
Abstract
Objectives:
Adolescence is a critical phase of life, involving both risks and opportunities. Preventive health services in this phase contribute to the development of adolescents’ models for adulthood. The current study aimed to illuminate adolescents’ experiences regarding health education through a patient visit in a hospital, which provides a more informal learning environment than classroom instruction.
Design:
Qualitative one group experimental design.
Setting:
Participants were 16 high school students of a medium-level socio-economic status in Turkey, some of whom smoked cigarettes.
Method:
We visited patients in the pulmonology inpatient unit with the students. Data were collected through interviews, video recordings and field notes. Data were analyses using content analysis in which coding schemes are developed directly from the textual data to focus in on students’ health beliefs.
Results:
Findings revealed that the students who interacted face-to-face with patients and listened to their reflections on their illness and life experienced changes in their health beliefs. The visit provided moral support for the patients as well.
Conclusion:
Results indicate that such hospital patient visits offer significant opportunities for health education.
Introduction
Engaging in preventive health measures and staying healthy are critical to individuals’ well-being and long-term outcomes. Factors such as increasing healthcare costs, improved research and control over disease, and heightened awareness of the significance of health outcomes and quality of life, all contribute to the development of this perspective (Geckil et al., 2004; Gözüm and Çapık, 2014). Adolescence is a critical phase of life for the acquisition of behaviours for maintaining and promoting health (Sawyer et al., 2012).
Adolescence, covering ages from 10 to 19, can be a risky period in life, with young people experiencing disease, injury and even death to a worrying extent (World Health Organization, 2020). However, significant diseases or death are largely preventable at this time in life because they arise due to behavioural, social and environmental factors. Moreover, behaviours or dependencies that can negatively affect health are acquired in this phase, which may lead to future chronic disease. Therefore, preventive actions to reduce unhealthy or risky behaviours among members of this age group have gained importance (Özdemir, 2019). A study in the USA revealed that 9 out of 10 adult tobacco users started smoking by age 18, with 99% of them starting by age 26 (Centers for Disease Control and Prevention, 2019). A similar study on alcohol use reported that 47% of young Europeans start using alcohol by age 13 (Kraus and Nociar, 2016). However, a study in Australia noted an increase in the average ages of starting smoking, drinking alcohol and using drugs between 2001 and 2019 (Australian Institute of Health and Welfare, 2020) demonstrating that preventive health education and treatment can deliver promising results.
Various models have been developed to theorise the development, adoption and practice of health behaviours. One such model, the health belief model (HBM), focuses on the association between beliefs and behaviours. This model posits that individuals’ beliefs, values and attitudes affect their health behaviours (Gözüm and Çapık, 2014). The HBM includes the basic concepts of perceived severity, perceived susceptibility, perceived threat and perceived barriers, in order to predict why people may take action to prevent, test for or control disease (Champion and Skinner, 2008; Hobbs, 1977). Rosenstock et al. (1988) argue that motivation to take action regarding one’s health depends on two factors: the belief that one might experience a severe health problem (perceived threat) and the idea that one might benefit from acting in accordance with health advice (perceived benefit). As a cognitive model for understanding health risk behaviour, HBM has formed a basis for numerous prevention-focused interventions and research in areas such as smoking, substance abuse, obesity, sexual risk-taking and HIV (Downing-Matibag and Geisinger, 2009).
Encouraging young people to adopt healthy behaviours, one of the main functions of health education, can be realised through formal education. However, such learning can also occur through informal education as part of daily life. While informal learning is the sum of activities during the time when individuals are not in the classroom in the presence of a teacher (Gerber et al., 2001), out-of-school learning involves all the learning that takes place outside of the school environment (Tal and Morag, 2009). Informal learning settings encourage student learning to a greater extent than more formal environments. In informal settings, students can acquire understanding in line with their preferred learning style, absorb information at their own pace and devote more time to a particular interest area (Melber and Abraham, 1999). Out-of-school learning that supports school curriculum can be of various types (Fägerstam, 2014), and hospitals are one important informal learning environment for young people. In this study, we organised student visits to patients in hospitals to support the formal health education they received in school and interpreted the results of these practices using the components of the HBM.
Methods
Research design
The study employed a qualitative experimental design. As an exploratory and heuristic kind of experimentation, the study sought to intervene scientifically on an important social issue (Kleining, 1986, as cited in Ravasio et al., 2004). The study sought to understand hospital visits as a social and educational process and focused on the opportunities presented by such visits as an alternative form of health education.
Participants
Study participants were selected by convenience sampling (Lune and Berg, 2017) and comprised 16 high school students – 11 girls and 5 boys – from Kocaeli province in Turkey. At the time of data collection, participants attended a medium-level socio-economic status high school, where the school managers indicated that the percentage of students who smoked was relatively high. This study was conducted prior to the COVID-19 pandemic.
Data collection
The key steps undertaken in data analysis were as follows (see also Table 1).
Steps in data collection.
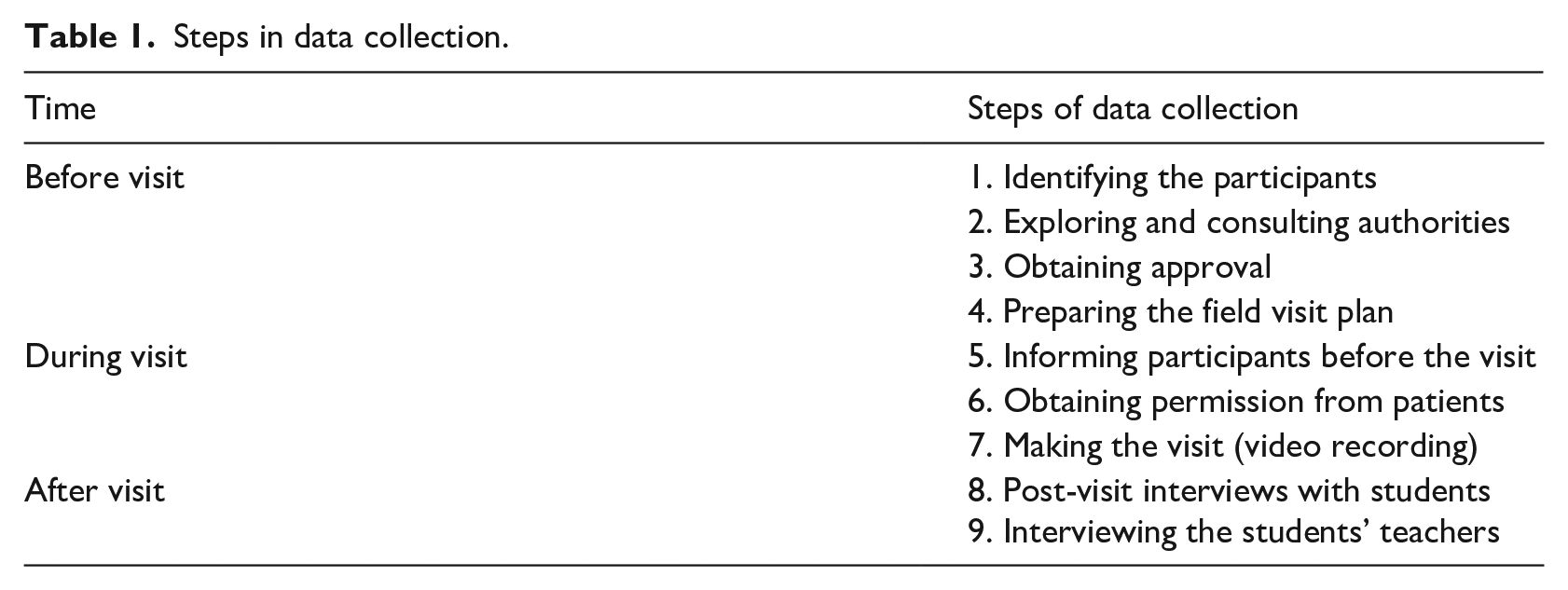
Step 1: The process of identifying research participants is described above.
Step 2: After identifying participants, we identified the hospital to visit. We chose the hospital that was located closest to the school. Before selecting the hospital, one of the researchers (H.B.) visited the hospital for observation. During the observation, he conducted interviews with staff members and informed them about the aim and process of the study. Since the hospital visit would take place in an environment with vulnerable people, care would be taken to respect privacy, minimise disruption and prevent any setbacks during the visit.
Step 3: Approval for the hospital visit was obtained from the school administration. The school then contacted the hospital to request permission for the visit. We also obtained permission from the high school students’ parents during this phase.
Step 4: We planned the field visit informed by the pre-practice observations in the hospital. We shared our plan with the school and hospital administrations to solicit their opinions and finalised the field visit plan based on their feedback.
Step 5: We informed participants about the planned activities before visiting to the hospital. We prepared questions for the participants to ask patients about and reminded them of hospital and hygiene rules.
Step 6: After informing participants about the activities, we paid the visit to the hospital. We visited patients in the pulmonology polyclinic inpatient unit. We selected the pulmonology polyclinic because many of those patients were receiving treatment for diseases linked to smoking, alcohol consumption and malnutrition. This was a deliberate choice to target students’ potentially risky health behaviours. We selected the specific patients to visit with the help of the unit staff. We obtained permission from both patients and their hospital staffs before the students entered their rooms.
Step 7: The hospital staff, students’ teachers and an assistant for video recording accompanied the students during the visits. Students visited the patients both individually and in groups, and the patients and their attendants were generally pleased with the results. Some of the conversations between the students and patients were recorded with a video camera. The patients and their unit staff gave their consent for video recording, and were assured we would not share the recordings with third parties. In addition, one of the researchers (H.B.) took field notes. Patients often gave students advice during the visits, and many of the students were intensely affected by the patients’ condition and the stories they had to tell.
Step 8: Following the visits, we interviewed students after they had returned to school. In these interviews, we aimed to explore the students’ experiences during the visit and their opinions about the experience.
Step 9: We conducted semi-structured interviews with the students’ teachers 3 weeks after the visits to understand whether the experience had had a lasting effect on the students. One of the researchers (H.B.) prepared notes following the interviews.
Data analysis and rigour
Data analysis started with a process whereby the interviews, observations and field notes were transcribed into text (Bogdan and Biklen, 2007; Kowal and O’Connell, 2014). After this, we analysed the data using content analysis. We utilised a conventional content analytic approach in which a coding scheme was developed directly from the textual data (Hsieh and Shannon, 2005). The four data analysis steps described by Green et al. (2007) were followed: data immersion, coding, creating categories and identification of themes. Details of these steps are provided below.
Data immersion
This involved reading and re-reading interview transcripts and contextual data and listening to the interview recordings (Hsieh and Shannon, 2005; Hunter et al., 2002). The researcher (H.B.) who observed the visits and conducted the interviews performed this step to ensure the integrity of data-context relationship.
Coding
This involved clustering the data into small segments to create units of meaning (Merriam and Tisdell, 2015; Miles and Huberman, 1994; Thornberg and Charmaz, 2014). We coded both the interview data and the video transcript. Then, we arranged these codes in tables to give us the chance to view the codes holistically.
Creating categories
Creating categories was both highly intuitive and systematic (Merriam and Tisdell, 2015). First, we read all the codes carefully. Then, we combined the codes we identified during the reading process to create four meaningful categories.
Identification of themes
A theme is more than a category. We created a single theme in this study by considering the relationship between the four categories initially identified.
Rigour
To ensure rigour in the research, we utilised a number of strategies throughout the study as recommended by Morse et al. (2002). These included data triangulation by interviewing student participants both before and after the hospital visits, video recording students’ conversations with patients, and taking field notes. The codes extracted by one of the researchers (H.B.) were carefully checked by other researchers to ensure the validity of the analysis. Finally, we provide direct quotations wherever possible in the write-up of this study, so as to present participants’ experiences in their own words. We used pseudonyms when giving direct quotes.
Findings
We classified the findings obtained during and after the visit into four themes, as shown in Figure 1.
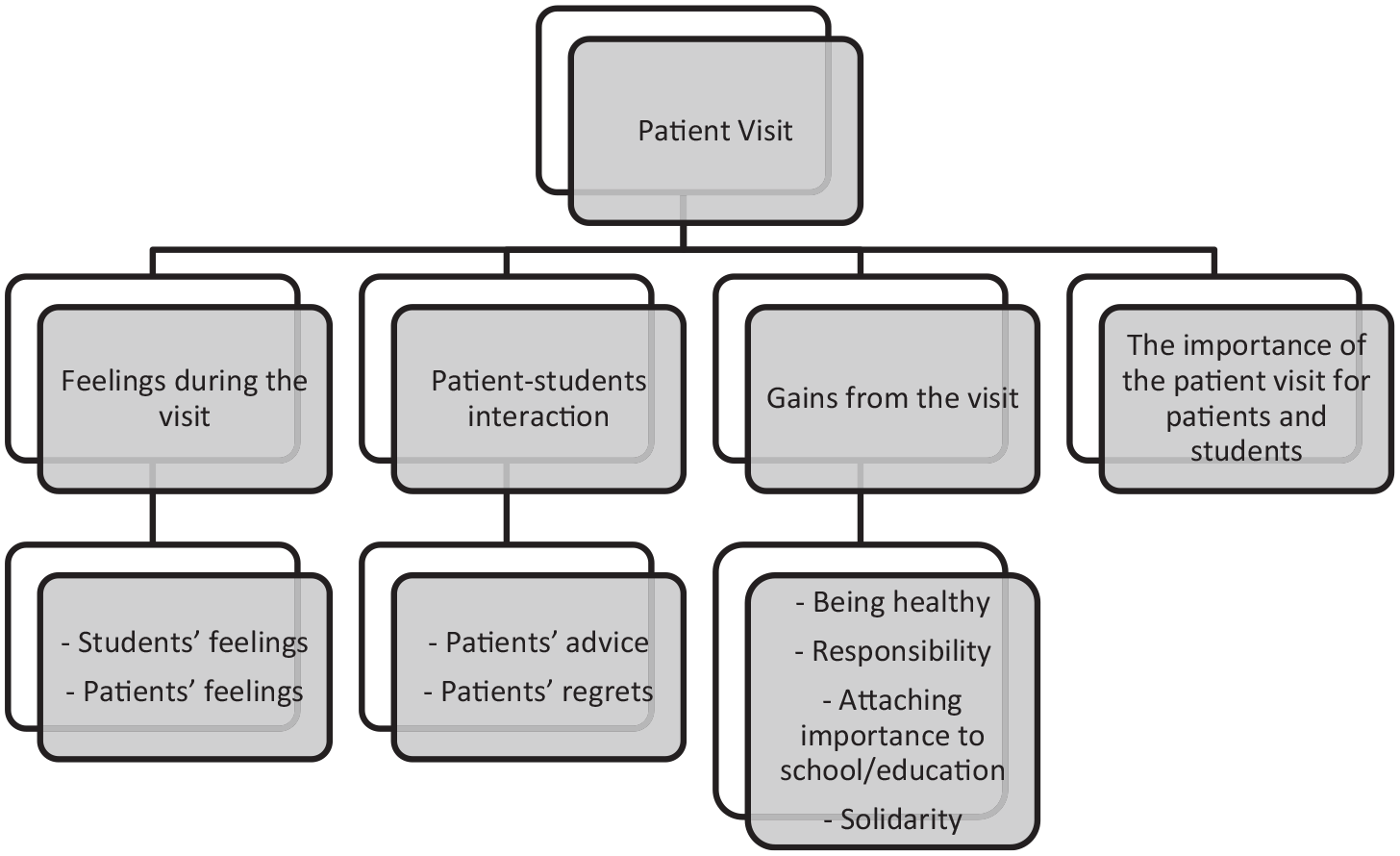
Findings obtained during and after the patient/hospital visit.
Feelings during the visit
The findings relevant to this concerned students’ and patients’ feelings. Most students reported feelings of intense sadness during the visit. A few students felt happy because they saw that the patients enjoyed the visit and had a chance to share their troubles. Ela (16) said, First of all, I was happy to participate in this visit. People’s happiness when they saw us and their sharing of their problems with us made us [feel] valuable. They talked about their life to people they did not know. This is such a great thing; this is indescribable!
Patient–student interactions
Two categories were identified under this theme: patients’ advice and patients’ regrets.
Patients’ advice to students
An examination of the interactions between the patients and students suggested that nearly all the patients provided abundant advice to the students. This advice included warning students not to make the same mistakes that they had in their youth, emphasising the importance of health, keeping away from harmful substances, avoiding developing poor nutritional habits and appreciating the value of youth. Students listened carefully to the guidance and began asking directly for advice after seeing a few patients.
One patient repeated the following statement four times: ‘Kids, escape from where you see cigarette smoke! It is such a terrible thing!’ The same patient told the students that the most important experience that convinced him to quit smoking occurred when his doctor showed him a patient whose legs had to be amputated due to tobacco abuse. The students’ reflections indicated that the patients’ warnings had a lasting impact. As Zeynep (16) explained, ‘This visit opened my eyes. The aunts’ and uncles’ advice was good. I saw how I would end up if I behaved like them’.
Patients’ regrets
When we asked the students about their opinions of the patients, most of them said that the patients showed remorse about their harmful past habits. The patients described their regrets at every opportunity, and this intensely affected the students. One female patient said, . . . Let me ask you before you ask me, which is better? Staying in a green place with fresh air or staying in such a bad and stinking place? We are here because of our mistakes. We shouldn’t have started smoking . . .
Hale (15) asked the following question to another patient, who had difficulty speaking because he was attached to a ventilator: ‘Uncle, do you ever say: ‘I wish I had never smoked?’’ His wife answered the question, because the patient could not speak: Of course he does. He has already regretted it, but it is too late. Three or four packets of cigarettes were not enough for him. He lit another cigarette as soon as the previous one was finished. Look, now. Although he quit smoking ten years ago, he is still suffering a lot . . . We could buy an apartment with the money he spent on smoking. We are now living in a shack . . .
Students frequently recounted these experiences during the post-visit interviews. Ali (17) said, ‘I felt that the uncle we visited was remorseful. He warned us not to make the same mistakes as him’.
Gains from the visit
Students’ eyes were opened by the visit. They explained that their values had shifted and that they planned to modify their behaviour accordingly.
Being healthy
All the students described how the hospital visits raised their awareness about healthy life choices and behaviours. They explained that the visit gave them the chance to observe the effects of harmful practices such as smoking, alcohol and poor eating habits on the human body. Students said this raised their consciousness about the risks of such habits, and they would strive to make better choices in the future.
Some of the students stated that they noticed how their friends and their social circle were negatively affected by cigarettes, alcohol and drugs. Their conversations with the patients enhanced their understanding of how these substances affected their peers. Nearly all the patients mentioned how a negative social environment had precipitated the development of their bad habits like smoking, alcoholism or using drugs. Some students said they would try to stay away from situations in which cigarettes and alcohol were consumed and avoid friends who used them.
In addition to avoiding situations that might cause harm, some students indicated that they had decided to actively protect their health by engaging in regular exercise or physical activity. None of the patients had mentioned exercise during the hospital visits; however, the students deduced that they should get active to maintain their health.
Responsibility
We noted that following the hospital visit, students became more conscious of the importance of avoiding harmful habits such as smoking, alcohol and drugs. Some students felt empowered by this new knowledge to educate their social circle about making healthy choices. Hale (15) said, ‘I will not allow my uncle to smoke any longer, because my father or my uncle could be in the beds we visited today’. Nil (16) said, ‘This visit led me to warn those who smoke’, while Arda (16) explained, ‘I will warn my smoking friends’. Some of the patients said, ‘We would not have started smoking or alcohol if there had been good role models for us’. Informed by this perspective, Emel (15) said, ‘I should do my best to be a good model for my social circle by avoiding bad habits’, stressing the importance of setting an example for other people.
Attaching importance to school/education
The hospital visit contributed to areas of development beyond health knowledge and behaviour. It also helped students attach greater importance to school and education. Some patients described how they adopted harmful habits because they did not see education as important in their youth, and advised students to focus on their schooling. This also influenced the students, including Nil (16), who said, ‘Formerly, I did not care about school much, but now I will because one of the patients told me: “If I were young, I would study at school.” This impressed me a lot’. Zeynep (16) and İsa (16) shared similar thoughts, saying ‘I want to study and help people’ and ‘I will care about my health and study’.
Solidarity
Overall, students felt a sense of solidarity with the patients, which represent another positive effect of the hospital visit. They explained that they felt the moral support they gave the patients during the visit could contribute to their care. Arda (16) explained, ‘We gave the patients moral support by visiting them, so they can recover sooner’. The patients also reacted positively to the students and expressed their pleasure about the visit. This led students to feel solidarity with them, with some indicating they wished to make patient visits a habit. As İrem (17) put it, ‘Patient visits enable social solidarity. I understood this well after the visit’.
The importance of the visit for patients and students
We asked students to consider the importance of the patient visit as they reflected on their experience. Students highlighted the importance of the visit both for themselves and for the patients. They considered the visit important because it gave moral support to the patients, decreasing their loneliness and hopefully expediting their recovery. Hale (15) explained, ‘It is important because making the patients happy gives them energy. They feel better and they see that they are not alone’.
Students’ most frequently provided reasons for the importance of the visit included the chance to make one-on-one observations of hospital patients, listen to their regrets and receive advice. Students learned lessons about health from these interactions, moving them to make a greater effort to live a healthy life. İsa (16) explained, ‘It is important for getting aware [of these things] and seeing the harmful aspects of something that we considered normal’. Can (16) added, ‘The patient visit was indeed like a symbol of advice. It is an important activity for raising people’s awareness. It is surely beneficial’.
The visit also appeared to develop empathy among the students, as evidenced by their statements about listening to patients and trying to understand their experiences. Ece (15) said, ‘The visit was important for understanding the patients and putting ourselves in their shoes. Because we may also be remorseful like them one day’. Damla (16) added, ‘The visit was important for showing empathy because we could be the one who was lying in the bed’.
Discussion
This study originated in the idea that patient visits might facilitate the acquisition of healthy behaviours; thus, we paid a visit to a hospital, an informal learning environment, with a group of adolescent students. We made sense of students’ experiences using the framework provided by HBM concepts (Figure 2).
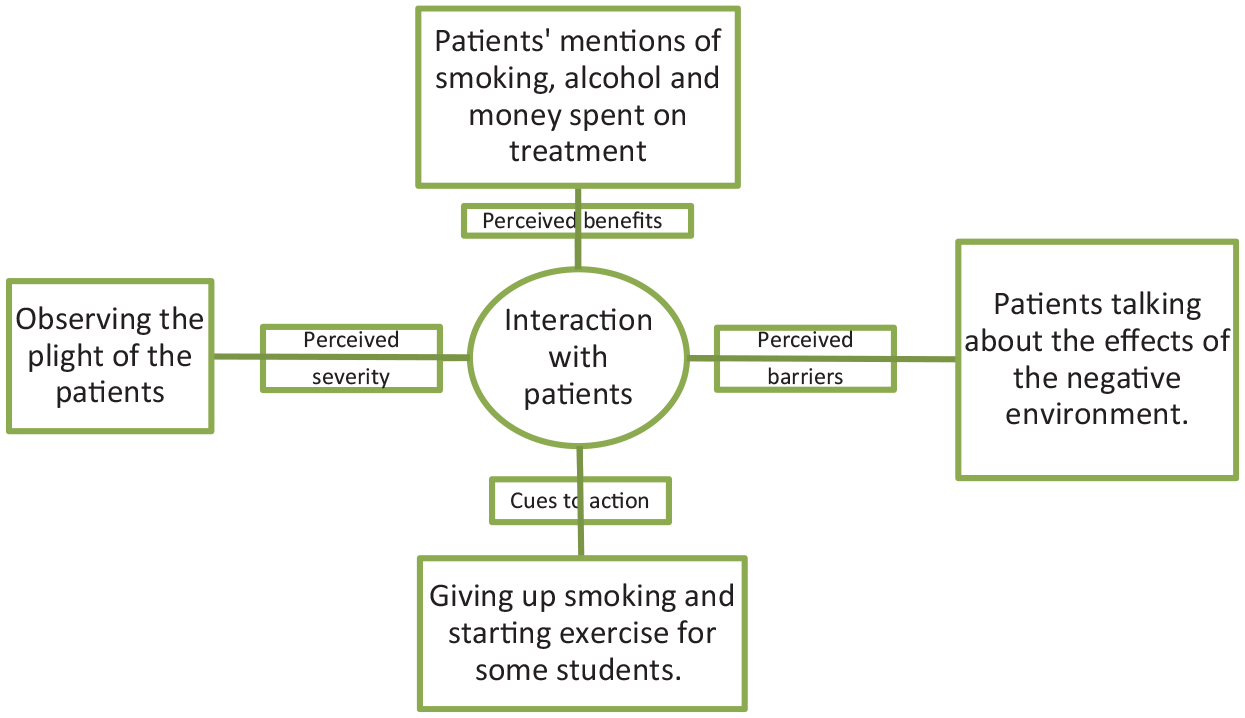
Interpretation of the results based on the health belief model.
Students became aware of many aspects of health thanks to the patient visit. This awareness was not limited to knowledge such as ‘what to do to maintain health’, but extended into action when participants stated that they would ‘keep away from places where there are bad habits such as smoking, alcohol, or drugs’. The present study contributed positively to health behaviours that can be explained conceptually by HBM, as visualised in Figure 2.
Student participants had the chance to see patients and listen to their stories firsthand as part of the activity, which contributed positively to their understanding of what could happen if they themselves did not take care of their health (perceived severity). In addition, students developed increased awareness of barriers to healthy behaviours. Interactions within the patient visits served as external cues to action for the students, providing a trigger for the acquisition of new health behaviours (Janz and Becker, 1984), one of the least-explored components of the HBM (Champion and Skinner, 2008).
Similar to the results of the current study, previous research has demonstrated that health education programmes based on physical activity and providing targeted information on topics such as diet or smoking yield positive results (Calman et al., 1985; Fairbrother et al., 2020; Rani et al., 2013; Reid and Massey, 1986; Robertson et al., 1994). Although there are numerous health education studies based on the HBM (Sharifi-rad et al., 2007; van Zyl et al., 2014), we could not find any studies that brought students and patients together, enabling social interaction and giving students the chance to observe patients directly. Because of the limitations regarding the effects of knowledge on behaviour (Baric, 1978), health education should focus on experiences and interactive activities (Meillier et al., 1997). The current study offered the students such an experience, which appeared to be effective in motivating them to change.
The hospital visit helped students act in line with important values. Based on their experiences during the visit, some students stated that they would not only exercise caution and stay away from smoking or alcohol, but they would also try to raise their loved ones’ awareness on the issue. In this way, the visit promoted the students’ responsibility and sensitivity towards others in their social circle. Some of the patients told the students that they had not cared much about school when they were young, and they made bad friends, who led them to develop harmful habits. This affected the students, who saw greater value in education after the visit. There is a cyclical relationship between health and academic achievement; poor school performance may lead to behaviours that negatively impact health, while adverse conditions such as substance abuse, poor nutrition and a sedentary lifestyle may lead to lower academic achievement (Murray et al., 2007).
The visit also contributed to social solidarity. Students were able to personally experience helping and providing moral support to another person, and many said that they enjoyed the experience. The positive effect of this may encourage them to help other people in need. Comprehensive health education in schools aims to support students’ moral, ethical, cultural and social development (Chester et al., 2019). Considering the emotions that the visit triggered, this kind of activity may also prove useful in the values education field.
Limitations
Like all studies, this one had its limitations. This study was limited to a single visit to one hospital and had a small sample size. There are several reasons for this, including the difficulty of obtaining permission from hospital administration and the sensitivity of making a patient visit. Moreover, the patient–student interactions were relatively short, due to some patients’ breathing difficulties and the reluctance of the hospital staff involved in the visit to allow a longer stay. Finally, the study’s generated only qualitative data through interviews and observations written up as field notes.
Conclusion
This study provided students with the opportunity to interact and learn from hospital patients and observe them directly. In so doing, it contributed to the development of personal values such as responsibility, the importance of school and education, and solidarity with others. In several ways, a hospital visit contributed to students’ cognitive, affective and psycho-motor development. Socially rich learning environments that enable students to interact with others have a positive contribution to make as part of health education. Hospital and patient visits can make a significant contribution to out-of-school health education with lasting effects. As James and Williams (2017) have argued, classroom learning and field learning should be combined to deepen conceptual understanding of personal and environmental well-being and health.