
Abstract
Objective:
Perceived self-efficacy (PSE) is considered a foundation for effective self-care in the context of chronic disease and illness. In order to improve patient and caregiver knowledge about self-care in B-cell non-Hodgkin’s lymphoma (NHL), we designed and delivered an online, patient-focused education activity. Educational impact on PSE was evaluated using a mixed quantitative/qualitative methodology. We report here on the qualitative characteristics of self-efficacy.
Methods:
We interviewed participants using open-ended questions based on a semi-structured interview guide. Interviews were audio-recorded and transcribed verbatim, and analysed using constant comparative method with software support (NVivo for Mac 11, QSR International).
Results:
In all, 12 people diagnosed with B-cell NHL were interviewed. Descriptive analysis showed that participants were able to summarise key education messages about B-cell NHL presented in the programme. Key themes linked to self-care knowledge and practice included normalisation of self-care, learning the hard way, everyone is different and being prepared. Participants described four key strategies linked to the notion of ‘being prepared’: (1) asking questions, (2) building relationships with oncologists, (3) developing/maintaining a philosophy of life, and (4) connecting with others. These themes provide context for the experience of PSE and may also reflect beliefs that have implications for self-efficacy education.
Conclusions:
Interview data affirm PSE as a foundation of self-care and identify beliefs underpinning PSE. A dominant belief of ‘being prepared’ was sustained by four strategies that education content reinforced. Educators can use these insights to strengthen self-efficacy education interventions for patients with B-cell NHL and other types of cancer.
Keywords
Background
B-cell non-Hodgkin’s lymphoma (NHL) is a haematological disease with several subtypes and a potentially chronic trajectory. Treatment depends upon the particular subtype, as well as stage of the disease, and includes involved-site radiotherapy, chemotherapy, targeted therapies, and active surveillance (American Cancer Society, 2017). While targeted therapies have improved prognosis, and patients may live with their disease for several years, patients receiving a diagnosis of B-cell NHL suffer from significant distress and poor quality of life, and require considerable supportive care and education on the implications of their disease for treatment, treatment-related side effects, and self-care (Mols et al., 2007; Oerlemans et al., 2011; Smith et al., 2013). Self-care education is becoming increasingly necessary as many types of cancer, including B-cell NHL, evolve into chronic conditions for which patients need extensive management over years or even decades (American Cancer Society, 2016). Yet such education for patients with B-cell NHL is currently limited in availability and scope. Indeed, a recent Dutch survey found that up to 43% of patients with NHL lack credible information about diagnostic testing and treatment options, and 39% felt there was a lack of guidance and support (Stienen et al., 2014).
The available evidence suggests that education on self-care strategies, such as communicating with health professionals, goal-setting, and problem-solving, can help to reduce uncertainty for patients, foster a sense of control over the experience of living with cancer, and buttress self-efficacy (e.g. Boger et al., 2015; Kidd et al., 2009; McCorkle et al., 2011; Porter et al., 2008). Self-efficacy is a core psychological concept used to predict and explain people’s motivations to take up particular health behaviours, such as self-care. In models of behaviour change (e.g. the Transtheoretical Stages of Change Theory; Prochaska and DiClemente (1982)), self-efficacy presumes rational action (Fishbein and Ajzen, 1975), and is typically measured as a predictor of future behaviour following exposure to an educational programme or activity (Peterson, 2006). In the context of health and illness, these theories posit that learning, action, and behaviour change are influenced by self-beliefs derived from interactions between personal, environmental or situational and behavioural determinants.
Perceived self-efficacy (PSE) is a corollary of self-efficacy that is considered a mediator between the act or process of learning and the implementation of new knowledge or skills in a health context (Williams et al., 2015). PSE refers to ‘beliefs in one’s capabilities to organise and execute the courses of action required to manage prospective situations’ (Burke et al., 2009), which are influenced by a range of behaviours, environmental factors and personal/cognitive characteristics (Prochaska and DiClemente, 1982). Four sources of information are deemed especially crucial in the formation of PSE beliefs: (1) previous performance or mastery experiences, (2) vicarious experiences from observation and social comparison, (3) social persuasion (e.g. education messages) and (4) experiences arising from physical and emotional states (e.g. anxiety). Positive experiences related to each of these areas are believed to increase the likelihood of high levels of PSE (Peterson, 2006).
In order to support self-efficacy for patients living with B-cell NHL, PlatformQ Health Education, LLC (PQH), in conjunction with the Leukemia and Lymphoma Society (LLS) and the University of Nebraska Medical Centre (UNMC), launched an online patient and caregiver-centric video programme to improve knowledge about B-cell NHL and offer strategies to enhance quality of life through better disease and side effect management. We evaluated the impact of this education on knowledge and self-efficacy via a mixed methods outcomes methodology. Following the quantitative measurement of knowledge uptake, we also explored the impact of the educational intervention on knowledge about and perspectives on B-cell NHL self-care and self-efficacy via qualitative interviews with education participants. Here, we report on characteristics of self-efficacy that emerged in analysis of qualitative outcomes.
Methods
Patient education programme design, delivery and evaluation of knowledge uptake
The education programme, Patient Education on B-Cell Non-Hodgkin Lymphomas from Diagnosis to Treatment, consisted of one 60-minute session with 4 parts, each of which could be viewed in its entirety or separately on http://www.cancercoachlive.com/. Programme design was directed by findings from a comprehensive needs assessment that identified specific gaps in patient and caregiver knowledge about B-cell NHL. The programme featured insights from multiple sources and patient vignettes and provided participants with a range of resources such as fact sheets and web links to support organisations. The web-based activity was initially launched live and online on 4 August 2016, and was available on-demand for one year. The sessions were filmed in a production studio with three faculty-panel members – an oncologist from the University of Nebraska Medical Centre, the Executive Director of the Leukaemia and Lymphoma Society, and a nurse practitioner from the Dana-Farber Cancer Institute, Boston, Massachussetts – who discussed the following topics:
Understanding the diagnosis. What does it mean to have B-cell NHL?
The work-up. What tests to expect for B-Cell NHLs;
Treating B-cell NHLs;
What to do between doctor visits and treatments. Self-care, resources.
Patient participants were able to submit questions before and during the live programme, and faculty answered a sampling of these questions throughout the 4 sessions. Live polling questions regarding social support, treatment concerns and other relevant topics were also interspersed with faculty discussions and question responses and integrated into the discussion flow. In total, 535 learners participated in the educational programme on cancercoachlive.com, and an additional 26,174 viewed the programme via social media channels (25,166 on Facebook and 1,008 on the Leukaemia & Lymphoma Society YouTube Channel).
We evaluated trends in knowledge uptake associated with programme participation using Moore et al.’s seven-level evaluation framework (Moore et al., 2015), up to outcomes level 6 (patient impact). The goal of the outcomes plan was to (1) assess the degree to which the proposed initiative facilitated positive knowledge and behaviour change, (2) assess the degree to which the proposed initiative facilitated positive health-related self-efficacy and (3) gather information to help inform and guide future education in this therapeutic area. We measured trends in knowledge uptake via pre- and post-test online surveys that were administered to all activity participants before and immediately following programme completion, as well as via an online follow-up survey distributed within 8 weeks of the activity completion date.
Exploring patient knowledge of and perspectives on self-care
Qualitative data collection and analysis
In addition to quantitative evaluation of knowledge outcomes, we explored the impact of the educational intervention on knowledge about and perspectives on B-cell NHL self-care and self-efficacy via qualitative interviews with education participants
We recruited potential interview participants 6–10 weeks following activity participation via email. Participants were eligible to participate in interviews if they had (1) a confirmed diagnosis of B-cell NHL, (2) currently resided in the USA and (3) recalled viewing the education programme. We determined this eligibility via an invitation and screener emailed to programme participants. Those who did not meet the inclusion criteria were not invited to participate in interviews. When screening for potential interviewees began, 183 participants had completed the education activity (13 September 2016) and 37 responded to interview invitations. Of these 37 invitation respondents, 15 were eligible as per inclusion criteria and 3 did not respond to scheduling information. A small honorarium was offered for completing an interview.
The interview topic guide (online supplementary file) was designed to explore patient understandings of B-cell NHL symptoms, tests at diagnosis, treatment options and treatment-related side effects, and self-care strategies via open-ended questions. One of the authors (A.H.), a PhD-level trained medical sociologist, conducted these confidential, 30- to 45-minute telephone interviews, which were scheduled at convenient times for participants. Western Institutional Review Board granted ethical approval for the study, and we obtained informed consent from all participants prior to interviews. None of the participants were personally known to the authors.
We audio-recorded interviews via cloud-based, web-conferencing software (ww.uberconference.com), transcribed interviews verbatim and imported them into NVivo for Mac (QSR International), a software package designed to support systematic analysis of unstructured data. We used a process of constant comparison to structure analysis of participant responses to questions both across interviews and within interviews (Corbin and Strauss, 2015). This approach included three components: (1) data immersion and familiarisation, (2) descriptive data coding and (3) thematic coding (Saldaña, 2013). One of the authors (A.H.) initially coded transcript content into descriptive categories that broadly followed the structure and focus of the interview categories concerning the education activity impact on self-reported knowledge and behaviour. Following descriptive coding, a second round of coding identified themes across the dataset until thematic saturation was achieved. These themes were further explored for connections and relationships (Roller and Lavrakas, 2015). The principal investigator (W.T.) corroborated the analysis to ensure it reflected the study aim, which, as stated above, was to explore the impact of the educational intervention on knowledge about and perspectives on B-cell NHL self-care and self-efficacy.
Findings
Descriptive analysis: education impact on knowledge
We interviewed 12 people with a diagnosis of B-cell NHL, aged between 43 and 78 years, with a mean age of 60 years (Figures 1 and 2).
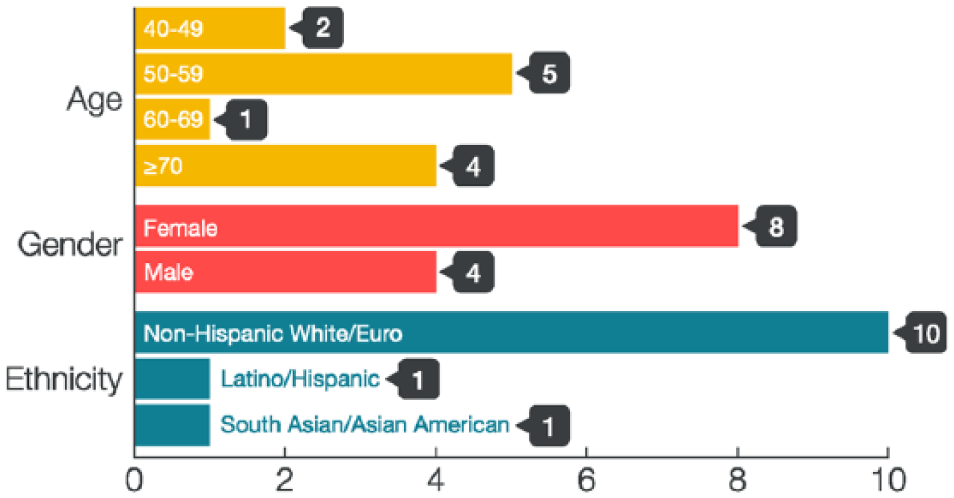
Participant characteristics: age, gender and ethnicity.

Participant characteristics: region and B-cell type.
Time from diagnosis ranged from 2 to 24 years prior to interview. As not all participants provided this information, we did not explore relationships between this attribute and descriptive or emergent themes.
Descriptive analysis showed that participants demonstrated prior knowledge about topics covered in the learning objectives and were able to summarise key education messages about B-cell NHL presented in the programme, including the broad approaches to, and benefits of, treatment options and treatment-related side effects.
Participants generally felt that the education activity reinforced their understanding of B-cell NHL and provided a ‘good way to learn more about the disease’. As one participant noted, ‘the more you hear things and do things over and over, the better you get at you know explaining to others’ (Patient 4). Participants also described a range of self-care strategies that were in line with education messages, such as engaging in daily activity, eating well, getting rest, and having a positive mental attitude.
Thematic analysis: foundations of self-care knowledge and practice
Thematic analysis generated several themes linked to self-care knowledge and practice, including normalisation of self-care, learning the hard way, everyone is different, and being prepared (Table 1).
Interview themes.

Normalisation of self-care
Participants were emphatic about the importance of engaging in self-care practices as a normal or central part of their lives to maintain health/well-being.
It’s very important to get up and move for a lot of reasons. (Patient 7) Try to get out of bed and take walks and just get out and not just stay under the covers like I did because you’re going to feel bad no matter what. You might as well be part of life. (Patient 11) I guess one of the things I can do for myself is to be aware of my diet, to eat really healthy and nutrition is really important because what you take into your body really will help to maintain your immune system. (Patient 9) I found that you have to be in good spirits. You have to do your exercise. Your diet is very important. (Patient 5)
Participants contextualised the self-care strategies they described in terms of being aware of one’s body and checking for bodily changes (‘you have to listen to your body and your body is going to tell you that things are a little bit different now’), caring for one’s immune system by minimising interaction with people (treatment is associated with immune system compromise), and making adjustments to activities in the presence of fatigue or other bodily signs and symptoms. Rest was identified as important to help manage the treatment process (i.e. infusions) and treatment-related side effects, as was the notion of being kind to oneself.
Learning the hard way/everyone is different
Participants’ experience had taught them that the approach to B-cell treatment could change over time. They emphasised the importance of having information available to them to support their active involvement in self-care as a life-time task, and to prepare them for what many viewed (in particular, those with diffuse B-cell NHL) as a long, but potentially manageable journey. Despite the need for such information, as summarised in Table 1, learning the hard way represented a principal learning modality for knowledge acquisition about B-cell NHL self-care. Participants described having little awareness of, or access to, information to support self-care, for instance, in relation to treatment side-effect management. Participants also recognised that the experience of B-cell NHL diagnosis and treatment is unique for everyone – that ‘everyone is different’ and no one is ‘a textbook patient’ – especially since there are so many sub-types.
Being prepared for self-care
Participants’ descriptions of self-care practices were accompanied by a recurring belief in the importance of being prepared, that is, being proactive in learning about their disease and updating their information about potential treatment and management options via four key strategies: (1) asking questions, (2) building relationships with oncologists, (3) developing/maintaining a philosophy of life and (4) connecting with others.
Asking questions
When asked to describe to another person about what to expect at diagnosis (Figure 1, Q4), participants emphasised the importance of asking questions about which tests they ought to have at diagnosis and emphasised the importance of being engaged with their diagnosis by doing their own research: You need to do your own research is what I would tell everybody and I would also say, whatever their diagnosed with, whether it’s lymphoma or anything else, question authority. Question the doctor. If something doesn’t feel right or sound right, you need to look it up and tell them. (Patient 12)
Patient involvement in discussing options for treatment was a key message presented in the education activity, which provided examples of questions to ask healthcare providers. Participants saw these questions as an especially valuable resource to support being prepared. Even though participants were motivated to engage in self-care behaviours, and in many cases already well-equipped to do so, they felt that having specific examples of questions to ask was an additional tool that enabled them to be more in control of their disease experience and more involved in decision-making: I don’t want you just telling me this is the treatment because if I tell you I have these issues of medical history and things like that will that alter the course? I want to make sure that my doctor is open minded. I want to make sure that my doctor has, is willing to tailor and customise a plan and not have this one size fits all. (Patient 1)
Participants also emphasised the importance of asking healthcare providers about the range of options available across the disease trajectory, and patients who volunteered as peer supporters with LLS also wanted to be equipped to encourage other patients to ask questions.
2. Building relationships with oncologists
Having a good oncologist, getting a second opinion, or switching to another oncologist represented further dimensions of being prepared. Half of the participants shared stories about a convoluted diagnostic process involving what they viewed as poor clinical judgement or skills, poorly managed and painful bone marrow biopsies, not getting a straight answer or poor bedside manner. These were commonly cited triggers for finding an alternative oncologist and building robust relationships with physicians: I asked my oncologist if I was going to die straight out and he said no. So just ask. Whatever fears you have, just ask him and if he doesn’t really respond, then you get a different oncologist. (Patient 11) If you are not satisfied, which I did, go and see another one for a second opinion. In America, there is nothing wrong in that. It is your right, I think. That’s what I will say. If you get a right doctor and right diagnosis, you are on the right track. (Patient 5)
3. Developing/maintaining a philosophy of life
Participants emphasised the importance of building a support system to provide practical support (e.g. grocery shopping and general household chores) and ‘to encourage you to do the things that you know you should do’. Many of the participants in this sample were single, and described themselves as ‘doing this alone’. Online resources and local support groups helped this group cope with their disease and the side effects of treatment. Faith, spirituality and having a positive attitude also played a role as part of ‘being prepared’: I’d say my faith is very important to me, and so that’s a big thing that got me through is the people that I knew were praying for me and I prayed for myself. (Patient 9) I think you need to live your life as much as you can. (Patient 6)
4. Connecting with others
Active engagement as patient citizens was also connected to being prepared. Such engagement included volunteering for the LLS, acting as peer support providers, offering advocacy, and participating in fund raising. Most participants also commented during their interview that they were eager to participate in the education activity, and saw it as an opportunity to not only refresh their own information, but also as a way to remain connected to the LLS and/or B-cell NHL community.
The patient vignettes included in the education content also offered an opportunity for connection. Participants viewed the vignettes as providing a window into the real-life, lived experience of B-cell NHL. In contrast to ‘textbook science mumbo jumbo’, (Patient 7) vignettes provided a personalised, authentic opportunity for participants to learn ‘from people that actually are going through it’ (Patient 6), ‘how they experienced it, what they decided to do and where they are today’ (Patient 7): It was helpful to hear what other peoples’ experiences were. I think that’s probably the most valuable thing that I think that I was seeking out. I mean, it’s one thing [if] you can find a lot of research on or, you know, finding different medical treatments and pros and cons and all that, but it’s a little harder to find actual feedback from patients’ experiences. It would be good for some peoples’ psychological aspect to see there’s a lot of success stories out there. (Patient 7)
Discussion
Qualitative insights on self-care and PSE in B-cell NHL
This study explored education impact on knowledge about and perspectives on self-care and self-efficacy in the context of a B-cell NHL diagnosis. Following participants’ participation in an online education activity, participants demonstrated sustained knowledge about practical self-care behaviours, and were able to describe key messages presented in the programme. They emphasised the importance of intentionally caring for themselves via functional behaviours (e.g. practicing good nutrition, being physically active within their personal limits, connecting with others in ways that were consistent with not only education messages) that also correspond broadly to categories of self-care previously described in the literature on chronic disease (Barofsky, 1978; Bury et al., 2005). Participants emphasised the value of learning about which questions to ask, and reported they would use them going forward when they next met with their healthcare providers. These findings suggest that the education achieved its aim to support self-efficacy by reinforcing existing PSE through social persuasion. This finding is consistent with social cognitive theory (e.g. Bandura, 1997), on which models of health behaviour change are based. These models assert that self-beliefs derived from interactions between personal, environmental or situational and behavioural determinants influence learning, action and behaviour change.
The health behaviour literature describes PSE as an important precursor to action that is sustained by an individual’s beliefs in their ability to act in ways that will accomplish particular outcomes (Bandura, 1986, 1995; Prochaska and DiClemente, 1982). Although PSE beliefs reflect what people believe they are able to do in a particular situation rather than actual performance, such beliefs are, nonetheless, seen to influence the performance of particular behaviours, such as engaging in self-care in the context of chronic disease or cancer. In turn, PSE beliefs are influenced by information from several sources, including one’s own experience and social persuasion. However, there is little empirical description of the beliefs that underlie PSE (Burke et al., 2009). Instead, much of the health education/behaviour literature on self-efficacy utilises quantitative scores (e.g. PSE for Fatigue Self-Management Scale, Hoffman et al., 2009) to measure self-efficacy as a cognitive construct. These measures presume the significance of rational action in health behaviours and practices but overlook the sources, salience, and specificity of PSE beliefs, as well as, more broadly, the social contexts that influence beliefs, and in which beliefs are enacted (Burke et al., 2009).
When we explored interview data inductively, we discerned four themes related to the practice of self-care, including normalisation of self-care, learning the hard way, everyone is different and being prepared. These themes provide context to the experience of self-efficacy in the context of B-cell self-care, and suggest that in order to enact self-care, participants believed that they needed to be prepared, and pointed to a number of strategies that enabled them to be prepared. These findings point to self-efficacy as a fluid social concept and underscore the need for wider exploration of the meanings that people hold for self-efficacy in the context of self-care. In a similar vein, recent systematic reviews suggest that the meaning and enactment of self-efficacy varies across cultural context and ethnicity (Stewart et al., 2009) and represents a resource for both individuals and communities (Boehmer et al., 2016).
Practice implications
The themes identified in this study have potential implications for self-efficacy education. First, participants viewed self-care as a normalised aspect of living with B-cell NHL. As cancer evolves into a chronic disease, educators can cultivate this normalisation through interventions that enable patients to view self-care as a part of the routine of living long-term with cancer, and help them make tailored adjustments and modifications to daily activities in response to changes in disease- and treatment-specific signs and symptoms.
Second, knowledge acquisition about B-cell NHL was hard won for participants in this study; however, learning the hard way has the potential to stymie self-efficacy. Expanding the availability and accessibility of information for patients with B-cell NHL is a necessary foundation for building self-efficacy in relation to self-care in this context. Third, the experience of living with B-cell NHL differs for people by subtype and other factors. The perception that everyone is different poses potential barriers to self-efficacy if patients do not see themselves reflected in educational materials. Educational interventions can encourage PSE and authenticate self-care strategies by reflecting variations in the lived experience of others by using, for example, vignettes that provide a window, or a ‘vicarious experience’, into the experience of B-cell NHL.
Finally, being prepared may represent an underlying belief that supports PSE in the B-cell NHL context. Participants linked being prepared to specific strategies such as asking questions of healthcare providers, building relationships with healthcare providers, enacting a philosophy of life and connecting with other B-cell patients. This linkage between belief and action points to self-efficacy as a dynamic process, as well as a cognitive construct. As such, the meanings that people hold for self-efficacy in other self-care contexts warrant empirical specification as a foundation for developing meaningful, targeted patient education.
Limitations
Participants who chose to participate in this educational intervention self-selected to seek further information about B-cell NHL, and may be atypical of the general population with this disease. We contend, however, that the strong engagement of participants with their disease allowed us to explore the meaning of self-efficacy from their perspectives, and to flesh out the factors associated with influencing and reinforcing PSE. The sample size is small; however, small sample size is conventional in qualitative research, when the purpose is to yield meaningful insights or generate hypotheses, versus generalisable results.
Conclusion
Patient education programmes are becoming especially germane in the context of changing epidemiology and patient demographics (Beaser et al., 2017; Rothrock et al., 2006). Such education is important to enable patients with chronic disease and illness, including some cancers, to participate in self-care. As populations in both Europe and the USA age, the prevalence of chronic conditions – including many cancers – will also increase, and both clinician shortages and rising healthcare costs add to the necessity of patient involvement in disease self-care (Frenk et al., 2010). Research suggests that patients with the capacity to cope with disease, treatment and treatment-related side effects are better able to adjust to their diagnosis and experience a greater quality of life (Zachariae et al., 2003). Building self-efficacy is key to developing this capacity to cope with self-care; however, the beliefs underpinning self-efficacy remain under-investigated. The themes generated by this qualitative study provide insights on which educators can draw to strengthen self-efficacy education interventions for patients with B-cell NHL and other types of cancer. In particular, educators can consider soliciting information from patients about the experience and meanings of both self-care and their self-efficacy beliefs.
Supplemental Material
Online_suppementary_File – Supplemental material for Perceived self-efficacy in B-cell non-Hodgkin lymphomas: Qualitative outcomes in patient-directed education
Supplemental material, Online_suppementary_File for Perceived self-efficacy in B-cell non-Hodgkin lymphomas: Qualitative outcomes in patient-directed education by Alexandra Howson, Wendy Turell and Anne Roc in Health Education Journal
Footnotes
Acknowledgements
We are grateful to the people who participated in this education programme and who agreed to be interviewed for this study.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by an independent educational grant from Pharmacyclics LLC, an Abbvie Company, Janssen Biotech, Inc., (administered by Janssen Scientific Affairs, LLC), and Genentech.
Supplementary Material
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.