
Abstract
Objective:
This evaluation examined the effectiveness and cultural compatibility of a community health worker (CHW) training programme on water, sanitation and hygiene (WASH) in Haiti.
Design:
Mixed-methods including pre- and post-course tests of WASH knowledge, focus group discussions and semi-structured observation.
Setting:
Haiti is among the world’s most underdeveloped nations for WASH infrastructure. In rural areas of the country, fewer than half of households have access to clean water and 22% have adequate sanitation facilities. The study evaluated a ‘train-the-trainer’ programme in rural southeast Haiti.
Methods:
Participants were 22 CHW supervisors responsible for training and monitoring the work of rural junior health agents (JHAs). The training programme was delivered by international trainers and consisted of 1 week of classroom training and 1 week of community-based experiential learning. Paired-samples t-tests were used to assess changes in knowledge, and robust qualitative methods were used to analyse focus group discussion and observation data.
Results:
Participants showed statistically significant improvement in WASH knowledge from pre- to post-test. In experiential supervisor-led training sessions, participants effectively conveyed course content to JHAs, and successful home visits demonstrated the potential for content to reach community members. The programme would benefit from providing educational materials to enhance dissemination. Participants expressed dissatisfaction with translations of course content and requested more frequent training, more emphasis on leadership development and specific content areas for future training.
Conclusion:
The CHW training programme enhanced trainees’ WASH knowledge and capacity to educate JHAs to disseminate the knowledge to local residents. The train-the-trainer model offers a cost-effective strategy for building local capacity for health education.
Introduction
The UN Sustainable Development Goals established access to safe water, sanitation and waste management as essential to the health and well-being of all people (United Nations, 2016). Water, sanitation and hygiene (WASH) are critical to reducing waterborne disease and associated deaths (Zwane and Kremer, 2007). Haiti is among the world’s least developed nations in terms of WASH infrastructure. In 2015, only 40% of rural Haitians had access to a safe drinking water source and 22% had access to sanitation facilities (World Health Organization [WHO]).
A number of factors contribute to the lack of WASH access for Haitians. For complex historical and sociopolitical reasons, few resources have been dedicated to central water and sanitation systems in Haiti, especially in rural areas (Cohen and Figaro, 2014; Khan et al., 2017). A long-standing history of political instability has hindered government investment in infrastructure, leading to disorganised or unsustainable improvement efforts. The situation magnified by recurring natural disasters such as the massive earthquake that struck Haiti in 2010 and Hurricane Matthew in 2016. The 2010 earthquake destroyed much of Haiti’s already-fragile infrastructure (Handzel et al., 2013). Many Haitians were forced to seek temporary shelter, placing an enormous burden on WASH facilities and increasing exposure to waterborne diseases.
The lack of WASH facilities in Haiti regularly contributes to the consumption of unsafe drinking water and open defaecation. These practices contribute directly to diarrhoea and waterborne diseases such as typhoid and cholera (Khan et al., 2017). Cholera has been particularly impactful since the 2010 earthquake. By 2016, approximately 800,000 known cases of cholera were reported in Haiti with an estimated death toll of 9,300 (USAID, 2016). In response, the Haitian Ministry of Public Health and Population (MSPP) and the National Directorate for Water Supply and Sanitation (DINEPA) identified WASH as one of four priority areas in the National Plan of Action for the Elimination of Cholera in Haiti: 2013–2022 (Gelting et al., 2013). The plan places special emphasis on establishing networks of community health workers (CHWs) in communes at risk for cholera (MSPP and DINEPA, 2013). Despite the policy emphasis, WASH remains a pressing concern in Haiti; the nation has the highest rates of infant, under-5 and maternal mortality in the Western hemisphere and diarrhoea is one of the leading causes of death.
Diarrhoeal illness disproportionately impacts rural Haitian communities, as 62% of reported cases of diarrhoea were found in these areas, despite making up only 43% of the population (WHO, 2015). This is particularly problematic in the centre, south and southeast regions of Haiti, where 85% of the area’s population resides in rural areas (Verner, 2008). Therefore, WASH educational interventions focusing on rural populations are critical in improving the overall health and well-being of people living in Haiti.
The current study presents the results of a mixed-methods evaluation of a WASH training programme implemented in the rural Sud-Est (Southeast) department of Haiti, a region with substantial health needs and minimal water and sanitation infrastructure (Verner, 2008). WASH education programmes in low-resource settings can encourage healthy behaviours related to water and sanitation, such as hand washing, utilising safe water storage and water treatment methods, and avoiding open defaecation, to aid in the reduction of diarrhoeal illness and related deaths (Fung et al., 2013; Kariuki et al., 2012).
Overview of the CHW training programme
In the aftermath of the 2010 earthquake, a US-based nongovernmental organisation (NGO) called Heart to Heart International and the MSPP established a yearly CHW training course in rural southeast Haiti to train a cohort of CHWs to (1) expand health literacy and (2) encourage healthy WASH practices in the community. Becton Dickinson (BD), a US-based medical technology company joined these efforts in 2012 to expand the CHW training with financial, logistical and human resource support. Since its inception, the training programme has been conducted annually, mostly by foreign instructors who travel to Haiti to teach unpaid Haitian CHWs. The CHWs are then tasked with disseminating the content to the community through home visits and community presentations (Knettel et al., 2017).
In 2013, the CHW training programme was formalised with the establishment of Kore Fanmi (Creole for Family Support), which used new UNICEF funding to advance healthcare, health education and WASH services in the region, including vaccines, outreach to vulnerable families and latrine projects. The Kore Fanmi staff is entirely Haitian and includes 4 administrators, 9 CHW supervisors and 96 junior health agents (JHAs) recruited through a competitive application process, all of whom receive regular salaries. Supervisors and their assigned JHAs provide educational coverage for an assigned geographical area. UNICEF also assisted in establishing a tablet-based system for tracking services, as well as support for transportation and new training opportunities.
In order to reach high-need families, Kore Fanmi CHWs and JHAs act as links between the community and the formal health system. The programme’s pyramid structure also has a substantial ‘cascade’ effect (Brady and Keogh, 2016), as the 96 JHAs directly interface with approximately 15,000 vulnerable families in three communes of southeast Haiti (see Figure 1).
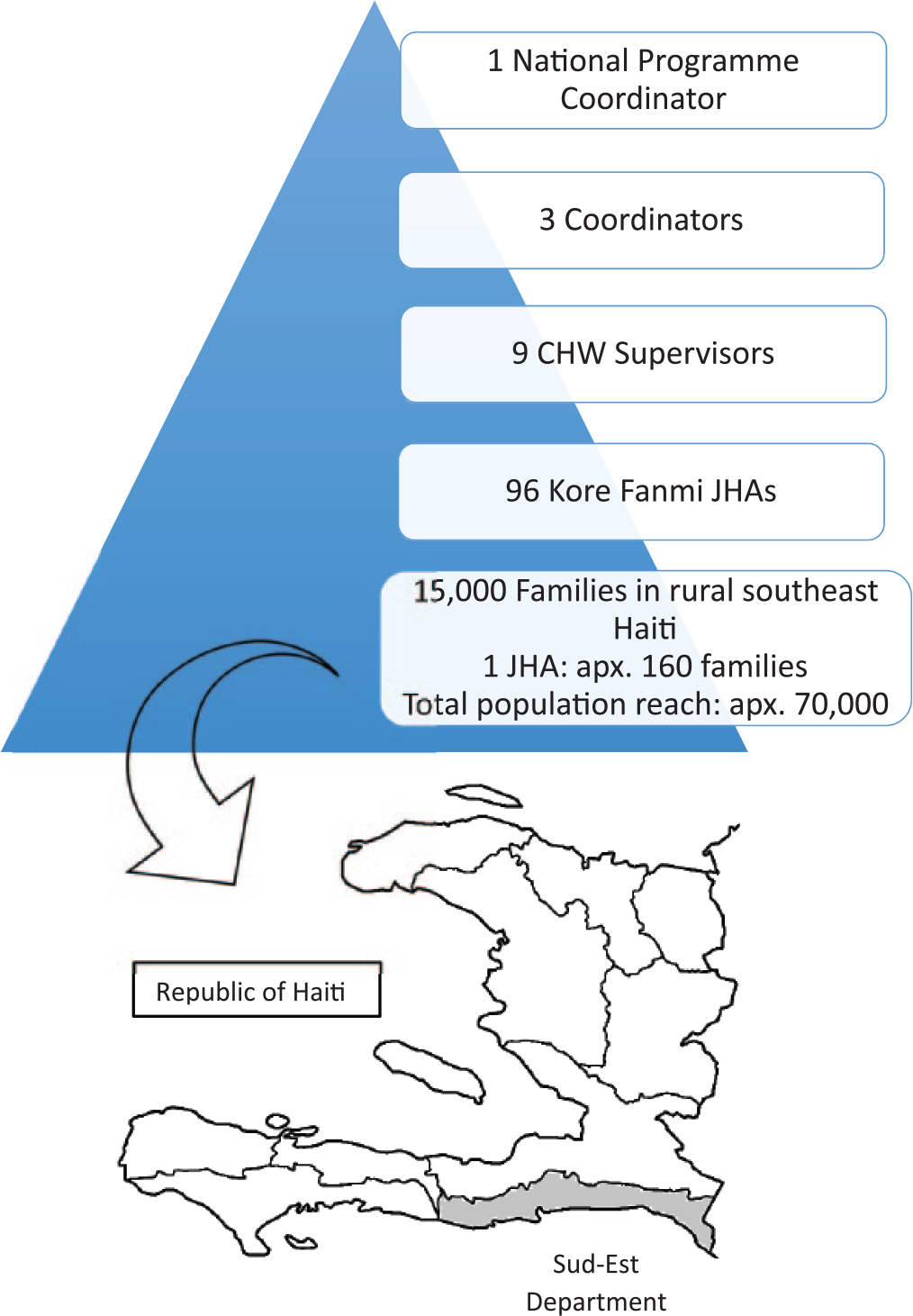
Kore Fanmi organisational structure and reach.
The 2016 programme
Each year, the sponsoring NGO and corporate partner work with Kore Fanmi to offer a two week CHW training course. For the May 2016 training course, Kore Fanmi leaders requested training in WASH topics based on a curriculum established by the Haitian MSPP. The 2-week training programme, titled Healthy People, Healthy Community, consisted of three distinct parts: (1) a classroom-based didactic component where supervisors learned the WASH curriculum, (2) a practical component in which CHW supervisors taught WASH topics to JHAs and (3) a field coaching component where JHAs disseminated course-specific health information during home visits in the nearby community.
The first week of the training programme was the didactic training portion in which instructors from the sponsoring NGO and corporate partner taught WASH content to 22 Kore Fanmi supervisors and invited volunteer CHWs from local organisations. The four instructors were health professionals from the USA and South Africa, plus one Haitian nurse. 1 Each instructor was responsible for adapting the MSPP curriculum for an assigned topic, writing this into a course textbook provided to each participant and teaching the content for one full day. The course was primarily presented in English but immediately translated to Creole by a trained interpreter. The training incorporated topics such as tools and techniques for improving WASH, personal hygiene and environmental sanitation, WASH for the mother and child, and prevention of common WASH-related diseases as well as more general concepts such as leadership and communication skills. In addition to lectures, instructors employed interactive activities, discussions and small group activities.
Week 2 of the training consisted of the practical and field coaching components. The role of the supervisors shifted from trainees in week 1 to trainers in week 2. The nine Kore Fanmi supervisors selected a topic from the week 1 curriculum and presented a training session to 5–8 JHAs. The training sessions were conducted in the NGO offices or local community centres and each session was observed by one or more instructors from week 1, who provided feedback on preparedness, supervisor-JHA rapport, instructional tools used, effectiveness of the instruction and accuracy of content.
After the lecture, instructors and supervisors accompanied JHAs into the community as they practised disseminating the information to families. Each group of JHAs conducted, on average, five home visits near the training location. Debriefing sessions were then held to provide feedback on JHA–community rapport, effectiveness of delivery and accuracy of content. The supervisor lectures and field coaching components were newly implemented for the 2016 programme.
Train-the-trainer model for health education
As the project has grown, it has adopted a tiered, ‘train-the-trainer’ (TTT) model, which aims to be (1) efficient, as a small number of trainees can pass knowledge on to a number of others; (b) sustainable, since the trainees receiving the most intensive training are expected to take on greater organisational leadership as their expertise grows; and (3) culturally relevant, as the trainers are members of the local community and may serve as ‘cultural filters’ of content (Knettel et al., 2017), ensuring that it is applicable to the local context.
Because of these strengths, the TTT model has received substantial support in under-resourced and hard-to-reach populations (Besculides et al., 2011; Brady and Keogh, 2016; Orfaly et al., 2005). In Haiti, a past TTT programme effectively improved knowledge of techniques for hand washing and water sanitisation in an effort to prevent cholera transmission (Rajasingham et al., 2011). Rajasingham et al. (2011) concluded that TTT programmes could assist organisations to quickly and efficiently reach the most underserved areas of Haiti and reduce the spread of the cholera epidemic.
Aims of the evaluation
The current study presents the results of a mixed-methods evaluation of the 2-week CHW TTT programme conducted in 2016. We assessed (1) the effectiveness of the training at improving Kore Fanmi supervisors’ knowledge in WASH content, (2) supervisors’ ability to teach that content to JHAs and (3) the potential for JHAs to transmit WASH knowledge to the community during home visits, where knowledge is consistent with the didactic training and in line with local cultural norms (Vizeshfar et al., 2018).
Methods
The training programme was offered to 22 participants, all of whom were Haitians living in the Sud-Est (Southeast) department of the country. This evaluation was completed by four US-based international scholars, two from the USA, one from India and one from China, with considerable input from Kore Fanmi staff in design, implementation, data analysis and interpretation.
The study received ethical approval from the institutional review board at Lehigh University. Signed informed consent was obtained from all participants prior to taking part in the training. Participants were notified that a decision not to participate in the evaluation had no bearing on their standing in the training course. Participants were not compensated for their participation in the training course or for the evaluation.
Measures
Pre- and post-course tests of WASH knowledge
At the start of the didactic training (week 1), participants were asked to complete a knowledge test consisting of 30 multiple-choice and true-false questions to measure their baseline knowledge of WASH topics. Test questions were written by course instructors to reflect key concepts of their instruction, including proper hand washing, water sanitation, defaecation and waste disposal practices, managing diarrhoeal illness, and leadership and communication skills. Each question accounted for 1 point, for a total range of 0–30 points. At the end of the didactic training, participants repeated the same test to assess their change in knowledge. No test-specific feedback was provided after the pre-course test or at any time during the training course. Example items included, ‘What should a mother feed her baby for the first 6 months of life?’ and ‘If you visit a family and discover their 3 year old son has had progressing diarrhoea for three weeks, what is the best solution?’ (complete Knowledge Test can be found in the Supplementary Material).
Pre- and post-training focus group discussions
Prior to the course, participants were split into two groups. Two members of the evaluation team used a semi-structured guide to facilitate 40–60 minute focus group discussions about prior experiences with WASH training and practices, existing WASH practices within communities and participants’ expectations for the course. The prompts for the pre-training group were
What kind of work do you do in your community under the Kore Fanmi programme or community organisation?
How many people live in your community that you work in? (provide a range)
What are some common water, hygiene and sanitation issues you face in your community?
How was your experience with the last year’s WASH training?
How did you apply the training in your respective communities/organisations?
How will this training be used in your daily lives?
Each prompt was followed by group discussion around the topic, including follow-up questions informed by participants’ initial responses.
A second set of focus groups were held on the final day of the didactic course using the same format and structure as the pre-training groups. Participants offered feedback on the course to inform future training. Prompts included, ‘What aspects of the training did you find helpful/not helpful?’ ‘How might you use the information from this training in your work in the community?’ What challenges would you face in implementing what you learned?’ What did the instructors do well/not well?’ What kind of support will be helpful as you work to implement your new knowledge/skills?’ and ‘Do you think this training will change your community’s WASH practices?’
Observation protocols
We conducted two sets of observations in the second week of the programme: (1) observations of supervisors as they taught WASH topics to JHAs and (2) field observations as JHAs disseminated WASH information to community members. Pre-established rubrics were used to record the time and location of services, to whom the services were delivered, tools and techniques used, fidelity to the curriculum, interpersonal skills, level of involvement/engagement of the participants and the compatibility of the instruction to the context of community members’ lives. Rubrics were completed during the delivery of services, and feedback was provided during debriefing sessions at the end of each day.
Data analysis
To assess changes in knowledge from pre-test to post-test, we used paired-samples t-tests confirmed by a nonparametric Wilcoxon signed-rank test. To assess the retention of knowledge from the previous year’s training, we used independent-samples t-tests to compare the pre-test scores of participants who had attended the previous training with those who had not attended. Qualitative data from focus groups and observations were analysed using an inductive approach informed by principles of consensual qualitative research (Hill et al., 2005) and constant comparative method (Bradley et al., 2007). In each step of the qualitative process, team members individually coded emergent themes from the data and then met for consensus building, where themes were combined into a single combined model. The team also worked together to identify quotes that represented the core ideas present in the data. At each stage in the analytic process, an external auditor reviewed the results for accuracy and representativeness and provided feedback to the full team for re-examination to consensus. To minimise potential bias, the study team discussed and addressed aspects of personal identity, culture, expectations about the data and team power dynamics throughout the research process (Hill et al., 2005).
Results
We evaluated the three primary goals of the CHW training course to improve WASH knowledge among CHW supervisors, to improve the capacity of supervisors to educate JHAs, and to empower JHAs to disseminate the knowledge in rural Haitian communities, including cultural compatibility of the content.
Demographic background of participants
The first week of didactic training was offered to 22 participants. The group consisted of 2 regional coordinators, 9 Kore Fanmi supervisors and 11 volunteer CHWs from local community organisations. Thirteen participants (59%) had received previous training on WASH topics. Participants ranged from 24 to 58 years old (M = 38). Ten held a university degree (45%), 10 held a high school degree (45%) and 2 participants had a primary school education (9%), representing a highly educated group in this setting. A majority of the participants (n = 17, 77%) were men. The second-week observational component included only the 9 Kore Fanmi supervisors (6 men, 3 women) who were overseeing the work of 45 JHAs.
Knowledge of WASH content and perceptions of usefulness
To examine the effectiveness of the training course at improving WASH knowledge among CHW supervisors, we examined changes from pre- to post-course on the test of WASH knowledge. Scores on the pre-course test were non-normally distributed, with skewness of −1.907 (standard error [SE] = 0.524) and kurtosis of 4.985 (SE = 1.014). Scores on the post-course test were normally distributed, with skewness of −.309 (SE = .524) and kurtosis of .900 (SE = 1.014). Since t-tests are moderately robust to violations of the assumption of normality (Hamilton, 2012), we use paired-samples t-test to examine the effectiveness of the training. Among the 19 training participants who completed both pre- and post-tests, there was statistically significant improvement in knowledge scores, with a mean improvement of 1.31 points, t(18) = 2.12, p = .048 (see Table 1). Given the small sample size, we also ran a nonparametric Wilcoxon signed-rank test which does not assume normality. The results confirmed that there was significant improvement in knowledge scores (Z = 2.12, p = .030).
Results of pre- and post-course knowledge tests on the course curriculum.
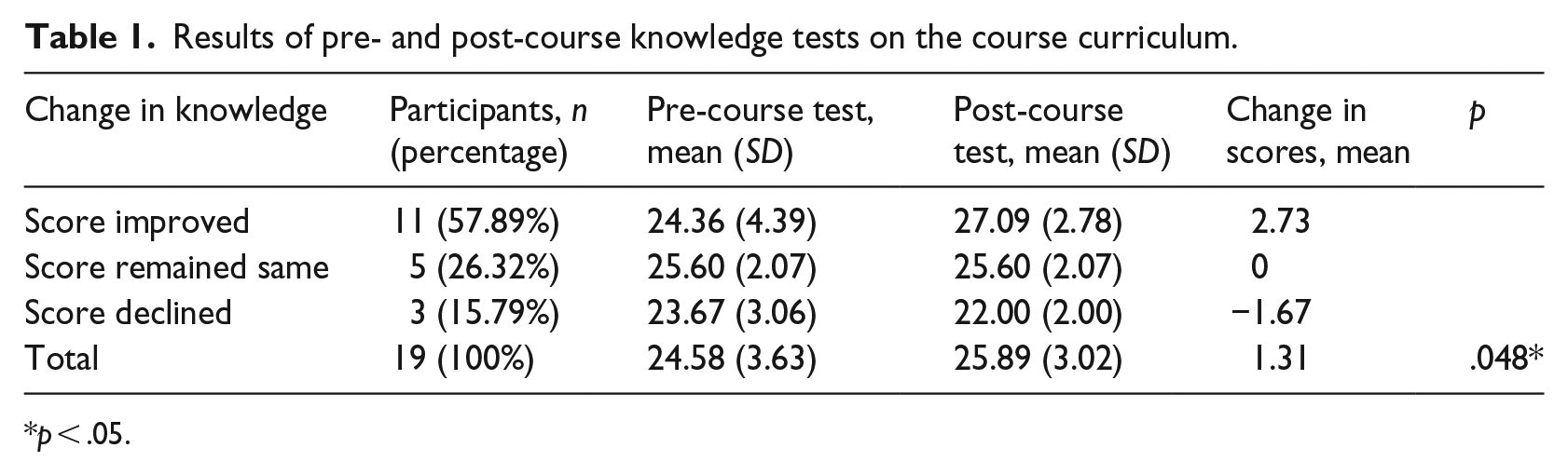
p < .05.
Participants with a university education scored higher than those with a high school education or less on both the pre-test (mean = 26.8 vs 22.0) and post-test (mean = 27.2 vs 24.8). Lower educated participants showed much greater improvement from pre-test to post-test; however, the improvement of university participants may have been hindered by a ceiling effect.
We assessed knowledge retention over the course of a year by comparing pre-course test scores of new versus repeat participants. Results of independent samples t-test revealed no significant difference in scores between those who completed last year’s training (n = 13, mean = 24.29, SD = 3.95) and those who had not (n = 6, mean = 25.40, SD = 2.70). A nonparametric Mann–Whitney U test confirmed the finding (U = 31.00, p = .754). Although limited by the small sample size, this result may indicate that course knowledge was not well-retained 1 year later.
Helpful aspects of the didactic training
In focus groups, participants consistently reported that the course was helpful for their work in the community (see Table 2). Participants strongly approved of the training focus on practical tools for promoting healthy WASH practices. They noted that learning to build fly and rat traps helped them to see how they could implement teaching by building useful tools with community members. Similarly, participants spoke highly of the interactive teaching methods used by the instructors, including role-playing, participant presentations and group discussions. One participant stated, ‘you did not just teach us, but also included everyone to share their experiences with us’.
Qualitative results of pre–post focus groups.

Typical: endorsed by more than half of participants; variant: endorsed by more than two, but fewer than half of participants; rare themes (endorsed by two or fewer participants) not listed. WASH: water, sanitation and hygiene; CHW: community health worker.
Unhelpful aspects of the didactic training and areas to improve
When prompted to provide areas of improvement for the training, about 40% of participants talked about needing more practice in teaching methods. Many noted that the need for translation to Creole slowed the teaching process, took away from valuable classroom time and hindered their ability to make personal connections with the instructors. Participants felt the inclusion of more Creole-speaking trainers would save time and improve comprehension.
Others expressed the desire for more frequent training, with a preference for courses every 3–6 months rather than only once per year. A number of trainees expressed that they would like to have more community members have the opportunity to participate in the training, particularly ‘those representing local federations and working in different community roles, for example, school or church leaders’. Finally, participants requested additional information on certain content areas, such as expansion of the content on leadership development and managing diarrhoeal illness, and adding information about the Ebola virus, which was not discussed in this year’s programme.
Ability to teach content to JHAs
Through observation of supervisors’ training presentations and JHA field visits, our evaluation concluded that the TTT model improved practical application by bridging the gap between theory and implementation. Participants enthusiastically expressed that they would take personal responsibility to disseminate the knowledge they gained in the training, both within the Kore Fanmi network and in the community at large. For example, one participant stated, ‘I am already a community leader; I will be going to local schools, churches, and markets to reinforce the capacity of my community workers’. As supervisors (n = 9) provided training sessions to JHAs, the content was accurate and highly reflective of the week 1 didactic training. In addition, participants expressed a desire to follow the lead of the course instructors by using more interactive teaching methods in their training activities.
In observations of the training presentations, supervisors utilised a variety of tools and materials, similar to the approach of the instructors from week 1. All supervisors used fly-charts for visual aids and emphasised key points with relevant examples. They engaged participants in discussions to encourage depth of processing. Six supervisors used role-plays to demonstrate and practice home visits, including strategies for managing challenging situations that the JHAs might face. Supervisors frequently referred to the training textbook and used examples and images provided in the text, which contributed to high fidelity of the presentations to the CHW training course. Notably, three supervisors provided live demonstrations during the didactic training, including an innovative way of building a ‘tippy-tap’ or hands-free water spout using local materials. Participants were able to transmit knowledge in creative ways, appropriate to the local audience and context (see Table 3).
Qualitative results: observations of training presentations/home visits.
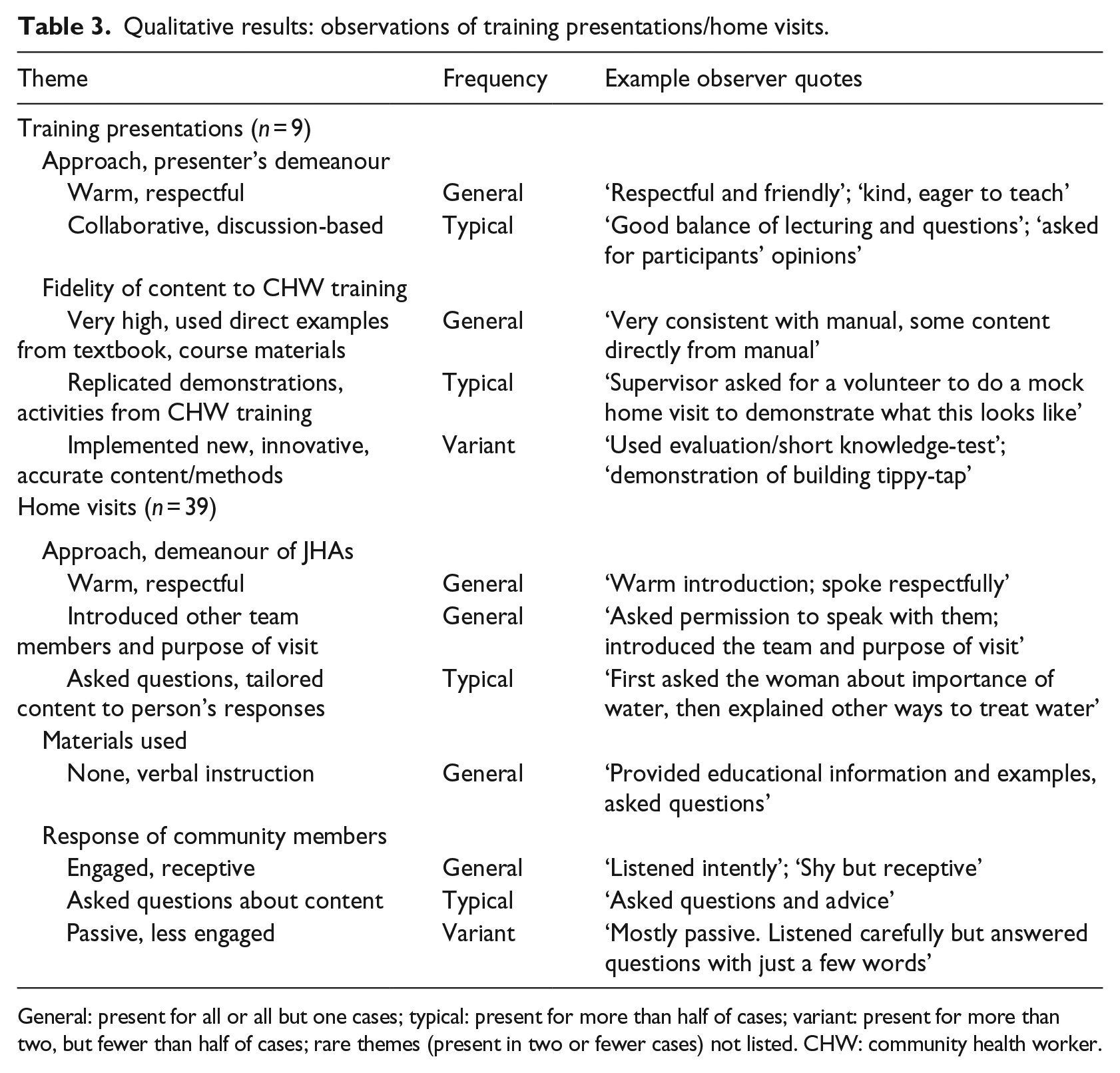
General: present for all or all but one cases; typical: present for more than half of cases; variant: present for more than two, but fewer than half of cases; rare themes (present in two or fewer cases) not listed. CHW: community health worker.
Potential for transmission of knowledge to the community
Following their training presentations, each of the nine supervisors accompanied JHAs into nearby neighbourhoods to observe the delivery of content to community members. Each group completed 3–5 home visits for a total of 39 visits. The instructors observed the home visits in order to assess the application of the training curriculum and provide guidance during feedback sessions held immediately afterward.
Keeping with cultural norms, JHAs were courteous and respectful throughout the visits. They first asked permission to speak to the residents and introduced themselves and the purpose of their visit. A majority of the JHAs first assessed the individuals’ knowledge of the topic and then provided additional information as necessary. The content covered during the home visits, such as assessing the family’s water sanitation practices, discussing proper handwashing, discussing the dangers of open defaecation and the proper disposal of food waste, was consistent with the didactic training and closely reflected the cultural and practical realities of community members. For example, JHAs discussed the importance of keeping water vessels clean and storing them indoors when not in use, rather than encouraging the use of sanitation tablets or other methods that are expensive or not readily available. When children were present, JHAs appropriately assessed needs and provided information about children’s vulnerability to diarrhoeal illness (see Table 3).
Barriers to implementation
When participants were asked to identify obstacles to implementing the training content, multiple trainees noted that ingrained cultural practices were an important issue. One participant shared, ‘People have pre-set expectations about how it should be, and it is difficult to change old practices among people’. Some trainees expressed concern about addressing topics considered culturally taboo, such as male participants discussing menstrual cycles and menstrual hygiene with women, but participants responded well to instructor suggestions to manage discomfort around such topics.
Cultural compatibility
While the sponsoring organisations have made efforts to improve the cultural fit of the programme, there are challenges associated with using non-Haitian volunteers to lead the training. A new development for 2016 was that course instructors completed a cultural competency training prior to their arrival in Haiti. This included an interactive workshop led by a psychologist with expertise in cross-cultural education. Participants arrived in Haiti 2 days prior to the start of the training to orient themselves to the country, including a presentation from a Haitian staff person, a visit to a museum and visits to local health clinics. The cultural competency training and orientation, although brief, provided valuable opportunities for the instructors to learn about the Haitian context in order to inform their instruction.
In the didactic component of the course, instructors worked closely with the interpreters to adapt class materials, illustrations and group activities. The interpreters were valuable members of the team who were frequently asked to assist in cultural, as well as linguistic, interpretation. However, the need for translation also created delays in instruction, particularly when difficult concepts or cultural misunderstandings had to be clarified. Based on feedback from the 2013 evaluation, the 2016 programme included a Haitian instructor for the first time. In training sessions conducted in Creole, the content was delivered more efficiently and questions were answered more clearly. As a result, these lessons were received more positively by participants.
Participants were generally enthusiastic about the knowledge they gained in the training but expressed concern about putting the knowledge into practice. For instance, one participant noted, ‘If they are talking about water disinfection, they need purification tablets. If they are talking about malaria, they need mosquito nets. When teaching about family planning, they need condoms’. Although the 2016 training attended to concerns related to resource scarcity by incorporating lessons about how to build tools using locally available materials (e.g. building fly traps from plastic bottles), health workers continued to express a need for new resources to carry out their work.
Discussion
The CHW training programme used the tiered leadership structure of Kore Fanmi to implement a TTT course focused on WASH. Evaluation findings demonstrated that supervisors improved in their WASH knowledge in clean water practices, proper handwashing, waste disposal, food preparation, sanitation and hygiene for mother and baby, and latrine basics, and they appreciated the course content and manner of instruction. They strongly felt that the training would be helpful and would positively influence their work. In assessing the application of course content, WASH knowledge was effectively transmitted from course instructors to supervising CHWs and JHAs. As a result, a small number of well-trained supervisors now has the capacity to reach approximately 15,000 families in the region by educating the JHAs assigned to meet with those families. Supervisors’ training content was largely consistent with the didactics of the first week and participants effectively served as cultural filters by ensuring content was reflective of the local context. Similar positive results were achieved as JHAs disseminated WASH knowledge to local households. JHAs interacted with community members warmly and respectfully, inquired about existing knowledge to identify gaps and needs, offered sound guidance and culturally appropriate education, and were observant of their surroundings.
While the findings were largely positive, concerns remain about the retention and application of course content. New participants had similar pre-test knowledge when compared to those who participated in a previous training. Participants also reported lacking resources or opportunities for further education or feedback, which likely contributed to the lack of retention. To address these challenges, CHWs require more consistent support in their work, reinforcement of instructional content and encouragement to apply their knowledge in the community.
Limitations
Several limitations in the study should be acknowledged. The training was offered to a small cohort working in a limited geographic area. Thus, results should be generalised with caution. Future evaluations may seek to include a larger sample and a control group, or utilise a single-subject design, to better understand the mechanisms of change and potential influence of confounding variables (Lwin et al., 2018). We took steps to reduce social desirability bias; however, participants may still hesitate to give negative feedback for fear that it may negatively impact their standing or the sponsors’ support of the programme. Finally, the study was a short-term evaluation that did not measure impact beyond the initial training period. Future studies should follow up on programme participants over time to assess the sustained practical application of knowledge and impact in the community.
Implications and recommendations
The Kore Fanmi training programme has successfully replicated previous CHW frameworks to develop ‘a readily available network of CHWs who can provide a community-based system of care and support that complement the formal health care system’ (Han et al., 2007: 519). Moreover, given the success of the training programme in Haiti, a similar model was recently implemented in the rural region of the USA by Heart to Heart International. This not only indicates the potential replicability of the model but also the mutually beneficial nature of global partnerships of the kind implemented here (Knettel et al., 2017).
In addition to these successes, there are challenges to the programme worth noting. Participants lack resources or opportunities for further education or feedback after the initial training. Thus, it is vital to provide more frequent, ongoing training for supervisors and to support an apprenticeship model that focuses on practical application of knowledge among JHA trainees (Kaiser and McLean, 2015). The apprenticeship model moves beyond the TTT approach by emphasising peer supervision, oversight and support in the daily work of JHAs, with gradual steps towards independence. For example, an apprentice JHA might first shadow a more experienced health worker, then conduct home visits while being observed, before taking on an apprentice of her or his own. This model enables trainees to receive immediate feedback within a supportive environment.
Active, collaborative and participatory teaching strategies have proven to be particularly effective in health worker trainings (Missingham, 2013; Werner and Bower, 2012). We recommend future workshops continue to include these components. This includes demonstrations using local resources and are economical to implement, such as the tippy-tap.
In this study, participants expressed concern about the inefficiency of translating the training content from English and responded positively to Creole-speaking instructors. Consistent with earlier evaluations (Knettel et al., 2017), we recommend that future CHW training programmes integrate Haitian instructors to minimise cultural confusion and content gaps. The recruitment of local trainers also allows for more regular contact among instructors and participants, empowering participants to seek support and enabling instructors to offer more consistent mentorship for course participants.
Towards the future
The Haiti Kore Fanmi tiered organisational structure and the growing capacity of CHW supervisors sets the stage for future success. However, future evaluations must move beyond simply assessing the potential for community impact and examine the actual effectiveness of the CHW programme in improving community health literacy and health behaviour. Based on our results, we predict that a lack of tools and supplies will create challenges for JHAs’ ability to motivate behaviour change in the community. Without practical resources such as instructional materials, the health education offered by CHWs may not have the desired impact of improved health outcomes in the region. Future programmes need to provide trainees with laminated instructional materials to assist them in explaining their ideas. In response to the concern of resource scarcity, we recommend that the sponsoring organisations move beyond didactic instruction to provide tangible, economical and durable resources for improving community health. This includes pairing educational programmes with investment in broader economic development and improvement of community infrastructure, such as water treatment tools and/or sanitation facilities (e.g. latrines).
Conclusion
Overall, this evaluation found that the TTT model was effective at improving the reach of educational content and would likely be a strong fit for many international organisations administering similar programmes. Week 1 training was effective at improving participants’ WASH knowledge, and the practical component in week 2 demonstrated the potential for effective dissemination. The combination of didactic training and practical application serves to build local capacity and empowers CHWs to take a leadership role in health education in local communities (Han et al., 2007). When implemented effectively, a TTT model of health education can have a cascade effect, whereby sound education provided to a small number of CHWs can reach thousands of families in hard-to-reach areas.
Supplemental Material
Appendix_A_KnowledgeTest_(1) – Supplemental material for Healthy People, Healthy Community: Evaluation of a train-the-trainers programme for community health workers on water, sanitation and hygiene in rural Haiti
Supplemental material, Appendix_A_KnowledgeTest_(1) for Healthy People, Healthy Community: Evaluation of a train-the-trainers programme for community health workers on water, sanitation and hygiene in rural Haiti by Xiaoran Yu, Asmita Pendse, Shay Slifko, Arpana G Inman, Peggy Kong and Brandon A Knettel in Health Education Journal
Footnotes
Acknowledgements
We thank our partners from Kore Fanmi. We also thank Janice Ballard, Steve Hower, Steve Weber, Paula Kapotes, Carla Orner, Jennifer Farrington, Christophe Rodrigue, Josue Andre, Luxon Atis, Cito Baptiste and Fristzcar Jean for their support in carrying out the study.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: Expenses associated with conducting this evaluation, including travel and lodging in Haiti, were covered by Heart to Heart International and BD. The authors received no additional compensation for the research.
Supplemental material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.