
Abstract
Background:
The growth of academic medical centres associated with international programmes has raised questions about the benefits and harms of medical experiences abroad for medical trainees and patients. Few studies explore the potential benefits to the institution or country that send these individuals.
Objective:
This pilot qualitative study explores the benefits medical professionals perceive they bring back to the USA from their global health experiences abroad.
Methods:
Medical staff who participated in University of North Carolina (UNC)–Project Malawi and who could meet for an in-person interview from October 2016 – March 2017 were recruited. Interviews were guided by an a priori semi-structured questionnaire. Each interview was transcribed and analysed by three reviewers.
Results:
A total of 8 out of 13 (62%) eligible potential respondents were interviewed. Participants perceived UNC-Project Malawi to benefit themselves, partnership institutions, and patients in Malawi, North Carolina, and throughout the world. After returning to UNC, participants recalled specific instances of increased diagnostic confidence (2/8) influenced by their experiences abroad. In addition, by partnering in research, participants felt that certain concepts were advanced including the syndromic management of symptomatic patients with sexually transmitted infections (1/8), the use of antiretroviral therapy to treat and prevent HIV transmission (2/8), and malaria vaccine development (1/8).
Conclusion:
Participants perceived that their global health experience either influenced their thought processes concerning the medical management of patients in the USA or resulted in a better understanding of research relevant to the global standard of care for specific diseases. International academic medical centre partnerships can offer rich settings for career skills development and a unique platform for collaborating on the management of clinical diseases that affect patients globally. These benefits can be maximised by establishing bi-directional curriculum goals and defining shared research agendas.
Keywords
Introduction
Academic medical centres (AMCs) in the USA are increasingly engaged in global medicine, and many AMCs have ongoing relationships with health centres abroad (Drain et al., 2009; Washington, 2019). As early as the 19th century, the larger community assumed that participation in global health care endeavours such as medical missionary work and Doctors Without Borders was humanitarian and charitable. However, in the past decade, the number of international AMC-associated programmes has increased, and this growth has raised questions about the benefits and harms of short-term medical experiences abroad (Harrison et al., 2016; Lu et al., 2018; Melby et al., 2016; Petrosoniak et al., 2010). Furthermore, in the context of current US economic market variability and financial debt, government support for such efforts without clear direct reciprocal benefit may limit the level of funding supporting these programmes (Kaiser Family Foundation, 2019). This pilot study aimed to explore the benefits to patient care perceived by medical professionals as a result of their international health experiences.
The majority of research from published systematic reviews, interviews, surveys, commentaries, and reflections primarily describe benefits or challenges medical trainees experience as healthcare providers abroad (Aziz et al., 2012; Campbell et al., 2010; Chetta et al., 2018; Elliott et al., 2012; Jacobs et al., 2002; Jeffrey et al., 2011; Lu et al., 2018; Ozgediz et al., 2005; Rodriguez et al., 2015; Sawatsky et al., 2010; Vu et al., 2014; Yao et al., 2016). Few studies have explored potential benefits to the participant’s host institution or country (Bido et al., 2015; Jones et al., 2013; Syed et al., 2012). Bido et al. (2015) reported that medical staff found their practice mentality in the USA changed to reflect greater awareness of different healthcare providers’ roles, teamwork, and resource costs, after an annual 1-week mission trip to the Dominican Republic. Syed et al.’s review identified 10 health system areas in which developed countries could learn from developing countries (Syed et al., 2012). A review by Jones et al. of whether health partnerships with organisations in lower income countries benefitted UK partners revealed seven domains of professional development benefits and five domains of associated costs (Jones et al., 2013). Both reviews concluded with a plea for more studies of academic rigour in reporting partnership benefits. Currently, there is a paucity of research addressing how medical experiences abroad may or may not benefit patients back in the USA.
This study was a pilot investigation into whether participation in global medicine at an AMC changed participants’ perspectives on the practice of their profession, regardless of where that practice takes place, and if it resulted in any perceived benefits to patient care back in the USA. Founded in 1990, the University of North Carolina (UNC)–Project Malawi hosts physicians, medical trainees, researchers and medical staff from UNC and other institutions for varying lengths of clinical involvement. Similar to previous studies, this study first aimed to understand how medical staff are involved in international medicine and explore how these experiences affected their career paths or professional development. A second aim was to assess whether their experiences resulted in any perceived benefits to their own approaches to patient care, which has been rarely reported in the literature (Busse et al., 2014). In the context of over a quarter century of partnership between UNC and Malawi, we hypothesise that there are bidirectional benefits of AMC global health collaborations that are likely underreported in the literature.
Methods
Following approval by the UNC Office of Human Research/Institutional Review Board (IRB #16-2421), eligible participants for this study were identified with assistance from the director of international operations for UNC-Project Malawi. This included a total of 13 previous and current UNC medical staff members who had participated in UNC-Project Malawi at Kamuzu Central Hospital (KCH) and could potentially meet for an in-person interview in either Malawi or North Carolina. Each candidate was contacted by email with an introduction to the research project and an enquiry for voluntary participation. A one-time follow-up email was sent to initial non-respondents. Volunteers who were willing to participate determined the time and location of the interview at their own convenience. At the time of the interview, respondents were provided with informed consent and given the choice to allow or refuse interview recording, future quotation and/or anonymity.
In-person interviews were conducted by one reviewer from October 2016 to March 2017 in either Malawi or North Carolina. A semi-structured survey was developed to guide the interview process. The interview consisted of two sections. The first section included background questions to understand the participant’s role and involvement in UNC-Project Malawi. This was then followed by approximately 10 open-ended reflection questions about the experience of providing medical care in Malawi compared to the USA, the perceived benefits of involvement abroad to medical practice back in the USA and the impact of the experience on the participant’s career development. The interviews were recorded on a password-protected Samsung Galaxy S6 Active. After the interview, the audio files were transferred to a password-protected laptop, saved to a password-protected hard drive, and deleted from the Samsung smartphone.
Each interview was transcribed, and a coding system was developed by the first reviewer to analyse both the closed- and open-ended responses. A second reviewer independently and blindly analysed the transcripts with the provided coding system. The data were then assessed for areas of consensus between the reviewers and tabulated. Variables that were discordant on the first two reviews were reconciled by a third expert reviewer, who moderated the first two reviewers’ disagreement and adjudicated a final assessment and categorisation. This report defines ‘count’ as the number of participants out of the eight that were interviewed. For example, a count of three means three out of the eight participants.
Results
Participants
A total of 8 out of 13 (62%) eligible healthcare providers involved with the UNC-Project Malawi global health experience agreed to be interviewed. Their occupations ranged from medical residents and research fellows to programme directors and board directors (Table 1). Two were interviewed in Malawi (October 2016–November 2016) and six were interviewed in North Carolina (December 2016–March 2017). Their length of involvement with UNC-Project Malawi ranged from 1.5 years to 24.6 years. During this time, half of the respondents had at some point stayed in Malawi for at least six consecutive months. Six of the eight (75%) providers had previous experience with providing medical care outside of the USA prior to participating in UNC-Project Malawi which included Asia, Mexico and the Caribbean, and other regions of Africa.
Participant characteristics.

Experience: observations and reflections
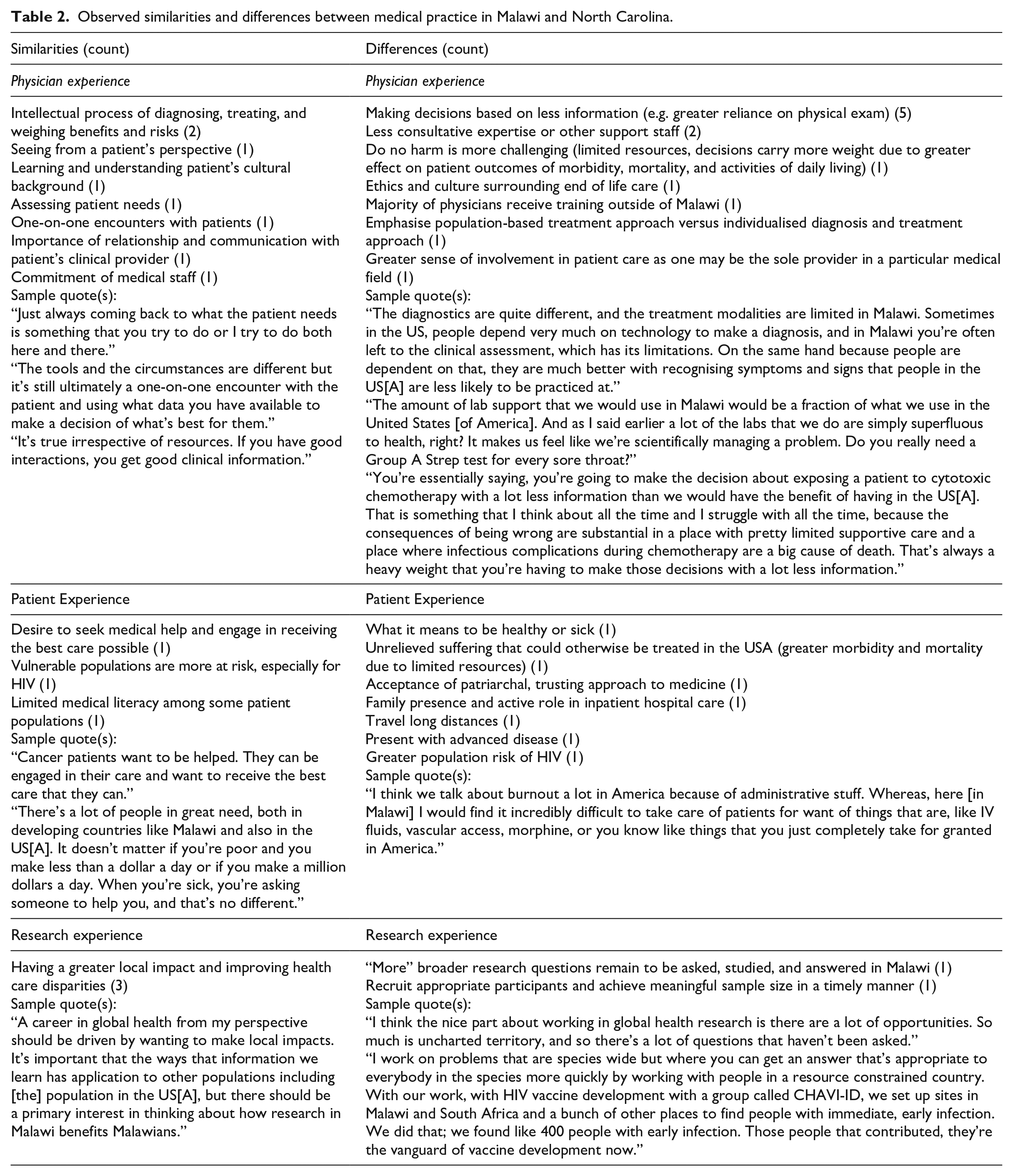
Given the diverse roles and responsibilities, the interview first sought to understand participants’ experiences abroad. The participants were asked to compare their experience as healthcare providers abroad with their US experiences. The most commonly perceived similarity between providing medical care in the USA and Malawi was the process of diagnosing and treating patients. The predominant perceived differences were making decisions in Malawi with a greater reliance on the physical exam given limitations of available laboratory and imaging tests as well as less available assistance from consultative experts or support staff. The most prevalent resource constraints mentioned by six out of eight participants were the limited medical equipment and materials available, such as laboratory tests, intravenous fluids for dehydration, and medications. Other resource limitations included food insecurity and medical wards/units needing expansion. One respondent commented that even with these resource limitations, the laboratory testing at KCH was advanced compared to that of the surrounding regions. Overall, participants perceived more differences than similarities. These are categorised into physician experience, patient experience and research experience in Table 2.
Observed similarities and differences between medical practice in Malawi and North Carolina.
Respondents were then asked to reflect on how the experiences abroad influenced their perspective as healthcare providers back in the USA. Having experienced the challenges of trying to provide the best health care possible with limited resources, several participants expressed gratitude for the plethora of material and human resources in the USA (3/8) and had an increased sense of privilege, fulfilment and appreciation of their role in providing health care upon returning to the USA (2/8). Other changes noted by participants upon returning to the USA included feeling humbled and inspired by interactions with Malawians, thinking twice about placing orders for diagnostic studies or therapies, noticing the patient more as a whole person, having a deepened sense that humans are similarly vulnerable when facing illness and seeking medical help, and contemplating the meaning of health care that is free at the point of access. Increased consideration about the need for orders included greater awareness of clinically meaningful tests or interventions rather than focusing on tests that were readily available or used for research.
Participants also said that the Malawi experience influenced them to consider combining care for patients and research (2/8), teaching (1/8) and expanding global involvement by being part of launching a new programme or a multicentre research project (1/8). These data suggest that experiences abroad heighten participants’ awareness of the resources in their work environment and makes them more attuned to their role as decision makers and care providers. This may in turn motivate medical practitioners to expand their involvement to also encompass other health care roles such as education, research and leadership upon returning to the USA.
Perceived benefits
Although this study assessed perceived benefits to the participants themselves, questions also focused on exploring the perceived benefits at the organisational, national and global levels. This interview also included attention to potential benefits for patients in the USA. The number of instances of different benefits mentioned by participants are tabulated (Figure 1). Respondents commented on gaining or improving personal skills in research (5/8), communication (4/8), teaching (4/8), supervising (3/8), clinical practice and diagnosis (3/8), and in regulatory and political affairs (5/8).

Perceived benefits as reported by participants.
The gains to the host institution included additional funding (2/8), building capacity and expertise (2/8), improving diagnosis and treatment (2/8), and creating opportunities for KCH to contribute to regional, national, and international conferences and journals (1/8). A research fellow said, ‘Hopefully what I’m doing in a very small way shifts the funding focus toward non-communicable and surgical diseases here and can maybe help people [patients] that I see every day because they’ll have more available’. The oncology programme director explained the importance of funding, We’ve helped put in some products that have gotten international attention and have allowed us to be internationally competitive for big NCI
1
grants. That ultimately brings resources to help develop people, help develop programmes, and help improve care. Those resources would not exist in Malawi otherwise.
Another research fellow said, ‘We’ve seen a pretty dramatic improvement in trauma associated mortality over the last 5 years, and we’ve been increasing the number of surgical providers at [KCH]’. However, these gains to KCH and Malawi are described from the perspective of the support being offered by the US partner institution and did not include the perceptions Malawians themselves may have had about the project.
By taking part in this collaboration, UNC received recognition by association, which helped it become known as a university with an Institute of Global Health (2/8). One physician said, ‘The growth of the programme in Malawi was a metaphor for how UNC became a global university’. This was separately confirmed by a resident’s comment, ‘I think that the fact that UNC has it is a huge advance and being able to emphasise that as a recruiting tool is also important for UNC as . . . an attractive place to come [for residency]’. These findings suggest that an institution gains recognition and a recruitment advantage from participating in global health.
Clinically, UNC-Project Malawi participants received exposure to the diagnosis and treatment of diseases that are rarely reported in the USA. This could help inform care in the USA (1/8), in particular the importance of minimising costs by ordering tests to answer clinically meaningful questions rather than to follow an algorithm (1/8). In addition, there was growth in confidence in diagnostic skills (1/8). A researcher in the HIV clinical unit provided the following examples: We’ve certainly learned about better treatments. How to treat tuberculosis in someone who has HIV. That informs how we treat people here [in the USA]. We could have never done the research here because there aren’t enough patients, and there are other examples. There’s this common cancer in HIV called Kaposi Sarcoma that occurs very commonly over there, so learning how treatment affects that cancer over there informs my care here.
A pathology fellow shared similar thoughts: I mean the sad reality is that there are huge numbers of patients with HIV who develop lymphoma in Malawi and we learn an enormous amount about HIV associated lymphoma from our work there and that absolutely benefits patients here.
With regard to ordering tests, a pathologist shared, I’m much more careful. I used to do things very algorithmically here [in the USA]. Now I’m like, well . . . or [I] just call [the clinician]. You ask the clinician if it makes any difference [to order a specific test] in this context and they usually say no.
These findings provide examples of instances where experiences abroad influence physician’s diagnostic and management approach to patient care back in the USA.
Remarkably, participants who had been part of UNC-Project Malawi since its inception highlighted several wider benefits. They reported that partnering in research meant that the concepts of syndromic management of symptomatic patients was initiated as early as during a first sexually transmitted disease clinic visit (1/8). In addition, they felt that the project helped promote antiretroviral therapy to treat and prevent HIV transmission (1/8), malaria vaccine development (1/8), and international collaboration to identify and develop HIV vaccines for early infected individuals (1/8). One of the previously mentioned directors explained that for ‘HIV vaccine development with a group called CHAVI-ID, we set up sites in Malawi and South Africa and a bunch of other places to find people with immediate, early infection’. These findings suggest that for some research questions, international collaboration may be a timely and effective method to achieve adequate scientific quality and generalisability.
Discussion
The outcomes of this study demonstrate both indirect and direct as well as short-term and long-term benefits to patient care in the USA as a result of healthcare providers participating in UNC-Project Malawi. From these eight interviews, we learned that participating in the project led to the development of new clinical skills and leadership capabilities, as well as greater appreciation and more conscientious use of resources available in the USA. This benefits patients in multiple ways. First, it may encourage returning physicians to be more critical when considering the standard diagnostic and management algorithms for patients they encounter. This can help to stimulate proactive discussion about the most appropriate workup for individual patients, rather than simply adhering to an algorithm. Second, returning physicians expressed interest in expanding their clinical roles and responsibilities beyond the clinical practice of medicine, such as participating in research and teaching. These other roles may contribute to the future development of patient care. This study also suggests direct benefits from global health research to patients back in the USA. Knowledge of the management of Kaposi sarcoma and HIV was acquired among partnership institutions over years of research at multiple global sites.
Some of the most important lessons learned by participants in this study involved the more judicious use of medical resources. On a national and international level, there has been increasing pressure in the USA and other high-income countries to avoid the overuse of unnecessary diagnostic testing. The Choosing Wisely initiative, for example, was developed by the American Board of Internal Medicine in 2012 with the intent of improving the utilisation of medical resources (Baird, 2019). This campaign seeks to develop recommendations to reduce the unnecessary use of specific medical services, especially those that are not truly necessary or supported by evidence.
Eliminating the overuse of unnecessary diagnostic testing, therapeutic procedures, and medication prescriptions may be difficult for a variety of reasons. The varying cultures of medicine at specific institutions as well as the policies of the hospital often play a significant role in decision-making by medical personnel (Chalmers et al., 2021). Maintaining patient satisfaction is also a significant driver of medical overuse (Mira et al., 2018). While the amount of control a physician has over some of these factors may be variable, having previous experience working with limited resources may play a significant role in improving an individual’s medical utilisation.
Similar to other studies, we found widespread agreement among participants on the need for improved cultural competence, commitment to service, and concern for global health (Aziz et al., 2012; Bido et al., 2015; Campbell et al., 2011; Elliott et al., 2012; Jafari et al., 2017; Jeffrey et al., 2011; Lu et al., 2018; Vu et al., 2014; Yao et al., 2016). Participants also shared similar views to healthcare providers in other studies who noted expanded medical knowledge and clinical reasoning capabilities, refined physical examination and procedural skills, increased consideration of cost-effective measures, more positive attitudes towards leadership, and improved growth in ACGME 2 core competencies (Aziz et al., 2012; Campbell et al., 2010; Chetta et al., 2018; Lu et al., 2018; Ozgediz et al., 2005; Pieczynski et al., 2013; Sawatsky et al., 2010; Yao et al., 2016).
Unlike previous published research, our study tabulated the instances and types of benefits that each participant perceived as having been gained from the experience abroad, but did not quantify the magnitude of the perceived benefits. However, a potential marker of productivity for UNC-Project Malawi is the number of publications. This is based on the premise that apart from an interest in global health, research collaboration draws and unites the participants in the programme. Interestingly, a search on Web of Science indicates 196 publications with 1068 associated citations and an h-index of 15 for UNC-Project Malawi investigators. This speaks to the magnitude of the work by attending physicians and directors on improving global patient care and less explicitly acknowledges the volume of contributions made by medical trainees and staff from both institutions. Assessing these collaborations and experiences may help institutions and programmes develop new curricula for individuals interested in learning through health care experiences abroad. Thus, our findings suggest that engaging in global health through an academic medical centre partnership with an international organisation can produce multiple effects. This includes achieving service to underserved populations, bi-directional education in medical knowledge and research methodology, deeper discussion of ethics and even potentially enabling ‘reverse innovation’ in patient care within developed countries (Cohen et al., 2012; Jones et al., 2013; Ozgediz et al., 2005).
‘Reverse innovation’ is a term used to describe the transfer of knowledge from low- and middle-income countries (LMIC) to individuals and institutions in high income countries. This is a fairly new area of investigation, but globalisation will likely lead to more international collaborations and ideas exchange (Kulasabanathan et al., 2017; Syed et al., 2012). Harris et al. (2017) showed that the majority of healthcare professionals and researchers implicitly associated good research with rich countries rather than poor countries. The syndromic management and early treatment of HIV as well as characterisation of rarer disease such as Kaposi sarcoma and multicentric Castleman disease mentioned in this study’s interviews exemplify, to the contrary, that good research can be performed in LMIC countries with appropriate resources and support. Shared efforts in problem-solving may improve the cost-effectiveness and timeliness of answering clinical questions by pooling resources and bolstering the sample size for global diseases.
Limitations
Like all research, this study had limitations. These included a small sample size and lack of exploration of the harms and costs of such an international partnership. To respect the time and other commitments of the medical professionals interviewed, conversations were brief, and did not explore other questions such as perceived harms, opportunity costs, and funding costs of participating in service work abroad. Identified challenges elsewhere in the literature include funding, safety, health risks, and quality and structure of rotations abroad (Lu et al., 2018; Melby et al., 2016; Rickard et al., 2018; Vu et al., 2014). In addition, the perceived benefits and harms to the host country’s participants were not assessed in this study. This lack of research limits understanding of whether costs outweigh benefits. Continued discussion to identify areas of improvement by both parties, minimise risks of harm, ensure bi-directional reciprocity, and address funding needs are encouraged (Binagwaho et al., 2013; Butler, 2016).
Future research
With respect to future research, it would be interesting to further assess the short- and long-term impacts of these medical experiences on healthcare providers with different backgrounds or in different stages of their career. The study participants were all in later stages of training or were established attending physicians. For pre-medical and medical students, an overseas medical experience may provide the first opportunity to see a different healthcare system and help trainees gain a better understanding of the disparities in global health. For established physicians, the experiences abroad expose them to new ways of practicing medicine and thinking critically about the best ways to utilise available resources. Finally, it would be worthwhile to assess the difference in perceptions between healthcare providers from different backgrounds. Physicians who grew up in underprivileged areas themselves may very well have a different view on medical resource utilisation compared to those who did not.
Conclusion
In summary, this study revealed how international collaboration can create a programme that develops the clinical and research skills of both North Carolinian and Malawian healthcare providers. With decades of partnership and collaboration, the medical knowledge gained from the UNC-Project Malawi programme not only had a local benefit of improving health care resources and medical staffing available to Malawians, but also contributed to the transformation of UNC into an institution for global health. These are examples from one academic programme, and more studies are needed to better characterise what developed countries learn from reverse innovations.
Footnotes
Acknowledgements
We thank Thomas Egan for expressing interest in understanding more about how trainee experiences abroad influenced patient care in the USA. We would also like to thank Teresa Edwards at the Odum Institute for improving the semi-structured interview questionnaire. This project was made possible through a Perkins-Burke MD/MPH Global Health Fellowship. Thank you to participants for sharing your time and experiences.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.