
Abstract
Objective:
To systematically review evidence for interventions to prevent early childhood caries (ECC) in Indigenous children in high-income countries.
Search strategy:
In November 2016, we searched Medline (from 1946), Embase (from 1980), the Cochrane Central Register of Controlled Trials (CENTRAL), PubMed (from 1996) and the Cumulative Index to Nursing and Allied Health Literature (CINAHL) (from 1982) for randomised and quasi-randomised controlled trials including children aged 0–5 years. Outcomes included the decayed, missing and filled teeth (dmft) index or similar index; the number of children with reported pain or emergency dental visits because of pain; the number of children referred for dental care; plaque scores; the amount of oral debris present; change in parent/carer attitude or knowledge towards baby teeth; reported regular dental visits and adverse outcomes. Two authors independently screened for inclusion and assessed the risk of bias.
Main results:
Four trials reported in five papers with 2,311 participants were included. Interventions were fluoride varnish with counselling/health promotion, chlorhexidine varnish, and motivational interviewing techniques plus oral hygiene materials and a dental examination. Two trials showed fluoride varnish applied biannually over a 2-year period reduced caries prevalence (mean difference [MD]: –3.00; 95% confidence interval [CI]: –4.94 to −1.06; MD: –2.47; 95% CI: –2.57 to −2.37). Motivational interviewing with oral hygiene materials and a dental examination can reduce the number of carious lesions in children aged 30 months (d2–4efs > 0 MD: –5.10; 95% CI: –8.74 to −1.46; d3–4efs > 0; MD: –4.40; 95% CI: –7.55 to −1.25).
Conclusion:
Fluoride varnish applied biannually over 2 years is effective at reducing ECC in Indigenous children. Motivational interviewing has some benefit in caries prevention. Further research is required to test other preventive programmes.
Introduction
Across the world, Indigenous children from high-income countries have a higher level of early childhood caries (ECC) than their non-Indigenous counterparts (Mathu-Muju et al., 2016; Schroth et al., 2009). In some countries, this gap is widening (Davies et al., 1997; Nash and Nagel, 2005). In Australia, oral health is improving in non-Indigenous children and adults but is deteriorating in Indigenous children and adults (Phelan et al., 2009; Slade et al., 2011). The reasons for health and oral health inequality between Indigenous and non-Indigenous people in the USA, Canada, Australia and New Zealand vary between countries and within each country. Common barriers to equality include the provision of culturally inappropriate, non-holistic dental services; inequality in service provision between metropolitan and rural areas; and social determinants, with social disadvantage being linked with an increased sugar intake, infrequent tooth brushing and reduced level of oral health (Mejia et al., 2010). In Australia, Indigenous Australians are recognised as a population priority group in the National Oral Health Plan 2015–2024 as young Indigenous children have unfavourable oral health outcomes and an increased likelihood for premature tooth extraction because of advanced dental caries (Council of Australian Governments Health Council, 2015).
Under current approaches, Australian Aboriginal children have two to three times the levels of decayed, missing and filled teeth (dmft) when compared with non-Aboriginal children, with 80% of Aboriginal preschool children having dental caries (Parker et al., 2010). Similarly, Maori children in New Zealand are three times more likely to experience dental decay (Schroth et al., 2009; Thomson, 1993). ECC is also a major health concern for Indigenous children in the USA (American Indian, Alaska Native) and Canada (First Nations, Inuit and Métis) (Canadian Paediatric Society et al., 2011). The dmft of Canadian Indigenous children ranges from 3.1 to 13.7 depending on the community involved (Lawrence et al., 2008), with ECC affecting 90% of children in Canadian Indigenous communities (Canadian Paediatric Society et al., 2011; Parker et al., 2010). The American Indian/Alaska Native child population has five times more dental caries than non-Indigenous children, and 68% of dental caries among the Indigenous children is not treated (Parker et al., 2010).
Dental caries is a dynamic process that results in the loss of hard tooth tissue following constant interaction between bacteria and fermentable carbohydrates (Featherstone, 2008). ECC can cause pain, infection and loss of sleep, and it can reduce the ability to learn (Gussy et al., 2006; Petersen and Kwan, 2011). Many Indigenous people live in regional or rural locations and have limited access to dental care (Australian Bureau of Statistics [ABS], 2016; Barnett et al., 2017; Martin-Iverson et al., 2000). In addition, Indigenous children living in remote areas have a higher prevalence of dental caries than those living near major cities (Smith et al., 2015a). Treatment is not without risk to the child as a general anaesthetic is commonly required. General anaesthetic rates are higher for children who are 4 years old or younger, of Indigenous heritage or living in a rural or remote area (Jamieson and Roberts-Thomson, 2006). Indigenous children are more likely to require a general anaesthetic for the treatment of severe dental caries than non-Indigenous children (Schroth et al., 2016). This may be due to the severity of the disease, geographic location and not having received dental treatment in a timely manner (Jamieson and Roberts-Thomson, 2006). Treatment under a general anaesthetic is not always easily accessible, is often associated with long waiting lists, is costly and carries the risk of serious adverse effects (Canadian Paediatric Society et al., 2011; Lawrence et al., 2008; Milnes et al., 1993). In New Zealand, twice as many Maori children require general anaesthetic for dental treatment compared with non-Indigenous children (Parker et al., 2010; Thomson, 1993). Some Aboriginal Medical Services offer a fly-in-fly-out dental service for culturally appropriate dental care; however, the focus of these services is on urgent treatment rather than the prevention of disease (Smith et al., 2007).
The evidence base for prevention of ECC in Indigenous children from high-income countries is uncoordinated and can be difficult for health professionals to access. Through this review, we hope to identify effective and culturally acceptable preventive measures that may help reduce the unacceptable inequality that exists between Indigenous and non-Indigenous children in high-income countries.
Objective
To systematically review the evidence for interventions to prevent ECC in Indigenous children from high-income countries.
Methods
The protocol for this systematic review has been published (Smith et al., 2015b) and registered with PROSPERO (ID CRD42016049391).
Criteria for selecting studies for this review
Types of studies
All randomised controlled trials (RCTs) and quasi-randomised trials (including cluster RCTs commonly used in health promotion research) of interventions for the prevention of ECC in Indigenous children from high-income countries.
Types of participant
Indigenous children aged 5 years and under at the time of study completion from high-income countries were eligible for inclusion. As advised by the World Health Organization (WHO), an inclusive definition of the term Indigenous was used (WHO, 2007). Countries categorised as ‘high income’ are those defined by the World Bank income category (WHO, 2014).
Types of settings
No limitations were applied.
Types of intervention
Any intervention intended to prevent dental caries was included. Studies evaluating interventions to treat dental disease, such as filling of cavities, were excluded.
Types of outcome measures
Primary outcome:
All outcomes related to caries prevalence; Number of children with reported pain or emergency dental visits because of pain; Number of children referred for dental care with or without general anaesthetic; Plaque scores and amount of oral debris present.
Secondary outcomes: Change in parent/carer attitude towards baby teeth; Change in parent/carer knowledge of oral health care of baby teeth; Reported regular dental visits; Adverse outcomes.
No limitations were applied to the outcome assessor as dental facilities in rural and remote areas are limited (Martin-Iverson et al., 2000) and the type of health professionals working within them is inconsistent.
Search methods for identification of studies
Electronic searches
An electronic search was undertaken using the following terms: Aboriginal, ‘First Nation’, Indigenous, child*, infant, toddler, ‘health promotion’, ‘oral health promotion’, ‘oral hygiene advice’, ‘diet advice’, ‘tooth brushing’, fluoride, fluoridation, prevention, sugar, sucrose, ‘bottle feeding’, ‘dental caries’, ‘dental decay’, ‘early childhood caries’, ‘nursing bottle caries’, ‘bottle caries’, ‘nursing caries’, ‘baby bottle caries’, ‘dmf index’, ‘dmft’, ‘dmfs’.
The following databases were searched up to November 2016:
MEDLINE (from January 1946);
Embase (from January 1980);
Cochrane Central Register of Controlled Trials (CENTRAL) (The Cochrane Library, latest issue);
PubMed (from January 1996);
Cumulative Index to Nursing and Allied Health Literature (CINAHL) (from 1982).
The MEDLINE search strategy (Appendix 1) was adapted for other databases. No language or publication restrictions were applied.
Searching other resources
The reference lists of all included studies were checked for other potential suitable trials. The first authors of included trials and known researchers in the field were contacted via e-mail to assist in identifying relevant unpublished and published trials.
Data collection and analysis
Selection of studies
Two authors (L.S. and F.H.) independently assessed the titles and abstracts of all trials identified by the search. The same authors then independently assessed for inclusion full-text copies of potentially relevant studies. Authorship and results were not masked. Disagreements were resolved by discussion. Corresponding authors of trials were contacted as required to provide information to determine eligibility.
Assessment of risk of bias in included studies
Two review authors (L.S. and F.H.) independently assessed risk of bias of included trials using criteria described in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins and Green, 2011).
Data extraction and management
One review author (L.S.) extracted data from published reports using standardised, pilot-tested forms, and a second review author (F.H.) checked all extracted data. Study authors were contacted as necessary to provide missing information.
Analysis
Continuous data were analysed using mean differences (MDs) and 95% confidence intervals (CIs). Dichotomous data were analysed using odds ratios (ORs) and 95% CI. All included studies reported sufficient data for analysis. The Cochrane statistical package Review Manager 5 (RevMan 5, 2008) was used for statistical analyses. Data were entered by F.H. and checked by L.S.
Results
Selection of studies
Study selection is summarised in Figure 1. Electronic searches retrieved a total of 280 citations. A total of 54 trials were identified as potentially relevant, and 47 studies were excluded after reading the full text (Table 1).

PRISMA diagram – showing the location of papers at each stage of the systematic review process.
Reason for exclusion of studies from the review.
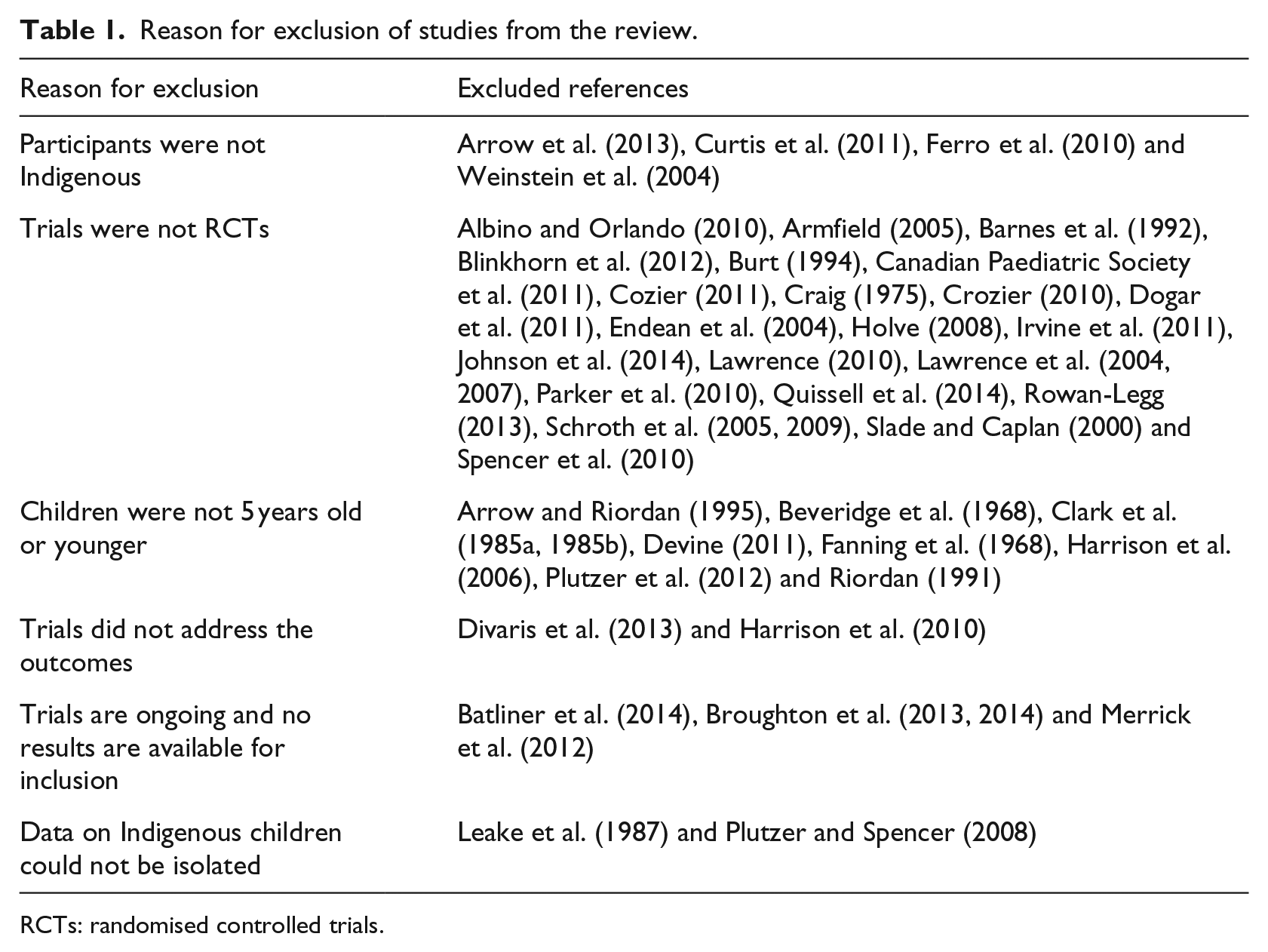
RCTs: randomised controlled trials.
Reasons for exclusion were: participants were not Indigenous, trials were not RCTs, children were not 5 years old or younger, trials did not address the outcomes and trials were ongoing and no results were available for inclusion.
The authors of two papers were emailed to isolate the data of Indigenous children. Both trials were excluded because this information was not provided (Leake et al., 1987; Plutzer and Spencer, 2008). In response to emails to known researchers in the field, no additional potentially relevant papers were identified.
Included studies
Five trials with 2,311 participants were included: two trials assessed caries increment with fluoride varnish with counselling/health promotion (1,703 participants) (Lawrence et al., 2008; Slade et al., 2011); one assessed caries increment through a chlorhexidine varnish (367 participants) (Robertson et al., 2013); and one assessed caries increment using motivational interviewing techniques plus oral hygiene materials (241 participants) (Harrison et al., 2012). The oral hygiene materials related to oral hygiene, dietary advice and access to a dentist for an examination (Harrison et al., 2012). One paper (Roberts-Thomson et al., 2010) was a secondary analysis of an included paper (Slade et al., 2011) and assessed change in parent/carer knowledge and attitude with health promotion. For ease of interpretation, the two papers reporting on the one trial will be referred to as one study.
The primary outcome of four trials was dental caries (Harrison et al., 2012; Lawrence et al., 2008; Robertson et al., 2013; Slade et al., 2011). Two trials (Lawrence et al., 2008; Slade et al., 2011) used the dmft index or a variation of this index, one used the number of new carious surfaces (NNCS) (Robertson et al., 2013) and one trial (Harrison et al., 2012) used caries diagnostic methods similar to Pitts and Fyffe (1988). This diagnostic method and the NNCS were not anticipated when the protocol for the systematic review was drafted but were included due to their similarity to other included outcomes.
All included trials were RCTs. Three trials were cluster-randomised (Harrison et al., 2012; Lawrence et al., 2008; Slade et al., 2011) and one was individual participant–randomised (Robertson et al., 2013). All trials were published in the English language in peer-reviewed journals between 2008 and 2012. Characteristics of included studies are summarised in Table 2.
Characteristics of included studies.
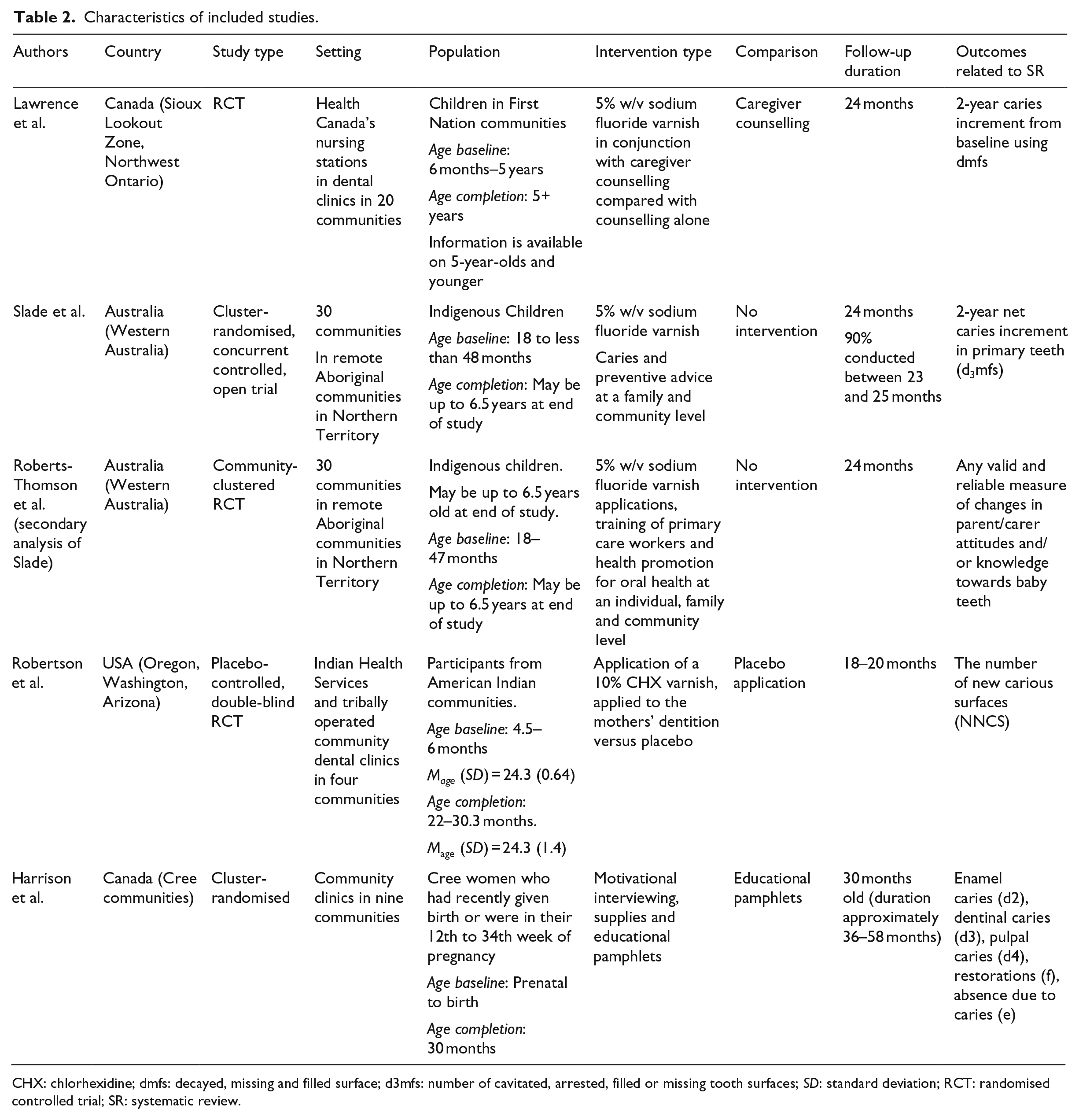
CHX: chlorhexidine; dmfs: decayed, missing and filled surface; d3mfs: number of cavitated, arrested, filled or missing tooth surfaces; SD: standard deviation; RCT: randomised controlled trial; SR: systematic review.
Risk of bias of included studies is summarised in Table 3. Only one trial blinded participants to the intervention (Robertson et al., 2013). This was achieved using active and placebo products. Using the Cochrane summary ranking, three trials received a high summary ranking for overall risk of bias (Harrison et al., 2012; Lawrence et al., 2008; Slade et al., 2011). This was primarily due to the lack of blinding, personnel and outcome assessors. One study received a low-risk summary ranking mainly due to its allocation concealment and blinding of participants, personnel and outcome assessors (Robertson et al., 2013).
Summary of risk of bias in the selected studies.

‘✓’ denotes low risk of bias; ‘X’ denotes high risk of bias; ‘?’ denotes unclear risk of bias.
Effectiveness of interventions
Results are presented in this section and summarised in Table 4.
Effectiveness of interventions.
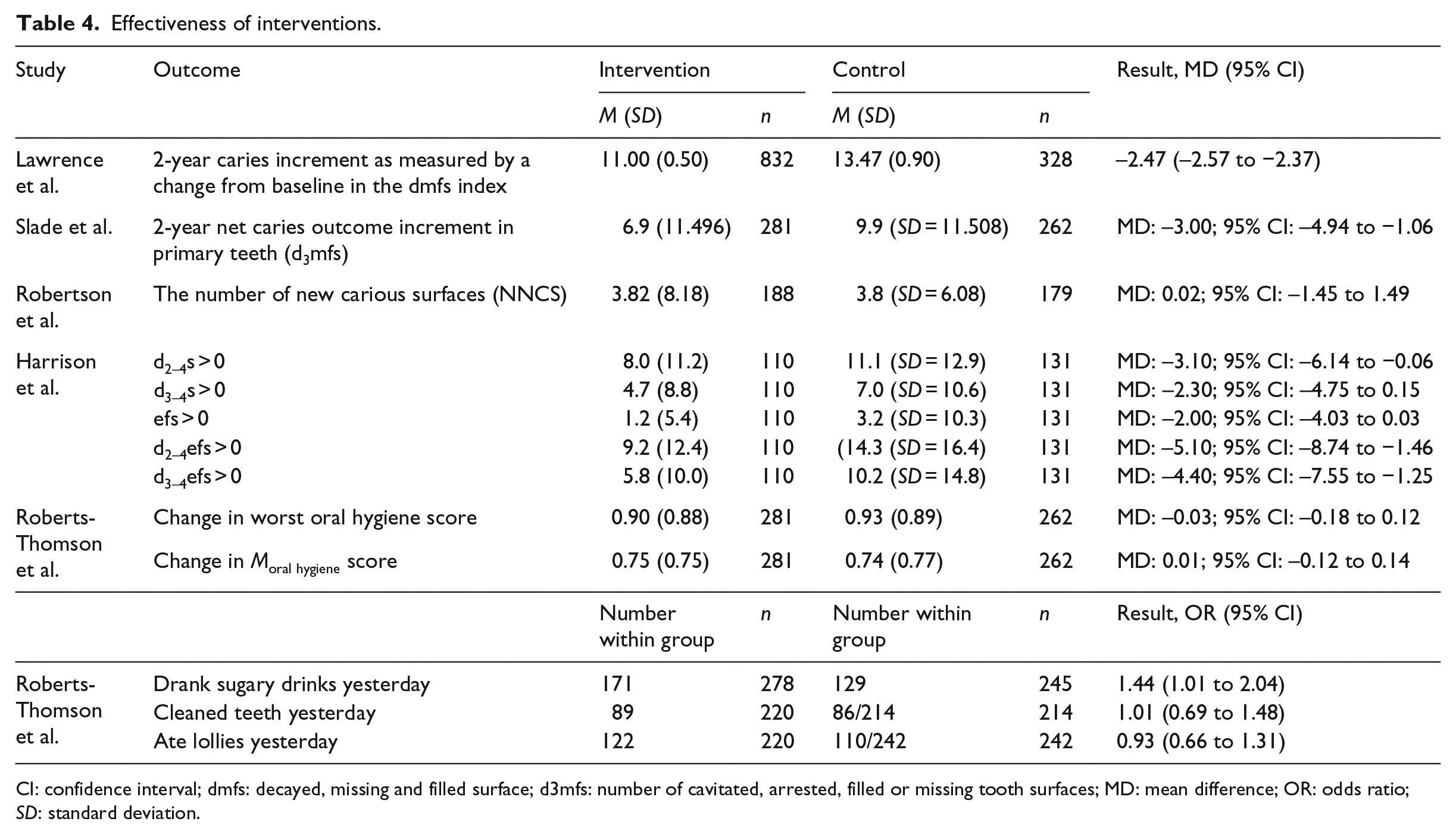
CI: confidence interval; dmfs: decayed, missing and filled surface; d3mfs: number of cavitated, arrested, filled or missing tooth surfaces; MD: mean difference; OR: odds ratio; SD: standard deviation.
Caries increment with fluoride varnish with counselling/health promotion
Two studies (Lawrence et al., 2008; Slade et al., 2011) aimed to reduce caries increment with the use of fluoride varnish and counselling or health promotion. Slade et al., (2011) applied Duraphat fluoride varnish (5% w/v sodium fluoride varnish) twice yearly for 2 years in addition to caries preventive advice at a family and community level. The control group received no intervention. The 2-year net caries outcome increment in primary teeth was assessed using the number of cavitated, arrested, filled or missing tooth surfaces (d3mfs) index (Slade et al., 2011). The MD in d3mfs index scores after 2 years was statistically significant in favour of fluoride varnish (MD: –3.00; 95% CI:–4.94 to −1.06).
Lawrence et al., (2008) assessed fluoride varnish with caregiver counselling compared with counselling alone. The 2-year caries increment was assessed using the decayed, missing and filled surfaces (dmfs) index. Duraflor fluoride varnish (5% w/v sodium fluoride varnish) was applied at baseline and at 4- to 6-month intervals. Caregiver counselling was provided at baseline and at 12- and 24-month visits for both control and intervention groups. The MD in dmfs index scores after 2 years was statistically significant in favour of fluoride varnish (MD: –2.47; 95% CI: –2.57 to −2.37).
Change in parent/carer knowledge and attitude with health promotion
One study evaluated oral health behaviours of Aboriginal children following a community-oriented health care intervention, including fluoride application (Roberts-Thomson et al., 2010). This study was a secondary analysis of another included paper (Slade et al., 2011). At follow-up examination, 61.5% (171/278) of children in the intervention group ‘drank sugary drinks yesterday’ compared to 52.5% (129/245) in the control group. This difference was statistically significant (OR: 1.44; 95% CI: 1.01 to 2.04).
There was no statistically significant difference between the intervention group and control group when comparing ‘cleaned teeth yesterday’ and ‘ate lollies yesterday’ (the mean of ‘change in worse oral hygiene score’ or ‘change in mean oral hygiene score’ (Table 3). There was little change in oral health behaviours between the intervention and control groups.
Caries increment with chlorhexidine varnish application
One intervention aimed to reduce the caries increment through a chlorhexidine varnish application (Robertson et al., 2013). Mothers received four weekly applications of the treatment (placebo or chlorhexidine) and a single application when their child was 12, 18 and 24 months old.
From the children included in the intention-to-treat analysis, the difference in mean NNCS at the final oral examination between groups was not statistically significant (MD: 0.02; 95% CI: –1.45 to 1.49).
Caries increment with motivational interviewing plus oral hygiene materials and dental examination
One included study aimed to reduce the caries increment through maternal counselling using motivational interviewing techniques plus access to oral hygiene materials and a dental examination. Mothers in the control communities received pamphlets, while those in test communities received pamphlets and up to seven motivational interviewing sessions. Mothers in the test group had access to oral hygiene materials and dental care (Harrison et al., 2012). The 2-year caries increment was assessed using enamel caries (d2 = substance loss), dentinal caries (d3), pulpal caries (d4), restoration (f) and absence due to caries (e). The MD in dental caries outcomes at a tooth surface level was statistically different for d2–4efs > 0 (MD: –5.10; 95% CI: –8.74 to −1.46) and d3–4efs > 0 (MD: –4.40; 95% CI: –7.55 to −1.25). The MD in dental caries outcomes at a tooth surface level was not statistically different for d2–4S > 0 (MD: –3.10; 95% CI: –6.14 to 0.06), d3–4S > 0 (MD: –2.30; 95% CI: –4.75 to 0.15) and efs > 0 (MD: –2.00; 95% CI: –4.3 to 0.03).
Discussion
There is evidence from two RCTs that the application of fluoride varnish reduces caries prevalence over a 2-year period in young Indigenous children. There is no evidence that chlorhexidine varnish when applied to mothers and infants reduces NNCS.
Evidence suggests that motivational interviewing plus oral hygiene materials with a dental examination reduces caries increment (Harrison et al., 2012). At 30 months, significant differences were noted between the intervention and control groups for d2–4efs > 0 and d3–4efs > 0. When analysed separately, differences in d3–4S > 0 and efs > 0 between groups were not statistically significant, but when pooled to d3–4efs > 0, the difference between groups was statistically significant, indicating that the individual analyses were likely underpowered to detect a significant effect. The specific oral hygiene materials provided to parents and children in addition to the motivational interviewing were not reported in the original study (Harrison et al., 2012).
There is limited evidence from one RCT that health promotion in combination with fluoride application can after 2 years reduce the consumption of sugary drinks but does not change other health behaviours, such as cleaning teeth and eating lollies. There is no evidence of adverse effects or that health promotion in combination with fluoride application improves the mean oral hygiene score after 2 years.
These findings are valuable when introducing preventive interventions to Indigenous children in high-income countries. Due to the severity of the disease and high prevalence of dental caries among Indigenous children, prevention is of high importance. Challenges faced by Indigenous children include pain, infection and limited access to timely dental care. Many Aboriginal families do not have regular contact with dental professionals, so introducing these findings on a larger scale to include Aboriginal Health Workers may be valuable. Involving Aboriginal Health Workers and Indigenous Health Services may help address barriers to accessing dental care. Common barriers experienced by Indigenous people from high-income countries include cost, accessibility and culturally considerate care (Ou et al., 2010; Stuart et al., 2011). In addition to preventing ECC in Indigenous children, a multi-level and sustainable approach is needed to address health inequalities experienced by approximately 370 million Indigenous people worldwide (Mejia et al., 2010; US Department of Health and Human Services [USDHHS], 2000).
This review highlights the paucity of RCTs relating to the prevention of ECC in Indigenous children from high-income countries. No trials evaluated fluoride in toothpaste, which is convenient and accessible for the prevention of dental caries within communities. This review is limited to RCTs and quasi-randomised trials. Health professionals must rely on lesser forms of evidence to inform their use of interventions that have not been evaluated in RCT. No trials were conducted in New Zealand, where it is known that Maori children have an increased prevalence and more severe dental caries than non-Maori children (Parker et al., 2010). Given that Aboriginal children living in high-income countries suffer high levels of caries, it is surprising that there are limited high-quality RCTs or quasi-randomised controlled trials to help these communities. Due to the shortage of dental facilities in remote areas, further good quality trials that aim to prevent ECC in Indigenous children through methods that do not require dental professionals may be of value. Although fluoride varnish is effective at reducing the prevalence of dental caries, legislation is not standardised so as to allow all Aboriginal Health Workers to apply this product.
Conclusion
Fluoride varnish applied at 6-monthly intervals and motivational interviewing plus oral hygiene materials with a dental examination are beneficial in reducing dental caries in young Indigenous children in high-income countries. The effectiveness of other tested interventions appears to be limited or have no clear benefit. Further research is needed to explore alternative culturally acceptable methods to prevent dental caries.
Footnotes
Appendix
Acknowledgements
This paper represents the views of the authors and not those of the Australian National Health and Medical Research Council or the New South Wales Dental Council. All authors conceived of the idea of the study and drafted the background. L.S. and F.H. completed the search, analysis and discussion. All of the authors approved the final manuscript.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by a grant from the Australian National Health and Medical Research Council (GNT1030546).