 2017. We set limits on the earliest publication date to ensure we included actions, programmes and interventions designed to align with the new Australian Curriculum for Health and Physical Education.
Information sources and search
Our search strategy included the searching of online electronic bibliographic databases and targeted Internet searches using Google Scholar. The following online databases were searched, adapting search terms according to the requirements of individual databases in terms of subject heading and syntax: PubMed, MEDLINE, PsycINFO, ERIC, ScienceDirect and A+ Education.
The search terms were based on (1) participants (e.g. secondary school-age* OR secondary school-age* OR secondary student* OR high school student* OR secondary school* OR high school*), (2) outcomes (e.g. health literacy* OR ‘health literacy’), (3) strategies (e.g. intervention* OR programme* OR curricul*) and (4) locations (Australia*). Following these searches, we also inspected the reference lists of all included primary source articles.
Screening of citations
Duplicate citations were removed from the search by the lead author (L.R.P.). The abstract of each citation was reviewed to determine whether it would be included in the review. Citations that were deemed ineligible based on the study’s eligibility criteria were reviewed by the co-author (L.R.) to confirm the decision or otherwise. The full-text articles of all potentially relevant citations were obtained and saved as Adobe-PDF files.
Study selection
Eligible studies included qualitative syntheses. Due to the heterogeneity of aims, outcomes and measures used in the two quantitative studies, only descriptive analysis was conducted.
Data extraction
Data were extracted from the included studies by the lead author from full-text articles and placed in tabulated form (see Table 1). The data included the following:
Study authors;
Year of publication;
Australian state of study;
Study design;
Dominant theoretical framework used to inform study design;
Study sample (size, grade, mean age of participants);
Intervention length and stated alignment with the Australian Curriculum;
Health literacy/educational outcomes;
Whether the intervention was linked to additional health outcomes (e.g. depression);
Statistical significance (p-value/95% confidence interval [CI]) or qualitative results reported.
Australian-based studies examining school-based interventions aiming to promote adolescent health literacy.
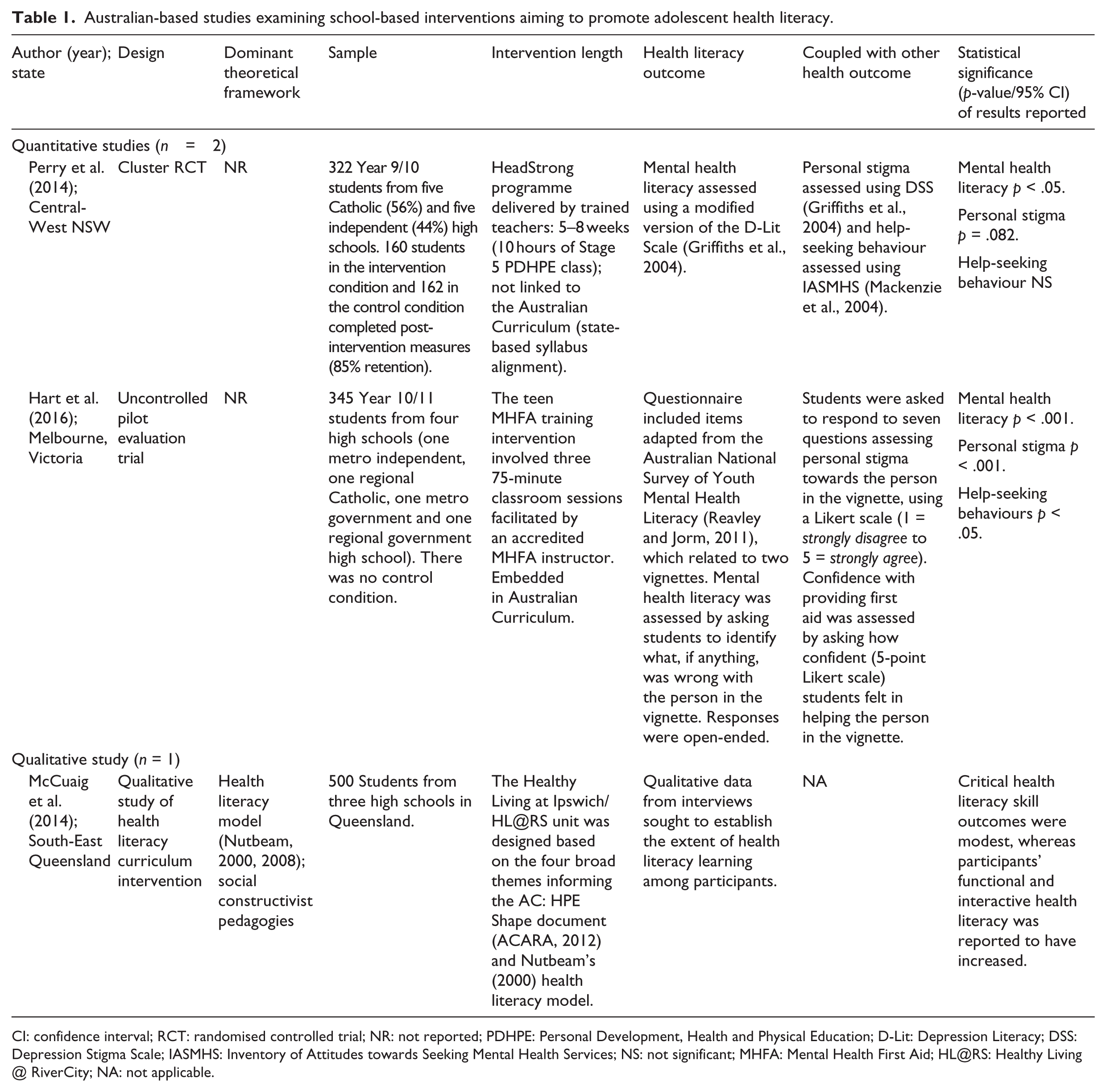
CI: confidence interval; RCT: randomised controlled trial; NR: not reported; PDHPE: Personal Development, Health and Physical Education; D-Lit: Depression Literacy; DSS: Depression Stigma Scale; IASMHS: Inventory of Attitudes towards Seeking Mental Health Services; NS: not significant; MHFA: Mental Health First Aid; HL@RS: Healthy Living @ RiverCity; NA: not applicable.
Results
Study selection
The titles and abstracts of an initial pool of 5,000+ records were screened. Due to the lack of health literacy studies included in the initial 5,000+ records, ‘health literacy’ was selected as a search term and the search was conducted again. This led to a pool of 623 records. The lead author screened the titles and abstracts of these papers and identified eight articles that made reference to adolescent health literacy. Four of these articles were excluded either because health literacy was not an outcome or they were not intervention studies. This left four articles that met the inclusion criteria. Two of these articles focused on the same study meaning that three unique studies could be included in our review (Figure 3).

Flowchart detailing study selection.
Study characteristics
Characteristics of the included studies are shown in Table 1. Selected studies were conducted in three different states of Australia: one in New South Wales, one in Victoria and one in Queensland. The study by Perry et al. (2014) involved 10 schools and used a cluster randomised controlled design, with randomisation at the class level. In all, 160 Year 9 and 10 students participated in the intervention condition, with 162 Year 9 and 10 students receiving the usual Personal Development, Health and Physical Education (PDHPE) curriculum as the control. The study by Hart et al. (2016) involved four schools and took the form of an uncontrolled pilot evaluation, with all consenting students (n = 345) in Years 9 and 10 participating in the intervention (Hart et al., 2016). The third study by McCuaig et al. (2014) was a qualitative investigation of three schools and the paper did not provide participant details.
Outcome measures
The two quantitative studies had mental health literacy as the primary outcome. Each used modified versions of questionnaires that had been found to be valid and reliable for their participant samples (Hart et al., 2016; Perry et al., 2014). In addition, the studies reported on two other mental health outcomes (i.e. personal stigma and help-seeking behaviours). These were assessed using different questionnaires.
The qualitative study measured teachers’ and students’ perceptions of health literacy learning and whether this had a perceived impact on further health behaviour (McCuaig et al., 2014). It used Nutbeam’s (2000, 2008) health literacy framework as the basis for asking teachers and students whether learning occurred at the functional, interactive or critical levels.
Definitions of health literacy
The three articles selected interpreted health literacy differently as evidenced in the varying theoretical frameworks underpinning programme design (or lack thereof) and the different measures of health literacy and educational outcomes.
Whole-school approach synthesis
Using the checklist for adolescent health literacy, the three studies were assessed according to the extent the programmes/interventions utilised a whole-school approach to the teaching of health literacy. The results can be seen in Table 2.
Use of whole-school approach to teaching adolescent health literacy.
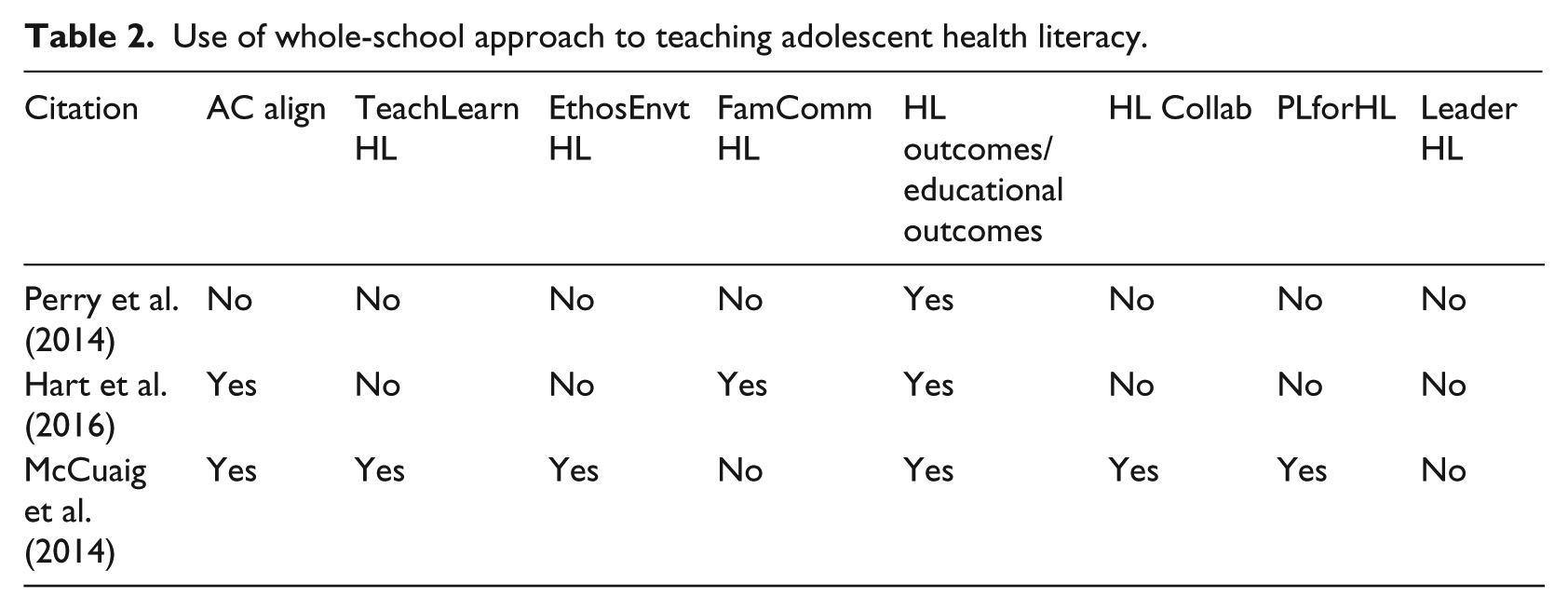
Of the three included papers, one study reported on the majority of the items in the whole-school action checklist (six of the eight checklist items; McCuaig et al., 2014). The two checklist items that were not evident in the study’s health literacy programme were clearly defined links with family and community (item 4) and leadership providing a framework for health literacy in all areas of the school (item 8). With respect to the family and community aspect, the study did include community-focused tasks in teaching, learning and assessment activities, but in the absence of direct community access and visits learning from these activities was somewhat limited.
In the other two studies, a smaller number of items in the Adolescent Health Checklist were satisfied: with Perry et al. (2014) study scoring on only one item out of eight (item 5) and Hart et al. (2016) scoring on three of eight items (items 1, 4 and 5). The absence of data in these papers demonstrative of whole-school action or a whole-school approach suggests that these interventions may have been missing key components essential for the development of health literacy in an educational context.
Discussion
This review has documented the existence of different understandings, definitions and concepts of adolescent health literacy in Australia. The two quantitative studies reported on focused on mental health literacy and measured similar health literacy outcomes (Hart et al., 2016; Perry et al., 2014). But in neither study did a clearly defined theoretical framework underpin the design of the health literacy programme and the outcome measures were different. Moreover, differences between these two studies make it impossible to reach firm conclusions concerning the nature of the interventions and their effects on mental health literacy. The third qualitative study used Nutbeam’s (2000, 2008) conceptualisation of health literacy to underpin the programme. Involving the use of socio-critical pedagogies across three dimensions of the HPS framework, the programme was viewed as acceptable by key stakeholders and showed modest self-reported gains in health literacy.
Given this diversity of understandings used in the three studies, it is important for future work to be more consistent in its approach to understanding and assessing changes in young people’s health literacy. One way forward might be to use the recent conceptualisation developed by Peralta et al. (2017), which builds on and incorporates some of the theories and frameworks most associated with health literacy (Nutbeam, 2000, 2008) within the context of the Australian Curriculum Health and Physical Education outcomes.
The Health Literacy for Adolescents checklist encourages school leadership to embed a concern for health literacy in the school mission, aims and policies so as to engage the school community. None of the studies in this review was able to harness this level of support and this may have limited health literacy learning. Other areas that school-based health literacy programmes/interventions should focus on include teacher professional learning, making changes to the school’s ethos and/or environment, engaging with families and/or communities and developing programmes in partnership with schools, teachers, students and educational and health researchers.
Teacher professional learning should be the cornerstone for future adolescent health literacy programmes, not only because of the paradigm shift expected of teachers by the writers of the Australian Curriculum for Health and Physical Education (Alfrey and Brown, 2013) but also because of the importance of professional learning for sustainable learning outcomes for students (Avalos, 2011). Engaging teachers in learning and collaboration with health experts will help overcome some of the current limitations associated with adolescent health literacy assessment. Ormshaw et al. (2013) review reported that studies that assessed health literacy via task-performance were more likely to measure health literacy than studies that assessed self-reported health literacy development.
Strengths and limitations
This is the first systematic review of programmes and interventions designed to increase adolescent health literacy in Australian secondary schools. The design and reporting of the review were guided by the PRISMA statement (Liberati et al., 2009); however, due to the small number of studies included and the different measures used, a meta-analysis could not be conducted.
It is of concern that only three studies met the inclusion criteria. Despite the developing literature on school-based health literacy, few studies have examined the short- and longer-term effects of actions, interventions and programmes, especially in Australia.
Studies included in this review used a variety of health literacy outcomes, teaching and learning strategies and assessment tools to assess health literacy. Future research may find it helpful to consider using a recent model of adolescent health literacy to guide the teaching and learning of health literacy (Peralta et al., 2017).
We also note that as additional studies emerge with the implementation of the Australian Curriculum: Health and Physical Education, it will be important to update this review.
Conclusion
Despite a burgeoning body of literature focusing on adolescent health literacy and school-based programmes, and the roll out of the Australian Curriculum for Health and Physical Education, the number of adolescent health literacy school-based programmes designed, implemented, evaluated and reported on in the peer-reviewed literature remains small.
Using evidence-informed practices, particularly the HPS framework, we reviewed three adolescent health literacy programmes. Only one study proved to be informed by the majority of evidence-informed practices, and even that was limited by the use of self-report data for the assessment of adolescent health literacy learning.
Recommendations for future school-based adolescent health literacy programmes include the use of the evidence-informed practices described in this review to inform larger-scale cluster-randomised controlled trials in which consistent framings of health literacy and consistent approaches to measurement are used (Ormshaw et al., 2013).