
Abstract
Objective:
This report identifies the profound effects that the COVID-19 pandemic and the resultant government lockdown have had on sexual health services delivery to a community of marginalised male sex workers in Nairobi, Kenya.
Methods:
Based on the experiences shared during ongoing virtual conversations with peer health workers, a case study was developed to identify the challenges encountered by peer health workers.
Findings:
Peer health workers confronted the new health crisis surrounding COVID-19 while also persisting in their efforts to deliver HIV services to male sex workers. Unable to receive status as ‘essential workers’, their actions often fell short in efforts to maintain male sex workers’ access to vital HIV prevention, treatment and care resources.
Conclusion:
The struggles encountered, amid dwindling resources, underscore the vital work needed to meet the health needs of a marginalised group that remains largely excluded from the government health system.
Introduction
We cannot get our peers as easily as we used to get them. The hotspots (places for cruising and selling sex) are closed due to curfew, and you know most sex workers work at night and the curfew prohibits people from working at night. And for those who are working, they are going to the clients’ homes, which is not safe since they cannot control the environment . . . the clients take advantage; condom negotiation is a problem and a lot of violence. The limitation in movement has limited what we as peer educators can do, for example, you can’t access your peers in the areas locked down, they can no longer come for their ARVs [anti-retroviral medication] in the clinic. We are forced to think about delivery since most clients are scared of going out . . . At times we feel we are sacrificing and risking our lives, and we don’t have PPE.
While the COVID-19 pandemic in Kenya has been characterised as less severe than in many economically advantaged countries, with fewer cases of serious disease and deaths reported (Nkengasong and Mankoula, 2020), the country’s response measures have been far more restrictive. They include a police-imposed curfew between 7 pm and 5 am and prohibited mobility between counties and neighbourhoods where the largest outbreaks have occurred (Kimani et al., 2020; Koh, 2020; Ombuor, 2020). In early July 2020, the Kenyan President Uhuru Kenyatta announced a ‘phased-strategy’ to loosen mobility by permitting domestic flights on July 15 and international travel on August 1, while lifting cessation of movement orders in the most highly affected regions of the country, including the Nairobi metropolitan area, Mombasa county and Mandera county. However, at the same time, the President extended the national curfew for an additional 30 days. Although restrictive measures, which take cues from World Health Organization (WHO, 2020) guidelines, are necessary for averting a major health systems crisis in an already resource-constrained and fragmented health system (El Sadr and Justman, 2020; United Nations, Economic Commission for Africa, 2020), we know far less about the inadvertent consequences of the COVID response for other important preexisting public health responses, such as HIV programming.
The HIV response in Kenya relies greatly upon the dedicated labour of peer health workers who are able to confront and mitigate forms of stigma that inhibit access to prevention and treatment resources (Geibel et al., 2012; Johnson and Khanna, 2004; Ngugi et al., 1996). The importance of peer health workers in Kenya’s HIV response extends a longer international history in which global systems of aid and national health development programmes invested considerably in the role that trained lay workers could play in delivering primary health care, especially in resource constrained settings where ‘failed’ and ‘hollowed-out’ states have given way to weakened health care systems (Maes and Kalofonos, 2013). Following the 1987 Alma Atta declaration, African governments institutionalised ‘community health worker programmes as a strategy to extend primary health care to impoverished rural and urban populations and to address the relationship between poverty, inequality and community health’ (Maes and Kalofonos, 2013). Today, with respect to HIV programmes, the centrality of community participation is vividly exemplified by the global policy integration of greater/meaningful involvement of people with HIV, a set of principles which has profoundly shaped the global landscape of HIV responses (Morolake et al., 2009; Mukherjee and Eustache, 2007; Ndhlovu and Matunhu, 2011).
An especially vital community-led response has been cultivated in Kenya among those who suffer the burden of the HIV epidemic – that is, ‘key populations’ which include highly marginalised people such as those who use and inject substances, female and male sex workers, and men who have sex with men. Groups of men who have sex with men have had an especially high HIV prevalence that well exceeds the national average (McKinnon et al., 2014). Within the context of state-sanctioned homophobia and the criminalisation of homosexuality, which was reinforced by a May 2019 Supreme Court ruling, 1 peer-driven approaches to health promotion have been crucial to reaching men who have sex with men and increasing their access to sexual health services.
In Nairobi, a dynamic network of specialised clinics run by and for men who have sex with men has fostered new norms around health care seeking and utilisation and created protected spaces in which these highly stigmatised men are able to take ownership over the course of their sexual health destinies. However, the Kenyan Ministry of Health (MOH) has yet to officially recognise these peer health workers as essential workers during the COVID-19 epidemic. This leaves their work unsupported by the state in terms of being eligible to receive personal protection equipment (PPE) and access to much-needed training afforded to other health workers at this time.
Based on our short case study of the response of one community organisation known as Health Options for Young Men against STIs (HOYMAS), we argue for the importance of recognising the essential contribution that these organisations make with respect to maintaining sexual health service delivery – a vital contribution laid bare in the era of COVID-19. We refer to the experiences shared with our team during a series of ongoing virtual conversations with peer health workers and activists in HOYMAS, and highlight some of the challenges to which they have responded in light of COVID-19 measures and the continued need for sexual health services. In other words, we emphasise the critical role that community health infrastructures have come to assume in fighting two epidemics.
HOYMAS’ response to COVID-19
The government suddenly announced the lockdown of Nairobi in March 2020, when Kenya’s earliest cases were detected, affording people little time to prepare. Peer educators quickly adapted their roles towards sensitising their peers to the threat of COVID-19. Through various social media channels, especially WhatsApp groups, peer educators provided members with the chance to exchange questions and answers. Immediately, regular programme meetings at the HOYMAS office and drop-in centre were halted. These cancelled meetings included support groups for HIV positive men, the PrEP club, 2 the security and paralegal group, and regular peer navigator and data review sessions. Regular events (such as ‘Beauty Fridays’) aimed at mobilising large numbers of peers for support, education and connection to clinical services and programme activities were also suspended. Internal staff meetings soon migrated to virtual meetings, while peer navigators adjusted by shifting in-person outreach activities to mobile text messaging and cell phone calls. Based on the emergent psychosocial needs expressed by members, HOYMAS initially attempted to conduct a number of support groups at the drop-in centre. Each support group was limited to a maximum of six people and insisted on a 2-metre physical distancing rule, as recommended by the MOH (2020) guidelines. However, support group attendance began to wane when matatu (local transport) costs doubled after the government placed restrictions on the number of passengers they were permitted to transport. Through a rapid assessment conducted by the HOYMAS adherence counsellor, HOYMAS staff came up with the criteria for those requiring nutritional support, issuing gift vouchers to the members with the most vulnerable health conditions.
Soon after Nairobi’s lockdown, HOYMAS modified its drop-in centre hours from daily between 8 am and 5 pm to Wednesdays and Fridays only, from 10 am to 2 pm. Members were served by scheduled appointments only to ensure that the number of walk-ins could be kept low. COVID-19 infection prevention was placed at the centre of all programming, carefully following various recommendations developed by the MOH (2020) with respect to wearing masks, hand washing and disinfecting surfaces. HOYMAS also modified the drop-in centre by setting up handwashing stations, dispensing sanitisers, displaying COVID-19 information posters on the walls and establishing 2-metre distancing in the seating area of the waiting room. With the permission of their global funders, HOYMAS was able to reallocate a portion of their HIV funding towards providing masks to all staff members and peers visiting the drop-in centre, full body gowns for the clinician, and electronic thermometers for fever detection upon entering the clinic (see Figures 1–4).

Temperature monitoring by HOYMAS clinical staff.
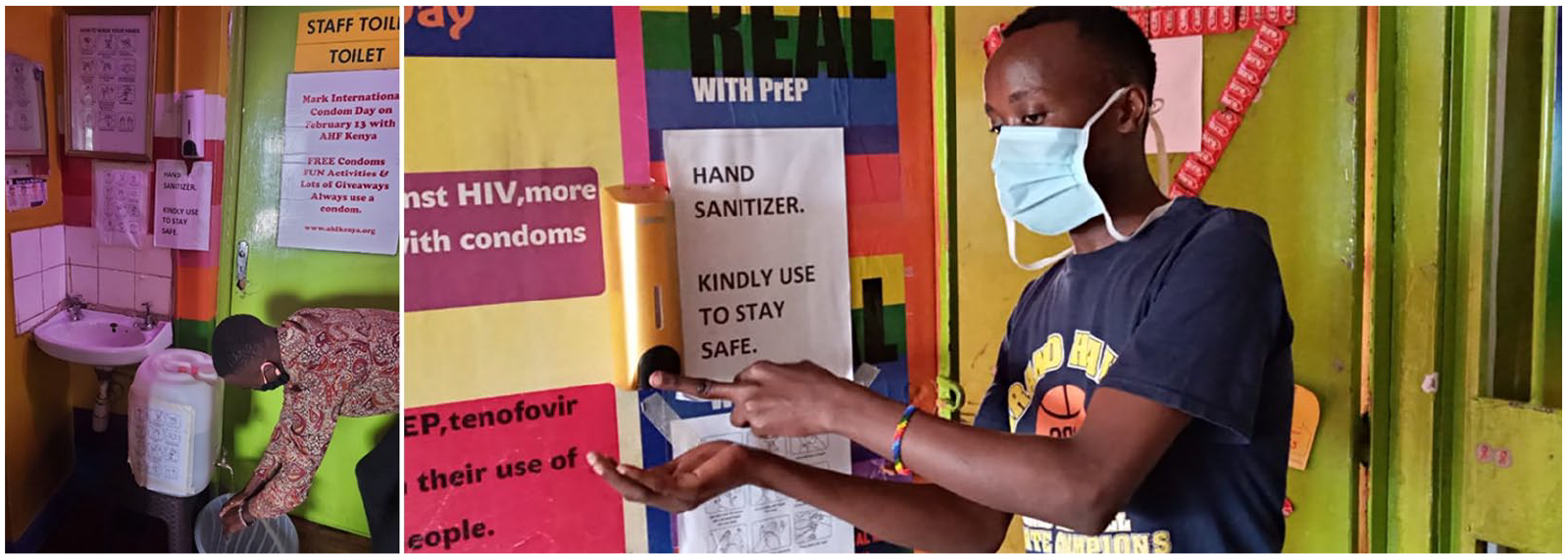
Hand washing and sanitisation stations set up in HOYMAS.

Sanitisers distributed by HOYMAS to members.
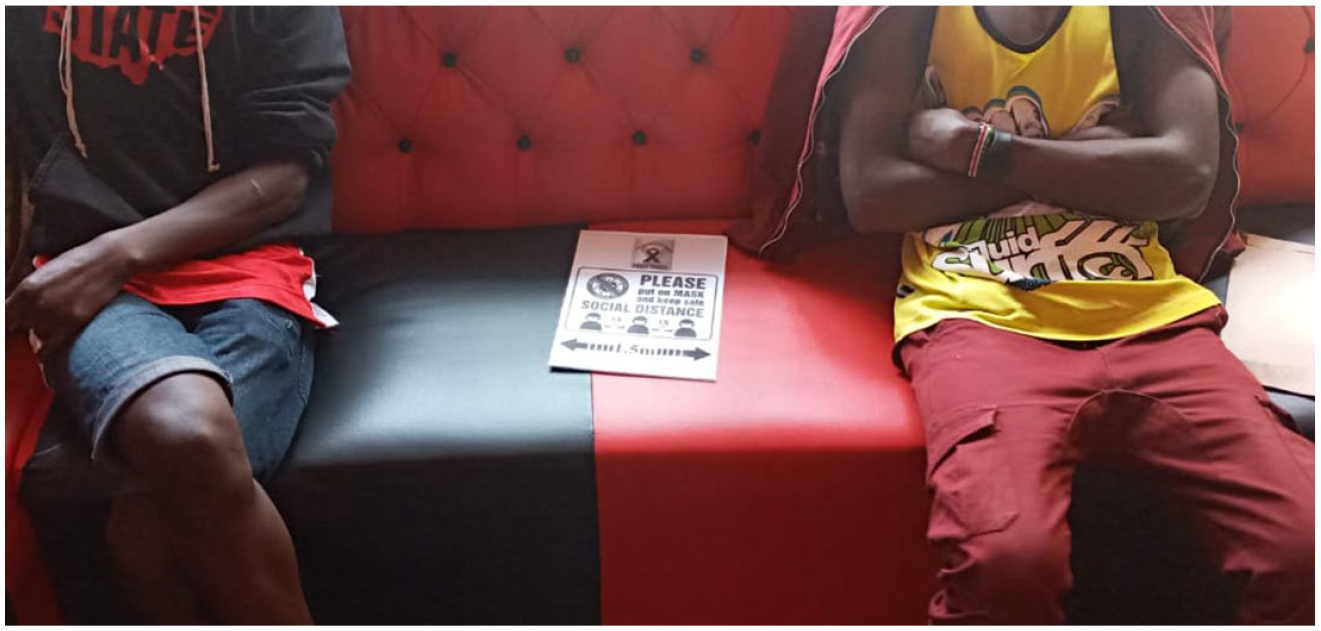
HOYMAS members physically distancing in waiting room area.
Impact on sexual health services delivery
Peer outreach and support
Prior to the government shutdown of non-essential businesses in Nairobi, HOYMAS peer health workers reached their peers in entertainment venues and cruising spots where men who have sex with men congregate to meet sexual partners and sell sex at night. HOYMAS geographically mapped these hotpots, periodically, with the assistance of technical partners, to conduct systematised outreach that allowed peer health workers to effectively distribute and track the disbursement of HIV prevention commodities, such as condoms and lubricant, and the number of contacts they linked to health services (Bhattacharjee et al., 2018b). This hotpot-based approach to outreach permitted the dissemination of educational materials, the notification of new programmes being offered and linkage of new peer contacts to sexual health services, including HIV testing, care and treatment. However, with government restriction on gatherings with nightly curfews, HOYMAS has been forced to reconsider how peer health workers can reach members. This has included the migration of outreach to virtual services for peer education, including WhatsApp groups, Facebook and other online forums. Given the financial problems facing men who sell sex in Nairobi in the era of COVID-19, however, challenges to the successful provision of health services quickly emerged. Many members of HOYMAS, as pay-as-you-go cell phone users, were unable to afford the air-time and Internet bandwidth necessary to connect to these platforms, and were unable to download the information, education and communication materials developed by the outreach team.
Clinical programmes
A number of community-led organisations in Nairobi run clinics, which offer specialised sexual health services to men who have sex with men. Prior to COVID-19, HOYMAS has provided regular testing, counselling and STI/HIV treatment for more than 5,000 members enrolled in their services. Over the last few years, HOYMAS has struggled to have their clinic officially recognised by the county government, which disqualifies the organisation from securing a greater number of full-time clinical staff, at the government’s cost, and in the era of COVID-19 excludes them from receiving PPE. Although permitted to reallocate some of their international HIV funding to a COVID-19 response, these resources were inadequate. For example, the Dutch funder Aidsfonds permitted HOYMAS to divert a portion of their outreach budget to purchase PPE; however, the organisation soon began to run out of these supplies.
Currently, HOYMAS continues to provide sexual health services while also striving to alleviate the burden of COVID-19. At the time of writing (August 2020), the organisation receives over 20 clients per day. Due to curfew, social distancing policies and requirements for PPE and crowd control, some clients have regrettably been turned away, given the presence of only one clinical officer on duty at a time. Staff have had to ensure that all members coming into their facility have masks and sanitisers as part of their basic prevention package. Although a large amount of staff time and effort is applied to hourly scheduling of clients, the temporal unpredictability tied to male sex work presents a persistent challenge when it comes to members being able to stick to set clinical appointment times.
For sex workers living with HIV, accessing clinical services in a time of COVID-19 is especially difficult. Medication delivery for those undergoing anti-retroviral therapy (ART) does not exist, and with rising transport costs coupled with fears of contracting the novel coronavirus (SARS-CoV-2), ART access is greatly inhibited among HOYMAS members. This considerable access gap also extends to other biomedical interventions that help to prevent HIV infection including pre-exposure prophylaxis (PrEP) and post-exposure prophylaxis (PEP). In addition, although approved for distribution free of charge within government clinics, a general shortage in HIV self-test kits in the country has meant that men who have sex with men (like other Kenyans) are unable to take advantage of an option that could allow them to get tested in their own private living spaces while being able to access cell phone–based counselling services.
Livelihood disruptions
Over 70% of male sex workers rely heavily on night hotspots to earn a living (National AIDS and STI Control Programme [NASCOP], 2012); however, this way of finding clients has ended with the closure of these public venues by order of the government. The lack of available nightclubs, brothels and hotspots has thus resulted in a gradual shift to online platforms to offer sexual services. Popular dating apps such as Grindr, Tinder, Telegram and lesser known hook-up chat rooms have expanded as virtual hotspots for male sex worker seeking clients during the time of COVID-19. The intense stigma of homosexuality in Kenya, however, has troubled the transition to online sex work, which has come to carry a number of risks. Blackmailing on the part of clientele has increased as more and more men utilise online platforms. For instance, when some male sex workers sold to clients short pornographic films in which they performed, attempts were made to extort money from the actors. Other male sex workers have been preyed upon by ‘producers’ who fail to pay the men for acting in pornographic films. The intense fear of public identity disclosure and lack of protection from any government systems cause male sex workers to be highly vulnerable to these work violations.
The pandemic has brought to light other challenges that especially affect young male sex workers. Many are now facing the possibility of homelessness. Before the rise of COVID-19, young men often formed shared living communities in order to escape discrimination by families and neighbours, to reduce rental costs, and to better facilitate access to clientele. With COVID-19-related restrictions in place, sex work within such safe spaces has been profoundly disrupted. Fear of police arrest, which has happened to female sex workers in Nairobi (Maundu, 2020), has led some men to return to unsafe environments, where discrimination and violence persist. This has dealt a major hit to their sense of self-determination and to their communal support, forcing some men to have to return to hiding their identities. Moreover, many individuals who previously depended on shared rent but who now live alone find themselves unable to afford the rent. Those with no income for rent, who can no longer stay with friends and who cannot go back to their family face impending homelessness.
Collapse in mental health and violence responses
Poor mental health outcomes related to depression, traumatic experiences, stigma and hazardous substance use have been well-documented among men who have sex with men in Kenya (Korhonen et al., 2018). In Nairobi, however, our team found that male sex workers who were affiliated with community-based organisations showed significantly higher levels of social support and quality of life compared to those unaffiliated with community-led organisations (Doshi et al., 2020). In the time of COVID-19, HOYMAS is seeing new increases in mental distress brought about by financial insecurity, impending homelessness, food insecurity and anxieties around the risk of contracting SARS-CoV-2 among immunocompromised members. Previous channels to accessing counselling and other mental health services are no longer available, and cell phone–based resources remain unaffordable to most members.
Those requiring crisis response for severe mental health problems face many challenges. HOYMAS’ rescue centre, staffed by trained paralegal workers (Bhattacharjee et al., 2018a), is no longer accessible due to COVID-19. Crisis response mechanisms have been crippled by mandatory curfews; lacking the status of an essential health worker, community paralegals can no longer move about at night to respond to violence. Men experiencing intimate partner and roommate violence, thus, have little recourse to the law, especially in the context of dealing with volatile police. Those living with substance dependency also have limited access to substance use support, for such resources have not been deemed as ‘essential’.
Conclusion
This report illustrates how a community-led organisation in Kenya confronts the new health crisis surrounding COVID-19 while also persisting in their efforts to deliver HIV services to their male sex workers. The many struggles encountered, amidst dwindling resources, underscore the vital work needed to meet the health needs of a marginalised group that remains largely excluded within the government health system. Indeed, access to ARV medications, regular sexual health check-ups, HIV prevention resources, counselling, social support and paralegal protection for more than 5,000 highly stigmatised men relies upon the dedicated labour of peer health workers. And in the era of COVID-19, the delivery of these sexual health services is in risk of collapse without government support and recognition.
The case of peer health workers simultaneously responding to two epidemics speaks to current parliamentary debates taking place in Kenya around the controversial Community Health Services Bill (Republic of Kenya, 2020) – rebuked by county governments because it advocates for the official recognition of ‘community health workers’ through stipends, expense coverage and training. The passing of this bill may be crucial to HOYMAS’ peer health workers claiming status as essential workers, 3 which would enable them to secure the necessary resources to sustain vital sexual health programmes and weather any future pandemics or other sudden national health crises.
This case study is also significant to the ongoing struggle HOYMAS faces in having its clinic officially recognised by the county government and resourced appropriately in terms of health provider staffing. Although serving a population of over 5,000 men who have sex with men, HOYMAS’ peer health workers – who include peer educators, community mobilisers, health care navigators and HIV testing counsellors – are ineligible for an essential services card 4 and therefore unable to receive PPE from the MOH. Through the NASCOP, however, the government of Kenya has helped HOYMAS advocate with external donors to permit the reallocation of their HIV funding towards the COVID-19 response.
This, however, presents two problems for sustained sexual health service delivery. First, the reallocation of funding from HIV to COVID-19 has left major gaps in HIV services. While the halting of hotspot-based outreach has freed up some of the budget to respond to COVID-19, the success of linking the community to vital HIV services (i.e. through support groups, counselling, ARV adherence support, etc.) nevertheless requires alternative virtual-based approaches that can only be effective if the costs are covered for the majority of members who are unable to afford Internet access. Second, although HOYMAS has been able to access some funding support to secure PPE for COVID-19 from their current and past international donors (e.g. Gilead, The Elton John Foundation, Linkages and Aidsfonds), these resources quickly began to dry up after the first month of the COVID-19 response. As we approach the sixth month of the COVID-19 pandemic, which in Kenya is projected to spike in mid- to late 2020, the sexual health of male sex workers in Nairobi is placed in jeopardy as the essential community-based infrastructure continues to crumble.