
Abstract
Background:
Developing sex and sexuality education programmes for adolescents has proved challenging in many parts of the world, especially in contexts where the importance of these programmes is not valued. In such settings, educating about sex and sexuality may also require dealing with detractors who are active in spreading misinformation.
Objective:
This article identifies contextual barriers encountered by those involved in developing the Échale Neurona programme in Mexico. Team members associated with the programme have been teaching about sex and sexuality in public secondary and high schools since 2016.
Methods and design:
Grounded theory approach using semi-structured interviews. Interviews took place with 10 participants including health promotion experts and programme officials. The main focus of the interviews was on the contextual limitations encountered when implementing sex and sexuality education workshops.
Results:
Findings reveal at least three types of barriers hindering the comprehensive sex and sexuality education developed by the programme: institutional, cultural and socio-educational barriers.
Conclusion:
Contextual barriers associated with family and school environments posed a significant challenge to implementation. Such barriers may facilitate or hinder sex and sexuality education programmes affecting the way young people develop their sex lives and live their sexuality.
Introduction
Recent data from Mexico presents a worrying picture concerning the sexual health of adolescents. Among members of the Organisation for Economic Cooperation and Development, Mexico ranks first in terms of the rate of teenage pregnancy, with 77 cases per 1000, according to the United Nations Children’s Emergency Fund for Childhood (UNICEF, 2018: 51). In 2016, there were an estimated 11,808 cases of birth among girls and adolescents aged 10 to 14 years, or 32 births daily. In the same year, the Consejo Nacional de Población (CONAPO) reported that 42.1% of births in Mexico were to mothers between 10 and 17 years of age’ (Secretaría de Salud, 2018, para. 3). Although these data may be recent, sexual health problems are not and have not been the subject of attention by national and local governments for a long time.
Colima 1 is a Mexican state in which the fertility rate for girls aged 12 and 14 years increased from 3.75 in 2010 to 4.34 in 2016 (Meneses and Ramírez, 2019). In 2015, it figured in the top 10 Mexican states with the highest rates of teenage pregnancy, an issue that continues to this day (CONAPO, 2017). In addition, Colima has also had an HIV/AIDS case rate above the national average for more than 7 years according to information from the Federal Secretariat of Health (Álvarez, 2019). In 2014, Colima registered 584 cases of sexually transmitted infection (STI) among adolescents aged 10 to 19 years. Of these, acute vulvovaginitis was the most frequent, followed by urogenital candidiasis and human papillomavirus infection (Secretaría de Juventud, 2016: 6). In Colima, age at first sexual intercourse has been reported to be 17.7 years (boys: 17.4, girls: 18.0), whereas the median age at first use of a contraceptive method for girls was 21.4, almost 4 years after sexual debut. Furthermore, although 99.6% of young people over 15 years of age know about at least one contraceptive method, ‘only 65% reported using one at first sexual experience’ (Secretaría de Juventud, 2016: 5).
To address these issues, the Échale Neurona programme was developed in 2016 to provide sex and sexuality education workshops in government schools. The programme is still active today. The term Échale Neurona means ‘add a neurone’, and the programme aims to encourage careful decision-making about sexuality. The work is coordinated by the Colima Secretariat of Youth in collaboration with the Secretariat of Health and Social Welfare and the Secretariat of Public Education. The education workshops developed focus on five topics: sex-gender relationships, STIs, correct condom use, contraceptive methods and violence. These five topics are covered in a 3-hour workshop. The programme aims to offer a comprehensive approach to sex education (Secretaría de Juventud, 2016), in line with international trends (Miedema, Le Mat, and Hague, 2020).
By the close of 2018, Échale Neurona had conducted workshops with more than 70,000 young people in school. Some had attended the workshops on more than one occasion. In an informal evaluation conducted with 384 young people who participated in the workshops, 97% considered Échale Neurona to be an effective programme. Among their responses, young people described how the programme ‘helped answer questions’, made them more aware and ‘feel more prepared’.
To enhance effectiveness, it is recommended that young people be actively involved in the design and implementation of sex and sexuality education programmes (Castillo Nuñez, Derluyn, and Valcke, 2018). According to Kang and Yun (2019: 10), ‘participating in multiple school health promotion programmes is related to a student’s comprehensive health’. Concurrently, several initiatives advocate for the mainstreaming of sex education in public schools (Martínez et al., 2012) and the need to understand ‘health promotion as an important element in improving the health of individuals and communities’ (Woodall and Freeman, 2020: 9).
Likewise, there is growing consensus about the importance of family with respect to sex education (Martin et al., 2018), specifically in relation to effectiveness (Ja and Tiffany, 2018). A focus not only on the biological aspects of sex and sexuality but also its psychological dimensions encourages the adoption of a human rights perspective (Miškolci et al., 2020). This may be difficult in a context such as Mexico where sex and sexuality education encounters many barriers, including cultural resistance and logistic challenges (Sani et al., 2018).
Against this background, this study aimed to identify some of the contextual barriers encountered by those involved in developing and implementing the Échale Neurona programme in public secondary and high schools in Colima, where there are contextual barriers sex and sexuality education work with young people in school. There is knowledge to be gained from identifying and understanding these barriers, and how to overcome them.
Method
The study was qualitative in nature with a focus on key behaviours, events and social discourses (Fernández, 2017). Grounded theory informed the data collection and analysis (Strauss and Corbin, 2002).
Participants, design and procedure
Data were collected by means of semi-structured interviews with health promoters and programme officials. Questions focused on the difficulties encountered in delivering the sex education workshops to teenagers. Seven health promoters with more than 1-year experience delivering the programme and three others who coordinated the programme participated. Interviews lasted approximately 30 minutes each and were audio recorded and transcribed.
Interviewees were between 23 and 31 years of age and had received training in psychology (6), social work (3) and nursing (1). Most had been employed in health promotion prior to participating in the Échale Neurona programme, working with young people on issues such as gender violence or sexuality, either in professional practice or in social services.
Participants’ accounts were coded in preparation for analysis (Gaete, 2014), with Atlas.ti 8 being used to assist with this. The software allowed us to identify topics and themes highlighted in participants’ responses. Codes and categories relating to these themes signalled the presence of one overarching category: ‘contextual barriers to successful implementation of the Échale Neurona sex education programme’. This central category comprised three contributory categories, each identifying a specific type of barrier: institutional, cultural and socio-educational. These three elements are derived from nine codes identifiable in health promoters’ accounts (Figure 1).
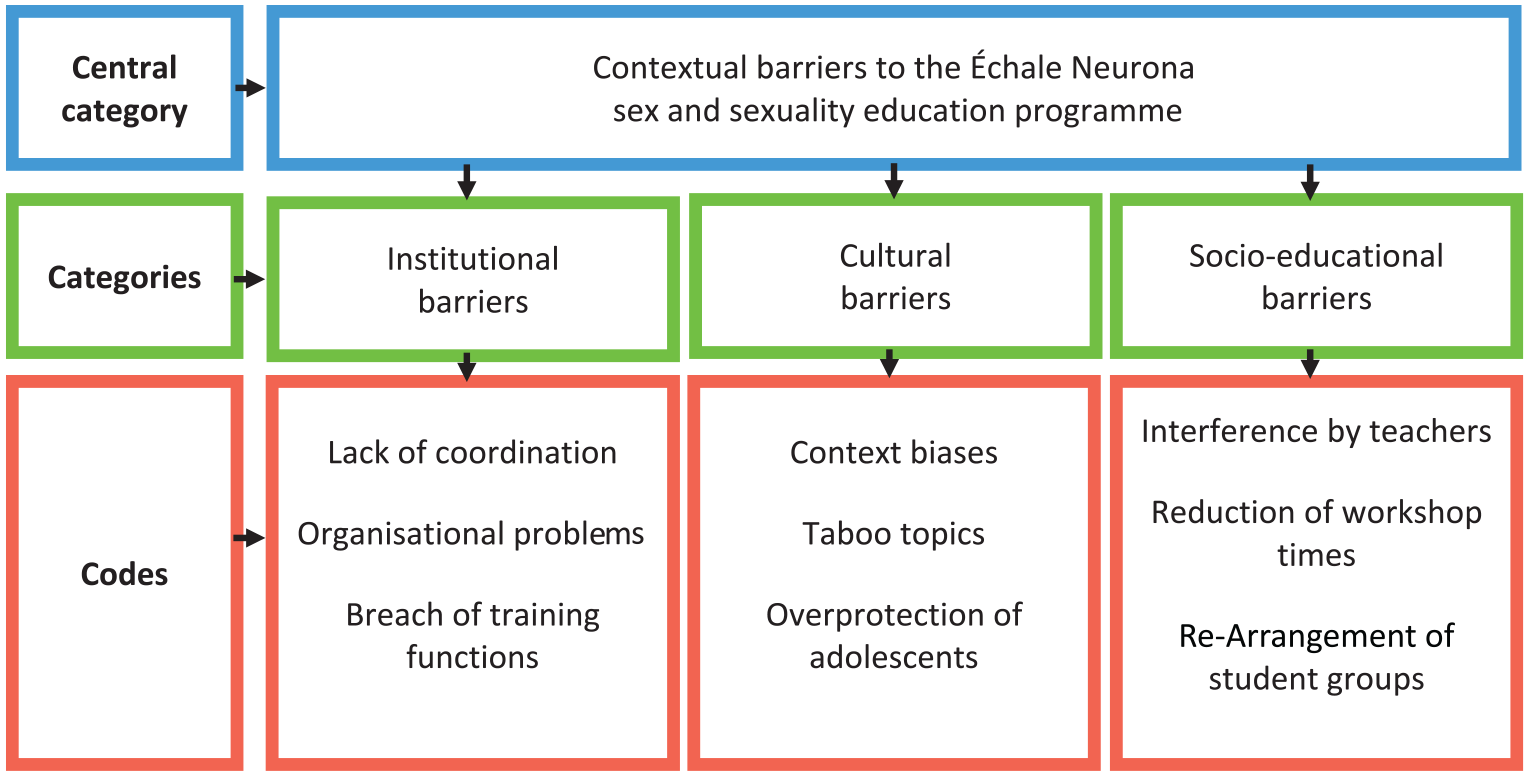
Contextual barriers encountered by the Échale Neurona programme.
Ethics approval
This study was approved by the Ethics Committee of the Faculty of Political and Social Sciences at the University of Colima, Mexico. Interviews took place with the informed consent of participants in the Échale Neurona programme. Data are reported using pseudonyms to ensure confidentiality.
Results
Three main types of contextual barriers hindered the sex and sexuality education work of the Échale Neurona programme.
Institutional barriers
Institutional barriers became evident in the first year of programme implementation, and arose from the two government institutions involved, the Secretariat of Health and Social Welfare and the Secretariat of Public Education. In both these institutions, there were failures of responsibility. One informant explained: The Secretariat of Health has not trained us again; they only provided [initial] training, but after that they never trained us again. Sometimes, in the Secretariat of Youth, there might be a course or training available, but nothing else is provided (promoter Ana, 2018).
In the Secretariat of Public Education, barriers were more closely linked to the failure to meet its responsibilities towards government schools.
. . . more logistic support would have been good because we sent a letter [to the Secretariat] detailing the programme when it started, and they responded. At that time, they supported the work and said, ‘Yes, that is okay, you can go ahead, we will send information out to supervisors so that they can forward it onto the addresses and the teachers’, but when we called the school principals, they did not know what we were talking about . . . So, I think there was a barrier there (health promoter Marlene, 2018).
These institutional barriers revealed poor communication between schools, the Secretariat of Youth and the Secretariat of Health and Social Welfare, which limited the overall effectiveness of the education provided by the programme.
I believe there were limitations regarding our relationship with the directors of the Secretariat of Education. For example, when we started in 2016, they helped us with the materials and scheduled the workshops for schools. So [at that time], there was no problem because the Secretariat of Education asked schools to run the workshop. However, currently we have to ask for permission ourselves and obtain all of the necessary signatures. We have to sort everything out ourselves (health promoter Inés, 2018).
Cultural barriers
In Colima, prejudices and taboos about sexuality in schools and within the family act as cultural barriers to sex education. One interviewee explained, ‘When we started the programme, I realised that sexuality in Mexico is still a taboo subject, and talking about it in Colima, which is a small very conservative state, is very difficult’ (health promoter Juan, 2018).
Échale Neurona workshops included teaching how to use a male condom. To demonstrate correct use, health promoters had to use a wooden model of a penis after some schools complained about the use of a latex anatomical model which looked too much like the real thing: ‘When we show [students] how to put on a condom, we used to use an anatomically correct model of a penis. But there were many institutions that objected saying: “No, do not use that”’ (health promoter Dionisio, 2018, personal communication). Crucially, the use of a wooden model prevented health promoters from demonstrating correctly, and the use of a misshapen model reinforced social taboos about viewing genitalia.
In general, there has been a lot of resistance to sex and sexuality education in Colima. Some teachers and school officials have spoken out against specific issues, even calling the work of Échale Neurona harmful to adolescents. In this regard, one interviewee said: This situation can improve if the Secretariat of Education trains its teachers to know and understand our work, [. . .] to understand that sex education does not only have to do with sex and penetration as many teachers think (health promoter Sarima, 2018).
However, resistance has decreased over time, and one of the achievements of the programme has been the sensitisation of teachers and administrators to its benefits.
[. . .] people are scared by the fact that we talk about masturbation, ejaculation and pornography although we do it in a very proper way. When they hear that we teach that content, they usually say: ‘No, no, not that’. There have been problems, but they tended to arise in the beginning. Right now, I have to say the programme has a certain kind of popularity and they [people in general] respect it more. They now tell us, ‘Oh yes, teach them, tell them’, but initially we encountered many more barriers (health promoter Dionisio 2018).
That said, school resistance has been a recurring theme in responses to Échale Neurona.
Once, we went into a school that we had tried to get into before, and the principal told me: ‘You come with a condom and say “look at this, nothing happens to you, do whatever you want”. At what point did we [actually] say that? To them, teaching teenagers how put on a condom people was the same as telling them ‘Do this, take it, you can do whatever you want’. Another time they told me, ‘You must not talk about abortion because it is a controversial issue’, so we have had problems with schools, struggling with teachers forbidding us to teach the kinds of things teenagers have a right to know about. However, we cannot do much to resist because we [too] are part of a government institution. A civil society organisation, on the other hand, could go in and talk to them openly about the issues [. . .] but for us it is not that simple, because we are seen as part of a government agency that ‘is teaching them those things’. This is what the parents may say afterwards (health promoter Aimara, 2018).
Importantly, most schools do not allow condoms to be distributed directly in programme workshops. After pressure from parents, they reached an agreement that Échale Neurona would leave condoms with the school administration and teachers would distribute them afterwards to those who needed them. Some of the problems derive from parents’ beliefs about childhood and youth.
Parents do not agree with the sex education workshops we do because they see them as a bad thing. Maybe they have religious beliefs or think that children are not old enough to learn about these things. They call them ‘children’, not adolescents (health promoter Marlene, 2018).
Socio-educational barriers
Socio-educational barriers to sex and sexuality education included teachers’ behaviour and the limited time made available by some schools for the implementation of activities. For example, in some schools it was usual for teachers to remain in the classroom during the workshop since they were required to be based there during working hours. One interviewee said the following: If the teacher is present, it is [like] they become another guest. Additionally, there are schools where the teachers are instructed to stay with us [. . .] to listen to what everybody is saying, which bothers the boys [in particular] because it is no longer the same; they no longer ask us things, and do not open up (health promoter Alicia, 2018).
It was also common for teachers not to know that teaching had been suspended to allow a workshop until the Échale Neurona health education team arrived at the school gates. Difficult-to-cancel events, such as examinations, may have been arranged. According to one interviewee, It can happen that when you get to the classroom, the teacher tells you: ‘I am sorry, but I cannot give up my class time because we are taking an exam’ [. . .]. I understand that it is not their fault, but the problem is that in the end, the students are the ones who lose [out] because they are no longer given the workshop, as they should. Not all of the information gets through (health promoter Camila, 2018).
On other occasions, the class teacher might allow the team to do their work but would stay with them in the classroom. Other teachers or school principals might drop by to contact students, collect homework or simply to enter the room (health promoter Ana, 2018).
When teachers stay in the classroom, they rarely not do so as spectators but intervene to bring order to the group or to give a good impression of the school. In addition, some may get involved in the organisation of activities, moving between subgroups, giving students ideas on how to solve a task, silencing some contributors or reminding them how much time they had left to complete a task (health promoter Maday, 2018).
To make best use of available time, health promoters adjusted activities to meet school requirements. Sometimes, this would lead to reduced workshop time.
The Échale Neurona programme has also needed to work with student groups already assigned by the school. Depending on the number of students and available space, some pre-existing groups may be joined together, making group dynamics difficult. Bringing together different groups in this way makes some young people shyer, as being in front of others they do not know may make them feel less confident. ‘We do not set up the groups. We only teach those that have already been assembled by the school’, said health promoter Alicia.
Discussion
The contextual barriers documented in this study illustrate how difficult sex and sexuality education for young people can be in places where conservative morals prevail (Secor-Turner et al., 2017). In Colima, cultural barriers and religiosity set limits on what can be achieved (Coss and Vázquez, 2018). In addition, as Zermeño et al. (2002: 31) have pointed out, ‘the social ecology of Colima does not favour freedom for young people, not even those who have committed themselves to a family life, let alone single people’. In this context, sex and sexuality education for young people may be both necessary and challenging.
Other research has identified similar barriers in other parts of Mexico. For example, Rojas et al. (2017: 25) have pointed out how ‘primary and basic level teachers are rarely well prepared to address sex education competently and confidentially’. This is likely due to the fact that such teachers have not received such education at school, or in their own homes. When ‘prejudice and religious morality is thrown [into the mix]’, it becomes impossible to educate about sexuality (Jesús-Reyes and González Almontes, 2017: 148).
Elsewhere in the Latin American context, similar issues arise. Paz (2018: 36), for example, has documented how in Ecuador sex education policies in schools may be rejected by ‘the people who implement, execute and receive’ them. Romero (2018: 74) has pointed out that in Argentina, teaching staff fears and prejudices often constitute ‘the main cultural barrier that make it difficult to approach sex education’. A study in Chile found obstacles including ‘not having appropriate teaching material, and refusal and lack of interest of other teachers to participate’ (González and Riquelme, 2018: 27). Together, these findings demonstrate similarities between the barriers encountered by the Échale Neurona programme and those in other Latin American contexts.
However, the fact that Échale Neurona is slowly gaining greater acceptance reflects value of the awareness-raising work undertaken with teachers and managers. In this regard, Uribe et al. (2016: 44) have argued that it is crucial ‘to develop competences in teachers, professionals, and parents [using] necessary information and materials [and] practical [. . . measures . . .] to generate change and social transformation’. Looking forward, Estrada et al. (2017: 556) have argued that ‘studying family and school support [and] considering the influence of the social environment [will] allow for a greater understanding of the acquisition of skills for preventive sexual behaviour’ from an early age.
Limitations
The main limitation of this study is derived from its scope, since it focused only on the implementation of a specific programme. Ideally, its results should be compared with those of other similar programmes across Mexico to identify more general trends when it comes to sex and sexuality education nationally. In addition, the study lacks young people’s own perspectives as beneficiaries of the programme. Future research should focus on identifying young people’s own views about sex and sexuality and what an ideal programme ought to include.
Conclusions
In this study, the analysis of data from interviews with health promoters allowed us to identify three types of contextual barrier to the provision of sex and sexuality education in public schools. Institutional barriers included difficulties of coordination between partner agencies resulting in a failure to support the training of health promoters. Cultural barriers are derived from the prejudices some families and teachers had towards sex and sexuality education in a context where the use of condoms or talk about abortion continue to be taboo subjects. This relates to families’ overprotection of young people with respect to sex and sexuality. Finally, socio-educational barriers restricted the time available, health promoters’ autonomy to carry out their work and the organisation of student groups. This made it hard to create a supportive educational environment in which adolescents and young people feel comfortable talking about their sexuality (Bengtsson and Bolander, 2020).
Ultimately, as Seiler-Ramadas et al. (2021) have argued, the effectiveness of sex and sexuality education is dependent on whether educators can adapt to what they provide to the needs of students and the conditions in which they work, even in societies with very traditional cultural patterns. The fact that young people live in a context that does not favour comprehensive education about sex and sexuality further justifies the value of educational work by Échale Neurona. Overcoming these barriers and continuing to educate openly and honestly about sex and sexuality will allow the programme to enrich the symbolic universe of both adolescents and older people. In turn, this will generate a better understanding of the social, sexual and gender factors influencing young people’s lives (Le Mat et al., 2019; Naezer et al., 2017; Ruthven, 2017). If we can negotiate the contextual barriers identified by this study and transform sex and sexuality education workshops into spaces for social change, there will more likely be a positive impact on rates of STIs and teenage pregnancy.
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study derives from the first author’s doctoral thesis, which was supported by a grant from the Consejo Nacional de Ciencia y Tecnología de México and Consejo Latinoamericano de Ciencias Sociales (784757, 2016–2020).