
Abstract
Objectives:
First aid programmes should include not only the transfer of knowledge and skills but also improve participants’ helping attitudes. The aim of this study was to evalute the immediate and long-term effects of a 3-day first aid programme for kindergarten children.
Methods:
One hundred and eighteen kindergarten children (5–7 years old) from an inner-city kindergarten located in Pécs, Hungary, were involved in this study between January 2016 and June 2017. Training consisted of three 45-minute sessions involving the transfer of theoretical knowledge and practical skills about first aid. Knowledge, skills and attitudes were assessed by means of a questionnaire developed for the study and through observation. Participants were tested before and immediately after the programme and at 4 and 15 months.
Results:
The majority of children had no prior knowledge in first aid. Knowledge and skills significantly improved immediately after training and remained significantly higher at 4 and 15 months when compared to baseline – calling the ambulance (p < 0.01), performing cardiopulmonary resuscitation (CPR; p < .01), using an automated external defibrillator (AED; p < .01), handling an unconscious patient (p < .01) and managing bleeding (p < .01). Attitudes towards first aid improved significantly after the programme (p < .01) and remained improved after 4 and 15 months when compared to baseline (p < .01).
Conclusion:
Beginning first aid education in kindergarten can be useful. Children cannot become professional bystanders immediately following training, but the programme can offer an introduction of first aid. However, the results decreased substantially after 15 months so regular refreshing training should be recommended.
Introduction
Bystander first aid can improve the chance of survival in the event of a sudden injury or illness. The frequency and quality of first aid provision differs worldwide but is usually lower than expected (Gräsner and Bossaert, 2013). In countries with high-quality first aid education outcomes are better (Wissenberg et al., 2013). The majority of the Hungarian population attend first aid training only when acquiring a driver’s licence (Bánfai et al., 2015).
First aid education in early childhood can be key to increasing effective bystander numbers. The Kids Save Lives project was endorsed by the World Health Organisation (WHO), the International Liaison Committee on Resuscitation (ILCOR), the European Resuscitation Council (ERC), the European Patient Safety Foundation (EuPSF) and the World Federation of Societies of Anaesthesiologists (WFSA). Based on findings from this project, cardiopulmonary resuscitation (CPR) education was recommended from the age of 12 (or younger) for every child worldwide (Böttiger and Van Aken, 2015). School resuscitation education is mandatory in several European countries, in many US states and in Canada (Cave et al., 2011; Hart et al., 2013; Semeraro et al., 2016). However, first aid training should be more inclusive than focusing on resuscitation only (De Buck et al., 2015). The Hungarian national school curriculum has included first aid and resuscitation education in primary and secondary schools (from the age of 13 years) since 2012 (Governmental decree, 110/2012 (VI. 4.)). Despite mandatory legislation, however, school first aid training has not been successfully implemented.
First aid training in childhood can improve participants’ knowledge, skills and willingness (Oliver et al., 2014). However, there is a lack of evidence about the best starting age (Cave et al., 2011; De Buck et al., 2015; Plant and Taylor, 2013; Wilks and Pendergast, 2017). Our previous first aid programme for primary school children demonstrated that 7- to 14-year-old children can learn basic first aid (Bánfai et al., 2017). In this study, we investigated whether it could be effective among younger children. The aim of the study was to evaluate the effects of a 3-day first aid programme for 5- to 7-year-old kindergarten children. Our goal was to measure the children’s first aid knowledge, skills and helping attitudes before, immediately after, at 4 months and at 15 months following the programme.
Methods
Study participants
Children were recruited from an inner-city kindergarten in Pécs. All children (5–7 years old) were required to participate in a 3-day education programme held between January 2016 and June 2017. Both children who had not attended all three lessons or who did not participate in any of the tests were excluded from the study (Figure 1).
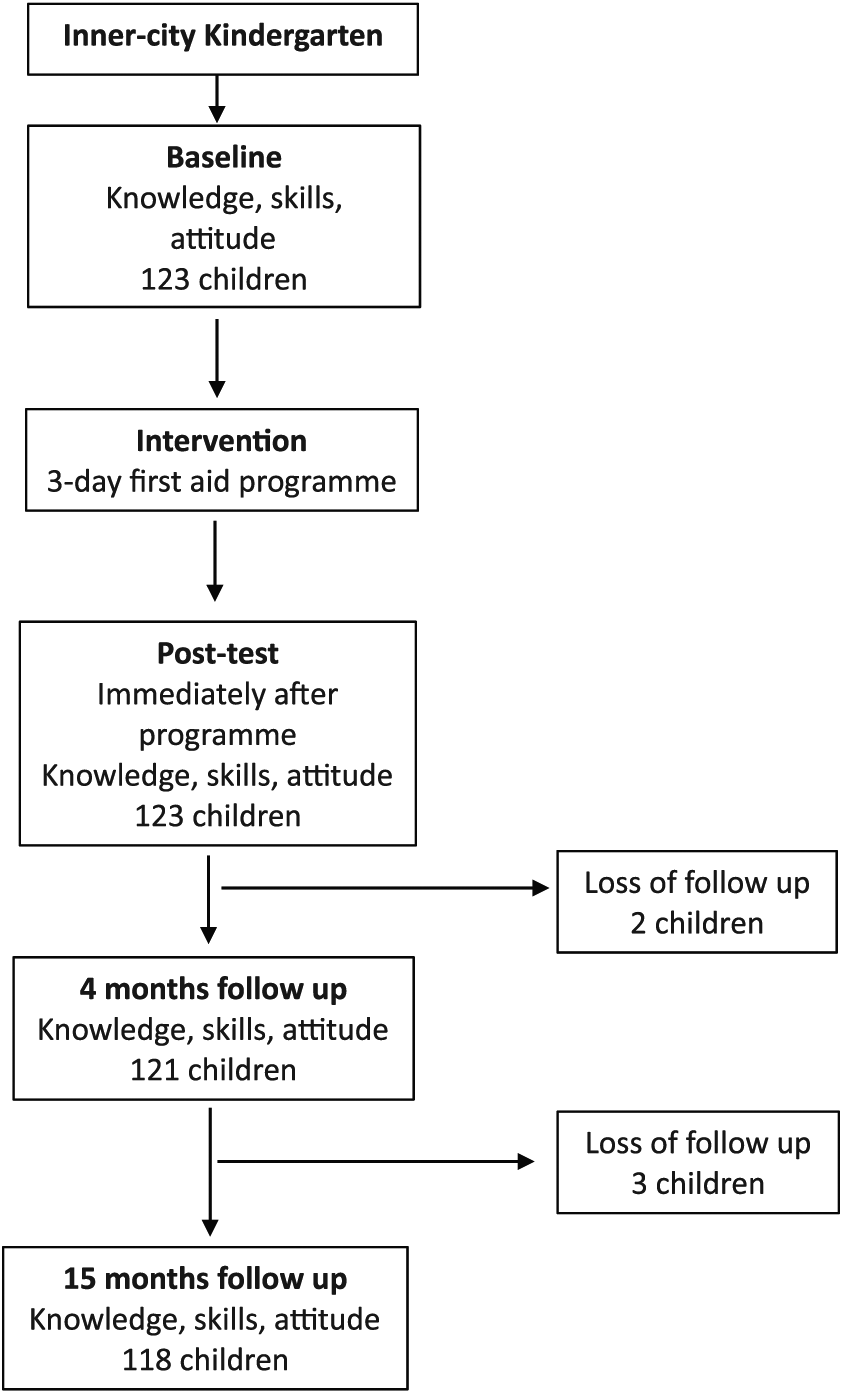
Study flow-chart.
Education programme
The methods used were the same as those reported in an earlier evaluation of a 3-day first aid programme for primary school children (Bánfai et al., 2017). Training consisted of three sessions (45 min each) on three consecutive weeks (one per week). The following topics were addressed: calling the ambulance, adult basic life support (BLS), using an automated external defibrillator (AED), handling an unconscious patient and managing severe bleeding. The education programme was adapted to the needs and abilities of kindergarten children. All of the instructors were paramedics. We had earlier assessed the willingness of kindergarten teachers to teach the first aid programme. Based on their answers and the belief that they were not able to teach first aid (lack of time, lack of knowledge and experience of first aid), we selected paramedics experienced to teach the first aid. The training programme contained both theoretical and ‘hands-on’ training components. Knowledge and skills transfer took place in small groups (8–10 children/group).
Measurement
We administered a questionnaire to the children before, immediately after, and at 4 months and 15 months following the education programme. The questionnaire used open-ended questions because we believe the answers of open questions provide better insight into understanding among young children compared to multiple-choice tests (Bánfai et al., 2017). Kindergarten children also have a lower level of cognitive status, so questions could be asked and answer orally. Children were also tested using first aid scenarios before and immediately after teaching, and then re-tested at 4 and 15 months. Completion of the questionnaire and skills assessment took place on the same day.
The sex, age, body height and weight of all children were recorded and their body mass index (BMI) was calculated since it was believed that these factors might influence practical skill acquisition. Children used a ‘code word’ when they were measured, so we could follow them anonymously throughout the duration of the entire programme.
We also measured children’s ability to recall the correct telephone number of the local ambulance service (104 or 112 in Hungary) and to give necessary relevant information (location, nature of the emergency, number of victims, own telephone number). To test this ability as part of practical skills, we described a number of emergency situations, and for each situation, the children had to decide whether it was necessary to call the ambulance service.
To evaluate CPR performance, we used an AMBU® Man W model with AMBU® CPR Software (AMBU A/S, Baltorpbakken 13, DK 2750 Ballerup, Denmark) (Table 1) throughout a CPR scenario of 2 minutes duration. To teach and practise AED, we used a Lifepak® 1000 AED Trainer. Artificial wounds using materials such as makeup and syrup were made to simulate severe bleeding. The accident victims were other children or adult actors. Measurements were conducted in a private classroom, while the remainder of the participants waited in another room. First aid skills were scored by an instructor using checklists developed according to ERC guidelines (Perkins et al., 2015; Zideman et al., 2015).
Chest compression and ventilation measured with AMBU CPR Software (n = 118).
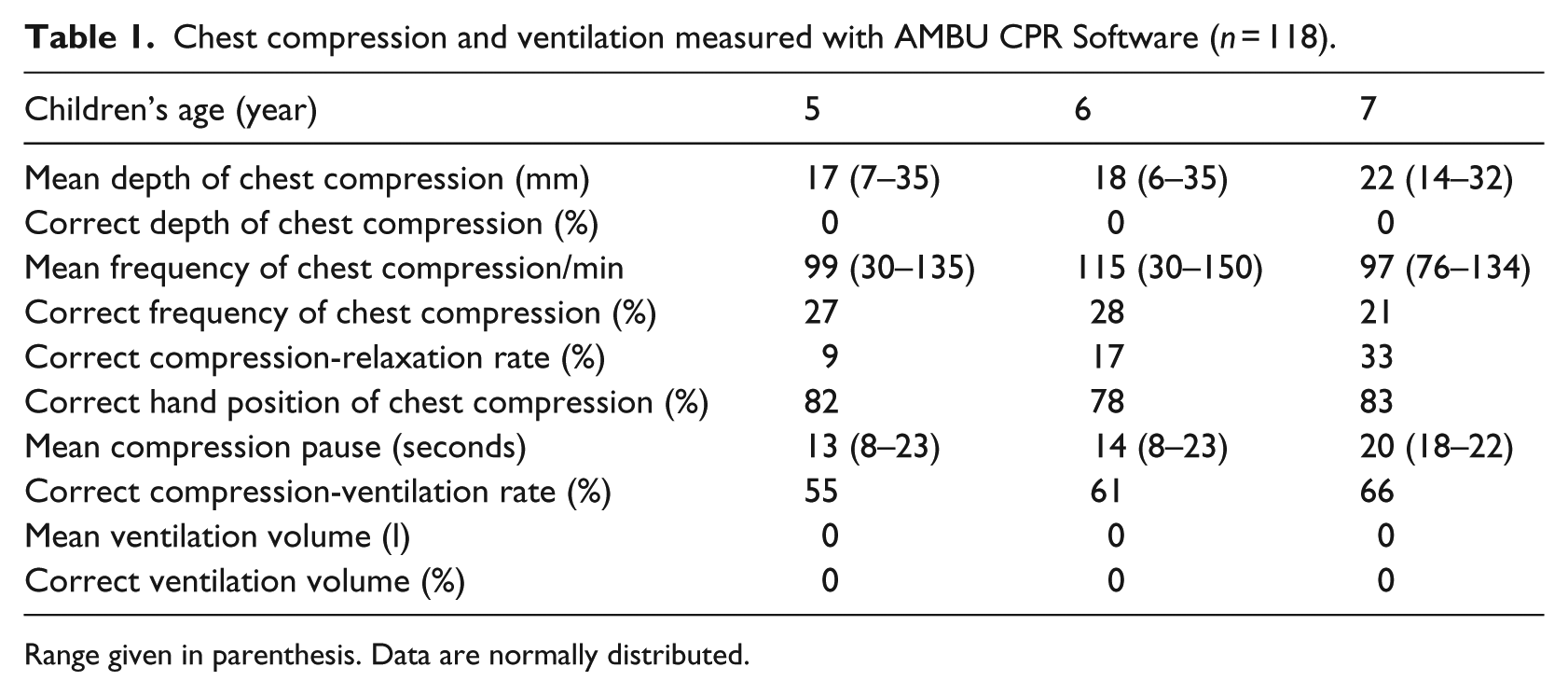
Range given in parenthesis. Data are normally distributed.
Willingness, helping attitude
Data about opinions and attitudes towards providing first aid and our programme were collected orally (Table 2).
Attitudes towards the first aid education programme (n = 118).

p < 0.01 compared with the pre-test (Chi-squre-test).
Statistical analysis
Statistical analysis was conducted using SPSS 22.0 (Statistics Package for Social Sciences, Chicago, IL, USA) statistical software. Descriptive statistics were calculated (percentages, means, medians with interquartile ranges). Categorical variables were presented as percentages and were compared using Chi-square-tests or Fisher’s exact test as appropriate. One-way analysis of variance (ANOVA) and t-tests were used to test the association between knowledge, skills (pre, post-, after 4 and 15 months) and selected demographic characteristics (age, body weight and height, BMI). Pearson’s correlation analysis was applied to test CPR quality (chest compression depth and ventilation volume vs age, BMI, body weight and height). Attitudes were presented using descriptive statistics (percentages) and were compared using Chi-square-tests or Fisher’s exact test as appropriate. A p < .05 level was considered to be statistically significant.
Ethical considerations
Since this study set out to evaluate a first aid education programme, it did not fall within the mandate of research ethics committees in Hungary, and therefore, no approval was needed according to Hungarian law and regulations. The participants, their parents, and teachers received written and oral information prior to study commencement. They were informed of their right to withdraw at any time with no personal consequences. The children’s parents provided written informed consent before their child entered the study.
Results
One hundred twenty-three kindergarten children were recruited into the study. Of these, five were excluded from the study because they did not participate in at least one of the tests (Figure 1). There were therefore 118 study participants (5–7 years old), comprising 71 girls (60.2%) and 47 boys (39.8%). Demographic data are displayed in Table 3.
Demographic profile of the children (n = 118).
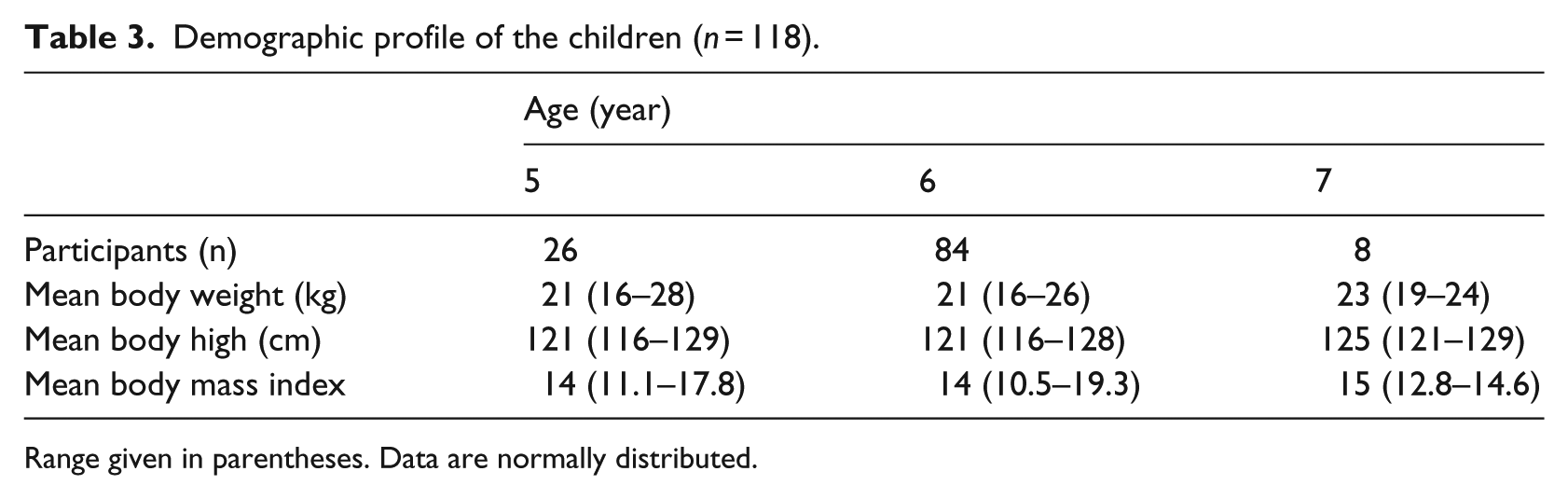
Range given in parentheses. Data are normally distributed.
Theoretical knowledge
The majority of children did not have any knowledge on the measured topics before the programme. Children’s theoretical knowledge immediately after the programme, at 4 months and at 15 months was significantly higher than at baseline (p < .01) (Table 4). Theoretical knowledge was independent of children’s age, sex and physical factors (Table 5).
Success rate (%) of correct answers of the theoretical measurements (based on questionnaire results, n = 118).

p < 0.01 compared with the pre-test (Chi-squre-test).
Effects of age, sex and Body Mass Index (BMI).

Sex was compared with correct answers using Chi-square-test. Age and BMI were compared with correct answers using ANOVA and t-test.
Practical skills
Participants scored significantly higher on all skills immediately after training, at 4 months and at 15 months when compared to baseline (p < .01) (Table 6).
Success rate (%) of correct answers of the practical measurements (based on the scenarios) (n = 118).
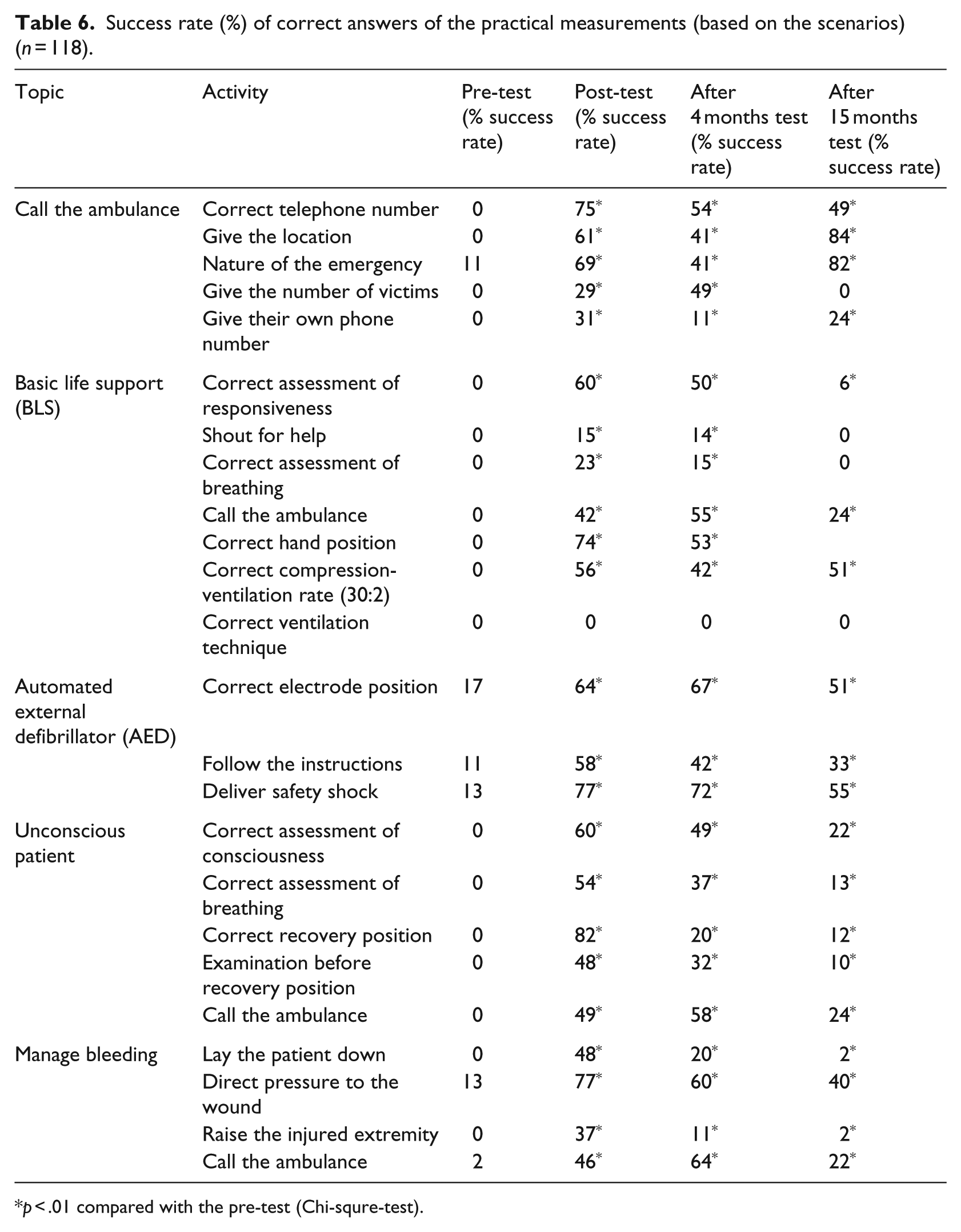
p < .01 compared with the pre-test (Chi-squre-test).
In the facilitated situation game, the number of participants who correctly decided it was necessary to call the ambulance before training, immediately after training, at 4 months and at 15 months after the training were 62 (53%), 78 (66%), 106 (90%) and 67 (57%), respectively.
CPR effectiveness (chest compression and ventilation) with AMBU® CPR Software was only measured immediately after training (Table 1). None of the participants were able to achieve effective chest compression depth and ventilate the patient. There was no significant correlation between chest compression depth and children’s age (r = .123; p = .50), body weight (r = –.206; p = .25), height (r = –.257; p = .15) and BMI (r = –.124; p = .50). There was also no significant correlation between chest compression depth and children’s sex (p = .06). Correct hand position was neither dependent on sex (p = .62), BMI (p = .36) nor knowledge of correct compression-ventilation ratio (p = .49; p = .33). Chest compression frequency was independent of age (r = .098; p = .59), sex (p = .42), body weight (r = –.042; p = .82), body height (r = .090; p = .62) and BMI (r = –.087; p = .63).
While none of the participants knew the function of an AED before training, approximately 11%–17% of the children knew the correct electrode position, followed the instructions correctly and could safely deliver a shock before our programme. AED ability rose from 11% to 17% at pre-test to >50% after the programme and remained significantly higher than at baseline at 4 and 15 months.
Before the programme, only 28% of participants could identify if a patient was breathing correctly. This percentage increased to 64% immediately after training, to 66% at 4 months but fell to 43% at 15 months. More than three-quarters of the children were able to perform the correct recovery position immediately after training. However, these results decreased substantially at 4 and 15 months, with only 20% and 12% of children being able to place an accident victim in the recovery position, respectively. Only a very small number of children could place an adult patient in the recovery position unaided because of their physical abilities. Other children solved the problem by working in groups. The management of bleeding also significantly improved after training and remained significantly higher at 4 and 15 months compared to baseline. Practical skills were independent of children’s age, sex and physical factors (Table 5).
Willingness, helping attitudes
Attitudes towards first aid improved significantly after training (p < .01). At 4 and 15 months, willingness and helping attitudes decreased but remained significantly higher than at baseline (p < .01) (Table 2). Helping attitudes were independent of children’s age (p = .512), sex (p = .332) and physical factors (p = .421).
Discussion
This study is the most comprehensive longitudinal study so far conducted on the effects of a first aid (not only resuscitation) programme among kindergarten children. The main findings of our study are that children as young as 5 years are able to learn some basics of first aid including calling the ambulance service, starting CPR, using an AED, handling an unconscious patient and managing severe bleeding. After our 3-day first aid programme, as well as at 4 and 15 months after training, most of the knowledge and skills were significantly better than before the training. No other study has investigated this age group so extensively. Theoretical knowledge, practical skills and attitude were also measured.
Overall, approximately half of the children correctly performed all of the activities (except effective CPR and some other parts of BLS process) immediately after training. Approximately three-quarters of the children were able to give the correct ambulance phone number. Previous studies demonstrated that young children are able to call for help and give basic first aid (Bánfai et al., 2017; Bollig et al., 2009, 2011; Fleischhackl et al., 2009). In our study, approximately half of the participants were able to decide whether it was necessary to call the ambulance at baseline. Immediately after training, the number of these participants who could give the correct answer increased and remained higher at 4 months, but was similar at 15 months to baseline.
In this study, none of the children could perform effective chest compression depth and ventilation because of their physical abilities, but several participants were able to learn the cognitive parts of BLS as well as older children (Bánfai et al., 2017). No previous study has investigated the CPR skills of kindergarten children. Teaching BLS under the age of 10 years can be useful. The majority of these children cannot perform effective CPR, but they can learn about some aspects of resuscitation (e.g. assessment of breathing, correct hand position). These knowledge and skills can be useful in a possible real emergency situation.
At baseline, approximately one-tenth of participants could correctly use the AED without any prior knowledge. Our results demonstrated that more than half of the kindergarten children could use the AED after training. In our previous study, the results of primary school children’s AED skills were similar (Bánfai et al., 2017).
The majority of participants were able to learn the correct recovery position. Previous studies have shown similar outcomes: more than three-quarters of 6- to 7-year-old children and approximately half of 4- to 5-year-old children could place the victim in the correct recovery position after training (Bollig et al., 2009, 2011). In this study, children assessed the breathing of an unconscious pseudo-patient more often than they did in the BLS scenario, perhaps because the ‘patient’ in the BLS scenario was a mannequin, whereas another child or an adult actor played the victim in the situation with the unconscious patient.
More than half of the children in our study were able to apply a correct dressing to minimise bleeding. Previously, only a few studies have analysed the impact of manage severe bleeding as part of a training programme for children (Bánfai et al., 2017; Uray et al., 2003).
Improving first aid knowledge can improve attitudes towards giving help (Hawks et al., 1992; Oliver et al., 2014). In our study, less than half of the participants showed willingness to help another person before our programme. After the programme and at 4 and 15 months, these results were significantly higher than at baseline. Nonetheless, it is important to note that we do not know whether children could help in a real emergency situation (Yeung et al., 2017).
Children are easily motivated to attend a first aid programme (Semeraro et al., 2017). In this study, the majority of participants said they would like to attend another first aid programme in the future.
Despite the positive results of this study, there was a decline in the majority of theoretical knowledge and practical skills after 15 months so annual refresher training is recommended.
Based on the findings of this and previous (Bánfai et al., 2017) research, we have developed an outline curriculum for first aid education in early childhood which is available in online Supplemental material (Appendix A).
Limitations
Being conducted in only one centre, this study is not representative for the population of kindergarten children in Hungary. Children were re-tested after 4 and 15 months, but we do not know the effects of training after a longer period of time. There was also a small loss (5 children) to follow up. The reaction of children to a real emergency remains unknown. A follow-up study in the future could help to measure the long-term knowledge and skill retention, and the possible effects of refresher training.
Conclusion
In conclusion, first aid education in childhood can have a far reaching impact by potentially increasing the number of active bystanders over time. Bringing some aspects of first aid education into the kindergarten can be useful. Kindergarten children who participated in our 3-day first aid programme learned some of the basics of giving help. In no sense can these children be considered professional bystanders immediately after training, but the programme can be an introduction and sensitisation to the importance of first aid. The most important thing for young children is to be able to recognise emergency situations and call for help. The main benefits of our programme are that it includes not only the transfer of knowledge and skills, but also it enhances the motivation children to perform first aid and develop their attitudes.
Supplemental Material
Supplementary_material – Supplemental material for Little lifesavers: Can we start first aid education in kindergarten? – A longitudinal cohort study
Supplemental material, Supplementary_material for Little lifesavers: Can we start first aid education in kindergarten? – A longitudinal cohort study by Bálint Bánfai, Attila Pandur, Bence Schiszler, Emese Pék, Balázs Radnai, Henrietta Bánfai-Csonka and József Betlehem in Health Education Journal
Footnotes
Acknowledgements
The authors would like to thank the children, their parents and teachers for their participation in the study.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.