
Abstract
Objective:
Human papillomavirus (HPV) vaccination rates among Hispanic adolescents in the USA are far below recommended levels. Using a social marketing theory framework, we assessed the four Ps (product, price, place and promotion) as they relate to efforts to promote HPV vaccine initiation.
Design:
Qualitative study involving in-depth interviews.
Setting:
A large Southern city in the USA.
Method:
Eighty-five in-depth qualitative interviews were conducted with Spanish-speaking Hispanic mothers divided into initiated and uninitiated market segments based on whether or not their adolescent child had received the first dose of the HPV vaccine. Data were analysed using directed qualitative content analysis.
Results:
Results suggest that the desire to prevent illnesses and protect their child drives the decision to vaccinate (product). Most initiated mothers did not experience barriers to vaccination, and market segments described different potential barriers (price). Both marker segments reported that they needed vaccine information before vaccinating (price). Finally, interventions should target clinics, schools and community centres to raise awareness about the importance of vaccinating against HPV (place and promotion).
Conclusion:
Findings from this formative study can inform the development of an intervention to increase HPV vaccine initiation among Hispanic adolescents.
Vaccinating against human papillomavirus (HPV) is critical to reducing the incidence of HPV-associated cancers. HPV vaccine was approved for use in young women and men between the ages of 9 and 26 in 2006 and 2011, respectively (Markowitz et al., 2014). The vaccine protects against seven high-risk HPV types known to cause cancer (Food and Drug Administration, 2014; Markowitz et al., 2014; Saraiya, 2015) and two HPV types that cause approximately 90% of all cases of genital warts (Markowitz et al., 2014). Two doses of the vaccine are recommended for individuals who initiate vaccination between the ages of 9 and 14, and three doses are recommended for individuals who initiate between the ages of 15 and 26. Individuals with compromised immune systems should receive three doses of the HPV vaccine regardless of age at initiation (Meites et al., 2016). Vaccine initiation rates, among Hispanic girls and boys between the ages of 13 and 17 in 2014 (in Texas) were 55.1% and 39.3%, respectively (Centers for Disease Control and Prevention [CDC], 2014). These rates are comparable to the initiation rates of White, non-Hispanic adolescent girls and boys (54.2% and 25.2%, respectively) and Black adolescent girls and boys (62.1% and 22.1%, respectively) (CDC, 2014). Current vaccination rates are far below the US Healthy People 2020 goal of 80% vaccine coverage (US Department of Health and Human Services, n.d.) and indicate a need to increase vaccination. Furthermore, the Cancer Moonshot Initiative Blue Ribbon Panel Report, 2016, highlighted the need to promote and increase HPV vaccination (Singer et al., 2016).
Previous studies have found that mothers are more often than not responsible for vaccinating their children (Fazekas et al., 2008; Leader et al., 2009; Sperber et al., 2008). Because of this, in order to increase HPV vaccine initiation rates among Hispanic adolescents, we need to know what factors mothers consider when making the decision to vaccinate their children (Jozkowski and Geshnizjani, 2016). Only then will we be able to develop effective interventions to increase vaccine initiation in this population. To this end, we must first select a conceptual/theoretical framework on which to base our behavioural model and intervention (Glanz and Bishop, 2010).
Social marketing theory offers one such framework. This theory, as applied to public health, employs the concepts and techniques used in commercial marketing to develop interventions (Bryant and Grier, 2005; Glanz et al., 2008). It is derived from the principles of marketing, including social exchange theory, audience segmentation and the marketing mix (Bryant and Grier, 2005; Emerson, 2015). Social exchange theory suggests that an individual makes the decision to engage in a behaviour after weighing the costs and benefits and then only if the benefits outweigh the costs (Emerson, 1976). Audience segmentation is the process of taking a population and dividing it into different groups or segments based on specific characteristics that are related to a given product (Forthofer and Bryant, 2000). The marketing mix, also known as the four Ps (i.e. product, price, place and promotion) form the central principles around which social marketing theory-based interventions are developed and implemented (Bryant and Grier, 2005; Glanz and Bishop, 2010). Product describes the benefits associated with a given behaviour. Price describes the potential costs associated with the behaviour. Place details where the behaviour will occur along with individuals or entities that provide information or other tangible goods that will facilitate the behaviour. Finally, promotion addresses aspects of designing and delivering messages about the behaviour.
Social marketing has been successfully applied in the field of public health to promote positive health behaviours including physical activity and healthy eating (Wong et al., 2004; Young et al., 2004), HIV prevention and testing (Gibson et al., 2010; Wei et al., 2011) and smoking cessation (Lowry et al., 2009; McCausland et al., 2009). We previously employed this framework to examine HPV vaccine series completion (Roncancio et al., 2017). However, given that factors predicting vaccine initiation and completion differ (Dorell et al., 2011), it is necessary to employ the theory to understand each behaviour separately. As such, the aim of this study was to apply social marketing theory to assess the needs and preferences of Hispanic mothers of adolescent girls and boys as related to initiating the HPV vaccine series. This will provide guidance for future interventions to increase HPV vaccine uptake. We proposed to identify the four Ps of social marketing theory, including the (1) benefits of having their child initiate the HPV vaccine series (product), (2) barriers associated with having their child initiate the HPV vaccine series (price), (3) location where mothers make decisions about or consider HPV vaccine uptake for their child (place) and (4) design and delivery of messages about HPV uptake to mothers (promotion).
Methods
We employed a qualitative research design in the form of in-depth interviews to better understand Hispanic mothers’ culturally specific values, attitudes and beliefs related to HPV vaccine initiation. In-depth interviews, using convenience sampling, were the chosen method of data collection because the topic under investigation is considered sensitive with respect to perspectives and experiences (Mack et al., 2005). Using Bryant and Grier’s (2005) definitions of the four Ps as a guide, we developed operational definitions for product, price, place and promotion.
Participants
We conducted 85 in-depth interviews with Spanish-speaking Hispanic mothers of adolescent girls and boys aged 11–17 from May 2014 through January 2015. Participants were recruited from community sites including back to school fairs, community outreach centres, health centres and clinics in Houston, Texas. Eligibility criteria included being women, self-identifying as Hispanic or Latino, speaking Spanish as a primary language and having a child between 11 and 17 years of age. We included mothers whose child had initiated the vaccine series and mothers whose child had not in order to identify the perspectives of both groups and increase our knowledge of the behaviour (Middlestadt et al., 1996). Participants were classified to a market segment, based on their child’s HPV vaccination status: uninitiated: daughter or son had not received any doses of the HPV vaccine, and initiated: daughter or son had received at least one dose of the HPV vaccine. Our sample consisted of 34 mothers of uninitiated girls or boys (18 mothers of girls and 16 mothers of boys) and 51 mothers of initiated girls and boys (32 mothers of girls and 19 mothers of boys).
Procedure
Women were approached in Spanish by a member of the research team and given a brief oral description of the study. The research team consisted of Hispanic women who were all native Spanish speakers. We explained the purpose of the study, eligibility criteria, length of the interview and incentive amount. Those who met eligibility criteria and were interested in participating provided written informed consent. Participants first completed a brief 15-minute demographic survey, which was administered by the interviewer. This was followed by the interview which was audio-recorded. Mothers were compensated $20 for their participation. All procedures were approved by the Institutional Review Board at the University of Texas Health Science Center–Houston (HSC-SPH-13-0594).
Interview instrument
Based on a literature review, we created interview guides for mothers from each market segment. The interview guides consisted of open-ended questions designed to elicit responses related to product, price, placement and promotion (Bryant and Grier, 2005; Parsons and McCormack Brown, 2004). Questions included, ‘What made/would make you decide to give your daughter/son the first dose of the HPV vaccine?’ and ‘What are the positive effects of having your child initiate the HPV vaccine series?’ (product); ‘What made/would make it difficult for you to have your child initiate the HPV vaccine series?’ and ‘What information did/would you need before deciding to give your daughter/son the first dose of the HPV vaccine?’ (price); ‘Where did you first hear about the HPV vaccine?’ (place); and ‘If you needed it, where did/would you look for information about the HPV vaccine?’ (promotion).
Data analysis
Interviews were transcribed verbatim by native Spanish speakers. Participants were not involved in the analysis and did not review transcripts before analysis. It is both common and recommended to take field notes during the interview process (Phillippi and Lauderdale, 2018). We took field notes at two points. The first was during the interview and the second was during transcription. Interviewers recorded the date of the interview, participants’ study identification number, setting of the interview and the presence of any other individuals during the interview. During transcription, notes and comments were added to provide non-verbal content (e.g. pauses and laughter). These notes provided additional context during data analysis.
We followed published recommendations for collecting and analysing qualitative elicitation interview data (Middlestadt et al., 1996). Given that we were guided by an existing theoretical framework, we employed directed qualitative content analysis (Hsieh, 2005). Specifically, we employed the Framework Method (Gale et al., 2013). Before initiating the coding process, the primary author read through all of the transcripts several times to obtain a sense of the data as a whole in relation to the four Ps. This step also facilitated the development of operational definitions. Then, the primary author read the transcripts line-by-line, highlighting and making notes of words that captured the operational definitions discussed for product, price, place and promotion. Through this process of open-coding, a list of code labels for each key concept emerged.
Then, as prescribed by the Framework Method (Gale et al., 2013), the primary author developed a spreadsheet with matrices for each interview question. Participants’ responses/quotes were entered into the rows and the codes were entered in adjacent columns at the top. Each coder received a copy of the spreadsheet and read each response and marked the cells under each code as appropriate. The interview transcripts were then independently coded by three members of the research team. All coders were Hispanic women and native Spanish speakers. Two coders were of Mexican ethnic origin and the third was a native of Argentina. Transcripts were coded in groups by child’s gender and number of HPV vaccine doses received (e.g. group 1: all mothers of girls who had not received any doses of the HPV vaccine; group 2: all mothers of boys who had not received any doses of the HPV vaccine; group 3: mothers whose daughters had one vaccine dose; etc.). Frequency counts of each code assigned to each participant for each question were calculated, and thus we were able to establish theme counts. All discrepancies between the three coders were examined, discussed and resolved. Given the diverse backgrounds of the coders, the discussion and resolution of coding discrepancies was crucial. Finally, we combined the group counts by market segment (i.e. uninitiated and initiated) to determine the frequencies of responses mentioned by each market segment.
Results
Examination of the demographic characteristics of the sample (N = 85) revealed that just over half of the participants were under the age of 40 (54.1%; mean = 39.9; SD = 6.8). Most were married (67.1%), had not completed high school (76.5%) and were non-US born (96.5%). Specifically, 58.8% were born in Mexico; 16.5% were born in El Salvador; 11.8% were born in Honduras; 4.7% were born in Guatemala; 3.5% were born in the USA; 2.4% were born in Nicaragua and 1.2% were born in Cuba. Regarding the characteristics of their adolescent children, as reported by the participants, 18.8% did not have insurance coverage and of those who did, 77.7% were covered by government subsidised insurance. The children were almost evenly split in terms of age with 34.1% between 11 and 12 years old, 38.8% between 13 and 14 years old and 27.1% between 15 and 17 years old.
Product
Mothers from the uninitiated market segment mentioned several factors that would make them decide to have their child initiate the HPV vaccine series. They included protection from HPV, receiving more information about the vaccine, preventing HPV and other illnesses, and speaking with the doctor about vaccination. We found that having information about the vaccine, initiated mothers reported that they had decided to have their child initiate the vaccine series: to prevent HPV and other illnesses, to protect their child from HPV, after speaking with the doctor about vaccination and after having more information about the HPV vaccine. The role of the doctor was found to be important in the decisions of initiated mothers to have their child initiate the vaccine series. The last deciding factor mentioned by both groups was the child’s opinion about being vaccinated. See Table 1 (Product a) for examples of participant responses.
Product.

HPV: human papillomavirus.
The majority of benefits mentioned were health-related. Mothers in the uninitiated group most frequently mentioned that the vaccine would provide protection for their child. Another health-related benefit of vaccinating mentioned was that the vaccine would prevent HPV and other illnesses. Mothers also expressed that the vaccine would be good for the child’s health. Everything was another frequently given response. The final health-related benefit mentioned most frequently was the vaccine serving its purpose and working as it is supposed to (i.e. preventing HPV). The initiated group cited the following health benefits: prevention of HPV and other illnesses, protection for their child, the vaccine is good for the child’s health, everything about the vaccine is good and the vaccine serves its purpose and works as it is supposed to. See Table 1 (Product b) for examples of participant responses.
The non-health related benefits reported by the uninitiated group were that initiating the vaccine series would provide an opportunity to teach their child about maintaining good health practices and provide the mother with a sense of security in knowing that the vaccine will keep her child healthy. We also found that some mothers believed that vaccinating would somehow positively influence their child’s behaviour. See Table 1 (Product a) for examples of participant responses.
Non-health benefits mentioned by the initiated group were that initiating the vaccine series provides an opportunity to teach their child about maintaining good health practices, a sense of security in knowing that the vaccine will keep her child healthy and a sense of comfort knowing that the child is up-to-date with her or his vaccinations. Some uninitiated and initiated mothers expressed their uncertainty about the positive effects of vaccinating. See Table 1 (Product b) for examples of participant responses.
Price
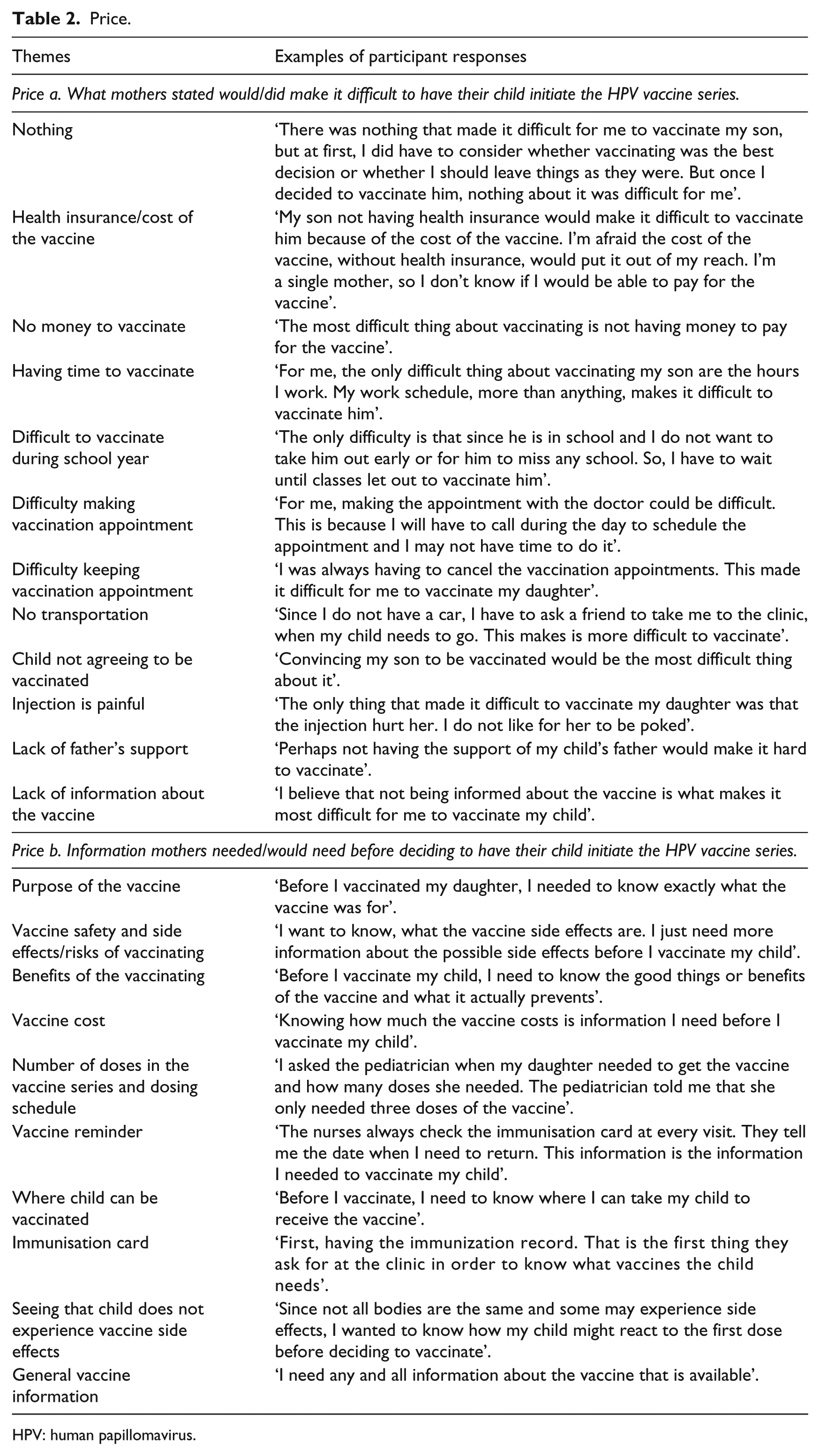
We identified the price or barriers to mothers having their children initiate the HPV vaccine series. Mothers in the initiated group listed twice as many potential barriers than the uninitiated group. However, the most frequently mentioned response to this question given by mothers in the initiated group was that nothing made it difficult for them to have their child initiate the vaccine series. Nothing was also the third most frequent response of the uninitiated group. See Table 2 (Price a) for examples of participant responses.
Price.
HPV: human papillomavirus.
The barriers, mentioned by the uninitiated group included not having health insurance, not being able to afford the cost of the vaccine and not having money to pay for the vaccine. Other barriers mentioned included not having a clinic nearby, the child not agreeing to be vaccinated, lack of father’s support and a lack of information about the vaccine. The barriers mentioned most frequently by the initiated group included not having health insurance, no transport, the injection being painful, not having time to take the child to be vaccinated, difficulty vaccinating during the school year because the child will have to miss school, and difficulty making and keeping the vaccination appointment. See Table 2 (Price a) for examples of participant responses.
Mothers in the initiated group listed more informational barriers or needs than the uninitiated group. However, we also found that more initiated mothers reported that they had all the information they needed about the vaccine compared to mothers from the uninitiated group. The informational needs mentioned by the uninitiated group included a lack of vaccine safety information including the side effects and potential risks, a need for general vaccine information, unawareness of the benefits of vaccinating and not knowing what the vaccine prevents. Other barriers not related to vaccine safety and benefits included not knowing what the vaccine will cost and not knowing where the child can be vaccinated. The informational needs mentioned, at least twice, by the initiated group included not knowing the purpose of the vaccine. General vaccine information, the benefits of vaccinating, information about the safety of the vaccine including the side effects and potential risks, knowing what the vaccine prevents and vaccine dosing information were other informational needs mentioned. Other informational needs about the HPV vaccine included not knowing the vaccine age recommendations, not knowing if the child would have a negative reaction to the vaccine, needing a vaccine reminder and not having the child’s immunisation card. See Table 2 (Price b) for examples of participant responses.
Place
The majority of mothers from the uninitiated market segment had not heard about the HPV vaccine before they participated in this study. Mothers from the uninitiated group who had previously heard about the vaccine primarily heard about it at the clinic. The television, the child’s school, the newspaper, a friend and a relative were other sources of information mentioned. Mothers from the initiated group primarily heard about the HPV vaccine on the television. Other sources from which mothers first heard about the vaccine included the clinic, a friend, a relative, the child’s school, a community centre and the Internet. See Table 3 for examples of participant responses.
Place: Where mother first heard about the HPV vaccine series.

HPV: human papillomavirus.
Promotion
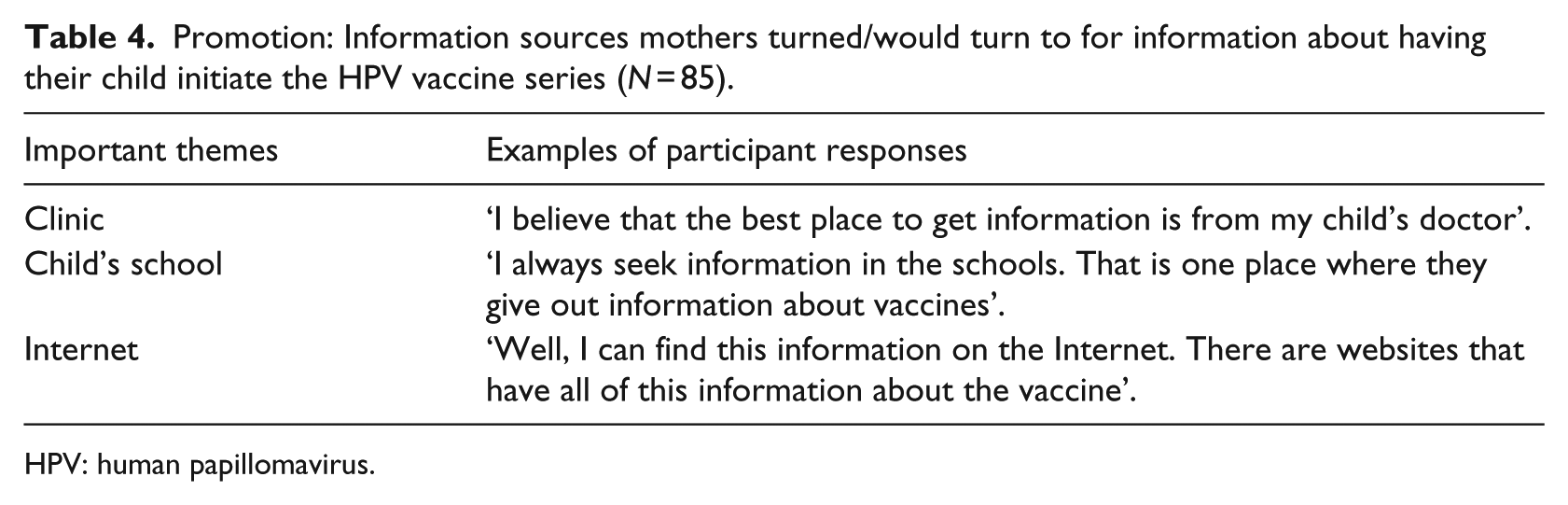
Both market segment groups mentioned the clinic as their most preferred source of information. The uninitiated group’s second most mentioned source which was the Internet. The other preferred informational source mentioned by the uninitiated group was a community centre. Other informational sources mentioned, by the initiated group, aside from the clinic, included the television, a brochure and the child’s school. See Table 4 for examples of participant responses.
Promotion: Information sources mothers turned/would turn to for information about having their child initiate the HPV vaccine series (N = 85).
HPV: human papillomavirus.
Discussion
Study findings add to existing knowledge of how we might effectively use social marketing theory to reach Hispanic mothers of adolescent girls and boys and encourage them to give their child the first dose of the HPV vaccine. We identified factors that influence mothers’ decisions to have their adolescent children initiate the vaccine series. In addition, we found a desire among Hispanic mothers to obtain different types of information about the HPV vaccine including benefits and safety information, and where they could take their child to be vaccinated. Finally, most of the mothers who had not heard about the HPV vaccine, before the interview, were mothers of boys. This is supported by the literature (Das et al., 2010) and indicates a need to increase awareness of the vaccine among mothers of boys.
Product
Both uninitiated and initiated market segments expressed the desire to protect their children and prevent HPV are strong drivers of vaccination. However, we found mothers in both groups who were unsure of the benefits of vaccinating. This is supported by existing research which shows low levels of parental knowledge about the HPV vaccine and parental desire for information about the vaccine (Katz et al., 2016; Kepka et al., 2012; Yeganeh et al., 2010;). Taken together, these findings indicate a need to provide members of this population with information about the vaccine. Furthermore, given that the child’s opinion about vaccinating was important to both market segments, we should provide HPV vaccine information for adolescent children and equip mothers with the skills to discuss the importance of vaccination with their children.
Price
Mothers identified barriers to vaccination that are similar to those described in previous studies (e.g. not having health insurance, not being able to afford the cost of the vaccine, not having a clinic and a lack of information about the vaccine) (Aragones et al., 2016; Holman et al., 2014; Katz et al., 2016; Walhart, 2012). Despite identifying more potential barriers, the majority of initiated mothers responded that nothing made it difficult for them to have their child initiate the vaccine series, suggesting that few mothers in the initiated group actually experienced barriers. As such, to mothers considering vaccination, we should emphasise that perceived barriers can be overcome or will not necessarily arise at all. One tactic might be to employ behavioural journalism (McAlister, 1995) by having initiated mothers share their experiences through testimonials.
The informational needs of the initiated group appear to be more practical or based on the process of vaccinating (e.g. knowing about the dosing schedule, receiving a vaccine reminder and having the child’s immunisation card to present to the doctor). These informational needs confirm previous research findings (Aragones et al., 2015; Javanbakht et al., 2012; Mills et al., 2013). Taken together, these findings suggest that interventions should create messages that provide the type of vaccine information we identified including instructions on how to prepare for the vaccination visit. It is also noteworthy that a lack of father support was mentioned as a barrier to vaccination by the uninitiated group. While it is common for mothers to be responsible for making vaccination decisions for young children (Fazekas et al., 2008; Sperber et al., 2008; Leader et al., 2009), this finding suggests that fathers’ influence on mothers’ decision to vaccinate requires additional investigation. For example, will providing communication strategies for mothers to discuss vaccination with their child’s father increase HPV vaccine initiation?
Place
There are five principal communication methods: intrapersonal, interpersonal, organisational, community and public/mass communication (Corcoran, 2007). Most mothers in both market segments first heard about the HPV vaccine and considered vaccination via community communication method (i.e. the clinic, the child’s school, a community centre and a community newspaper). Interpersonal communication methods were second (i.e. a friend or relative) followed by public/mass communication methods (i.e. television or the Internet). Our findings add to existing literature (Dorell et al., 2011; Grabiel et al., 2013; Maconachie and Lewendon, 2004) and further confirm that clinics (and doctors) are particularly important in raising HPV vaccine awareness and consideration of vaccination. They also suggest that public/mass communication methods can successfully raise HPV vaccine awareness and vaccination. Future research should further explore these communication methods and determine how we can effectively use each to increase HPV vaccination in this population.
Promotion
Community communication channels, especially clinics, were preferred by both market segments. While this is not surprising (Gargano et al., 2015; Grabiel et al., 2013), this finding underscores the importance of educating physicians, nurses and other clinic personnel about the importance of speaking with mothers about the HPV vaccine. In addition, public/mass communication channels (e.g. Internet, television and brochures) are the second most preferred information sources that could be used to disseminate messages to promote HPV vaccination.
Limitations
The limitations of the current study include the use of a convenience sample, which may be potentially limited by selection bias. In addition, as with all self-report data, participants’ responses may have been influenced by social desirability effects. In addition, our findings may not be representative of mothers who are not Hispanic or who do not speak Spanish. Also, 58.8% of our participants were of Mexican descent and the remaining participants came from a variety of Latin American ethnic backgrounds. It is possible that the beliefs of our large number of Mexican-origin participants drove the results, and findings may not accurately reflect the beliefs of participants from other ethnic backgrounds. There is also the possibility of interviewer bias because data were collected via one-on-one interviews. To minimise this bias, we used a structured interview guide and provided extensive training to our interviewers.
Conclusion
Overall, our findings point to a need for practical information regarding the HPV vaccine series and how mothers can obtain the vaccine for their children. Increasing HPV vaccination among Hispanic adolescents will reduce the rates of HPV-associated cancers in general and the cervical cancer health disparity among Hispanic women in particular. Comparing the attitudes and beliefs of mothers from both the uninitiated and initiated market segments provided important insights. Specifically, we were able to capture the perspective of those who had engaged in the behaviour and those who had not. This allowed us to examine similarities and differences in both groups. We identified preferred information channels, which can be used to disseminate messages that promote HPV vaccination. This formative research can inform the development of a social marketing intervention to increase HPV vaccine uptake among adolescent Hispanic girls and boys.
Footnotes
Authors’ Note
Angelica M Roncancio is now affilated with Department of Social Sciences, University of Houston-Downtown.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the US National Institutes of Health/National Cancer Institute (Grant number K01CA181437) and US National Institutes of Health/National Institute on Alcohol Abuse and Alcoholism (grant number K01 AA025992).