
Abstract
Background:
Medical students are at risk of poor mental health and burnout compared to general population age- and education-matched peers, which has future implications for patient care. Research has suggested that demographic factors can predict mental illness and burnout among medical students. However, less is known about predictors of mental health and how they compare to predictors of burnout, and few studies have examined multiple demographics simultaneously.
Objectives:
This study examined and compared demographic predictors (gender, ethnicity, age, level of education, year of study and proposed specialty) of mental health and burnout in first to fourth year Canadian medical students.
Method:
Medical students (n = 129) completed online surveys comprised of validated questionnaires.
Results:
Multiple regression indicated that third year (β = −.243, p = .013) negatively predicted mental health (R2 = 15.0%). Female gender (β = .242, p = .005), ‘other’ ethnicities (β = .189, p = .028), third year (β = .391, p < .001) and fourth year (β = .212, p = .023) positively predicted burnout (R2 = 32.7%). Female gender and fourth year predicted mental health and burnout differently. ‘Other’ ethnicity, second year and third year predicted mental health and burnout similarly.
Conclusion:
Findings fill gaps in the literature and may inform medical stakeholders in developing targeted programmes for improving medical students’ mental health and burnout. Medical students with greater well-being can progress into physicians who will be more likely to promote well-being in their patients.
There has been a growing concern regarding the increase in mental illness in the general population over recent years. By age 40, about 50% of the Canadian population will have experienced a mental illness (Canadian Mental Health Association, 2018). Rates in the USA are similar, with almost half the population (47.4%) experiencing a mental health disorder in their lifetime (Kessler et al., 2009). Conversely, positive mental health is more than the absence of mental illness. Keyes’ complete state model conceptualises mental health as the combination of emotional, psychological and social well-being, with higher levels of each representing better mental health (Keyes, 2002). Keyes’ dual continua model later defined mental health along one continuum, ranging from languishing, the lowest level of mental health, to flourishing, the highest level of mental health, with mental illness being on a separate continuum (Keyes, 2014).
Burnout is another construct composed of high levels of emotional exhaustion (EE), depersonalisation (DP) and low levels of personal accomplishment (Maslach et al., 1996). Signs of EE include increased fatigue or feeling worn out from one’s work, DP can be seen with negative attitudes towards patients and feelings of cynicism, and a lack of personal accomplishment includes reduced confidence and satisfaction regarding one’s work (Maslach et al., 1996). Burnout has been defined as an emotional response to workplace stressors, such as heavy workload (Maslach et al., 2001). Medical students are one group that is at an increased risk of burnout compared to the general population (Brazeau et al., 2014; Dyrbye et al., 2014). For example, nearly 50% of medical students in one US study reported burnout compared to 36% of general population peers (Dyrbye et al., 2014). If burnout in medical students is left untreated, problems can arise, including substance abuse, depression, suicide and poor patient care (Dyrbye et al., 2017).
Medical students are at an increased risk of mental illness during their education relative to the general population and age-matched peers (Brazeau et al., 2014). Depression prevalence in Canadian medical students has been reported at 41.5% in cross-sectional research (Matheson et al., 2016) compared to 4.7% in the general population (Statistics Canada, 2018). What is more worrisome is that the consequences of mental illness have been shown to persist into physician-hood (Dyrbye et al., 2005). In fact, early career physicians are over six times more likely to require treatment for a mental health problem if the issue was experienced during their education (Tyssen et al., 2001).
Much research has reported on the relationships between certain demographics and mental health, mental illness and burnout in medical students. A systematic review reported that female medical students show higher rates of depression than male medical students (Dyrbye et al., 2006). Furthermore, third year medical students report more depressive feelings and higher levels of burnout compared to medical students in other years of study (Cecil et al., 2014; Santen et al., 2010). Minority ethnic medical students who are relatively older (Dyrbye et al., 2012), have higher levels of education prior to admission (Puthran et al., 2016) and who are interested in pursuing primary care specialties (Compton et al., 2008) also report worse mental health and higher levels of depression and burnout.
However, two systematic reviews show that research has predominantly examined the relationship between demographics and mental illness in medical students (Dyrbye et al., 2006; Puthran et al., 2016), leaving a dearth of knowledge of predictors of mental health. Two studies have examined the relationship between demographics and medical students’ mental health, not mental illness, but did not address as many demographic variables as the present study aims to (Dyrbye et al., 2012; Van Dijk et al., 2017). In addition, research on age and education level as predictors of medical students’ mental health is scarce and warrants further investigation (Kim and Kim, 2017). Finally, no studies have compared predictors of mental health and burnout in medical students. This study sought to address these gaps in the literature.
Regrettably, it is not uncommon for medical students to let mental health issues experienced during medical school go unaddressed as the culture of medicine reinforces the view that medical professionals are invincible and it is frowned upon to show signs of weakness (Dunn et al., 2008; Wallace et al., 2009). Research has shown a direct link between the mental well-being of physicians and patient care, making physician wellness an indicator of healthcare system quality (Wallace et al., 2009). One example of this is the association between poor physician health and increased medical errors (Dyrbye et al., 2017).
Providing knowledge on demographic predictors of mental health and burnout in medical students may help to de-stigmatise these issues (Hampson et al., 2018) and can inform preventive efforts in at-risk groups, thus highlighting the importance of this study. This knowledge can benefit stakeholders in developing targeted programmes to address issues concerning mental health and burnout in medical schools to optimise medical students’ mental health. Given that mental health issues can persist beyond medical school and negatively affect patient care (Dyrbye et al., 2005), promoting the positive mental health of medical students could be the first step in supporting the ongoing well-being of medical professionals and their patients.
The aim of this study was to investigate demographic predictors of mental health and burnout in Canadian medical students. The primary objective was to examine how six common demographics (gender, ethnicity, age, level of education, year of study and proposed specialty) predict mental health in medical students. It was hypothesised that medical students who are women, of minority ethnic background, relatively older (i.e. >30 years), have higher levels of education, are in the third year of study and are intending to pursue primary care (e.g. family medicine) would have lower levels of mental health (Cecil et al., 2014; Compton et al., 2008; Dyrbye et al., 2012; Puthran et al., 2016). A secondary objective was to examine whether or not these six predictors are similarly related to both low levels of mental health and high levels of burnout. Given that mental health and burnout are negatively related (Puig et al., 2012) yet exist on two separate continua (Keyes, 2002; Payton, 2009), it was hypothesised that there would be some similarity in how demographics relate to mental health and burnout, but that there would not be a complete overlap of these relationships.
Methodology
Research design
This study used a cross-sectional design. Data were collected using online surveys comprised of validated questionnaires. Approval from the Faculty of Medicine and ethical approval from the Queen’s University Health Sciences and Affiliated Teaching Hospitals Research Ethics Board (no. 6022151, department code PHE-172-17) and the McGill University Research Ethics Board II (no. 177-0917) were granted for the study.
Participants and procedures
The population of interest was all medical students enrolled at two large Canadian universities. Inclusion criteria were that students must be in the first to fourth year of study and comprehend English. The sample (N = 141) was obtained through opportunity sampling out of a possible 1,140 enrolled and corresponded to a 12.4% response rate. This was expected as it is consistent with other studies among medical students (Cecil et al., 2014; Dyrbye et al., 2014). Furthermore, our sample size was deemed sufficient as a power analysis indicated that 98 participants would be required to achieve a medium effect size with 80% power and six predictor variables in each regression model. Medical students in this sample ranged from 19 to 42 years of age (M = 24.91, standard deviation [SD] = 4.31) and just over the majority were women (56.6%), which is representative of the Canadian medical student population (The Association of Faculties of Medicine of Canada, 2018). Table 1 provides additional sample characteristics.
Mental health, burnout and demographic characteristics of first to fourth year medical students (n = 129).
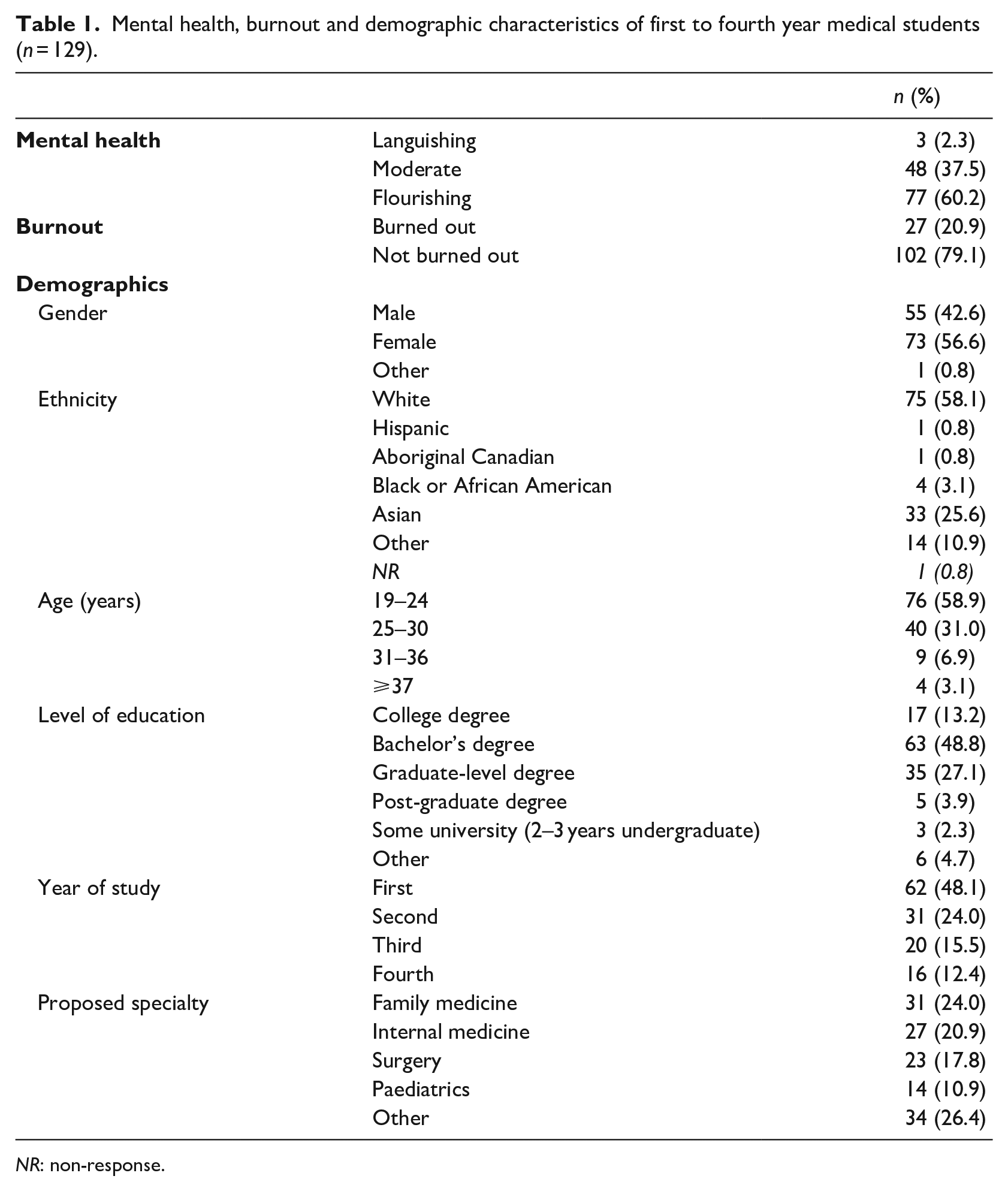
NR: non-response.
The survey was administered between November 2017 and January 2018 through the online platform SurveyMonkey, which follows data collection methods for other mental health studies among medical students (Cecil et al., 2014; Dyrbye et al., 2007; Matheson et al., 2016). Survey links were distributed through medical student Facebook groups and e-newsletters as well as an in-class announcement for first year students at one university in November 2017; announcements were not approved by the Faculty of Medicine at the second university. Two follow-up reminders were sent in an effort to increase the response rate. All participants provided written informed consent for their data to be used in this research via a yes/no checkbox on the first page of the online survey.
The survey was administered mid-semester in an attempt to give an adequate representation of medical students’ usual mental health. Nonetheless, some students completed the survey after the end of semester. However, there were no significant differences in medical students’ mental health or burnout between these two time periods. To reduce potential harm due to sensitive questions on mental health and burnout, contact information for local psychological services was provided should participants wish to access it. Participants were incentivised to partake with the opportunity to provide an e-mail address to enter a prize draw to win a FitBit Alta.
Measures
Demographic measures
Six questions provided information on gender (male, female or other), ethnicity (White, Hispanic, Aboriginal Canadian, Black/African American, Asian or other), age, highest level of education to date (college degree, undergraduate-level degree, graduate-level degree, professional post-graduate degree or other), year enrolled in medical school (first, second, third or fourth) and medical speciality most likely to be practised in the future (family medicine, internal medicine, surgery, paediatrics or other). Other ethnicities reported by medical students included South Asian, Jewish, Sri Lankan, Iranian, North African, Arab, European, Bengali Canadian, Mediterranean, Han and Asian-Caucasian. These are common categorisations of demographic variables based on previous studies with medical students (Compton et al., 2008; Dyrbye et al., 2007).
Mental health measure
The 14-item Mental Health Continuum Short Form (MHC-SF) 1 was used to assess mental health according to three dimensions of well-being: emotional (three items, for example, ‘happy’), social (five items, for example, ‘that you belonged to a community’) and psychological (six items, for example, ‘that your life has a sense of meaning to it’) well-being (Lamers et al., 2011). Items are rated on a 6-point Likert-type scale assessing their frequency in the past month (0 = ‘never’, 1 = ‘once or twice’, 2 = ‘about once a week’, 3 = ‘about two to three times a week’, 4 = ‘almost every day’ and 5 = ‘every day’). These items showed very good internal consistency (Cronbach’s alpha = .91) (Pallant, 2016). Similar to previous research (Van Dijk et al., 2017), total continuous mental health scores of 0–70 were used, with higher scores representing better mental health.
Respondents were also categorised as flourishing, moderate or languishing. Flourishing was indicated by feeling ⩾1 emotional well-being symptom(s) ‘every day’ or ‘almost every day’ (items 1–3) and ⩾6 social or psychological well-being symptoms ‘every day’ or ‘almost every day’ (items 4–14). Languishing was indicated by feeling ⩾1 emotional well-being symptom(s) ‘never’ or ‘once or twice’ (items 1–3) and ⩾6 social or psychological well-being symptoms ‘never’ or ‘once or twice’ (items 4–14). Moderate mental health was indicated by scores that were neither flourishing nor languishing (Keyes, 2002).
Burnout measure
The two-item Maslach Burnout Inventory (MBI) was adapted from the full 22-item MBI (Maslach et al., 1996) and has been deemed to be a valid and reliable instrument that has been widely utilised for measuring EE, DP and total burnout in medical students (Shanafelt et al., 2019; West et al., 2012). Responses for the two items, assessing EE and DP, are rated on a 7-point Likert-type scale (0 = ‘never’, 1 = ‘a few times a year or less’, 2 = ‘once a month or less’, 3 = ‘a few times a month’, 4 = ‘once a week’, 5 = ‘a few times a week’ and 6 = ‘every day’). Scores for EE and DP are added for a total burnout continuous score of 0–12; higher scores indicate higher levels of burnout. This scale showed an acceptable internal consistency (Cronbach’s alpha = .72); however, as the number of items was small, an inter-item correlation was run, which showed a strong correlation of .57 (Pallant, 2016). In line with previous medical student research using the two-item MBI, respondents were categorised as burned out if they responded ‘once a week’ or more often to either of the EE and/or DP subscales (Dyrbye et al., 2014; West et al., 2012).
Data analysis
Data from the online surveys were downloaded from SurveyMonkey into Microsoft Excel 2013. Statistical analyses were performed using the statistical software package SPSS version 23 for Windows (IBM Corporation, 2015).
Predictors of mental health in medical students
To address the first research question, correlation and multiple linear regression were used to identify predictors of mental health (continuous) (n = 129). As a secondary analysis, multivariate logistic regression was used to assess differences according to the mental health category (i.e. flourishing, moderate and languishing). Categorical demographics were dichotomised for correlation (Table 3) and were dummy-coded for linear regression (reference groups: male gender, White ethnicity, college degree, first year of study and family medicine). Gender was used as a dichotomous variable (male, female) as only one participant identified as transgender female-to-male, which was removed as the sample size was too small. Differences were determined as significant at an alpha level of .05. Effect sizes for linear regression were reported using Cohen’s f2 (⩾.02 small effect, ⩾.15 medium effect and ⩾.35 large effect) (Cohen, 1988) and effect size for logistic regression in odds ratios (ORs). Post hoc analyses to compute achieved power were run using GPower 3.1 (Erdfelder et al., 1996).
Comparing predictors of mental health and burnout in medical students
To address the second research question, all analyses were repeated using burnout in place of mental health. To test whether or not predictors of mental health and burnout were similar, standardised beta weights with 95% confidence intervals (CIs) were estimated using bias-corrected bootstrapping (1,000 resamples). Proportion overlap was assessed for overlapping CI arms of each pair of beta weights (Cumming, 2009). CIs with a proportion overlap of <50% corresponded to p < .05 and a statistically significant difference (Cumming, 2009). Since the MBI-2-item is scored negatively (i.e. higher scores indicate worse health) and the MHC-SF is scored positively (i.e. higher scores indicate better health), beta weights for burnout were reversed.
Results
Preliminary analyses
Preliminary analyses were performed to assess for violations of the assumptions of normality, homoscedasticity, independence of residuals and collinearity. Outliers were removed from continuous mental health (n = 3) and burnout (n = 6) total scores. A missing values analysis was run showing that 8.64% of data were missing. Four cases were missing not at random and were removed (i.e. respondents skipped entire questionnaires). Little’s MCAR (missing completely at random) test subsequently confirmed that some remaining data were missing completely at random, χ2(106, N = 129) = 103.863, p = .541, after which these data were imputed using Expectation–Maximisation (Musil et al., 2002). There were no differences in mental health (t = 1.037, p = .302) or burnout (t = 1.364, p = .175) between those who responded before or after 25 December, indicating no response bias. A correlation matrix is presented in Table 2.
Correlations between demographics, mental health and burnout in medical students (n = 129).
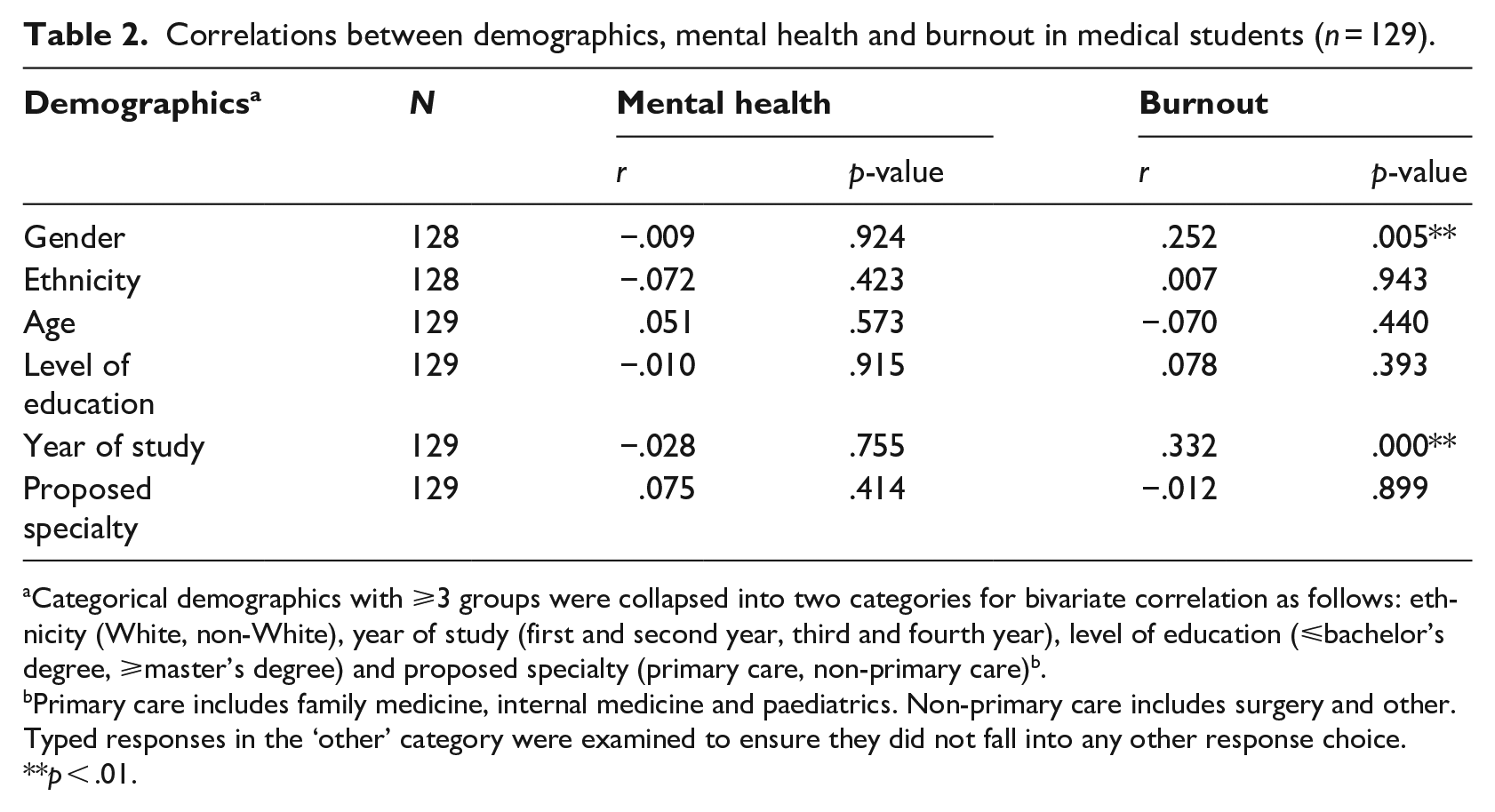
Categorical demographics with ⩾3 groups were collapsed into two categories for bivariate correlation as follows: ethnicity (White, non-White), year of study (first and second year, third and fourth year), level of education (⩽bachelor’s degree, ⩾master’s degree) and proposed specialty (primary care, non-primary care).
Primary care includes family medicine, internal medicine and paediatrics. Non-primary care includes surgery and other. Typed responses in the ‘other’ category were examined to ensure they did not fall into any other response choice.
p < .01.
Predictors of mental health in medical students
Results showed that the overall model explained 15.0% of the variance in mental health. Although this was not significant, p = .120, it showed a medium effect size (Cohen’s f2 = .153) and achieved a power of .92. Third year of study was the only significant predictor (β = −.243, p = .013), indicating that being in third year significantly predicted lower mental health scores compared to being in first, second or fourth year of study. Some responses were removed from the model due to elevated Mahalanobis values, including Hispanic (n = 1), Aboriginal Canadian (n = 1) and Black/African American ethnicity responses (n = 4), and 2–3 years undergraduate (n = 3) and post-graduate (n = 5) level of education responses.
Examination of demographic differences according to the mental health category confirmed the first analysis. Multinomial logistic regression was run with all independent variables; however, ethnicity was removed due to singularity in multiple categories (Aboriginal Canadian and Black ethnicities). The subsequent model explained between 41.8% (Cox and Snell’s R2) and 53.4% (Nagelkerke’s R2) of the variance in the mental health category; however, it was not significant, χ2(64, N = 129) = 69.790, p = .289. Year of study was the only significant predictor, with third year of study being a significant predictor of moderate compared to flourishing mental health (p = .003). Specifically, medical students who were in the third year compared to the fourth year were over 39 times more likely to report moderate compared to flourishing mental health (OR = 39.200). No significant differences among any other demographics were found according to mental health categories.
Comparing predictors of mental health and burnout in medical students
Results showed three significant predictors that explained 32.7% of the variance in burnout, p = < .001, with a large effect size (Cohen’s f2 = .366) and a power of .99. Specifically, being a woman (β = .242, p = .005) significantly predicted higher burnout scores compared to being a man (Figure 1), being in third year (β = .391, p = < .001) or fourth year (β = .212, p = .023) significantly predicted higher burnout scores compared to being in the first year of study, and medical students of ‘other’ ethnicities (β = .189, p = .028) significantly predicted higher burnout scores compared to those of White ethnicity. Age approached significance (β = −.166, p = .095), indicating that those who were younger were more likely to have reported burnout. Congruent with the mental health regression model, Hispanic (n = 1), Aboriginal Canadian (n = 1) and Black/African American ethnicity responses (n = 4) were removed due to small sample sizes and elevated Mahalanobis values. Both models are summarised in Table 3.
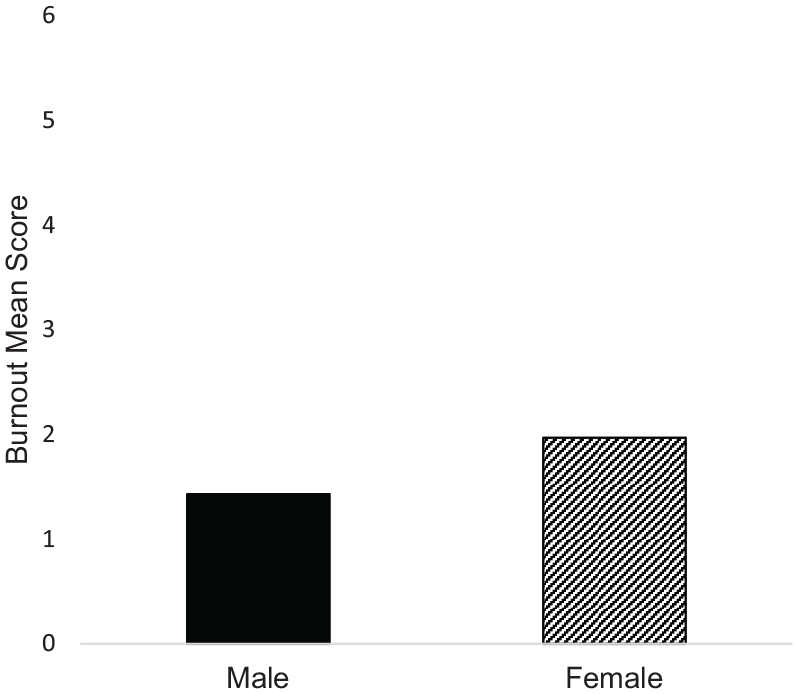
Differences in medical students’ burnout based on gender (n = 129).
Results from multiple linear regression of predictors of mental health and burnout.
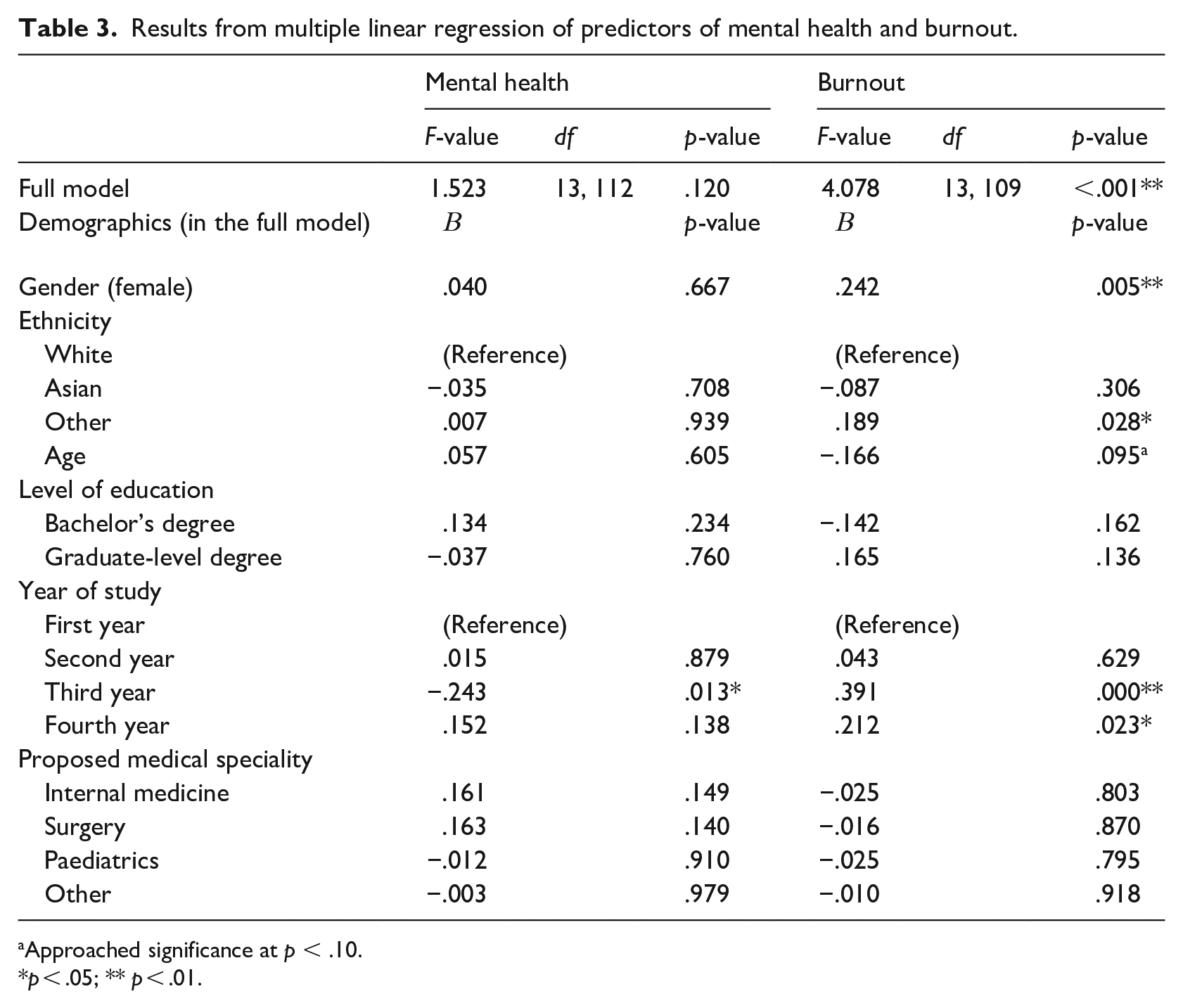
Approached significance at p < .10.
p < .05; ** p < .01.
Examination of demographic differences according to the burnout category partially confirmed the first analysis. The logistic regression model was significant, χ2(19, N = 129) = 35.790, p = .011, and explained between 24.2% (Cox and Snell’s R2) and 37.8% (Nagelkerke’s R2) of the variance in the burnout category. Third year of study significantly predicted burnout (p = .001), showing that medical students who were in the third year compared to first year were over 11 times more likely to be burned out (OR = 11.467). Female gender approached significance (p = .101), indicating that female medical students were almost three times as likely to report burnout compared to male medical students (OR = 2.665). No significant differences were found according to burnout categories among any other demographics.
Proportion overlap tests using Cumming’s (2009) parameters showed a significant difference for gender (proportion overlap <0.50, p < .05), indicating that female gender positively predicted burnout but did not predict mental health. ‘Other’ ethnicity similarly predicted mental health and burnout (proportion overlap >0.50, p > .05), indicating that although ‘other’ ethnicity positively predicted burnout, it was not statistically significantly different from its relation to mental health. Second and third year of study similarly predicted mental health and burnout (proportion overlap >0.50, p > .05), indicating that mental health outcomes paralleled burnout outcomes within each year of study (i.e. higher mental health plus lower burnout scores in second year and lower mental health plus higher burnout scores in third year). Finally, a significant difference was found for fourth year of study (proportion overlap <0.50, p < .05), indicating that fourth year positively predicted mental health and negatively predicted burnout (Figure 2). Age, level of education and proposed specialty were not significant predictors of mental health or burnout; thus, comparisons were not made. Table 4 shows all calculations.
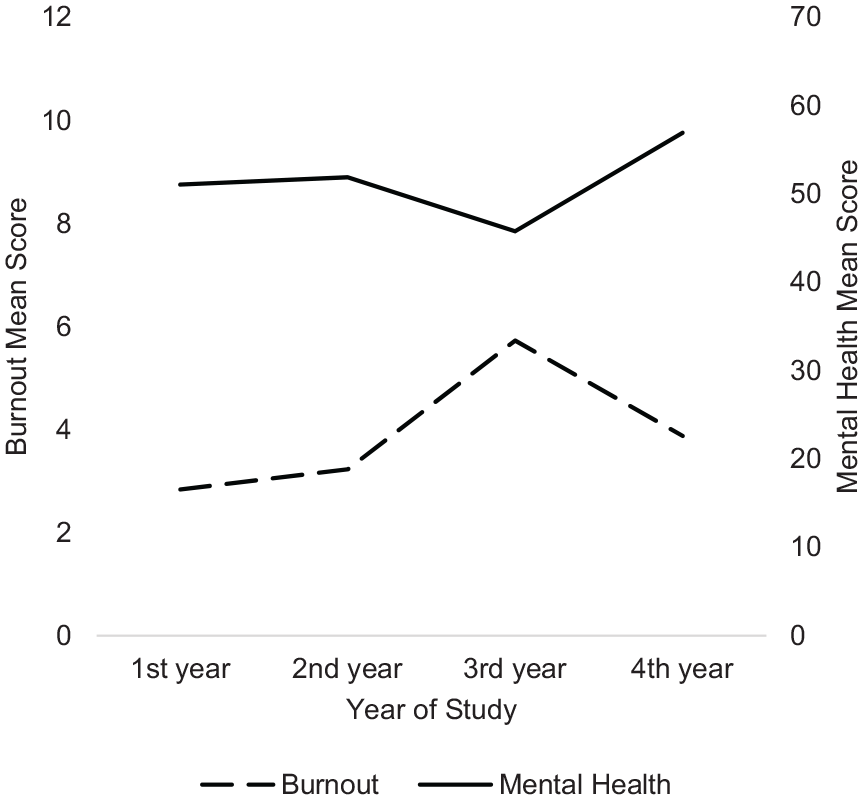
Differences in mental health and burnout between years of study in medical students (n = 123).
Results from testing the difference between 95% confidence intervals (CIs) of two beta (β) weights.
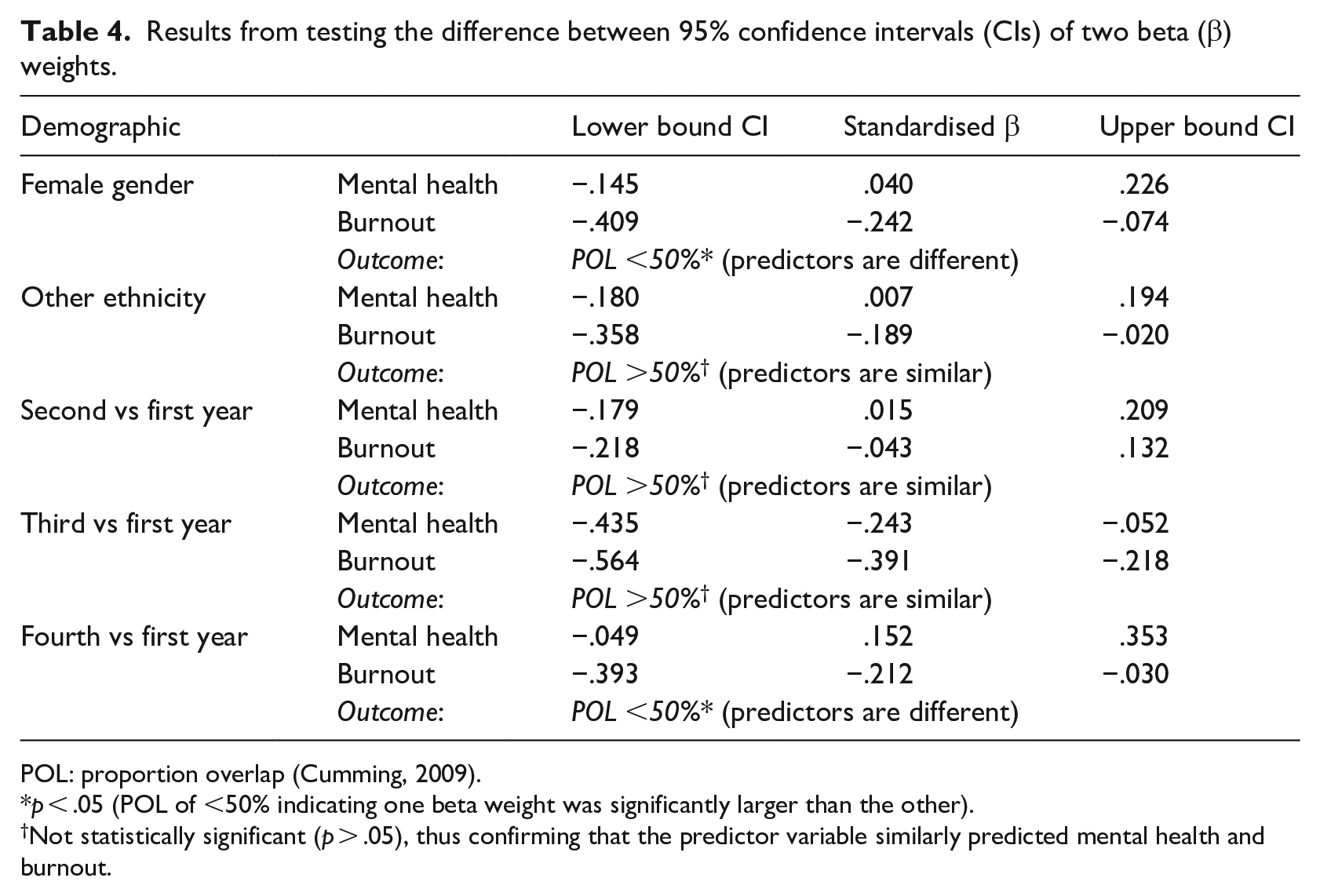
POL: proportion overlap (Cumming, 2009).
p < .05 (POL of <50% indicating one beta weight was significantly larger than the other).
Not statistically significant (p > .05), thus confirming that the predictor variable similarly predicted mental health and burnout.
Discussion
In line with our hypothesis, female medical students reported greater levels of burnout than male medical students. A recent systematic review has stated that female physicians may burn out as a result of fulfilling multiple family and work roles (Azam et al., 2017). Furthermore, research has reported a persisting climate of gender inequity in medicine (Jagsi et al., 2016). For instance, women in medicine report facing more sexual harassment than their male colleagues and feeling disadvantaged in their careers as a result (Jagsi et al., 2016). Specifically, one study found that 30% of female medical faculty reported sexual harassment compared to 4% of male faculty (Jagsi et al., 2016). Similarly, more female medical students have reported verbal or sexual abuse than male medical students (Dyrbye et al., 2005). Comparatively, mental health was similar between female and male medical students. Indeed, it is possible to experience high levels of burnout yet still feel happy, socially competent and psychologically fulfilled (Payton, 2009). Given the cross-sectional nature of this study, the factors contributing to burnout among female medical students in the present sample are unclear. Therefore, future research could investigate how both demographic (e.g. gender) and non-demographic variables (e.g. greater family responsibilities and spending more time with patients; Dunn et al., 2008) may contribute to higher levels of burnout among female medical students.
Medical students of ‘other’ ethnicities have reported higher burnout than medical students of White ethnicity. In other research, some minority medical students reported feeling that race had negatively impacted their education due to racial discrimination and cultural dissimilarities (Dyrbye et al., 2007). Despite action taken towards improving multiculturalism in Canadian universities over the past two decades, there remains a need to build an inclusive culture in medicine (Friesen, 2014). Specifically, a recent review has reported that increasing the representation of non-dominant cultures in leadership positions may help foster a positive workplace climate and promote the well-being of minority groups (Kang and Kaplan, 2019). Thus, future cross-sectional or qualitative research could examine the relationships between minority ethnicity status, inclusionary practices (e.g. engaging more medical leaders from minority or disadvantaged positions) and burnout among medical students.
As expected, third year of medical school significantly predicted lower mental health and higher burnout scores, which aligns with findings in systematic reviews (Dyrbye et al., 2006; Erschens et al., 2018). Third year medical students transition from classroom-based learning (i.e. didactic lecturing) to clinical training (i.e. clerkship and hospital rotations) and have reported greater patient responsibility and time constraints, identifying this transition as a major structural contributor to poor mental health and higher burnout compared to other years of study (Compton et al., 2008; Vogel, 2018b). Interestingly, our findings showed that mental health was lowest in third year and highest in fourth year, but burnout was high in both third and fourth year. This aligns with Keyes’ dual continua model (Keyes, 2014), which helps explain how medical students can experience flourishing mental health and high levels of burnout simultaneously (Figure 2). In support of this suggestion, a recent national survey among Canadian physicians found 60% to report flourishing mental health but 30% to report burnout (Vogel, 2018a).
Finally, moderate levels of mental health were reported by 70% of third year students in our study, further supporting the transition to clinical training as a psychologically difficult time for medical students. In sum, suboptimal levels of mental health in medical students should be of concern as less than flourishing mental health may diminish psychosocial health (Keyes, 2014) and patient care (Wallace et al., 2009).
Strengths and future directions
This study is the first to examine a combination of demographic predictors of positive mental health in medical students in a single study, which is a strength as most existing research has focused on mental illness using fewer demographics (Compton et al., 2008; Puthran et al., 2016). This research was also the first to compare predictors of mental health and burnout in medical students. Importantly, the study examined mental health instead of mental illness, supporting a positive shift from treatment to prevention. Findings from the study highlight an important gap in research examining medical students’ well-being, where the focus should not only be on mitigating negative health outcomes (i.e. burnout) but on achieving higher levels of positive health outcomes (i.e. mental health) as well.
In addition, this study identified demographic subsets of Canadian medical students at two institutions who are potentially at risk of poor mental health and burnout. Some key strategies to support long-term well-being may be applied moving forward. For example, intervention studies involving yoga (Prasad et al., 2016) or meditation (De Vibe et al., 2018) have been found to increase well-being among first to third year medical students. Thus, these approaches may be valuable for first and second year medical students to learn key health behaviours (e.g. physical activity) that help prevent burnout in third and fourth year.
However, some medical students may be reluctant to attend wellness-based courses voluntarily (Slavin et al., 2014); therefore, structural approaches could also be considered. For instance, research has suggested that incorporating practical experience into the medical curriculum earlier in training could enhance well-being among medical students in later years of training (Vogel, 2018b). Moreover, a review has identified role-modelling and zero-tolerance policies on harassment as two possible avenues for promoting positive workplace relationships and a culture of wellness in medical students (Dyrbye and Shanafelt, 2016). Importantly, changes such as these may offer value in efforts to mitigate harassment, competition and discrimination in the clinical workplace and to reduce burnout in medical students (Dyrbye and Shanafelt, 2016). Moving forward, cross-sectional or longitudinal research in these areas could help to better conceptualise the contributing factors to well-being in medical professionals in support of strengthening the healthcare system and providing better patient care down the line.
Limitations
The main limitation of this study was its cross-sectional design as no causality could be determined. Other limitations included the use of opportunity sampling and the low response rate, which can lead to bias and impact generalisability, as only a portion of medical students attending two of the 17 medical schools in Canada participated. Future research may usefully follow a cohort of medical students at a larger number of Canadian medical schools to measure changes in mental health and burnout longitudinally. Finally, future cross-sectional work should aim to survey the full student population at medical schools to produce more robust findings.
Conclusion
This study investigated demographic predictors of medical student mental health and burnout, indicating that third year of study negatively predicted mental health and positively predicted burnout, and female gender, ‘other’ ethnicities and fourth year of study positively predicted burnout. Practically, this research provides useful knowledge to medical stakeholders when targeting medical students at-risk for poor mental health and burnout to promote their ongoing well-being. Future efforts to improve mental health and burnout in medical students should be comprehensive, incorporating individual, organisational and structural approaches (Kang and Kaplan, 2019), such as through peer support, wellness programmes, curricular restructuring and improving workplace culture.