
Abstract
Introduction:
African women who migrate to the USA have a rich tradition of using herbs and spices to promote health. We conducted formative research on nutritional practices among East and North African women in the USA, focusing on whether traditional herbs and spices could support adherence to the Dietary Guidelines for Americans.
Methods:
In all, 48 adult African women living in San Diego, California participated in focus groups in July 2015. Inclusion criteria were 18 years or older, and able to answer focus group questions in one of five languages: Somali, Arabic, Amharic, Swahili or English.
Results:
Participants identified 62 unique spices and herbs that are traditionally used in meal preparation for flavour and health benefits. Participants also reported awareness that nutrients, foods, food groups and approaches to growing and preparing foods are important considerations for healthy diet. Barriers to healthy eating included costs, constraints around growing food in a different soil and climate than Africa, family size and the widespread availability of fast food. Groups identified opportunities for collaborations with researchers through educational programmes, and recommended seed and recipe exchanges that promote healthy eating across culturally heterogeneous African communities.
Conclusion:
A culturally informed behavioural intervention focused on spices and herbs would be feasible and accepted by African women in San Diego. This intervention may support adherence to the Dietary Guidelines for Americans during the nutrition transition and broader dissemination of practices that promote health across heterogeneous communities of Africans living in the USA.
Prevention of many chronic diseases requires healthy dietary practices, and for most of the population, there are significant challenges to consuming healthful diets and adherence to the Dietary Guidelines for Americans (US Department of Agriculture and US Department of Health and Human Services, 2015). Furthermore, in many parts of the world, the effects of the ‘nutrition transition’ can be felt. This term refers to growing chronic disease rates, such as cardiovascular disease and diabetes, following increasingly sedentary lifestyles and rising consumption of non-nutritional, high calorie foods as populations transition to Western lifestyle practices from traditional practices (Popkin et al., 2012). Those of lower socioeconomic status and racial/ethnic minority groups have substantially worse health for nearly every disease outcome, including those resulting from the nutrition transition (Fiscella et al., 2000; Nelson et al., 2009).
Migrants 1 from less economically developed countries may enjoy health benefits at their time of arrival that dissipates over time as they acculturate and likely experience other lifestyle transitions (Vandenheede et al., 2015). Cross-sectional research has established these dietary changes (Burns, 2004) as well as high rates of being overweight or obese, and rising chronic disease concerns with African migrants and refugees in Western countries (Drummond et al., 2011; Guerin et al., 2007; Murray et al., 2013; Renzaho et al., 2011). In the USA, there are significant challenges with adherence to the Dietary Guidelines for Americans (US Department of Agriculture and US Department of Health and Human Services, 2015) yet sparse information is available to inform how effectively to engage African migrants to preserve and promote healthy dietary habits.
Despite evidence of disparities in health, little progress has been made in reducing inequities that unjustly affect the most vulnerable populations. Changes in scientific approaches are required, such as the use of community-based participatory research (CBPR) methods to ensure health interventions reach and meet the needs of currently underserved populations (Blumenthal, 2011; Boyce and Olster, 2011; Carney et al., 2011). CBPR involves active collaboration with and within communities to emphasise strengths, leverage resources and facilitate co-learning and mutual benefit. Moreover, CBPR is an iterative and cyclical process that ensures transparency and ongoing feedback between community and academic partners (Israel et al., 2005).
This type of active collaboration, transparency and mutual respect is essential when working with individuals from a refugee background (Ellis et al., 2007; Johnson et al., 2009). The application of CBPR methods to dietary interventions could more effectively assess and address dietary factors that contribute to, and perpetuate, widespread health disparities. In comparison to other groups, very few research and intervention efforts have specifically involved African migrants although they represent a rapidly growing group in the USA (Terrazas, 2009). Among San Diego’s large African communities, there is substantial evidence of rising chronic disease rates alongside momentum, interest and a pressing need to address lifestyle factors that are related to chronic disease prevention (Murray et al., 2013, 2015). Changes in lifestyle and chronic disease profiles among African immigrants is not well understood and further research is needed (Venters and Gany, 2011).
In this study, a CBPR process was applied that built upon an established community–academic partnership. The primary aim of the study was to identify factors that influence adherence to healthful dietary practices among African women living in San Diego, California. Both community and academic partners identified the rich tradition of using herbs and spices to promote health as a possible focus for dietary intervention to facilitate adherence to the Dietary Guidelines for Americans following migration to the USA. This research used qualitative methods to gain understanding of community perspectives on challenges and opportunities for healthful eating in the context of migration. The use of herbs and spices in promoting healthy eating was explored.
Methods
Study population
Study participants were women from the Somali, Sudanese, Kenyan, Eriterian, Egyptian, Tunisian, Algerian, Ethiopian, Ugandan and Moroccan communities living in San Diego, California. Data were collected in July 2015. The inclusion criteria included being at least 18 years of age and having the ability to participate in a focus group conducted in one of five languages: Somali, Arabic, Amharic, Swahili or English. Word-of-mouth advertising by the community partner agency was used to recruit participants. The Institutional Review Board at University of California, San Diego (UCSD), provided human subjects ethics approval prior to initiating the study.
Study design
We conducted formative research by involving participants in focus group discussions. To inform the methodology for this work, we build upon an established partnership between the United Women of East Africa Support Team (UWEAST) and scientists at the UCSD School of Medicine.
UWEAST was created in 2009 and provides services across East African communities in San Diego through a participatory model, in which decisions are made through group consensus and programmes facilitated largely by members within the organisation. Over the past 7 years, UWEAST has developed the capacity to provide translation services, research support and peer education programmes. Initial project discussions arose in 2014 from ongoing partnership activities on other health topics. Nutrition concerns were identified by UWEAST as an area of interest for its constituents, in particular to learn from each other about the use of herbs and spices to promote health across diverse African communities resettled in the USA.
In designing the project, a memorandum of understanding (MOU) was developed collaboratively and signed by both partners. The MOU detailed inputs, outputs and processes to ensure an equitable partnership that met the needs of both the community and academic partners. Likewise, the MOU defined the decision-making process, steps to achieve mutual goals, and ensured accountability and transparency of processes.
Measures and data collection
Four focus groups were conducted including communities in UWEAST membership (i.e. Somali, Sudanese, Eriterian, Ethiopian, Kenyan and Ugandan), and communities outside of UWEAST membership such as Moroccan, Algerian, Egyptian and Tunisian women. Each focus group lasted 60–90 minutes and was guided by a semi-structured standardised interview protocol. The protocol included five questions with additional prompts to elicit participant feedback on traditional healthy diets and the role of herbs and spices in promoting healthful eating. The primary questions included the following: (1) What do you consider to be a healthy diet? (2) What types of spices and herbs do you use and how do you use them? (3) How do you access your herbs and spices? (4) What are some other barriers you have encountered in maintaining a healthy diet? and (5) Are there ways the team at UCSD can support healthy eating in your community?
Focus groups were offered in four different languages and participants self-selected a focus group based on preference. Groups were led by trained women from the Somali, Sudanese, Ethiopian, Ugandan and Moroccan communities with experience in qualitative interviewing and the ability to conduct the session and translate the data. They were also trained in the delivery of the questionnaires, which were individually administered orally in the participants’ native language. Focus group sessions were digitally recorded and staff members took notes in both the original language and the English translation. Within each focus group discussion, participation from every person was encouraged. For every question, the principle of saturation was used. When focus group leaders determined, based on the information obtained for each question, that involving another participant added no important new data, the group proceeded to the following question.
Demographic information, history of hypertension and related medications, and blood pressure (BP) monitoring behaviours were collected using an interviewer-administered questionnaire. A trained staff member obtained BP measurements. The purpose of the BP data was to provide some preliminary descriptive statistics on the prevalence and health behaviours surrounding hypertension within the sample, for whom there is little available data.
Analysis
We present both qualitative and quantitative data. Quantitative data were analysed using SPSS statistical software. Qualitative data were collected using recommended procedures for focus groups (Krueger and Casey, 2000) and analysed using thematic analysis (Braun and Clarke, 2006). The notes were reviewed by a primary coder then reviewed and refined within the research team. The team included people with a background in nutrition research (the primary coder) and those without (secondary coder and bicultural team members). Most members of the team had experience facilitating focus groups and the primary and secondary coders had experience in qualitative analysis on other research projects, including thematic analysis. The primary coder and bicultural team members who co-facilitated the groups reviewed the themes to ensure they adequately represented the focus group conversations. The notes were reviewed until the group felt the themes adequately represented the data and group discussion. The primary coder summarised the number of times each theme was present and findings were compared across the four groups. Quotes that reflect the main views expressed by participants are reported in the Results section verbatim. We stratified data by focus group type (i.e. by language as a proxy for region of Africa), to examine similarities and differences across countries of origin. Incorporating a multidisciplinary team with diverse backgrounds and content knowledge was done to balance biases inherent within the research team, including cultural biases and varying degrees of knowledge of nutrition practices in Western and African contexts.
Results
Demographic characteristics for the 48 study participants are shown in Table 1. On average, participants were 44 years old having lived in the USA for approximately 11 years and coming from 10 different countries. Participants in the group who spoke Somali were older and have lived in the USA longer. Almost 30% of participants in the group who spoke Arabic had advanced degrees beyond college education versus none in the groups who spoke Amharic, Somali and Swahili.
Demographic characteristics of focus group participants.

Table 2 shows themes that emerged in response to the question ‘What do you consider to be a healthy diet?’ All four groups reported that a diet containing fruits and vegetables is healthy. The major themes in the Amharic group were organic foods and a desire to grow foods. Major themes from the Arabic group were that nutrients (fat, protein, carbohydrates and sodium), foods (eggs, honey, sugar and juice), organic foods and home-grown foods are important in a healthy diet. This group also identified a connection between diet and health. Major themes in the Somali group were that all foods can provide nutrition and there was discussion about fruits, vegetables and meats. A theme unique to the Swahili group was a consideration of fresh versus preserved foods when thinking about a healthy diet. For this question, one participant commented that she wanted to ‘learn to use health food’ while another commented on wanting study staff to ‘teach us about portion size.’ A third commented that ‘If [I] have information [I] will choose right foods because [I] don’t know, not [choosing unhealthy foods] on purpose.’
Themes about what is considered a healthy diet.

The number represents the number of people in the group who endorsed this theme for a healthy diet.
When asked about spices and herbs, 62 mutually exclusive spices were identified (Amharic: 9, Arabic: 38, Somali: 19, Swahili: 11). Themes included the use of spices and herbs in cooking and baking (Amharic, Arabic, Somali, Swahili), for teas (Arabic, Somali, Swahili), to treat colds and influenza (Arabic, Swahili) and to treat other illnesses (Arabic, Somali, Swahili). Many of the spices and herbs that were used overlap for each group, but with some combinations that are distinct to some regions (e.g. Beriberi for Amaharic group). It was reported that spices and herbs are obtained from participants’ home country by mail or direct transport after visiting home countries (Arabic, Swahili), from local shops catering for migrants (Amharic, Swahili) or neighbourhood stores (Arabic, Swahili). Due to time restrictions, this question was not answered in the focus group conducted in Somali.
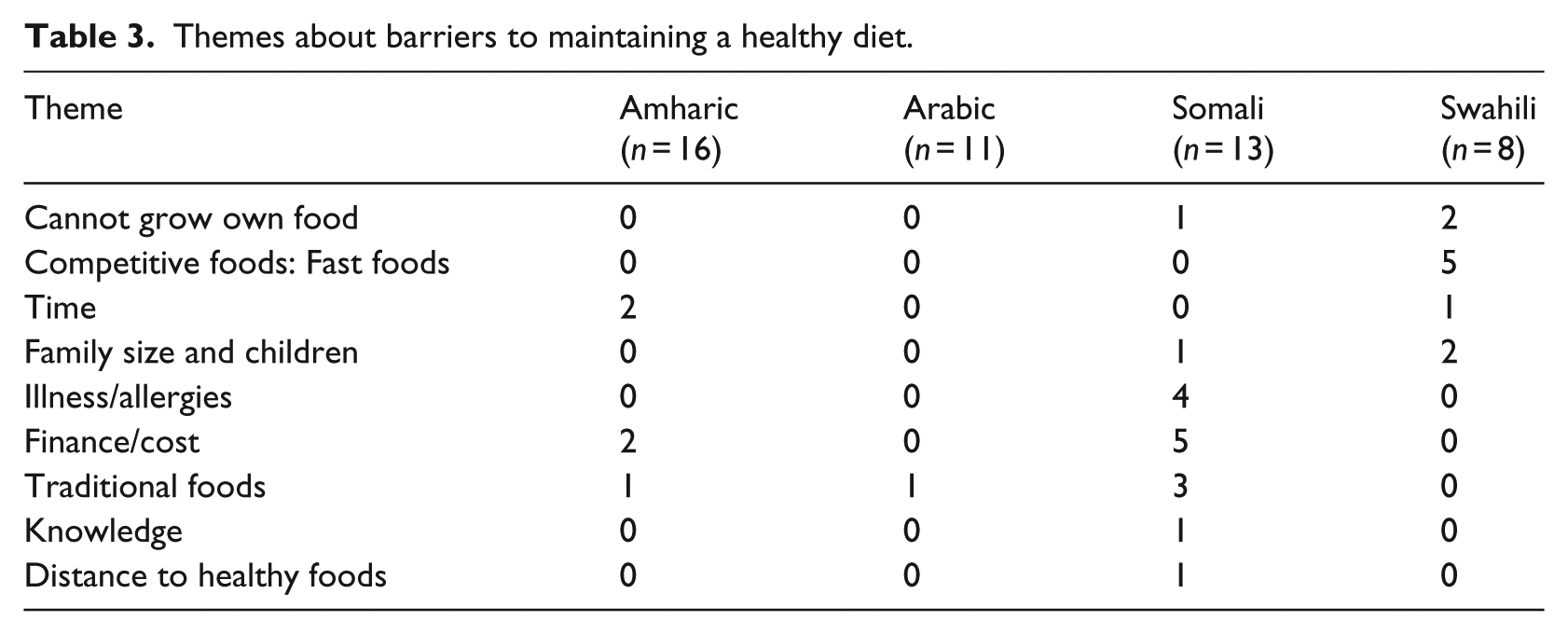
The themes related to barriers to maintaining a healthy diet are shown in Table 3. Barriers varied across groups and over 10 barriers were identified including constraints around growing one’s own food in the USA, family size, need to be cost-efficient (e.g. ‘if I buy healthy foods for everybody the food finishes in 10 days but what I need is food for a month’) and time-efficient (e.g. ‘because working, eat whatever instead of cutting a salad’ and ‘In Ethiopia we had time’), and a growing desire to serve fast food because their children ask for it, it is easy to find and it tastes good. One participant commented on the change in context where diet-related preventable diseases are the top causes of death in the USA: ‘[I] never see people get too sick in Ethiopia from food.’
Themes about barriers to maintaining a healthy diet.
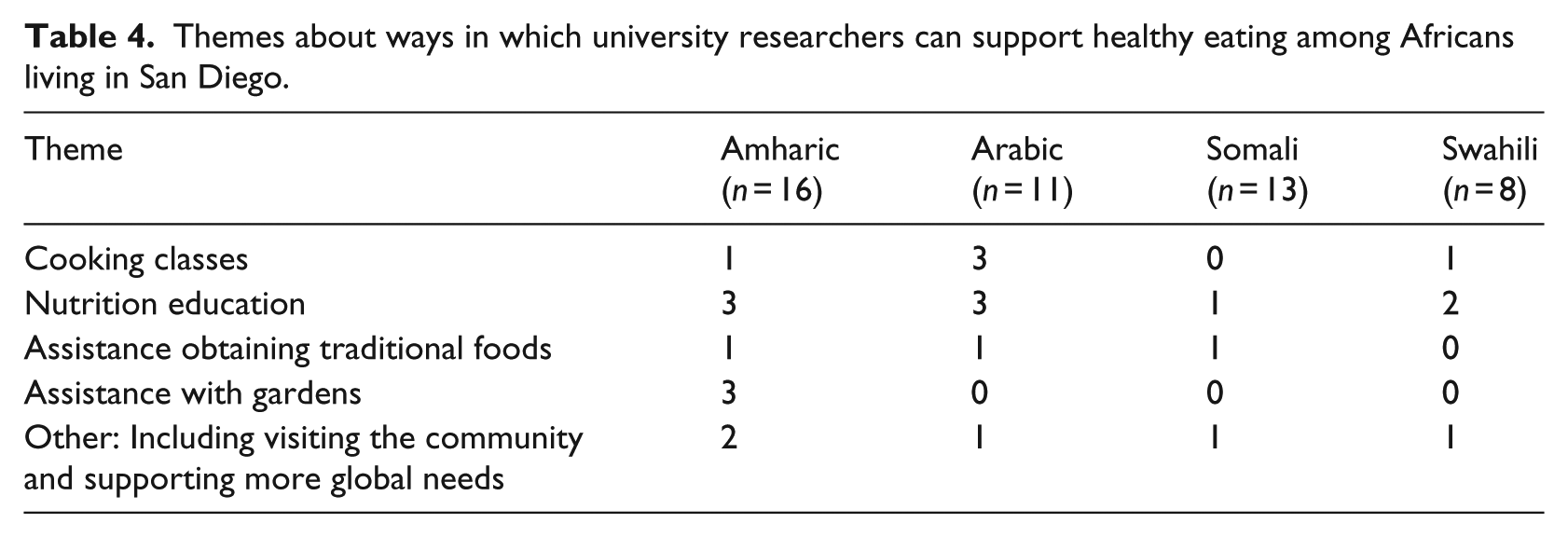
Across the focus groups, more than six ideas for continued collaboration between the university and community agency on nutrition topics were generated and are provided in Table 4. Themes included cooking classes, nutrition education and improving access to traditional foods, herbs and spices. Participants reported ‘[we need] space to garden and grow somewhere in the city that is for us’ but that there are challenges to growing food in their new environment. One participant said, ‘[We] would like to grow food but it is very wet at home and it is dry here and the mud might be bad.’ Opportunities for skills-based programmes and the sharing of traditional sources (e.g. seeds) and knowledge were identified as optimal points for intervention.
Themes about ways in which university researchers can support healthy eating among Africans living in San Diego.
Discussion
In this qualitative study of the nutritional practices among African women living in San Diego, participants reported (1) the use of 62 different spices and herbs and a desire to maintain use of traditional herbs and spices in meal preparation for flavour and health benefits; (2) multiple considerations for a healthy diet such as nutrients, foods, food groups and the approach to growing and preparing foods; (3) barriers to healthy eating including costs, constraints around growing food, family size and fast food; and (4) the strong desire to partner with the University for programmes/forums for sharing traditional foods and promotion of healthful nutritional practices across cultures.
To our knowledge, this is the first examination of the feasibility and acceptability of a nutrition intervention tailored to African populations living in the USA. Our findings indicate that barriers to healthy eating include cheap and convenient unhealthy foods. As immigrants and refugees acculturate to American society, pre-packaged and restaurant fast foods may be seen as an appealing option but the high consumption of these foods may result in diets that are inconsistent with the Dietary Guidelines for Americans. Given participants’ concerns about high BP, increased consumption of commercially prepared foods is concerning as it accounts for 80% of the dietary sodium intake in the USA (Anderson et al., 2010). Excess sodium intake is a risk factor for hypertension and cardiovascular disease, and the benefits of reduced sodium have been well documented (Appel et al., 2006, 2011; He and MacGregor, 2009). In addition, foods consumed in their home country may be prepared differently, and in less healthy ways, in the USA (i.e. self-rising flour added to injera, a staple Ethiopian flatbread commonly eaten with most meals, or use of preserved vs fresh products).
There are several strengths to our work. First, the study is a direct response to conversations between the UCSD and UWEAST teams to address concerns for UWEAST. The decision to include multiple African communities was made collaboratively with the community partner and follows CBPR methods (Israel et al., 2005) and recommendations for the dissemination of evidence-based programmes into community-based settings (Harris et al., 2012). Second, we address a pressing topic in preventive medicine by using a CBPR approach. Rigorous methods were used to obtain data that are mutually beneficial to the research partners. Third, these findings are likely to reflect honest opinions given trust established through prior work. 2
Our findings have clinical implications given the well-established relationship between dietary patterns and BP or clinically important parameters. In this study sample, the prevalence of hypertension ranged from 23%–33% and a healthy dietary pattern can reduce BP (Appel et al., 1997). Participants reported checking BP at home with many engaging in home BP monitoring an average of two times a month. This is a possible sign of interest in lifestyle interventions. Of those who reported having a diagnosis of hypertension, 12% reported taking anti-hypertensive medications. In the Swahili and Somali groups, 100% of those with diagnosed hypertension use anti-hypertensive medications in contrast to 63% in the group who spoke Amharic. Overall, of those who reported having a diagnosis of hypertension, 58% had an elevated BP reading highlighting a potential need to focus on management and control of hypertension in this population. Recent research has found that an intervention emphasising spices and herbs significantly reduced sodium consumption (~1,000 mg/day) when compared to a self-directed intervention that included only educational materials (Anderson et al., 2015). The acceptability of an approach of this type by African women was reinforced by focus group data.
There are also several public health implications of these findings. First, we address an important preventive health concern for a population that is underserved in San Diego. San Diego hosts one of the largest resettlement programmes in the USA, including one of the largest East African communities (Somali Family Services, 2009). Despite the unique health needs of people from a refugee background (Davidson et al., 2008), there is little research and few culturally adapted interventions. Second, there is a mutual interest between community and researchers in the prevention of diet-related health conditions that may occur after resettlement. Refugee resettlement represents one of the most controlled forms of human movement and provides unique opportunities for engaging in true preventive strategies to limit a rapid transition to incident chronic diseases. Finally, public health researchers and practitioners need effective strategies for addressing challenges to maintaining the authenticity of CBPR. Some of these challenges have been published, such as the onerous training and paperwork requirements for community members to accommodate university requirements and the time-consuming and longer-term perspective needed for truly collaborative efforts (Blumenthal, 2011). We felt these strains while trying to accommodate diverse timelines and varying responsibilities. The use of research ethics training designed for community researchers (Nebeker et al., 2015) along with development of the MOU helped to alleviate, but did not fully eliminate, those challenges.
Limitations
There are limitations of this work that should be considered. First, we were unable to obtain demographic data and BP measurements on all focus group participants. Obtaining these data was a secondary objective and asking the focus group questions was the primary. This experience taught us about technical and structural approaches that could be implemented in future work where clinical measurements are needed. Second, there is likely to be heterogeneity in the nutrition transition of Africans and the perceptions of spices and herbs in health and nutrition, and this may limit the generalisability of our findings. It is important to consider the heterogeneity present within and between all groups of people. This small-scale study aimed to gain insights into the experiences of local women coming from select countries in East and North Africa. Given the small sample and lack of representation across other regions, further research is needed to explore potential differences within and between different communities. We did not assess the women’s intentions to remain living in the USA, which may influence the extent to which they adopt local lifestyles and behaviours. Further investigation that examines variations in health behaviours and outcomes across different migrant groups (e.g. immigrants, refugees, temporary migrants) may identify differences to be considered in health programmes. Finally, our small sample size precludes us from looking at relationships between diet, demographics and disease, and this is a much needed area of future research.
Conclusion
Taken together, these findings suggest that a comprehensive and culturally informed behavioural intervention, focused on spices and herbs, would be feasible and acceptable for supporting adherence to the Dietary Guidelines for Americans in African migrant communities. Our work also reinforced that rigorous community-based research can result in mutual learning and equitable partnership.
Successful community engagement resulting in a strong and sustained community- academic partnership must be based on the premise that the community is an equal partner and that, while there are clear educational [research] goals …, the needs of the community must be put first. (Carney et al., 2011: s211)
Collaborative efforts such as those undertaken in this study are needed to accelerate progress towards methodologies which generate culturally competent knowledge that will not be viewed as inferior to clinical knowledge (Westerman, 2010). The results of this study will help ensure the development of culturally meaningful and accessible chronic disease prevention programmes that ultimately serve to improve dietary intake and practices.
Supplemental Material
0381-supplementary-file – Supplemental material for Community-based participatory approach to identify factors affecting diet following migration from Africa: The Hawaash study
Supplemental material, 0381-supplementary-file for Community-based participatory approach to identify factors affecting diet following migration from Africa: The Hawaash study by Cheryl AM Anderson, Kate E Murray, Sahra Abdi, Samantha Hurst, Amina Sheik-Mohamed, Bethlehem Begud, Bess Marcus, Camille Nebeker, Jennifer C Sanchez-Flack and Khalisa Bolling in Health Education Journal
Footnotes
Authors’ Note
Cheryl AM Anderson is also affiliated with Department of Family Medicine and Public Health, School of Medicine, University of California, San Diego, La Jolla, CA, USA.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by pilot research funds from the University of California, San Diego’s Department of Family Medicine and Public Health through the Center of Excellence in Health Promotion and Equity. Kate Murray was supported by MRSG-13-069-01-CPPB (American Cancer Society).
Supplemental material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.