
Abstract
Objective:
With the increasing prevalence of unhealthy weight status in pre-school children, this study sought to understand pre-school child weight management practices in Blackburn with Darwen, UK, with a view to informing appropriate intervention strategies.
Design:
Mixed-methods study (semi-structured interviews, quantitative survey).
Setting:
Urban–rural borough with high ethnic diversity in the North West of England.
Methods:
Phase 1 involved 15 semi-structured interviews with public health/service managers, health professionals and children’s centre staff to explore current pre-school weight management practices, challenges and perceived training needs. Phase 2 involved a quantitative survey of multi-disciplinary health professionals (n = 30) who work with pre-school children. Data were analysed thematically and perceived challenges organised into individual, interpersonal and organisational levels of the socio-ecological model.
Results:
Current pre-school child weight management practices appeared to be inconsistent, and staff were unable to locate clear protocols or referral pathways. Challenges most commonly related to individual family factors (e.g. families not perceiving child’s weight status to be a problem) and organisational factors (e.g. lack of time). Perceived training needs differed between professions and included body mass index calculation and interpretation, weight-related communication and pre-school nutrition/physical activity guidelines.
Conclusion:
Inconsistencies in practice and a lack of clear pathways limited pre-school child weight management practices in Blackburn with Darwen. Although many challenges were attributed as external to the individual, potential steps to help practitioners cope with these demands are outlined.
Introduction
Childhood obesity increases risk of both physical and psychological health problems in later life (Van Grieken et al., 2013). In England, in 2017–2018, over one-fifth of 4- to 5-year-olds were overweight or obese (National Child Measurement Programme, 2018). While the majority of research into unhealthy child weight status has focused on overweight, recent global evidence suggests the incidence of child underweight may also be increasing (Wake et al., 2013). Little is currently known about the health status of underweight children, but available evidence indicates an association with adverse health in later childhood and adolescence (Wake et al., 2013). Given the growing incidence and health risks associated with both over- and underweight, it is important both are given consideration in the development of child weight management strategies.
Children’s eating and physical activity (PA) habits are thought to be established in the pre-school years (Wolman et al., 2008), with children as young as 3–5 years shown to associate food with health (Wiseman et al., 2018). The pre-school years are therefore an important time for health promotion and prevention of future weight problems (Buscemi et al., 2014). Although limited, research into the treatment and prevention of unhealthy weight status during the pre-school years has demonstrated some positive behavioural outcomes (for both children and their parents), for example, increased fruit and vegetable consumption, increased frequency of family meal times and positive changes in PA and screen time (Willis et al., 2016). Health professionals (e.g. general practitioners [GPs], nurses, health visitors [HVs]) and childcare staff in contact with pre-school children and their parents are in a key position to identify and address unhealthy weight status at an early stage.
Current guidance around managing pre-school child weight advocates that health professional interventions incorporate a number of components including PA, diet and engaging with the whole family to promote behaviour change (National Institute for Health and Care Excellence [NICE], 2015). However, more specific information appears to be lacking, especially with respect to underweight. While weight is regularly monitored for infants (up to 2 years) and school-aged children, weight checks for children aged between 2 and 4 years are not currently routine within the UK. When opportunities do arise to measure a child’s weight status, the stigma attached to childhood obesity presents challenges for health professionals in discussing the child’s weight with parents (Chadwick et al., 2008). Nurses and HVs have reported a lack of confidence, feelings of intimidation and a lack of capacity, training and protocols in child weight management (Turner et al., 2016; Willis et al., 2012). There is a need, therefore, to develop effective strategies to equip professionals working with young children to effectively identify and manage unhealthy child weight status in the pre-school years.
Previous studies have framed child weight management research within Bronfenbrenner’s (1979) socio-ecological model (SEM; e.g. Huang and Glass, 2008; Steele et al., 2011). The SEM highlights the importance of influences on child weight management practices at the individual (e.g. lack of family motivation), interpersonal (e.g. risk to relationships), organisational (e.g. job pressures) and societal levels (e.g. normalisation of overweight). Understanding pre-school child weight management practices and the challenges professionals face at each level may help to inform the development of effective interventions to promote a healthy weight status in pre-school children. This study therefore uses the SEM to explore current practices in pre-school child weight management in Blackburn with Darwen, a mixed urban–rural borough in the North West of England with a Black and Minority Ethnic (BME) population of 31% and high levels of both over- and underweight pre-school children (Lancashire City Council, 2011). The study was initiated following concern from local public health and primary care practitioners that pre-school child weight management practices in Blackburn with Darwen needed improvement. Intervention cannot, however, take place until policy-makers understand ‘what is happening now’ (Craig et al., 2008). This mixed-methods study therefore addressed the following three research questions:
What are the current practices for managing child weight in the pre-school years (2–4 years) in Blackburn with Darwen?
What are the challenges faced in managing pre-school child weight?
What training needs do practitioners perceive in relation to managing pre-school child weight?
Methods
Design
Mixed methods
This study used a mixed-methods design as neither a quantitative nor a qualitative approach alone would have achieved an understanding of the multiple perspectives required to address the research questions (Creswell, 2013). The qualitative phase (phase 1) explored the experiences of multi-agency stakeholders in managing pre-school child weight. These findings informed the development of an online survey conducted with a larger sample of frontline health professionals in the later quantitative phase (phase 2) of work.
Qualitative phase (phase 1)
Participants and recruitment
Recruitment for phase 1 involved purposive sampling, with the aim of recruiting multi-disciplinary professionals with some knowledge of, interest in or involvement in the current pre-school child weight management practices in Blackburn with Darwen. Invitation e-mails were distributed via research steering group members and representatives from the local Clinical Commissioning Group (CCG) (it is not, therefore, known how many professionals received this invitation). Fifteen multi-disciplinary professionals (four GPs, two HVs, three community nursery nurses [CNNs], two children’s centre staff, four public health/service managers) consented to take part. The majority of participants were women (n = 12), White British (n = 11) and worked full-time (n = 10). Practice experience ranged from 5 to 34 years, with a mean of 17.6 years.
Semi-structured interviews
Interview topics were informed by the child weight management literature and the study research questions and included exploration of current pre-school child weight management practices, challenges in managing pre-school child weight and perceived training needs. As participants’ roles in child weight management varied, two interview schedules were developed: the first for frontline practitioners and the second for public health/service managers (see Supplementary Material for interview schedules).
In line with qualitative recommendations (Creswell, 2013; Shenton, 2004), pilot interviews were conducted with two health professionals unconnected to the research project (a children’s nurse and a GP) and subsequent amendments made to improve the clarity of questions. To enhance trustworthiness, participants were assured of their anonymity and were informed that the research was part of a study exploring pre-school child weight management and was not auditing practice. Interviews lasted between 20 and 41 minutes (mean = 29.8 minutes) and were conducted at the participant’s place of work.
Data analysis
Interviews were audio recorded and transcribed verbatim by D.B. and imported into QSR NVivo 11 qualitative software program for analysis. Thematic analysis, drawing on guidance from Braun and Clarke (2006), was conducted by D.B. with frequent debriefing sessions with P.M.W.
Data analysis occurred in two stages. First, after the familiarisation process (reading and rereading transcripts), data extracts were assigned codes as close as possible to the participant’s own words. Second, after all interviews had been coded, codes were scrutinised for patterns and similarities to form inductive themes relevant to each research question, which were then further reviewed and refined.
This process revealed challenges in managing pre-school child weight (research question 2) that related to individual, interpersonal and organisational factors. Therefore, it was decided to organise the themes for research question 2 (challenges in managing pre-school child weight) within the SEM framework (Bronfenbrenner, 1979) to enable a deeper understanding of the levels at which challenges were occurring.
Quantitative phase (phase 2)
Phase 2 involved an online survey (informed by the findings of phase 1 and current literature) with frontline health professionals. The purpose of this phase was to explore the extent to which the qualitative findings were representative of the perspectives of a broader cohort of practitioners.
Participants and recruitment
Invitation e-mails containing a link to an online survey were distributed to eligible health professionals via service leads and representatives from the local CCG. The survey link was open for 6 weeks with reminders sent out bi-weekly. Practitioners were eligible if they were involved in providing health care for pre-school children within Blackburn with Darwen. While it was not possible to know how many practitioners received the e-mail invites, it is estimated there were approximately 100 GPs, 70 practice nurses, 42 HVs and 8 CNNs working in Blackburn with Darwen who were eligible to take part.
Thirty health professionals (10 GPs, 3 practice nurses, 10 HVs and 7 CNNs) consented to take part and completed the survey. The majority of participants were women (n = 22), White British (n = 22) and worked full-time (n = 17). Years of practice ranged from 2 to 35 years, with a mean of 11.4 years. Due to the anonymity of the survey, it was not known whether any of the survey respondents participated in the phase 1 interviews.
Measures
Online survey
D.B. designed the survey through an iterative process of input and feedback from all co-authors (a mixture of clinicians, academics and public health professionals). The survey was delivered through the Bristol Online Survey (BOS) platform. Staff had the flexibility to complete it at a time and place of their own choosing, and responses were anonymous (Evans and Mathur, 2005).
Survey sections
In line with phase 1, the survey contained three sections each relating to the study research questions. Questions included multiple-choice questions, Likert-type scales and open response questions. Likert-type and multiple-choice questions were compulsory to answer for the respondent to be transferred to the next page, whereas open response questions were optional. The measure to assess challenges in managing pre-school child weight was adapted from Wu and Steele (2011) for a UK pre-school population (see Supplementary Material for full survey).
As recommended by Van Teijlingen and Hundley (2002), the survey was piloted with a GP and children’s nurse unconnected to the research study to check for understanding. No changes were made following the pilot testing, other than minor amendments to grammar and spelling.
Data analysis
Survey data was directly exported into SPSS 23 for analysis. Frequencies, percentages, medians and interquartile ranges were calculated where appropriate. To enable a comparison of results with phase 1, a secondary analysis of the data for research question 2 was conducted to group perceived challenges into the appropriate level of the SEM.
Ethical approval
Ethical approval was obtained from Liverpool John Moores University research ethics committee for both phases of the study (16/SPS/007, 16/SPS/027).
Results
Results from phases 1 and 2 are integrated and presented for each research question. Data for all professions are presented together, and differences are highlighted where relevant. Verbatim quotations with participant identifiers provide illustrative examples from interviews.
Current practices for managing child weight in the pre-school years (2–4 years)
Identifying weight status
Almost half of the interview participants indicated visual assessment as being an important cue for identifying weight status (‘[before weighing] you can see they are overweight’, GP 4). This was supported by survey findings that showed 83% (n = 25) of respondents would use visual assessments either always (40%, n = 12) or most of the time (43.3%, n = 13). It was acknowledged by interview participants that by weighing only those children who visually appeared to be over- or underweight, milder cases of unhealthy weight status might be missed. Interview participants also identified using growth charts, as recommended in their training (‘we put them on the chart and then obviously we follow the growth policy’, CNN3). This was supported by survey findings that showed that 63.3% (n = 19) of respondents would use growth charts ‘always’ (n = 13, 43.3%) or ‘most of the time’ (n = 6, 20%). None of the interview participants and only four (13.3%) survey respondents reported using body mass index (BMI) to identify a child’s weight status, with over half of the survey respondents saying they would ‘never’ use BMI (n = 17, 56.7%).
Communicating weight-related topics
Most interview participants stated that if they had concerns about the child’s weight status, they would raise these with parents (‘I would address it even if that wasn’t what they’d come for’, GP3). However, there were inconsistencies in practice, with other GPs indicating that unless a parent raised concerns about the child’s weight they would not discuss it. Some participants indicated that parental attitudes prevented them from addressing children’s unhealthy weight status due to concern of negative reactions. They noted the importance of a good relationship with families in facilitating weight-related conversations and parents’ acceptance of any advice or guidance given (‘I do manage to talk without offending them [parents] and the important thing is you don’t need to offend the parents so they don’t come back to you’, GP4). Growth charts were often used as an objective tool to raise unhealthy weight status with parents, providing an opportunity to relate their child’s position on the chart in comparison with where they should be (‘I think having the centile chart is a really good thing because obviously you can use that as a visual aid and parents can understand’, HV1). While survey responses suggested professionals were marginally more likely to raise the issue of overweight with parents (n = 22, 71.0%) than underweight (n = 20, 64.5%), interview participants indicated finding underweight easier to discuss as it can be attributed to more external contributory factors (e.g. fussy eating), thus reducing the onus on parental responsibility.
Practitioner interventions
After identifying unhealthy weight status in a pre-school child, interview participants reported employing their own interventions, for example, making further assessments (‘I might ask them to keep a food diary’, CNN3), providing advice and support to families (‘I may leave them with some literature to have a read of or websites to go on’, CNN 1), or arranging a follow-up appointment to assess the family’s progress in implementing any advice given (‘I might just sort of say, would you like some advice about that, you know, shall we weigh and measure them again sometime’, GP2). Survey findings suggested practitioners were slightly more likely to offer a follow-up being if the child was underweight (n = 12, 38.7%) compared to overweight (n = 10, 32.3%). A few interview participants noted that the results of any follow-up assessments provided additional information to pass on in case of referral.
Signposting and referrals
Interview participants reported referring to either local services (‘they’ve got the local children’s centres that we can refer to who run some physical activity sessions and things like that’, CNN1) or appropriate health professionals. It was suggested these referrals were in line with current guidance (‘there is a growth policy – if it crosses over more than two centiles up or down it is a referral to the GP’, HV1). Survey findings indicated little variation in referrals to specialist paediatric services. Professionals were marginally more likely to refer an underweight child to a paediatrician (n = 17, 56.6%) than an overweight child (n = 15, 50%). Respondents were, however, more likely to refer an overweight child to leisure centre services (n = 11, 35.5%) than an underweight child (n = 2, 6.5%). Knowledge of referral routes and services appeared to vary between individuals, with some interview participants reporting knowledge of referral routes and available services and others indicating little knowledge outside of their professional role.
Challenges faced in managing pre-school child weight
The challenges to managing pre-school weight identified in both phases of the study have been grouped into the appropriate level of the SEM. Challenges identified through the interview phase are displayed in Table 1 alongside verbatim quotes. Survey findings are displayed in Table 2, along with medians and interquartile ranges.
Challenges faced in managing pre-school child weight mapped in line with the socio-ecological model (SEM).
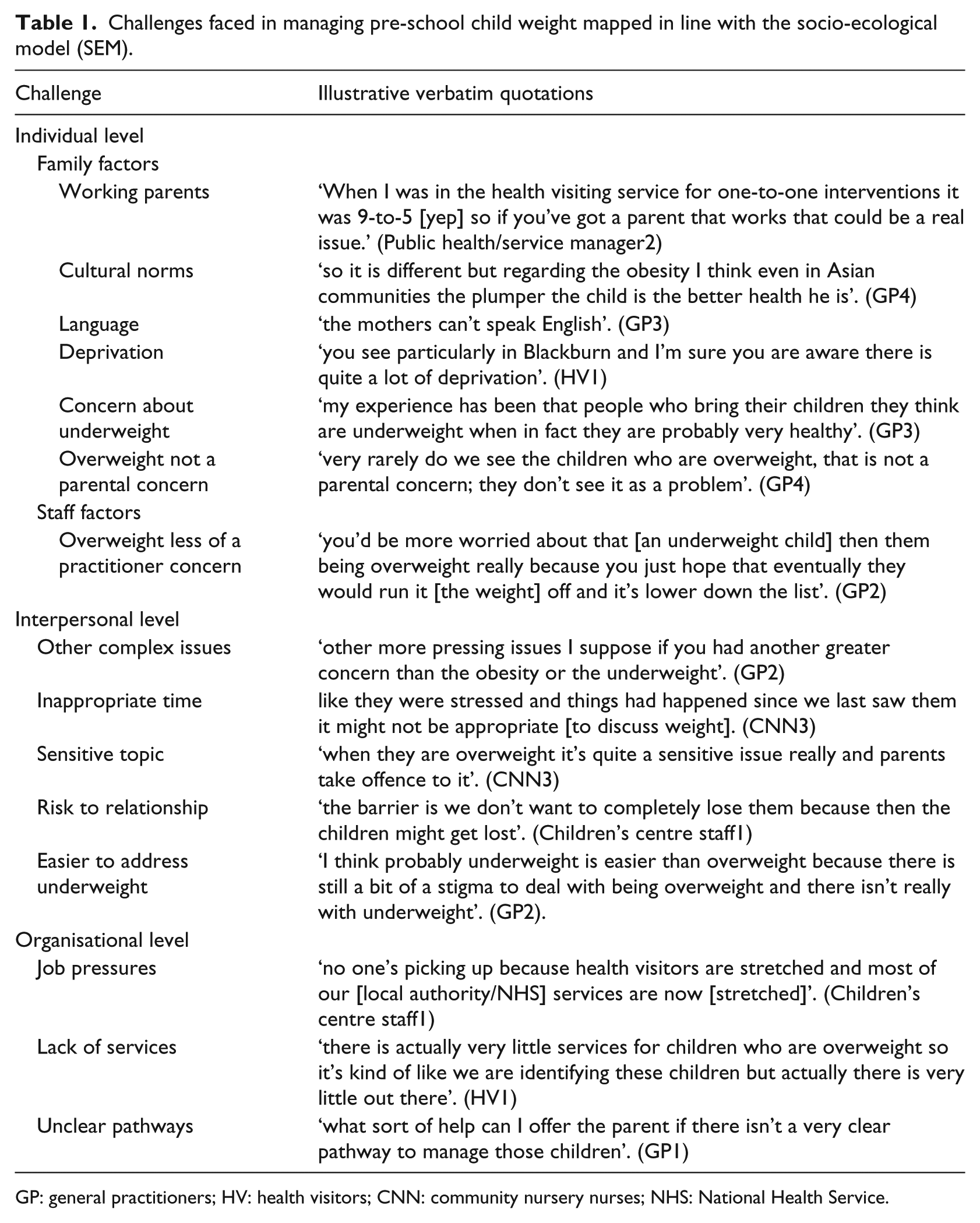
GP: general practitioners; HV: health visitors; CNN: community nursery nurses; NHS: National Health Service.
Median and interquartile range (IQR) for perceived barriers to pre-school child weight management (1 = not at all a barrier; 6 = very much a barrier).

BMI: body mass index.
A median score ≥4 suggests the issue was on average perceived as a barrier.
Factors perceived as a barrier (i.e. score 4 or above) are in bold.
Individual factors
In terms of family factors, interview findings highlighted that pre-school child weight management services are often inaccessible to working parents. Interview and survey results highlighted that familial demographic and cultural factors might pose a challenge in managing pre-school child weight, such as limited resources (Mdn = 4, IQR = 2), lack of proficiency in English (Mdn = 4, IQR = 3) or cultural norms that may favour a larger body size. Weight-specific challenges were identified by interview participants, such as parents expressing concern that their child was underweight when the child’s weight status was in fact healthy. Equally, where overweight was not deemed to be a concern for parents, this presented a challenge for survey respondents (Mdn = 5, IQR = 2). Only one individual staff barrier was identified in the interview phase relating to a lack of practitioner concern about overweight. Survey findings indicated that participants did not see staff factors as a barrier to managing pre-school child weight.
Interpersonal Factors
A number of interpersonal challenges were identified in the course of the interviews. Participants described how on some occasions it felt inappropriate to raise a child’s weight status due to other complex issues, for example, a complex or ‘chaotic’ home environment or child protection concerns. Overweight was viewed as a sensitive topic with stigma attached to it, and participants reported concerns that raising weight status could risk damaging relationships with families. In the survey, however, neither ‘feeling that it was an inappropriate time’ nor ‘worrying about harming their relationship with parents’ was seen as a notable challenge to addressing pre-school children’s weight-related health (both Mdn = 2, IQR = 2).
Organisational factors
Interview participants frequently reported job pressures as challenges to managing pre-school child weight, including factors such as lack of time and capacity, being understaffed, competing organisational priorities and stretched services. Survey data supported these findings, with both lack of time and lack of resources highlighted as challenges (both Mdn = 4, IQR = 2). Additional challenges identified through the interviews included insufficient and unclear pathways and referral routes. This knowledge differed between individuals, with a number of interview participants stating that even if they did identify unhealthy weight status in a child, they would not know what to do next. Survey data, however, indicated that being unfamiliar with local services (Mdn = 3, IQR = 4) and referral routes and pathways (Mdn = 3, IQR = 3) were not major concerns for participants.
Perceived training needs in relation to managing pre-school child weight
In both the interviews and survey, participants indicated the need for additional support and updates on managing pre-school child weight. Of the options provided in the survey (BMI calculation and interpretation, growth charts, weight-related communication, pre-school nutrition and PA guidelines), the highest reported training need was BMI calculation and interpretation (66.6%, n = 20) and the lowest was growth charts (20.0%, n = 6). In the interviews, GPs in particular identified a lack of training in managing pre-school child weight. This was reflected in the experiences of other health professionals (‘usually they [parents] will say the GP didn’t want to look at my [red] book [personal child health record] or didn’t understand what the centiles were for so it’s quite clear that they haven’t really got a clue’, CNN3).
In both the interviews and surveys, perceived training needs varied between professions. Most interview participants (CNNs, HVs and children’s centre staff) were confident in child health promotion and communication, whereas GPs indicated a lack of child-specific training (‘we had training about communication in the context of breaking bad news [yes] but not really addressing weight issues in toddlers and children’, GP1). Similarly, in the survey phase, 17 participants (54.9%) did not think they needed further training in child weight–related communication, with only one CNN indicating a training need (14.3%) compared to 100% (n = 3) of practice nurses and 60% (n = 6) of GPs. Over half of the survey participants (51.6%, n = 16) indicated a need for training in pre-school nutrition guidelines, particularly GPs (n = 7, 70%) and practice nurses (n = 3, 100%). The need for training in pre-school PA guidelines was reported by GPs (n = 9, 90%) and practice nurses (n = 3, 100%) compared to just one CNN (14.3%) and two HVs (20%). Interview participants from all professions indicated a need for greater knowledge of referral pathways and more regular training updates and refreshers.
Discussion
The aim of this study was to improve understanding of multi-agency pre-school (2–4 years) weight management practices in Blackburn with Darwen, a mixed urban–rural borough in the North West of England. The study found inconsistencies in pre-school child weight management practices within and between professional groups. The most frequently cited challenges related to individual family factors within the SEM, for example, low socio-economic status and families not perceiving the child’s weight status to be a problem. Perceived training needs differed between professions and included BMI calculation and interpretation, weight-related communication and pre-school nutrition/PA guidelines.
For health professionals to manage pre-school child weight, they need the skills and knowledge to identify whether a child’s weight status is healthy for their age and sex. This study, however, found inconsistencies in the measures used to assess pre-school child weight status. Participants in the interviews and surveys reported using a mixture of observation and growth charts. Consistent with previous research findings (Edvardsson et al., 2009; Regber et al., 2013), growth charts were perceived to be useful as an objective visual tool to assist parental understanding, provide reassurance or highlight an unhealthy weight status. Despite this, the majority of participants reported, at least in part, using visual cues to assess child weight status. This is concerning given health professionals have been shown to be poor at visually identifying children’s weight status (Robinson, 2017). Similarly, the use of BMI (to be converted to centiles for age and sex) was limited to only a few practitioners, despite being recommended as best practice by the Royal College of Paediatrics and Child Health (RCPCH, 2013) and advocated in the Blackburn with Darwen local growth policy. It was not, however, possible from our data to know whether participants who used BMI were able to interpret this appropriately in relation to age- and sex-specific centiles. While specific reasons were not provided for the lack of BMI use, it was notable the health visiting team was trained to use growth charts but not to calculate BMI or BMI centiles, and interview participants perceived a lack of clear guidance about best practice for pre-school child weight management, as reported elsewhere for school-aged children (Turner et al., 2016). Other studies have found practitioner reluctance to use BMI due to a perceived inability and lack of time to compute centiles (Barlow et al., 2007; Regber et al., 2013) and a lack of faith in BMI as a measure (Isma et al., 2012; Turner et al., 2016).
Although the current study focused on pre-school children, many of the challenges identified were consistent with findings from a recent meta-synthesis focused on children of all ages (Bradbury et al., 2018). In both studies, family factors (e.g. lack of parental concern over the child’s weight status, limited family resources) were cited as key challenges to managing child weight. These challenges were perceived by practitioners as outside their control and as inhibitive to families’ motivation to implement lifestyle changes. Although such findings suggest a tendency for practitioners to attribute barriers externally (i.e. to families rather than themselves), interventions to train staff in motivational interviewing (e.g. Bonde et al., 2014) have shown that development of psychological skills such as empathy and reflective listening can enhance the ability of practitioners to foster motivation in parents.
Unlike previous studies with school nurses (Kubik et al., 2007; Moyers et al., 2005; Steele et al., 2011; Turner et al., 2016), our multi-disciplinary sample did not report a perceived lack of knowledge or competency in managing pre-school child weight management. It is possible our participants had high levels of perceived competence in their practice. However, demand characteristics such as not wanting to admit to, or perhaps not being aware of, a lack of knowledge or competency may have contributed to these findings (Campinha-Bacote, 2003). GPs and practice nurses, however, indicated an awareness of their lack of expertise in the pre-school age group, highlighting need for training in areas including identifying weight status, nutritional and PA guidelines. This is likely to be attributable to the remit of their generic professional roles, when compared to health visiting and children’s centre staff who were specifically trained to work with children aged 0–5 years.
Blackburn with Darwen is an area of high ethnic diversity, and participants in our study cited challenges relating to ethnicity and cultural differences (e.g. cultural views of body size, language barriers). Given that parents from different ethnic backgrounds may perceive different body sizes as healthy (Trigwell et al., 2014), it is relevant to consider how pre-school child weight management practices can best support families from multiple ethnic backgrounds. It has been suggested that specific cultural knowledge is not necessarily required when addressing child weight–related health issues (Leonard, 2001; Purnell, 2012). Rather, what is needed is a recognition of the impact of culture on health behaviours and a willingness to explore and respect cultural views when addressing health problems.
There has been little published research on weight-related communication with families of pre-school children, but weight-related communication has been consistently identified as a challenge by health professionals working with school-aged children (Findholt et al., 2013; Kubik et al., 2007; Steele et al., 2011; Turner et al., 2016). In interview, a small number of participants identified areas that would prevent them from discussing a child’s weight status with a family, such as competing family demands and a fear of parental reactions. In addition, some GPs indicated that unless a parent raised concern about their child’s weight status, they would not discuss it. In the survey responses, however, communication was not identified as a challenge, although some professional differences emerged with GPs and practice nurses identifying communication as a training need. This is inconsistent with previous research which suggests health professionals face many barriers to child weight–related communication (Bradbury et al., 2018; Chadwick et al., 2008). There are a number of possible explanations for this inconsistency. Our sample may have been highly engaged practitioners with well-developed communication skills, there could be a mismatch between perceived and actual abilities, or health professionals may have been exhibiting ‘unconscious incompetence’ where they were unaware of the skills that they do not have (Campinha-Bacote, 2003). It is also possible challenges related to discussing weight status with school-aged children (e.g. children being able to understand the discussions, fear of instigating disordered eating; Findholt et al., 2013; Jones et al., 2014) may not be relevant when working with younger children.
A number of organisational challenges to managing pre-school child weight were identified, including job pressures, time and insufficient resources, which have all been reported as challenges to managing child weight elsewhere (Bradbury et al., 2018). A number of gaps in participant knowledge around the provision of services were also identified. Interview findings indicated a need for greater clarity and dissemination of pathways and referral routes for both over- and underweight. At times, the lack of clear pathways was cited as a disincentive to address children’s weight-related health issues. While this was not identified as a challenge in the surveys, to our knowledge no local care pathway in Blackburn with Darwen existed at the time of the study. Unclear weight management protocols are widely found when examining practice around children of all ages (Jones et al., 2014; Morrison-Sandberg et al., 2011; Turner et al., 2016). This highlights the importance of, and the need for, standardised practice and the development of clear child weight management care pathways (as outlined by NICE, 2018).
Strengths and limitations
Employing a mixed-methods approach enabled a deeper exploration of current pre-school weight management practices than would have been possible using either a quantitative or a qualitative approach alone. Unlike most previous research, the present study explored practitioner experiences of addressing both under- and overweight and their experiences of discussing these with the families of pre-school children. Mapping the challenges faced in practice to the SEM allows for the identification of multiple level factors to inform future interventions by both practitioners and policy-makers. Furthermore, this study was driven by local public health need and carried out by a multi-disciplinary research team comprising practitioners, academics and public health specialists. Such multi-disciplinary collaboration is important in bridging the gap between academic research and public health priorities, ensuring child weight–related research remains timely and relevant for practice (Watson et al., 2013).
In order to overcome the limitations of much mixed-methods research (Sparkes, 2015), the study aimed to integrate the qualitative and quantitative study findings (as advocated by Creswell et al., 2011). This required the integration of data from a survey (that included an adaptation of a previously validated questionnaire) with findings that emerged through semi-structured interviews. It is possible the different terminology and descriptors used within the survey and interviews may have contributed to some of the inconsistencies in findings.
Moreover, as study participants were volunteers (and in the case of interview participants were known to have a particular interest in pre-school child weight management), it is possible they were a compliant sample and caution should be taken when generalising to the wider workforce. In addition, the small numbers of participants from each professional group means any differences between professions may be due to individual rather than professional factors and should be viewed with caution. It is important to consider that both stages of the study relied on self-report; thus, responses reflect what participants perceived themselves as doing, rather than their actual behaviour during clinical contacts.
Conclusion
Tackling unhealthy weight status early in a child’s life is important in order to avoid potential physical and psychological health problems in adulthood. Pre-school-aged children generally have limited contact with health professionals. When contact does occur, it provides a valuable opportunity to identify unhealthy weight status and offer interventions. This study adds to the limited research in pre-school child weight management and how it is managed by multi-disciplinary professionals. The study found inconsistencies in practice in managing pre-school child weight both within and between professional groups. A number of training needs for health professionals emerged, including identifying and communicating weight status with parents and the need to develop clear weight-related protocols and pathways. Future research should be directed towards developing multi-disciplinary interventions to promote evidence-based pre-school child weight management practices.
Supplemental Material
Supplementary-resources-18-0147.R2 – Supplemental material for Multiple stakeholder views of pre-school child weight management practices: A mixed-methods study
Supplemental material, Supplementary-resources-18-0147.R2 for Multiple stakeholder views of pre-school child weight management practices: A mixed-methods study by Daisy Bradbury, Lorna Porcellato, Hannah Timpson, Gillian Turner, Shirley Goodhew, Ruth Young, Nabil Isaac and Paula M Watson in Health Education Journal
Footnotes
Acknowledgements
The authors wish to thank the study participants for their time and Anna Chisholm for advice provided as part of the wider project steering group. Ruth Young sadly passed away in December, 2018. She will be fondly remembered and we wish to dedicate this manuscript to her memory.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a doctoral grant to Daisy Bradbury, co-funded by Blackburn with Darwen Borough Council and Liverpool John Moores University.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.