
Abstract
Objectives:
To explore the preliminary effects and acceptability of a co-produced physical activity referral intervention.
Study Design:
Longitudinal design with data collected at baseline and post a 12-week physical activity referral intervention.
Setting:
Community leisure centre.
Methods:
In all, 32 adults with controlled lifestyle-related health conditions took part in a physical activity referral intervention (co-produced by a multidisciplinary stakeholder group) comprising 12 weeks subsidised fitness centre access plus four behaviour change consultations. A complete case analysis (t-tests and magnitude-based inferences) was conducted to assess baseline-to-12-week change in physical activity, cardiometabolic, and psychological measures. Semi-structured interviews were conducted (n = 12) to explore experiences of the intervention.
Results:
Mean improvements were observed in cardiorespiratory fitness (3.6 mL kg-1 min-1 [95% confidence interval: 1.9–5.4], p < .001) and moderate-to-vigorous physical activity (12.6 minutes per day [95% confidence interval: 4.3–29.6], p = .013). Participants were positive about the support received from exercise referral practitioners, but experienced some challenges in a busy and under staffed gym environment.
Conclusions:
A co-produced physical activity referral intervention elicited short-term improvements in physical activity and cardiometabolic health. Further refinements may be required, via ongoing feedback between stakeholders, researchers and service users, to achieve the intended holistic physical activity focus of the intervention, prior to a definitive trial.
Introduction
Physical inactivity (defined as not meeting guidelines of 150 minutes moderate-intensity physical activity [PA] per week) is the fourth leading cause of death worldwide (World Health Organization [WHO], 2018) and contributes to more than a quarter of deaths in the UK (British Heart Foundation [BHF], 2017). The greatest public health gains can be realised by supporting those who are most inactive to engage in at least a low level of PA, even if the full recommended dose (i.e. 150 minutes per week) is not achieved (Department of Health [DoH], 2004; Ekelund et al., 2016). For individuals with health conditions, PA is well-established as an efficacious ‘treatment’ (Kelly et al., 2013; Vuori, 1998), yet evidence typically stems from efficacy trials conducted in highly controlled environments (Beedie et al., 2015). Such evidence is difficult to translate to real-world (uncontrolled) environments (Public Health England [PHE], 2014) and research is therefore needed to explore how to effectively facilitate PA behaviour change within an ecologically valid environment.
Co-production that engages multiple stakeholders (e.g. policy-makers, practitioners, service-users) in intervention development may facilitate the translation of evidence to practice (Cornwall and Jewkes, 1995; Glasgow et al., 2003) through improved intervention context-sensitivity and acceptability, resulting in better chances of implementation success (Harden et al., 2016; Leask et al., 2017). The UK PA referral system is one field that might benefit from co-production. Traditionally coined ‘exercise referral’ or ‘GP referral’, interventions typically involve healthcare professionals referring inactive individuals with controlled health conditions and/or lifestyle related risk factors to 12- to 16-week gym-based exercise programmes (Pavey et al., 2011b). There are ~600 different referral interventions in operation in the UK, but despite recent promise (Stewart et al., 2017), evidence supporting their effectiveness is limited (Campbell et al., 2015). Focus continues to be on exercise prescription and few schemes have been underpinned by behaviour change theory (Beck et al., 2016; Dugdill et al., 2005). Furthermore, the failure to involve service-users and other stakeholders in development phases may compromise intervention acceptability (Beck et al., 2016; Din et al., 2015).
To overcome such challenges, we co-produced a PA referral intervention with multidisciplinary stakeholders (commissioners, practitioners, service-users and academics) that was evidence-based, drew on behaviour change theory and deemed feasible to implement within local infrastructures (Buckley et al., 2018). Underpinned by self determination theory (SDT; Ryan and Deci, 2000), the co-produced intervention differed from usual care in its focus on PA behaviour change (rather than exercise prescription), and inclusion of frequent one-to-one consultations with exercise referral practitioners (rather than formal contact at induction only). While the intervention framework was deemed feasible by multiple stakeholders in the co-production group, it was not known whether the intervention would be acceptable or effective when implemented in practice. Such evidence is crucial if we are to understand the relative value of co-production as a methodological approach. Yet, despite the growing popularity of co-production as a public health methodology (Batalden et al., 2016; Osborne et al., 2016; Rycroft-Malone et al., 2016), few reports are available documenting ‘what happens next’. The aim of this study was therefore to explore the preliminary effects and acceptability of a co-produced PA referral intervention (Buckley et al., 2018), with a view to informing intervention refinement prior to a subsequent experimental trial. This phased approach is advocated by the UK Medical Research Council (MRC) to ensure complex interventions are developed to the point they can have a worthwhile effect prior to investment in substantive trials (Craig et al., 2008).
Methods
Study design and context
The study took place in a city in the north-west of England with large areas of socio-economic deprivation (PHE, 2018). At the time of the study, a standard exercise referral programme was in place, delivered through 11 local authority fitness centres. Once referred by a health professional, participants were able to choose the centre most appropriate/convenient for them. The standard programme involved an induction with an exercise referral instructor, followed by 12 weeks’ subsidised access to gym, swimming and classes at the fitness centre. The co-produced intervention was piloted in 1 of the 11 fitness centres (Centre A), selected due to the centre’s local popularity and due to the involvement of centre staff in the co-production phase (Buckley et al., 2018). The study used a mixed-methods, pre-post design to explore preliminary effects and acceptability of the co-produced PA referral intervention.
Co-produced intervention
The co-produced intervention aimed to support participants to make gradual, sustainable changes to their PA levels. Participants received the same 12 weeks subsidised access to a fitness centre (swimming, gym and group classes) as the standard exercise referral scheme, plus a series of one-to-one behaviour change consultations (60-minute induction followed by 30-minute consultations at weeks 4, 12 and 18 [follow–up]). A log book was provided for each participant to set action plans, log progress and facilitate consultation discussions. Consultations were delivered by exercise referral practitioners and underpinned by SDT (Ryan and Deci, 2000), with the aim of enhancing autonomous PA motivation. Practitioners received training in SDT-based communication strategies led by a sport and exercise psychologist (last author [P.M.W.]), involving a 3-hour group workshop, two one-to-one sessions per practitioner and two follow-up group meetings over a 3-month period. We also observed exercise referral practitioners conducting baseline consultations prior to the start of training (needs analysis) and during delivery of the pilot in its early stages (progress tracking and personalised feedback). Training materials used in the initial workshop are available from the corresponding author (P.M.W.). The training focussed on helping practitioners understand key communication strategies for fostering autonomous motivation in participants, having time to try these out, then reflecting on progress and identifying further areas to work on. Full details of the co-produced intervention are described elsewhere (Buckley et al., 2018).
Participants
All exercise referral participants referred to Centre A between January and March 2017 received the co-produced PA intervention. Participants were eligible to take part in the research study if (a) their referral was due to a health-related risk factor (e.g. hypertension, hyperglycaemia, obesity) or a controlled lifestyle-related condition (e.g. diabetes, cardiovascular disease, depression) and (b) they were ⩾ 18 years of age. A purposefully diverse subsample of participants were invited and took part in an interview (n = 12). Participants were selected based on their baseline data to represent a range of ages, male and female, a variety of health conditions (cardiovascular, diabetes, mental health, musculoskeletal), as well as a range of body mass indices (BMIs).
Procedure
Data were collected at baseline and following week 12 consultations in university laboratories. Prior to testing, participants fasted for ⩾6 hours, avoided the consumption of alcohol for ⩾ 12 hours and strenuous exercise for ⩾ 24 hours. Upon arrival at the laboratory, participants’ written consent was obtained and anthropometrics measured. Following questionnaire completion, participants took part in a submaximal fitness test. Finally, an accelerometer was given to participants to record their PA levels for 7 days.
Outcome measures
Moderate-to-vigorous PA
PA was assessed via the commercially available tri-axial ActiGraph GT3x accelerometer (ActiGraph, Pensacola, FL, USA), which has been validated in a comparable population (Kelly et al., 2013). Participants were instructed to wear the monitor on the right hip during waking hours for 7 days. A diary was provided to record non-wear time. The monitor was set to record raw triaxial acceleration at 30 Hz. Following collection, data were downloaded to a computer using manufacturer software (ActiLife software version 6.13.3). Raw triaxial acceleration values were converted into an omnidirectional measure of acceleration, referred to as Euclidian norm minus one (ENMO; Hees et al., 2013). Data were calculated per 5 second epochs via 1 minute windows with an inclusion criteria of > 80% (Matthews et al., 2012). Minimum wear time was 10 hours per day and 3 days per week including one weekend day to be included in analysis. Signal processing was done offline in R (http://cran.r-project.org/). The R package GGIR (Hees et al., 2013) facilitated data cleaning such as non-wear time (15-minute detection and 60-minute evaluation window) and extraction of user defined acceleration levels (moderate PA > 69.1 g and vigorous PA > 258.7 g; Hildebrand et al., 2014).
Cardiometabolic and anthropometric measures
Cardiorespiratory fitness (CRF) (maximal oxygen consumption [VO2max-2]) was estimated via the Astrand-Rhyming cycle ergometer protocol (Astrand, 1960). The protocol is a single-stage cycle ergometer test designed to elicit a steady-state heart rate over a period of 6 minutes. The initial workload was 60 (female) or 90 (male) watts, cadence remained constant (60–70 r/min), and heart rate was recorded at 1-minute intervals (Polar Oy, Kempele, Finland). Oxygen uptake was estimated using the Astrand–Rhyming nomogram.
Blood pressure was measured in the supine position following 20 minutes of rest using an automated blood pressure device (Omron Healthcare UK Limited, Milton Keynes, UK). Using standard techniques (Lohman et al., 2004 [1991]) stature was measured to the nearest 0.1 cm using a Leicester Height Measure and body mass was calculated to the nearest 0.1 kg calibrated scale (both Seca Ltd, Birmingham, UK). Waist circumference was measured to the nearest 0.1 cm using an inextensible tape measure between the iliac crest and the lowest rib. BMI was calculated as mass divided by stature (kg/m2). Waist-to-height ratio was calculated as waist circumference divided by stature.
A clustered cardiometabolic risk score was calculated to minimise the impact of daily variation in individual risk markers (Alberti et al., 2009; Wijndaele et al., 2006). Standardised values for waist-to-height ratio, mean arterial blood pressure ([2(diastolic) + systolic]/3), and CRF (inverted) were calculated using baseline mean ± standard deviation. The sum of these standardised values was divided by the number of parameters included to give a clustered score. This approach has been used in a comparable adult sample (Knaeps et al., 2018).
Psychological questionnaires
Behavioural regulation was measured via the Behavioural Regulation in Exercise Questionnaire (Markland and Tobin, 2004). Four additional items were included to assess integrated regulation (BREQ-2R; Wilson et al., 2006a). The BREQ-2R plus integrated scale contains a total of 23 items, each answered on a Likert-type scale of 0 (not true for me) to 4 (very true to me). Cronbach’s alpha values for BREQ-2 subscales have been shown to exceed .75 (Wilson and Rodgers, 2004) and the addition of the integrated regulation items (BREQ-2R) can be used without compromising validity (Wilson et al., 2006a). Psychological needs satisfaction was measured via the Psychological Needs Satisfaction in Exercise Scale (PNSE; Wilson et al., 2006b). The PNSE includes 18 items, each answered on a 6-point Likert-type scale (1 = false, 6 = true) that measures participants’ perceived autonomy, competence and relatedness in an exercise context; from which Cronbach’s alpha values have been shown to exceed 0.7, 0.8 and 0.8, respectively (Mills et al., 2012).
Consultation attendance
Attendance at one-to-one consultations was logged by exercise referral practitioners.
Interviews
Semi-structured interviews (n = 12; 8 female) lasted 30–60 minutes and were conducted at Centre A following week 12. As participant perceptions of PA referral schemes have been reported (Mills et al., 2012; Sharma et al., 2012), the aim of the interviews was to explore participant perceptions of the components of the intervention that differed from usual care: (a) the PA content of the intervention and (b) the individual progress support offered (via one-to-one consultations). Interviews also covered SDT concepts such as motivation, needs satisfaction and perceived needs support. To enhance the depth and trustworthiness of the data, iterative questioning was used whereby the researcher used probes to elicit detailed data and returned to previously raised points by paraphrasing participant answers or rephrasing the questions (Shenton, 2004). All interviews were conducted by a single researcher (D.H.) who received training and mentoring from (P.M.W.), an experienced qualitative researcher.
Statistical analyses
Data were analysed using SPSS version 23 (IBM, New York, USA) with alpha level set at p ⩽ .05. Intervention effects were compared 12 weeks from baseline using paired samples T-tests and effect sizes (Cohen, 1988). Inferential statistics were computed using a minimum clinically important difference method (Batterham and Hopkins, 2006; Hopkins et al., 2009). Briefly, the approach forms inferences based on clinically meaningful magnitudes, and is supported alongside hypothesis testing. A spreadsheet (http://newstats.org/generalise.html) was used to compute quantitative and qualitative probabilities that the true effects were beneficial, trivial, or harmful. A minimum clinically important difference for (CRF) was set at 2 mL kg-1 min-1 based on previous epidemiological evidence (Lee et al., 2010; Simmons et al., 2009) and for moderate-to-vigorous PA (MVPA) was set at 10 minutes/day as identified by recent public health statistics (ONS, 2017) and magnitudes found in similar interventions (Gabrys et al., 2013). Minimum important differences for other variables were determined via previous epidemiological research and a small effect size.
Semi-structured interviews were audio-recorded and transcribed verbatim. Data were then analysed thematically following guidance from Braun and Clarke (2006). NVivo-10 software (QSR International Pty Ltd.) was used to aid data management and coding. Preliminary analysis was conducted by the researcher who conducted the interviews (and was thus immersed in the data), with regular meetings with B.J.R.B. and P.M.W. Transcripts were coded into emerging categories, themes and sub-themes, which were iteratively adapted as analysis progressed (as used by Din et al., 2015). Eight transcripts were read independently by three researchers (B.J.R.B. and P.M.W., and D.H.) before meeting to reflect on themes and discuss, resolve, and amend any areas of disagreement. A final revision of themes and adaptation for the purposes of the mixed-methods study was conducted by B.J.R.B., and reviewed by D.H. and P.M.W. This process has been recommended to improve rigour and reduce researcher bias in the qualitative results (Cohen and Crabtree, 2008).
Results
Participant characteristics
Thirty-six participants were invited to take part in the study and 32 consented, 19 of whom provided data for at least one 12-week measure (Figure 1). Incomplete datasets were due to inability to complete the CRF test (n = 3), declining the blood pressure measure (n = 1) and insufficient accelerometer wear time (n = 5). Table 1 outlines baseline characteristics for the whole sample, complete cases and interview participants.
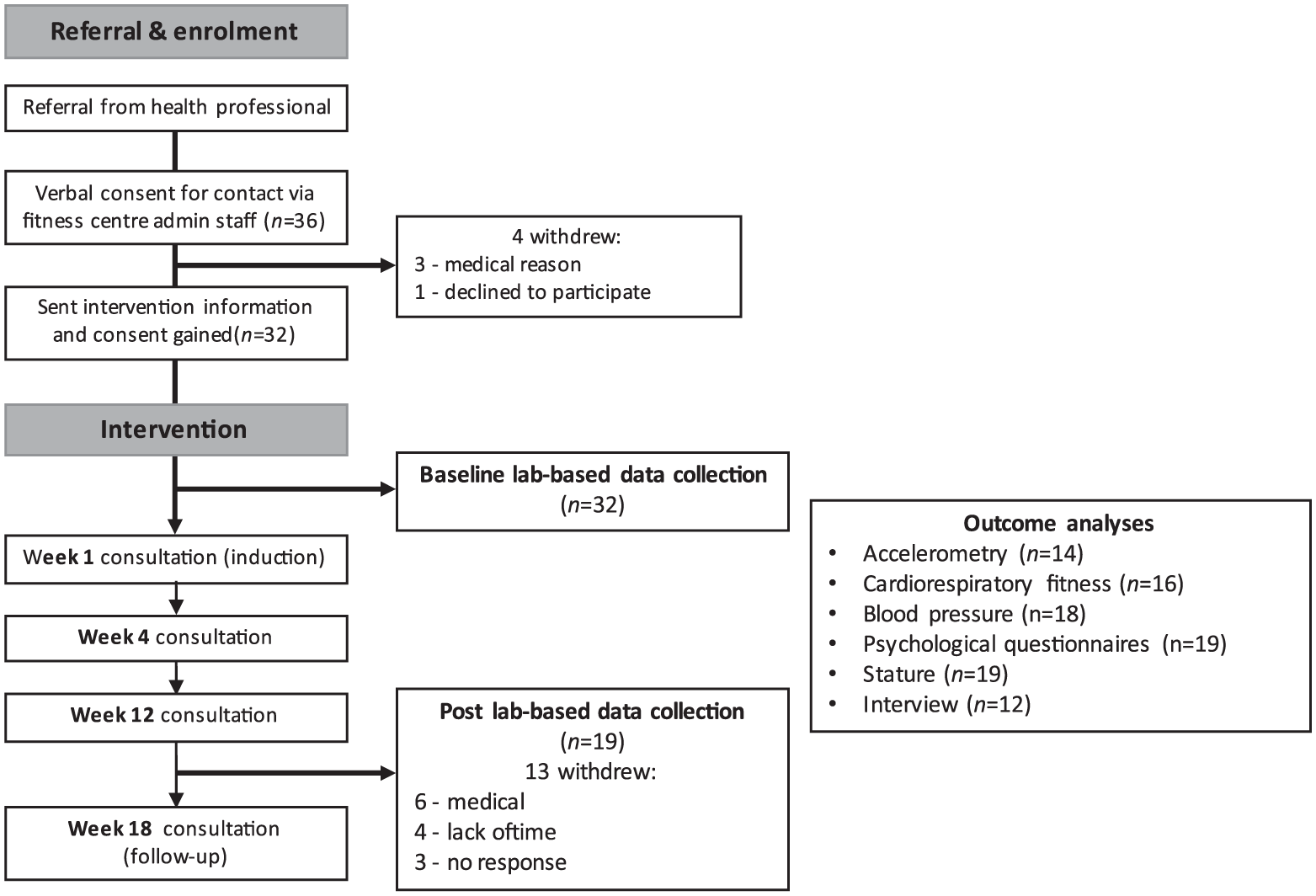
Flow diagram of intervention pathway.
Baseline characteristics presented as mean ± SD or % (n) of group.
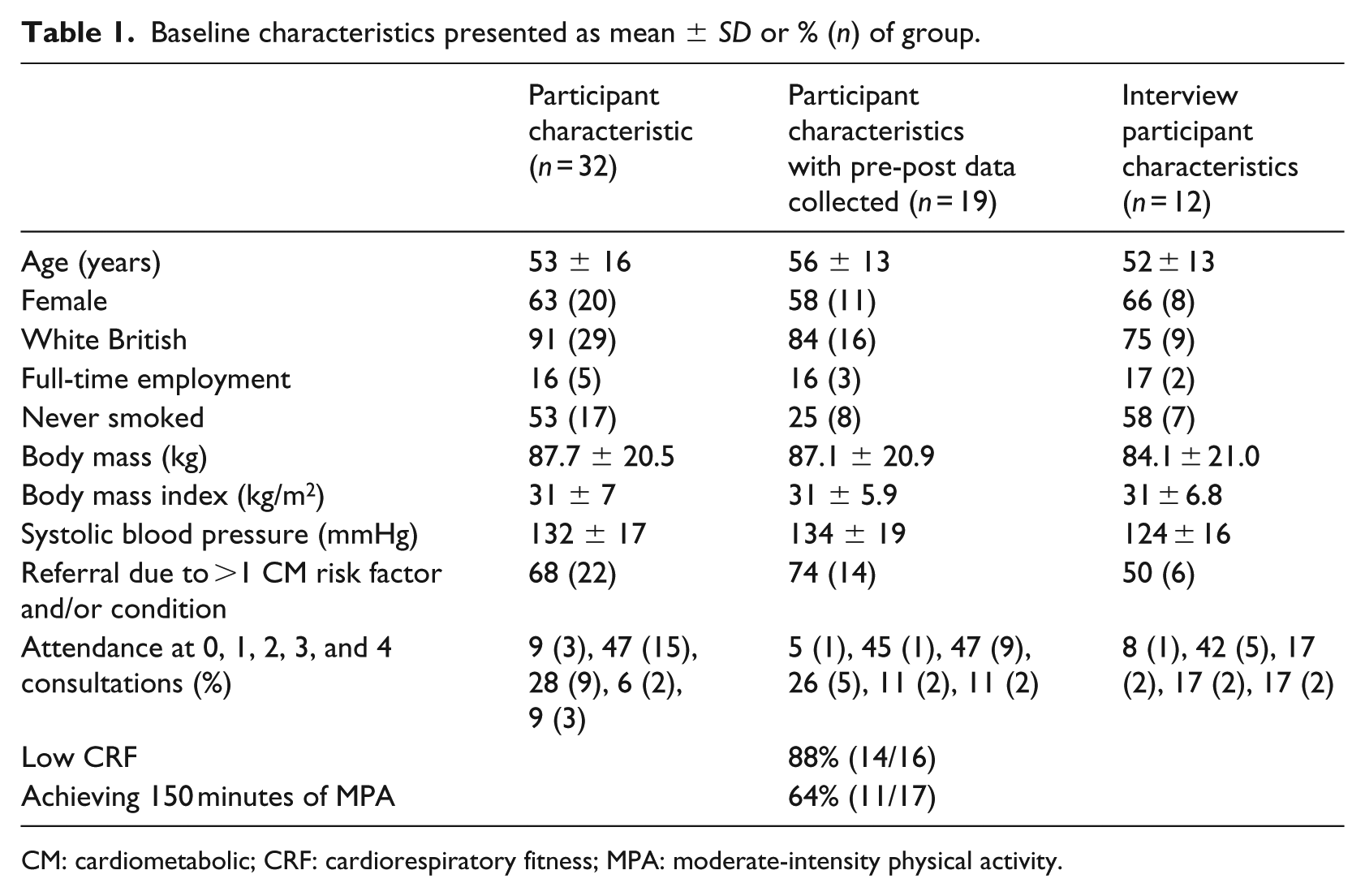
CM: cardiometabolic; CRF: cardiorespiratory fitness; MPA: moderate-intensity physical activity.
Intervention effects
Cardiometabolic, PA, and psychological questionnaire results are displayed in Table 2. Statistically significant mean changes in CRF (3.6 mL kg-1 min-1 [17% increase], benefit very likely), daily MVPA (12.6 minutes [46% increase]; benefit possible), systolic blood pressure (−9.8 mmHg [7% decrease]; benefit very likely) and waist-to-height ratio (-1 [2% decrease]; benefit unclear) were observed at week 12 compared to baseline. Correspondingly, a clustered cardiometabolic risk score demonstrated a significant reduction (benefit most likely) at week 12. No within-subject changes were observed from baseline to 12 weeks in any psychosocial variables.
Changes in cardiometabolic, physical activity (PA) and psychological outcome variables. For the cardiometabolic and PA variables, quantitative and qualitative magnitude-based inferences are reported. Due to the lack of agreement in what are meaningful/harmful changes in levels of motivation, magnitude based inferences were not calculated for psychosocial variables.
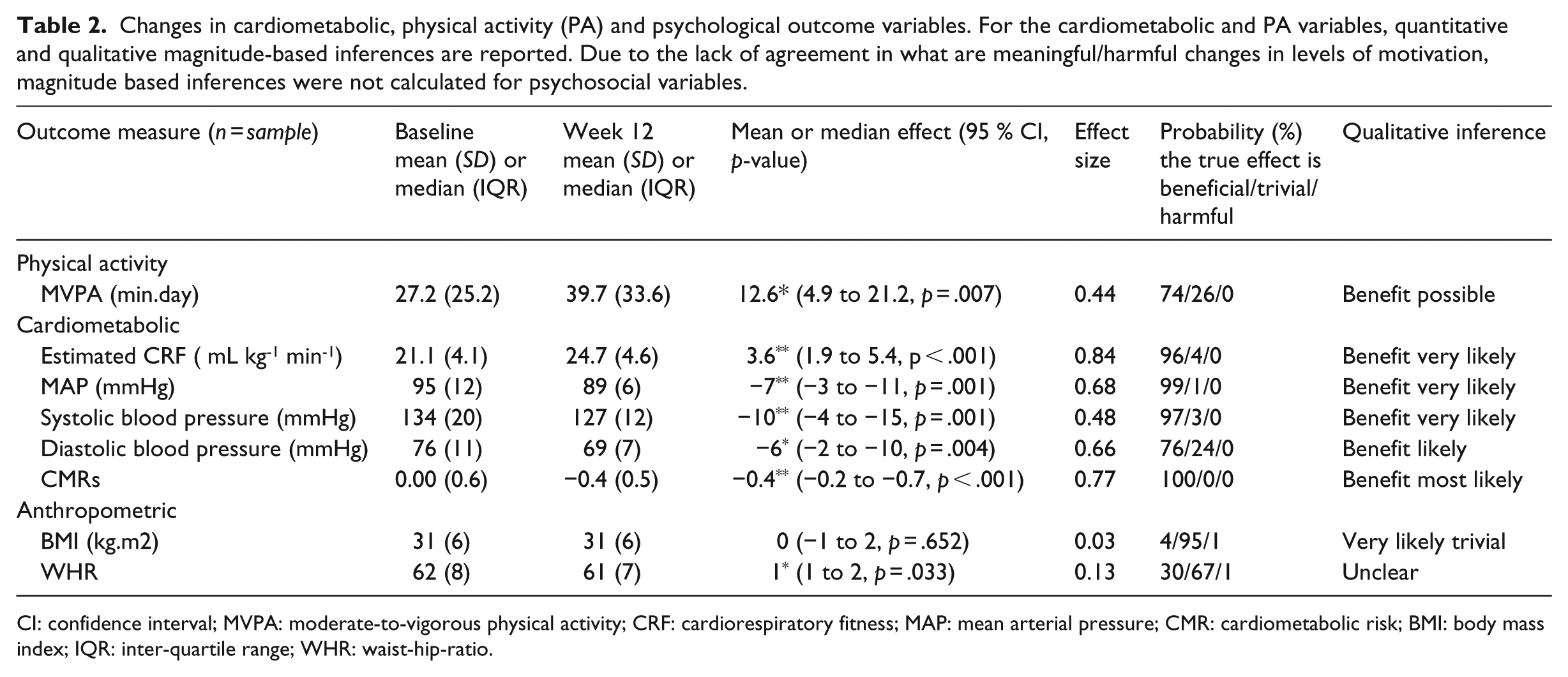
CI: confidence interval; MVPA: moderate-to-vigorous physical activity; CRF: cardiorespiratory fitness; MAP: mean arterial pressure; CMR: cardiometabolic risk; BMI: body mass index; IQR: inter-quartile range; WHR: waist-hip-ratio.
Process data
Three participants (9%) did not attend any consultations, 15 (47%) attended induction only, 9 (28%) attended induction plus one consultation, 2 (6%) attended induction plus two consultations, and 3 (9%) attended induction plus three consultations.
Interviews
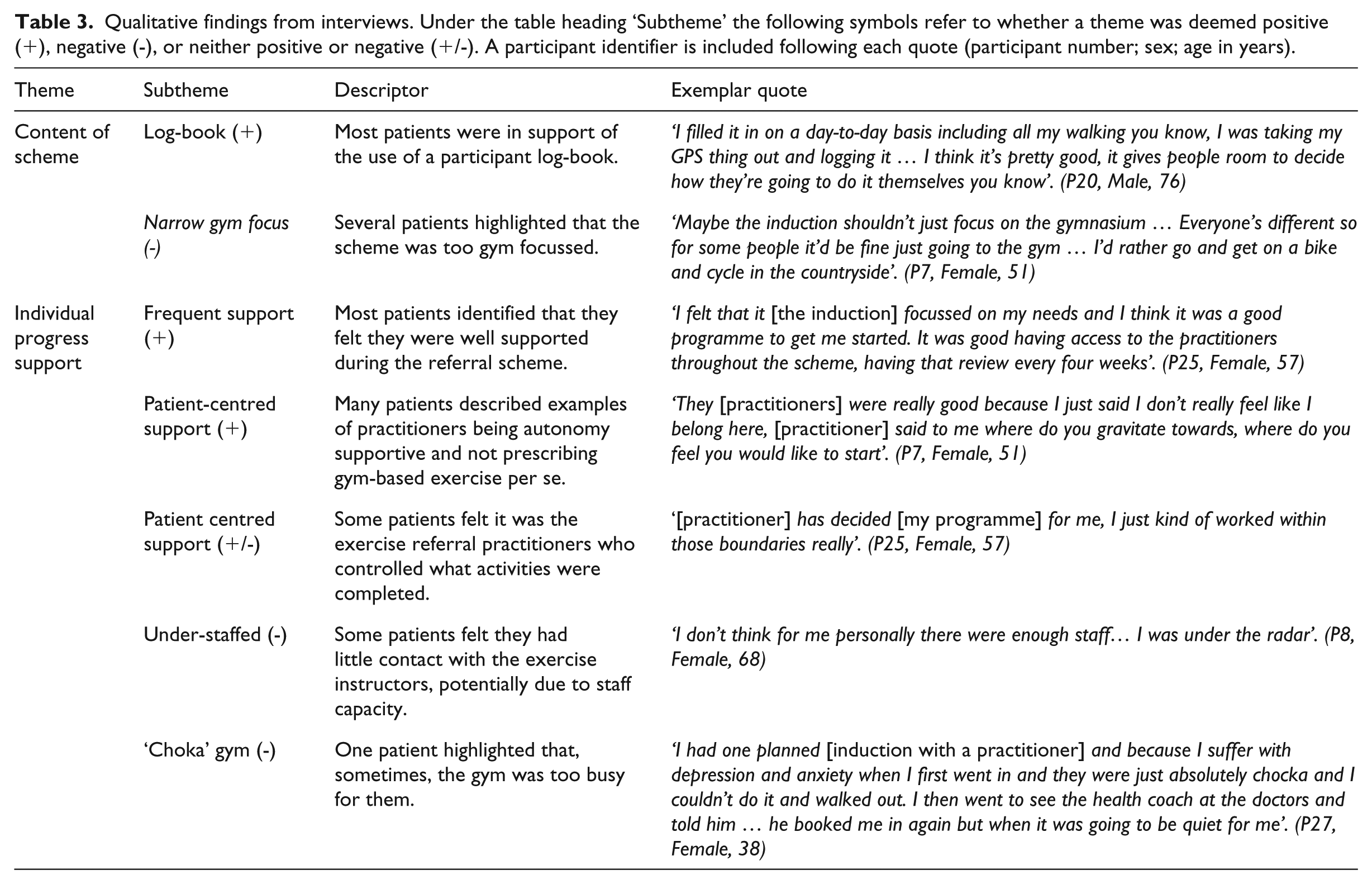
Table 3 presents participant perceptions regarding (a) PA content of the intervention and (b) individual progress support.
Qualitative findings from interviews. Under the table heading ‘Subtheme’ the following symbols refer to whether a theme was deemed positive (+), negative (-), or neither positive or negative (+/-). A participant identifier is included following each quote (participant number; sex; age in years).
Overall perceptions of the intervention were positive. Most participants described meaningful health improvements (e.g. ‘I’ve been off my anti-depressants … I was on them for about eleven years and I tried several times to come off them’ [P25, Jenny, 57]). While some participants felt the scheme was too gym-focussed, other participant reports suggested individuals were engaging in physical activities outside of the centre (‘obviously when the weather’s nice I’d rather go out walking than go on a machine’ [P7. Kathy, 51]), while noting the benefits a fitness centre provides when the weather is poor (‘I think one of the benefits is actually doing something active when it was not so nice outside’ [P7. Kathy, 51]).
It was not clear from the interviews how much autonomy participants felt in their PA behaviour change. While some participants noted their exercise programmes were set by the practitioners, this was not specifically identified as positive or negative. Participants did, however, describe how the frequent support was tailored to their needs and kept them coming back (‘[practitioner] said I could see him every four weeks to see how I’m doing … which I think is very good’ [P19, Mark, 57]).
Several participants felt the fitness centre was busy and under-staffed. Participant reasons for not receiving all of the behaviour change consultations included personal choice (‘wanting to be by myself’ [P7, Kathy, 51]), consultations being cancelled, and not rescheduled (‘unfortunately I had a phone call that said it was cancelled so I came in and did my usual … they tried to make an appointment again but I couldn’t do it when [instructor] wanted … so he said well you know we’ll make it at some other time, well that never happened’ [P8, Deborah, 68]) and one participant noted that ‘[Practitioners] just let you get on with it and I suppose if you went to them and asked them to help they’d give it to you’ (P31, Rita, 61).
Discussion
Main findings
This study explored the preliminary effects and acceptability of a co-produced PA referral intervention. Findings demonstrated significant improvements in MVPA and clustered cardiometabolic risk (CRF, waist-to-height ratio, blood pressure) from baseline to 12 weeks. There were no changes in psychological needs satisfaction or motivation towards exercise, although as only 9% of participants were recorded to have attended all four consultations it is possible participants did not receive the intended level of behavioural support. While participants were positive about the support provided by exercise referral practitioners, some felt the intervention was too gym-focused and the fitness centre was under-staffed and too busy.
What is already known
PA is recommended for maintenance of good health and as a treatment for individuals with health conditions. Despite UK PA referral schemes showing promise, systematic reviews have found they are not typically underpinned by theory and have reported a wide range of attendance rates (Campbell et al., 2015; Pavey et al., 2011a, 2011b). We previously co-produced a PA referral intervention that was underpinned by behaviour change theory and deemed feasible to implement in practice (Buckley et al., 2018). It was not known, however, whether the intervention was acceptable or effective and what value co-production had for intervention success.
What this study adds
This is the first study to explore the preliminary effects and acceptability of a co-produced PA referral intervention. Significant improvements in participants’ MVPA and cardiometabolic health profile were found following the co-produced PA intervention. The magnitude of change observed in CRF (>3.5 mL kg-1 min-1) has been demonstrated to reduce all-cause mortality risk by 13% (Lee et al., 2010). This may be particularly meaningful for our sample (whereby 14/16 participants (88%) demonstrated CRF levels < 27.7 mL kg-1 min-1), given the most striking differences in mortality rates occur between the least-fit and next-least-fit quintiles. Thus, the greatest public health benefits may be realised by increasing PA levels among the least fit (Lee et al., 2010). These findings are supported by physiological data from our cohort that demonstrated significantly improved vascular health from baseline to 12 weeks (published elsewhere–see Buckley et al., 2019). Despite the low fitness levels of our sample, however, it is notable that 64% of participants were achieving the recommended 150 minutes of moderate-intensity PA per week at baseline (device-based PA data). Such discordance demonstrates the importance of measuring both PA and CRF, while raising questions regarding the use of current PA guidelines (DoH, 2011) to assess eligibility for PA referral schemes (NICE, 2014).
The co-produced intervention aimed to support PA behaviour change within participants’ daily lives, rather than focussing on exercise prescription. While an increase in MVPA was noted, it is not clear what type of PA participants participated in, and qualitative accounts suggested some participants felt they were guided towards gym-based exercise rather than PA (‘the induction shouldn’t just focus on the gym’ P7, Kathy, 51). This perceived gym focus may have resulted from the intervention being delivered within a fitness centre, which was a co-produced decision driven by the need for accountability when working with individuals with health conditions (Buckley et al., 2018). A number of participants did, however, mention that they had made positive PA-related changes outside of the gym, which demonstrates there is potential for fitness-centre-based interventions to support more lifestyle-related PA changes. It may be that practitioners were not yet delivering the intervention with the intended PA focus. In addition, if participants were not attending the consultations, the gym/fitness centre environment was the only perceived intervention component. Taken collectively, it is worth investing in further work with the practitioners to see if it is possible to embed the intended holistic PA focus of the intervention and level of needs support provided by practitioners
This co-produced intervention was underpinned by SDT (Ryan and Deci, 2000) and intended to foster autonomous PA motivation through supporting the psychological needs of autonomy, competence and relatedness. We did not, however, find any change in psychological needs satisfaction or exercise motivation regulation at 12 weeks. Participants’ qualitative accounts suggested they may not have been exposed to the intended level of autonomy support, with some participants suggesting practitioners controlled their activity programmes. Participants also perceived the gym to be busy and understaffed, which may have impacted on practitioner ability to conduct consultations and/or participants’ perceptions of whether consultations occurred.
There are several possible explanations as to why changes in PA and fitness may have occurred in the absence of changes in psychosocial variables. Primarily, as it was not clear to what extent consultations were carried out as intended in the current study, it is possible the scheme that was actually delivered did not go much beyond the level of support typical of a standard exercise referral scheme (e.g. a 12-week gym programme). While our data do not allow conclusions to be drawn about the level of needs support provided by practitioners, challenges of implementing needs-supportive delivery within PA referral settings have been recognised elsewhere (Duda et al., 2014). Therefore, the short-term PA and cardiorespiratory fitness changes may have resulted from the more ‘typical’ exercise referral factors such as subsidised gym access and attention from an instructor. To our knowledge, however, no comparable evaluations of standard exercise referral have measured objective PA, and only one study measured CRF. Isaacs et al. (2007) found an increase of 11% in CRF at 10 weeks following an exercise referral scheme, which is less than the 17% increase in the present study. Comparison of the results from our co-produced intervention compared with typical exercise referral schemes is therefore limited. One study did, however, measure objective PA levels to evaluate an exercise referral scheme with embedded PA counselling and found a significant increase in MVPA (9 minutes), which is slightly less than the 12.6 minute increase observed in the present study (Gabrys et al., 2013). In addition, Sørensen et al. (2008) measured CRF to evaluate a 4-month exercise referral scheme with motivational counselling and found an increase of 2.3 mL kg-1 min-1, which is less than the 3.6 mL kg-1 min-1 observed in the present study. More evaluation work is therefore needed that includes objective health measures (i.e. device-based PA and CRF) to better compare standard exercise referral schemes with adapted initiatives.
Other potential explanations for the lack of change in motivational variables relate to the sample’s baseline profile and properties of the questionnaires used. It is noteworthy that participants did not have an ‘unhealthy’ motivational profile to start with. In particular, the mean perceived autonomy satisfaction at baseline was 4.76 + 0.88, indicating a positive level of perceived autonomy that we might not expect to change substantially (given the range is 1 to 6, and a score of 3.5 would be neutral). Finally, it must be acknowledged that the BREQ-2R and the PNSE both focus on exercise rather than PA. Therefore, it is possible that changes in PA related to non-exercise domains of PA (e.g. walking, lifestyle activity) might not be reflected in changes in exercise motivation or related constructs. Due to the complex nature of PA, however, it is challenging to measure specific motivation for the whole spectrum of PA (which may vary according to PA domain), nor are there current validated measures available.
The PA intervention in this study was previously co-produced by a team of health service commissioners, practitioners, service users and academics (Buckley et al., 2018). It is noteworthy that not all exercise referral practitioners delivering the intervention were involved in the co-production phase, which may have affected their sense of ownership of the scheme. The research team did, however, meet regularly with the delivery team and developed a reciprocal relationship that facilitated a sense of shared ownership of the project and ensured teething problems were addressed promptly. Such observations highlight the benefits of co-production continuing beyond initial development throughout subsequent delivery and implementation (Craig et al., 2008).
Strengths & Limitations
Despite this study’s strengths (high ecological validity, phased methodological approach and the use of objective CRF and device-based PA outcome measures), several limitations must be acknowledged. The intention of this study was not to determine definitive effectiveness, but to explore acceptability and estimate potential effects through magnitude-based inferences. As such, the sample size was small and there was no control group. The magnitude-based inference approach helps to prevent an over reliance on the P statistic, and instead facilitates the use of available evidence to infer meaningfulness. Furthermore, this study did not include a measure of practitioner delivery during consultations, which makes it difficult to draw conclusions regarding intervention fidelity. Systematic review data have reported wide-ranging uptake and adherence rates for exercise referral schemes (28%–100% and 12%–93%, respectively; Pavey et al., 2011a). We did not directly measure attendance at the fitness centre in the present study, thus we do not know how much or little participants used the facilities, regardless of consultation attendance. Nonetheless, consultation documents completed by exercise referral practitioners suggested incremental dropout (with 3/32 participants having attended all four consultations). Yet, 19 participants attended 12-week data collection at the university and anecdotal conversations with practitioners suggested attendance was higher than our results implied. Therefore, it is not clear if missed consultations were due to failure on the part of the exercise referral practitioner to offer the consultation, failure on the part of the participant to attend, or poor attendance monitoring (i.e. the consultation did actually occur). Future research should therefore include objective fidelity and attendance measures.
Conclusion
This is the first study to explore preliminary effects and acceptability of a co-produced PA referral intervention. Following the 12-week intervention, improvements in objectively measured MVPA and cardiometabolic health were observed. Process data suggested the focus on PA (rather than exercise) was not always achieved. Thus, further work may be required to embed the intended holistic PA focus of the intervention and the level of needs support provided by practitioners, develop objective means of monitoring attendance and adherence, and improve the delivery and content of the behaviour change consultations, prior to conducting an experimental trial. Importantly, this study provides novel insight into what happens beyond the co-production phase of a complex intervention. Findings highlight the challenges of implementing a complex PA referral intervention as intended and emphasise the importance of following MRC guidance (Craig et al., 2008), which advocates a phased approach to complex intervention development. While it is not possible to know how the delivery of this intervention would have differed had it not been co-produced, the authors wish to emphasise the importance of an ongoing reciprocal relationship between commissioners, practitioners, service-users and academics to ensure congruence between the way interventions are planned, delivered and received.
Footnotes
Ethical approval and informed consent
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and national research committee and the Declaration of Helsinki. Informed consent was obtained from all individual participants included in the study. UK NHS Research Ethics Committee approval was received for this study (REC reference: 16/WA/0231–Project number: 209923).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded as part of a fully funded doctoral studentship (B.J.R.B.) by Liverpool John Moores University.