
Abstract
Objectives:
Schools that have partnerships with health services have shown improvements in attendance and academic performance. This study examined the effects of intersectoral educational training (IET) between the health and education sectors on students’ learning outcomes, emotional experiences and subjective task values.
Design:
In this experimental field study, students in the control group were taught about health by a regular team of teachers, the experimental group was taught by a teacher–general practitioner team. Qualitative and quantitative data were collected at three different points of time.
Setting:
The study was conducted with students aged between 13 and 14 years in three classes at a secondary school in Baden-Wuerttemberg.
Methods:
Data were collected on demographic variables as well as learning outcomes assessed by a multiple choice test. For the assessment of emotional experiences, the validated Achievement Emotions Questionnaire was used and for subjective task values a modified Motivated Strategies for Learning Questionnaire was employed. Quantitatively, descriptive statistics were calculated and correlation analyses were conducted to explore the association of positive emotions and task value with knowledge after the intervention and follow-up.
Results:
Over time, 69 of 76 participants (91%) completed all three surveys. Both groups showed significant and sustainable knowledge increases, but there were no significant differences between the groups in knowledge increase, positive emotions and task values.
Conclusion:
Health education in public secondary schools seems useful for increasing students’ health knowledge both in the short- and longer-term. However, future research will need to examine the potential effects of IET approaches on students’ cognitive and motivational experience.
Keywords
Introduction
The risk factors associated with chronic diseases are largely preventable (Basner et al., 2015; Crowley et al., 2018; MacArthur et al., 2018; Rew et al., 2014), signalling the importance of health education and health promotion (Bay and Vickers, 2016; Deschesnes et al., 2003; Langford et al., 2015; Paffenbarger et al., 2001; Shih et al., 2016). Health behaviour can undergo significant change over the lifespan of an individual. Since most risk behaviours start in early adolescence, fostering good health knowledge from an early age is important (Kessler et al., 2010; Pinquart and Silbereisen, 2002; Poulton et al., 2002). One way of promoting health knowledge in children is via health education programmes in schools (Langford et al., 2015). The main benefit of school-based interventions is that a large and often heterogeneous cohort can be systematically educated with the goal of delivering education to those who need it most.
Growing realisation that the key drivers of health are socially determined has catalysed intersectoral collaboration between the health and education sectors to work to achieve health outcomes in settings other than clinical environments (Tooher et al., 2016). In consequence, schools are being viewed as suitable settings for intersectoral education focusing on issues such as mental health, nutrition, physical activity, drugs and alcohol, smoking, sex education and the prevention of sexually transmitted infections (Tooher et al., 2016). The Ottawa Charter among other health promotion initiatives stresses the importance of intersectoral collaboration for the promotion of health and the reduction of health inequalities (Van Dale et al., 2020). The term intersectoral education training (IET) had been used by Dubois et al. (2015) to describe a –. recognized relationship between a part or parts of the health sector with a part or parts of another sector that has been formed to take action on an issue to achieve health outcomes and intermediate health outcomes in a more effective, efficient, or sustainable way than could be achieved by the health sector acting alone.
In Baden-Wuerttemberg, Germany, annual health promotion days have been set up to help primary and secondary schools to implement programmes with a focus on issues such as alcohol drug dependency, violence prevention and health promotion. Many of these involve teachers and external partners working together. The regular curriculum is suspended for several days in favour of health promotion activities. As external partners, primary care professionals such as general practitioners have an important role to play in delivering health promotion and preventive care in local school-based settings (World Health Organization, 2018). GPs have a broad knowledge base concerning health issues and are often experts in health behaviour and disease prevention (Leeder et al., 2016). Involving them in the development of IET can ensure content-related accuracy and the topicality of the learning material.
School-based interventions for health can be effective in advancing health knowledge if they are designed properly. However, teaching quality is important (Renkl et al., 1996). High-quality teaching focusing on both cognitive and motivational issues is an important prerequisite of successful school-based interventions (Huber et al., 2015). Cognitive learning objectives are learning outcomes in form of knowledge and/or expertise. Motivational learning goals contribute to enhanced motivation during class, an interest in learning and favourable emotions towards a learning topic. Unfortunately, these two goals are not automatically in accordance with one another. Often, cognitive learning outcomes are realised but motivational outcomes are disadvantaged or vice versa (Stark et al., 1998). The students of teachers who manage to achieve both cognitive and motivational goals acquire more sustainable and more transferable knowledge and understanding (Seidel and Shavelson, 2007).
Studies have shown that a realisation of motivational learning goals leads to enhanced engagement with learning and deeper understanding (Rheinberg et al., 2000). Because positive emotions can facilitate the acquisition of knowledge (Pekrun et al., 2011), teachers should make an effort to promote students’ positive emotions during school-based health interventions. Within this context, achievement emotions may be defined as emotions related to achievement activities and their success and failure outcomes (Pekrun et al., 2011). In addition, a higher task value1 leads to higher interest, a stronger willingness to learn and better learning outcomes (Cole et al., 2008; Robbins et al., 2004) observed that subjective task value is an important predictor of the use of cognitive and metacognitive learning strategies and thus a good predictor of learning outcomes. Research also suggests that team teaching2 is a good way to facilitate the creation of a collaborative classroom environment (Anderson and Speck, 1998). It offers a collaborative model that not only lets students see how teachers can cooperate successfully, but also encourages students to become part of a shared process of learning, affecting students achievement emotions positively resulting in better learning outcomes (Anderson and Speck, 1998; Anwar et al., 2021; Hsieh, 2014).
Thus, school-based interventions aiming at fostering health knowledge generally seem to be successful if both cognitive and motivational learning goals are taken into consideration. For reasons of clarity, parameters like emotions and task value are here seen as ‘subjective dimensions’ in contrast to cognitive learning outcomes. The present study sought to examine the value of IET approaches in laying the foundations for this kind of outcome. It was assumed that the combination of a health expert and an education expert who share their expertise can create an intervention that is didactically well-designed and of good with respect to health content.
Hypotheses:
Both interventions (being taught by a regular team of teachers versus being taught by a teacher-general practitioner team) will foster students’ health knowledge, but more favourable effects will be found if teaching takes place by an interdisciplinary team of experts (GP and teacher) than by a team of school teachers alone.
Both interventions (being taught by a regular team of teachers versus being taught by a teacher-general practitioner team) will lead to knowledge increases in the long term but the retention rate from an intersectoral approach will be higher.
Knowledge taught by an interdisciplinary team of experts will lead to more positive emotions as well as a higher subjective task value.
The assessed subjective dimensions of teaching and learning (positive emotions and task value) are positively associated with the student’s health knowledge following an intervention.
Method
Sample
Participants in the study were 76 students (56.6% female) with a mean age of 13.37 years (SD = .49, range: 13–14) attending a regular, urban secondary school in the state of Baden-Wuerttemberg in Germany. The chosen intervention was implemented during the annual school health promotion days. In line with national and local policy, the school principal was asked for permission to conduct the investigation. Students and their parents were provided with written information about the study, and informed consent was obtained prior to data collection. The study was conducted in accordance with World Medical Association (WMA) Helsinki Declaration ethical principles for medical research involving human subjects, as revised in 2013.
Intervention design
The study took the form of an experimental field investigation. Students were randomly assigned to an experimental group (IET approach, n = 48) and a control group (traditional teaching approach, n = 28). The two groups were comparable in parameters such as age, gender distribution, personal relevance of health and perceived relevance of ‘prevention days’, as well as level of parents’ education and basic health knowledge at T1. Assessment of health knowledge, achievement emotions, motivation, cognitive and metacognitive processes was completed 1 week before the intervention (T1), immediately after the intervention (T2) and 8 weeks after the intervention (T3). From T1 to T3, seven participants (3 from the control group and 4 from the experimental group) dropped out of the study, meaning that 69 of former 76 participants (91%) completed all three surveys.
Both groups were taught about basic health issues such as physical activity, nutrition and stress for 90 minutes. A variety of instructional approaches were used, including direct instruction and activities such as physical exercise. In addition, moderated discussion between students focused on stress management. Learning goals include understanding the importance of physical activity, learning three different physical activities to activate the circulatory system, naming healthy foods, getting adequate sleep and developing a healthy circadian rhythm and becoming aware of bodily and psychological stress and applying strategies to calm down. Thus, the focus of both interventions was on knowledge, skills and specific practices. The provided content was identical for both the experimental and the control groups.
However, in the experimental group, the lesson was delivered by a team comprising a general practitioner (GP) and a teacher. In the control group, a team of two teachers delivered the lesson. To ensure similar teaching methods in both groups, all participating educators practised beforehand and all were advised to adhere to the given requirements.
Instruments
Cognitive learning outcomes like knowledge, understanding, judgement and problem-solving were assessed by an inventory of 18 multiple-choice questions with one correct answer and three distractor answers (e.g.: How many steps should you take in a day? (A: 100, B: 1000, C: 10 000, D: 50 000). A maximum of 18 points could be obtained in this test. This test was administered on three occasions (T1, T2 and T3).
To assess students’ achievement emotions (emotions experienced in achievement and academic settings) before, during and after learning, the Achievement Emotions Questionnaire (AEQ) was used (Pekrun et al., 2011). The instrument consists of 24 scales measuring emotions such as enjoyment, hope, pride, relief, anger, anxiety, shame, hopelessness and boredom using a 5-point Likert-type scale. The scales are organised into three parts assessing class-related, learning-related and test-related emotions. In total, the three AEQ questionnaires comprise 75-items (e.g.: ‘I am optimistic that I will be able to keep up with the material’.). The reliability of the scale has been shown to be good (AEQ 1: Cronbach’s alpha = .77, AEQ 2: Cronbach’s alpha = .91, AEQ 3: Cronbach’s alpha = .77).
To assess task value, Eccles et al.’s (1983) 12-item inventory with a 7-point Likert-type scale was used. Cronbach’s alpha was satisfactory for both times of measurement (T1: .65, T2: .76). The items were adapted from Stark et al. (2018), who combined the original six-item scale of the Motivated Strategies for Learning Questionnaire (Pintrich et al., 1991) with an additional six items derived from a study by Johnson and Sinatra (2013). According to Eccles and Wigfield (2002), the scale assesses (1) utility value (sample item: ‘… is useful to learn’.), (2) attainment value (sample item ‘… is personally highly important to learn’.), (3) intrinsic value (sample item: ‘… is very interesting’.) and (4) cost (sample item: ‘… is a waste of time’.).
Analytic strategies
To ensure there were no a-priori differences between the experimental group and the control group in factors such as age, gender distribution, personal relevance of health and perceived relevance of ‘prevention days’, as well as level of parents’ education and basic health knowledge, multiple t-tests were conducted.
A repeated-measures analysis of variance (ANOVA) was used to detect any increases in health knowledge following the intervention (T2). In addition, interaction effects were examined to assess whether students from medium and lower education levels profited more from the intervention than students from higher education levels. To examine whether the IET intervention produced more favourable results with respect to knowledge increase, a repeated-measures ANOVA was conducted and an interaction between group x time was expected. With respect to differences between T1, T2 and T3, a repeated-measures ANOVA was conducted to verify whether knowledge was higher for the experimental group at follow-up.
To analyse whether the IET fostered positive emotions during and after learning, an ANOVA was conducted, comparing the amount of positive emotions shown by both groups during and after learning, respectively. In addition, correlation analyses were performed to check for associations of positive emotions and task value with knowledge after the intervention and follow-up.
Results
The experimental and control groups did not differ in their health knowledge prior to the intervention, t(67) = -1.07, p = .287. Also, they did not differ concerning the amount of positive achievement emotions, t(76) = -0.86, p = .394; negative achievement emotions, t(76) = 0.16, p = .872; and their task value scores, t(75) = -1.02, p = .313.
Hypothesis 1: Both interventions will foster students’ health knowledge, but more favourable effects will be found if teaching takes place by an interdisciplinary team of experts (GP and teacher) than by a team of school teachers alone.
A repeated-measures ANOVA found that both interventions led to an increase in knowledge at T2, F(1, 67) = 127.90, p < .001, ŋ2 = .66. Both the experimental group (M = 15.39, SD = 1.44) and the control group (M = 14.13, SD = 1.89) had higher scores in the knowledge test after the intervention than before (experimental group: M = 11.50, SD = 2.29, control group: M = 10.88, SD = 2.32). There was no significant interaction between group and time, F(1, 76) = .94, p = .322, ŋ2 = .02. Thus, the first hypothesis was at least partly supported.
Hypothesis 2: Both interventions will lead to knowledge increases in the long term, but the retention rate from an intersectoral approach will be higher.
A repeated-measures ANOVA taking into account knowledge at all three measurement times showed that 8 weeks after the intervention, an increase in knowledge could still be seen in both groups compared to the initial measurement, F(1, 66) = 18.52, p < .001, ŋ2 = .22. Compared to the measurement immediately after the intervention, knowledge decreased significantly for both groups, F(1, 66) = 18.32, p < .001, ŋ2 = .22. However, the retention rate from an intersectoral approach was not higher than the retention rate from the traditional approach, F(1, 66) = .66, p = .419, ŋ2 = .01. Thus, both the traditional and the intersectoral programme led to sustainable learning outcomes but the retention rate in the intersectoral programme was not significantly higher than the one in the traditional programme. Therefore, hypothesis 2, was only partly supported. Relevant changes in health knowledge are displayed in Figure 1.
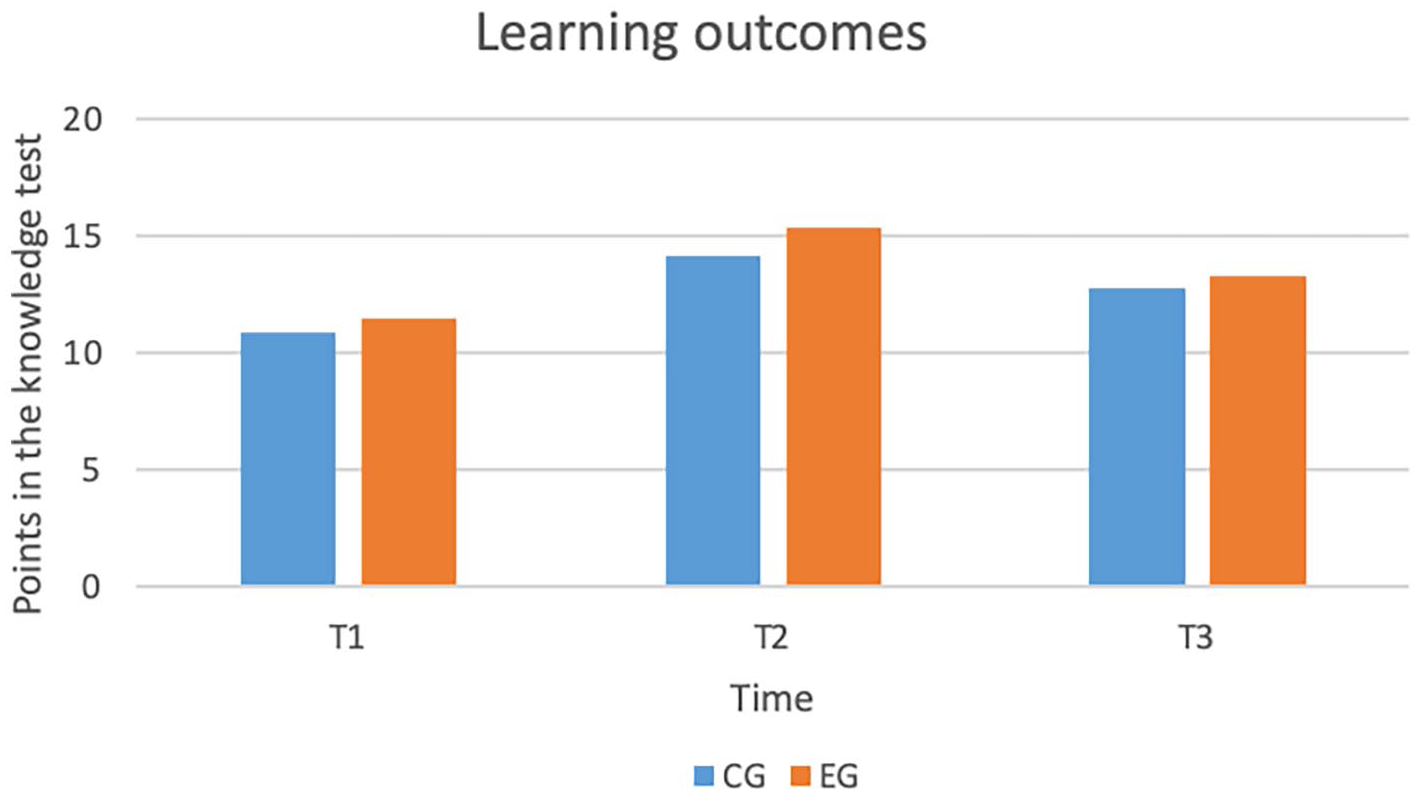
Knowledge test scores for the experimental and control groups at three measurement times.
Hypothesis 3: Knowledge taught by an interdisciplinary team of experts will lead to more positive emotions as well as a higher subjective task value.
The two groups did not differ in the amount of positive emotions expressed during learning, F(1, 75) = .10, p = .757, ŋ2 = .00. In the experimental group, students did not report more positive emotions (M = 3.16, SD = 0.64) than students in the control group (M = 3.21, SD = .55). Similarly, no significant differences were found in the amount of positive emotions after learning, F(1, 74) = 1.80, p = .184, ŋ2 = .02.
Students in the control group (M = 4.43, SD = 1.11) reported slightly lower task values than students in the experimental group (M = 4.50, SD = 1.17). However, this difference did not reach statistical significance, t(74) = .063, p = .950, ŋ2 < .001. Therefore, the third hypothesis could not be confirmed.
Hypothesis 4: The assessed subjective dimensions of teaching and learning (positive emotions and task value) will be positively associated with the student’s health knowledge following an intervention.
There were no significant positive associations between health knowledge after the intervention and positive emotions during learning (r = .13, p = .276), and task value (r = -.08, p = .508). Health knowledge at T3 was also not significantly associated with positive emotions after learning (r = .17, p = .149) and task value (r = .16, p = .183). Thus, the fourth hypothesis was also not confirmed.
Discussion
School-based interventions can enhance health knowledge as assumed in the first hypothesis. However, contrary to our second and third hypotheses, short- and long-term knowledge increase was not greater when the intervention was delivered by an interdisciplinary team of experts in comparison to a team of teachers only. There were also no significant differences in the amount of positive achievement emotions and task value as proposed in our fourth hypothesis.
One possible explanation for this may derive from the fact that both interventions were planned jointly by a GP and teachers in terms of content and didactics, and both interventions were implemented according to a detailed script. Similar teaching methods and content lessons may have led to comparable amounts of cognitive activation, similar styles of classroom management and a similarly supportive climate – resulting in no difference between the approaches. In future work, bringing medical expertise more fully into play (e.g. by providing selected firsthand case illustrations), abstaining from an elaborated script and increasing a focus on the consequences of problematic health behaviour may enhance the authenticity of the intervention, resulting in more substantial cognitive and motivational outcomes.
Intervention success may also be enhanced by tailoring content and topics more to the individual needs of each student concerning both health-related behaviours and knowledge. For instance, if a student already eats healthily and has a sound understanding of healthy eating, then he or she might be bored by the information presented and derive less benefit from the intervention. In such a case, it would make sense to provide information about other topics, such as exercise and sports.
In addition, previous research has shown that the retrieval of information leads to more enduring memories of that material (Roediger and Karpicke, 2006). To foster long-term increases in health knowledge, retrieval practice is necessary. Likewise, ongoing intervention in contrast to single-time interventions could further maximise the benefits.
Limitations
Like all research, this study had its limitations. First, additional participants would have increased the statistical power of the study. In addition, to be able to draw clear causal inferences, a ‘classical’, passive control group without any intervention should be integrated into the design. In addition, the nested structure of the data (the students in both groups were involved in other forms of learning together and may therefore have interacted with each other outside the intervention) should be taken into consideration at least statistically. In addition, the use of a common script to provide similar teaching methods in both groups, to enhance internal validity, may not only have reduced between-group-differences concerning intervention effects, and may also have reduce the ecological validity of the study. Therefore, future studies will be needed to show whether a more ecologically valid IET approach is more effective. Moreover in these studies, longer retention intervals of at least 3 months should be used to secure the sustainability of potential intervention effects.
Finally, the multiple-choice questionnaire used to assess knowledge increase was too easy for the students. Before the intervention, in both groups, approximately 61% of correct answers were given. Following the intervention (T2), 83% of the answers were correct. Thus, there was little potential for knowledge increase that could be reflected by the test. In future research, more complex forms of questioning (such as via open-response and transfer items3) could be used to assess students’ benefit from the interventions more broadly. Similarly, the inventories for the assessment of positive emotions and task value could be adjusted to an adolescent sample to improve their psychometric properties and reduce potential biases due to decreased motivation of the participants.
Conclusion
In this study, both the traditional as well as the IET approach were successful in fostering health knowledge, although no significant differences were found between the two groups, neither in terms of knowledge increase short- and longer-term, nor concerning positive emotions or task values. Future research will need to examine whether potential effects of the IET were undermined due to the experimental standardisation of the intervention and its implementation, or whether traditional approaches are as successful in fostering health knowledge as IET approaches combining the expertise of a GP and a teacher. Regardles of this, educational training to foster the growth of health knowledge should become a regular part of the curriculum in public schools.
Footnotes
Acknowledgements
We thank Joachim Boldt and Beate Simon for supporting the investigation at the Schubart Realschule Geislingen an der Steige in Baden-Wuerttemberg, Germany.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.