
Abstract
Objectives:
This manuscript describes the rationale and protocol for an on-line, school-based randomised controlled trial of Projecte d’Educació Postural a l’Escola (Postural Education in School Project’ (PEPE) which aims to prevent non-specific low back pain and promote healthy postural habits in children. The study will examine the effects of the intervention on back care knowledge, daily postural habits (DPH) and the correct use of backpacks.
Design:
Randomised controlled trial informed by self-determination theory (SDT) and the social-ecological model (SEM).
Setting:
A total of 880 students attending 10 primary schools (five experimental and five control) from different Majorcan cities will participate in this study.
Method:
The intervention (on-line 12-week intervention for class teachers, physical education teachers and families) will be conducted by the research staff; a control group will continue their routine activities. Physical fitness (PF) levels will be measured by a modified version of the ALPHA Fitness test battery for children while back care knowledge and other study variables will be measured by a self-reported on-line questionnaire at baseline and post-intervention. The primary outcomes will be PF, backpack weight, back care knowledge and DPH.
Conclusion:
Findings will provide a comprehensive understanding of the short-term effects of this school-based intervention on back care knowledge, DPH, the correct use of backpacks and PF levels in Majorcan children.
Introduction
Reducing the disease burden of unspecific low back pain (LBP) in children is of major public health relevance. Children with episodes of LBP tend to experience chronic back pain in adulthood, which is a major cause of sick leave and short-term disability in middle- and high-income countries. The Internet and mobile-based interventions have enabled the scaling up of preventive interventions worldwide. As an unintended consequence, however, individuals may depend less on knowledge and more on mass media cues to make judgements about the value of the messages conveyed, and current on-line resources fail to provide an overall prevention plan for back pain (Sniderman et al., 2017). The need for comprehensive on-line school-based programmes to prevent non-specific forms of LBP in children has been previously established (Bettany-Saltikov et al., 2019).
Non-specific LBP in children and adolescents
Non-specific or common LBP is defined as pain between the costal margins and the gluteal folds, usually accompanied by a painful limitation of motion and influenced by posture and movement, which may be associated with referred pain (Balagué et al., 2012; Calvo-Muñoz et al., 2018). When a condition is diagnosed as LBP, it is assumed that there are no underlying factors such as fractures, spondylitis, direct trauma or neoplastic-, infectious-, vascular-, metabolic- or endocrinologic-related processes that might have caused the pain. In many cases, it is impossible to identify an organic cause of the symptoms experienced (Deyo and Phillips, 1996).
LBP is one of the major health problem worldwide (Balagué et al., 2012; Steffens et al., 2016) and often begins during childhood. During adolescence, however, its prevalence is similar to that of adults (Michaleff et al., 2014). An episode of LBP during childhood is indicative of future LBP episodes (Diepenmaat et al., 2006), and the prevention of LBP among young people is central to addressing this problem. In adulthood, LBP accounts for considerable economic loss (Takura et al., 2015), and LBP or neck pain is the leading contributor to productivity loss (Wada et al., 2013). According to the EPISER study (Mendiola et al., 2002), the most frequent diagnoses reported by adult participants after a consultation for back pain were LBP (22.2%), osteoarthritis (15.6%) and scoliosis or mechanical conditions (7.1%). Prior to these diagnoses, the following were obtained from the participants: simple X-rays (33%), detailed history and exploration (27.9%), blood tests (9.4%), computed tomography (CT; (5.7%) and nuclear magnetic resonance (NMR) imagery (4.48%). Among the general population in Spain at least 1,800,000 radiological studies, 1,100,000 blood tests, 319,000 lumbar CT scans and 250,000 lumbar NMR imaging results were undertaken with patients with LBP in a recent 6 month study period (Mendiola et al., 2002).
Worldwide, the prevalence of LBP ranges from 7% to 63% (Limon et al., 2004). To date, the largest study on LBP in children recruited children from Majorca (Spain). It determined the prevalence of, and risk factors for, LBP in 16,357 children (Calvo-Muñoz et al., 2018). The results showed that between 13 and 15 years of age, 50.9% of boys and 69.3% of girls had suffered LBP at least once, and 21.0% of boys and 30.7% of girls had an episode of LBP that limited their daily activities.
Given the frequency of LBP and its long-term consequences, preventive efforts should be prioritised. Mapping the etiology or at least some of the risk indicators is a prerequisite for primary prevention. In children, the etiology of LBP is largely unknown and only a few risk factors have been identified (Skoffer and Foldspang, 2008). Variables such as gender (Siambanes et al., 2004), age, body mass index (Balagué et al., 1999), psychosocial factors (Korovessis et al., 1976), time spent sitting or watching television (Kopec and Sayre, 2005), physical fitness (Sheir-Neiss et al., 2003) and carrying of excessively heavy school backpacks (Kratěnová et al., 2007) have been identified as factors related to LBP, although the findings from some studies are contradictory.
Another important factor associated with back pain is physical activity. The relationship between the two is curvilinear in adolescents, with low and high levels of physical activity associated with an increased risk of back pain (Schwebel et al., 2009). Thus, one can hypothesise that LBP occurrence is dependent on the amount and intensity of physical activity. This hypothesis can inform LBP preventive measures since physical activity is amenable to behavioural intervention. Furthermore, physical training programmes in schools and during leisure activities can be adjusted to include activities that strengthen the back (Skoffer and Foldspang, 2008).
Schools are privileged settings for healthcare education interventions, considering that children spend much of their time with their peers in school (World Health Organisation, 2010). The specific types of physical exercise associated with back care education and assessment play a unifying role in the official school curriculum (Auvinen et al., 2008). Assessment instruments are needed to determine levels of knowledge about health and back care and their relationship with activity and exercise among students. Furthermore, considering the low level of specific knowledge on LBP among high school students, it is important to assess the level of knowledge that is considered a preventive factor or an indicator of LBP in students with or without LBP (Miñana-Signes and Monfort-Pañego, 2016).
The Projecte d’Educació Postural a l’Escola (PEPE) study framework
Intervention studies that included an assessment of general knowledge about back care have concluded that the inclusion of back care education in the curriculum is an effective way to improve the cognitive aspects of back care in schools (Cardon et al., 2002; Foltran et al., 2012).
The PEPE project aims to examine the effects of a multicomponent postural education intervention for teachers on improvement in the back health of school children. The intervention seeks to enhance back care knowledge, provide training in good postural habits and promote the correct use of backpacks.
Recent advances in the development of educational programmes provide a golden opportunity to further explore how LBP can be reduced by factors such as back care knowledge, physical activity and adoption of correct posture. However, further research should focus on testing hypotheses generated by implementing well-designed theory-informed randomised controlled trials.
Principal aim
To examine the effects of a 12-week postural educational multicomponent intervention on back health in school children.
Objectives
Objective 1: To study the effect of the intervention on daily postural habits in school children.
Objective 2: To study the effect of the intervention on the correct use of a backpack in school children.
Objective 3: To examine the effects of the intervention on LBP prevalence in school children at 9 months after the intervention.
Objective 4: To examine the effect of the intervention on back care knowledge, daily postural habits and LBP prevalence among teachers.
Methods
Study design
The study takes the form of an on-line school-based randomised controlled trial that will be conducted in Majorca. Majorca has a total population of 868,693 and 250 primary schools which children attend between the ages of 6 and 12 years.
Study population
The study population will include children aged 10–12 years, in the fifth and sixth grades. Previous studies have reported that the prevalence of non-specific LBP is very low among children younger than 7 years old (1%) (Taimela et al., 1997), whereas it is larger among children aged 13–15 years old (59.9% in boys and 69.3% in girls), according to data from a previously published Majorcan study (Calvo-Muñoz et al., 2018). These data suggest the need to address possible determinants of LBP early, in older primary school children.
The sample size calculation for an infinite population was used to obtain a theoretical sample of 1,067 participants, with a reliability level of 95% and predetermined sampling error of 3%. The study will be conducted in 10 randomly selected schools to reach a wholegiving a final sample of 1,100 participants.
Individual randomisation is not usually possible in intervention studies conducted in school settings as the natural school groups (classes) must be retained as organised by the school. The current study will, therefore take the form of a block-randomised controlled trial, in which groups instead of individuals will be randomised. The 10 schools will be randomised into the experimental (five schools) and control (five schools) groups. It is expected that a total of 150 teachers will be trained to carry out the intervention.
Permission from schools and parents of the participants will be required for participation in the study. The study protocol was approved by the local Ethical Committee at the University of Balearic Islands (nº, 130CER19) in accordance with the ethical standards in sport and exercise science research (Harriss et al., 2019).
Inclusion/exclusion criteria
Inclusion criteria
Children aged 10–12 years in the fifth and sixth grades of each school.
Exclusion criteria
Children with a medical condition that could affect the measurement results or with an ability limitation that could affect participation in the intervention programme.
Intervention
A 12-week intervention programme will be implemented comprising the following components (Figure 1).
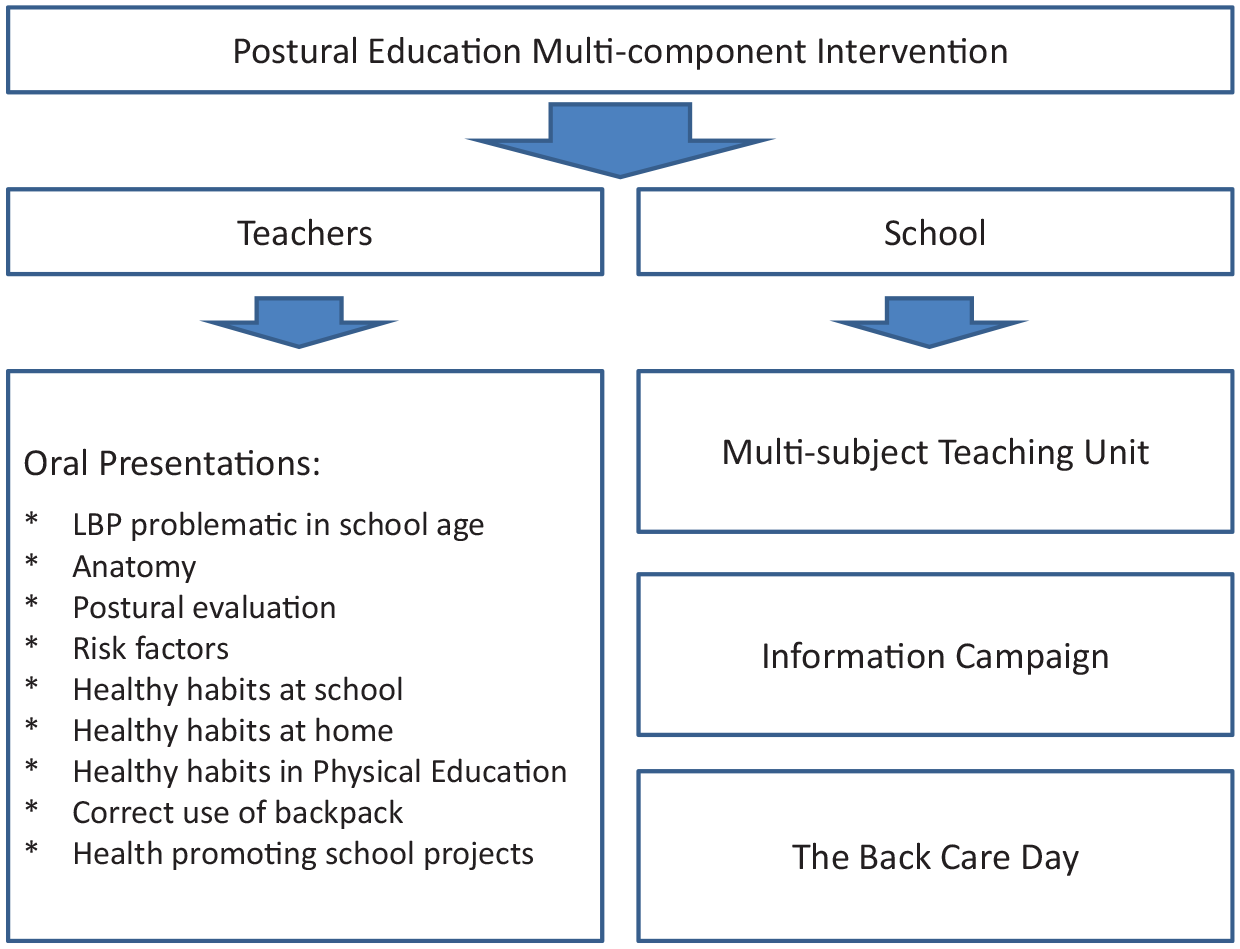
Flow chart for the PEPE study.
Nine oral presentations on subjects of relevance. The following topics will be addressed: scientific evidence concerning LBP, human anatomy and physiology, LBP risk factors, healthy physical exercise, ergonomics, postural hygiene, the correct use of schoolbags, healthy habits, back care recommendations for inclusion in Physical Education, and how to develop health promoting school projects.
Multi-subject teaching unit. A Postural Education Teaching Unit will be provided for teachers to build on and develop (as appropriate) within their subject areas. In physical education, sessions will consist of postural analysis; how to lift and carry objects correctly; carrying a backpack safely; balance, breathing and relaxation. In other subjects, the focus will be on the theoretical aspects of postural education.
Information information/awareness campaign to be implemented by the school (i.e. via posters, school website, social networks, etc.)
The Back Care Day at school. This will comprise a whole day’s activities with a focus on LBP. An information campaign will take place in school. During recess, games and activities will promote LBP prevention and healthy postural habits. These activities will be led by physical education teachers and volunteer teachers.
An information session will be organised for teachers and parents of participants to explain the procedures, aims and characteristics of the intervention programme in detail. Written information will be also provided to teachers and parents.
Participants will be assessed three times, prior to the intervention (baseline, month 0), after the intervention (post-test, month 3) and 6 months after the completion of the intervention (follow-up, month 9). Google forms will be used to administer on-line questionnaires to students in the classroom during regular school hours. The class teacher will read out the questions and answer any questions asked by students.
Measurement
This study will gather data using questionnaires and anthropometry, physical fitness assessments and backpack weight measurements. All measurements will be made at participants’ schools by trained research staff.
Outcome measures
Outcomes (both primary and secondary) will be assessed three times as follows.
Primary outcome – knowledge of back health
A validated questionnaire for Spanish children, Cronbach’s alpha (α = 0.82) will be used to determine the children’s level of knowledge on back care in daily physical activities (Monfort-Pañego et al., 2016). The questionnaire has 24 multiple choice items associated with the following:
topographical-anatomical knowledge (items 1, 2, 3 and 6);
functional–anatomical knowledge (items 4, 5 and 7);
habits in the standing posture (items 8–10), seated (items 11–13), or lying (items 23 and 24); and
habits in carrying heavy objects in a backpack (items 14–18); and how to move heavy loads (items 19–22).
In addition, a questionnaire that has been validated for Spanish school children and used in a study by Méndez and Gómez-Conesa (2001) will be used to assess back posture knowledge related to the general principles of good body mechanics and fear-avoiding beliefs.
Secondary outcome – daily postural habits
Daily life habits will be assessed using a questionnaire that will be answered by children at the three measurement points. The questionnaire (Palou et al., 2010; Vidal et al., 2013) includes the following items: being allowed to leave academic materials at school (yes = 1/no = 0), correct use of a sofa (yes/no), bending correctly (yes/no), taking care to sit correctly at home (yes/no), taking care to sit correctly at school (yes/no), frequent posture change on a chair at home (yes/no) and frequent posture change on a chair at school (yes/no). Each item will be coded as 0 = no and 1 = yes. A total score of daily postural habits score will be computed from the six items (range: 0 to 4): the higher the score the healthier the child’s daily postural habits.
Secondary outcome – backpack use
Correct use of backpack will be assessed using a questionnaire that will be answered by children at the three measurement points. The questionnaire (Palou et al., 2010; Vidal et al., 2013) includes the following items: try to load the minimum weight possible, carry the backpack on two shoulders, belief that a school backpack weight does not affect the back, and the use of a locker or something similar (for storage) at school. Each item will be coded as 0 = no and 1 = yes. A total score, namely healthy backpack use habit score, will be computed from the four items (range: 0 to 4); the higher the score the healthier the child’s backpack use habits. The weight of children’s backpacks will be also measured.
Secondary outcome – LBP prevalence
A validated questionnaire used in previous cross-sectional studies of school children in Mallorca (Palou et al., 2010; Real et al., 1999) will be used to evaluate LBP prevalence. The following data relevant to LBP will be assessed: LBP experience during the student’s lifetime (never, almost never, sometimes, often, always), LBP impeding usual activities (never, only when in pain, always), treatment received for LBP (no, rehabilitation, drugs, surgery, others), LBP in bed during the night or on waking (yes, no), LBP during the past week (yes, no), LBP during or at the end of a physical education (PE) class (never, almost never, sometimes, often, always), diagnosis of scoliosis and diagnosis of leg length discrepancy (yes, no).
Secondary outcome – back care knowledge
The LBP Knowledge Questionnaire will be used to assess the knowledge about back pain among teachers. The questionnaire is composed of 16 questions, divided into the following categories: general aspects, concepts and treatment. Possible scores range from 0 to 24 points, with a higher score denoting a better knowledge of LBP (Maciel et al., 2009).
Secondary outcome – LBP prevalence and daily postural habits
The Quebec Back Pain Disability Scale will be used to assess the daily postural habits of teachers (Davidson and Keating, 2002; Kopec and Sayre, 2005). The Quebec scale is a disease-specific measure of disability associated with LBP that has demonstrated good to excellent reliability and validity with young adult groups. The scale requests individuals to rate their level of difficulty performing 20 different daily activities. Scores range from 0 to 5 for each question, with lower scores indicating no difficulty at all and higher scores indicating inability to perform activities. The total score is the sum of the scores for each of the 20 questions and ranges from 0 to 100. This scale has also been used extensively with patients with LBP in randomised trials.
Secondary outcome – physical fitness
A modified version of the ALPHA Fitness test battery for children (Ruiz et al., 2011) will be used to measure core strength, aerobic capacity, flexibility, speed-agility and lower body explosive strength.
Secondary outcome – sociodemographic and anthropometric measures
Student and family questionnaires will be used to assess age, school grade and class, gender, high, weight, peak height velocity and sports participation. The student questionnaire will be based on work by Monfort-Pañego et al. (2016) and Palou et al. (2010). The family questionnaire will elicit parental sociodemographic data including socio-economic status, family income and parent education. It will be based on the Family Affluence Scale (FAS) questionnaire (Torsheim et al., 2016) (Table 1).
Variables of interest and instruments used to assess them, in line with the social-ecological model.

Data analysis
Only those participants who have completed data from three measurement points (baseline, post-test and follow-up) will be included in the analysis. The analysis will be conducted using PASW Predictive Analytics SoftWare (formerly SPSS, version 23.0; SPSS Inc., Chicago, IL, USA). Level of significance will be set at < 0.05 for all the analyses. One-way analysis of variance or Chi-square tests will be conducted, as appropriate, to assess group differences at baseline. To examine the effects of the intervention, we will use repeated measures analysis of co-variance, with baseline, post-test and follow-up results as dependent variables (in separate models), study group (experimental vs control) as a fixed factor and sex and age as covariates. A significant interaction between the groups and time from baseline to post-test will indicate an effect attributed to the intervention. Post hoc analyses will also be carried out to test whether significant changes occurred in the experimental and control groups between the different measurement points. For exploratory analysis, we will use a non-parametric test (Wilcoxon matched-pair signed-rank).
Discussion
The PEPE study will examine the effects of an on-line school-based non-specific LBP intervention on children’s back care knowledge, postural habits and backpack use. The effects of several possible mediators influencing the effects of this intervention will be examined informed by SDT and SEM frameworks. In addition, an evaluation of the intervention’s potential for public health impact will be conducted using the behavioural intervention techniques framework (Dobson, 1991).
The PEPE study has clear implications since school-based interventions of this kind with a focus on implementation as part of PE and classroom sessions in primary schools have been shown to lead to successful outcomes (Greiver et al., 2019). Because of the difficulty of implementing controlled trials in school settings and the overall low quality of the intervention designs used to date (Miñana-Signes and Monfort-Pañego, 2016; Miñana-Signes et al., 2021), only a few RCTs have been conducted. The design of this study is one of the major strengths, not least because it builds on relevant theoretical frameworks and incorporates the use of user-friendly materials. Both of these factors may contribute to the medium- and long-term sustainability and relevance of the intervention.
Several pragmatic adaptations pertaining to study design, implementation and evaluation have been made to conduct this research in a ‘real-world’ context. First, teachers will be able to choose participating class groups within the same grade, increasing their involvement in the intervention. Second, all primary schools will be included in the selection process and randomly selected schools will be invited to participate. That way, each school has the same likelihood of being selected. Third, the intervention includes on-line sessions delivered over a 1 month period. Fourth, the study and the assessments will take place over full trimesters to avoid possible effects due to holiday periods.
To summarise, conducting research in schools is important as a way of preventing unhealthy behaviours and related beliefs. Achieving a balance between the scientific requirements associated with randomised controlled designs and the constraints of real-world circumstances is necessary to improve the quality of research conducted in educational settings (Johnstone et al., 2017). Achieving a balance is also consistent with recent calls to align the requirements of evidence-based research more closely with contemporary practice in schools and other settings (Corder et al., 2020).
The intended outcomes for this study are to increase participants’ knowledge of back care, postural habits and backpack use to prevent future episodes of non-specific LBP. However, there is evidence that it may be difficult to change certain health behaviours though school-based interventions and the role of mediators is important. Previous reviews of school-based interventions for LBP prevention have noted the absence of mediators in statistical analyses (Miñana-Signes et al., 2021). In this study, an in-depth analysis of mediators will take place informed by SDT and SEM proportions. The effects of the intervention on these mediators as well as the possible effects of the mediators on the main outcomes will be analysed. The inclusion of an appropriate control group is crucial in order to assess the effects of the intervention.
Limitations
Despite these strengths, the PEPE study will have certain limitations. These include the relatively short duration of the intervention, lack of family involvement in it, uncertainties surrounding the sustained engagement of schools over time and the lack of an assessment of LBP prevention strategies used at baseline and progress post-intervention.
Conclusion
The PEPE study will evaluate a school-based intervention to promote non-specific LBP prevention. It aims to yield a comprehensive understanding of the effects on back care knowledge, postural habits, backpack use, child and parental perceived barriers to LBP prevention and peer social support .
The study will examine the mediator effect of variables such as back care knowledge of both students and teachers, daily healthy habits, backpack use and physical fitness on non-specific LBP prevention behaviours and overall physical fitness among children. Study findings have the potential to provide guidance for teachers, researchers and policy makers to implement effective interventions to promote LBP prevention and contribute more generally to healthier societies.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article. This work was supported by Grant RTI2018-101023-A-I00 funded by The Ministry of Science and Innovation (MCIN)/State Research Agency (AEI)/10.13039/501100011033 and by The European Regional Development Fund ‘A Way of Making Europe’ initiative.