
Abstract
Background:
Weight stigma and bias are present in education, employment, and health care institutions, and have increased in recent years. College students in pre-health majors have been documented to hold weight biases, and interventions to mitigate these beliefs have had varying results.
Objectives:
This study’s purpose was to assess the impact of a pedagogical intervention regarding weight stigma outcomes among first-year students.
Method:
Three instructors of lower-division health and social science courses implemented a 3-module lecture series on weight stigma, the environmental sources of weight variability, and body appreciation. Participants (N = 81; 48 from intervention (INT) classrooms, 33 from comparison [COM] classrooms) completed an end-of-semester survey regarding their anti-fat biases, fat phobia, and body appreciation, and a subset (n = 13) participated in a semi-structured interview about their experiences.
Results:
Results revealed no outcome differences between the treatment versus comparison groups, although self-reported body mass index (BMI) was a significant covariate (p = .008). A significant correlation emerged between BMI and fear of fat scores for COM (r = .52, p < .01) but not for INT students (r = .28, p > .05), suggesting the intervention may have impacted how students form their anti-fat biases in relation to their BMI. Qualitative findings yielded five themes – connected course material with personal experiences; learned about weight stigma; shifted perspective on weight stigma; recognised application of weight stigma; material to future career; and valued learning about weight stigma – that provided insight into how the intervention positively affected students.
Conclusion:
Informed by the findings from this study, future interventions should take a more immersive pedagogical approach.
Introduction
Weight stigma and bias permeate social institutions, including education, employment, and health care, and have increased in recent years (Lawrence et al., 2021; Nutter et al., 2016; O’Brien et al., 2010; Panza et al., 2018; Wu and Berry, 2018). Scholars argue viewing weight bias as a social justice issue is key to acknowledging and addressing structural weight bias, or the ‘societal and structural inequalities that impact people with large bodies’ (Nutter et al., 2016: 7). Weight stigma involves the depiction of people in larger bodies as lazy, lacking in will power, and ignorant (Geller and Watkins, 2018), while weight bias involves judgements that can lead to negative outcomes for those who encounter weight discrimination.
Individuals who experience weight-based discrimination (i.e. interpersonal weight bias) report more work and school absenteeism, diminished self-esteem, lower wages, increased social isolation, and a worsened health profile (e.g. psychological health, pain) (Lacroix et al., 2017; Pearl and Puhl, 2018; Phelan et al., 2015). These data are concerning given that 40% of individuals who are categorised as being in a larger body report experiences of weight bias (Puhl et al., 2018). In addition to interpersonal weight bias, individuals can also experience intrapersonal weight bias, reflecting the extent to which these forms of stigma are internalised and affect cognitive, emotional, and behavioural well-being (Lacroix et al., 2017). Body appreciation is a related intrapersonal factor, and is associated with appearance acceptance, self-esteem, optimism, satisfaction in life, internalisation of societal appearance ideals, and self-compassion (Avalos et al., 2005). It then becomes important to consider weight bias at the intrapersonal, interpersonal, and societal levels to adequately address this issue from a social justice perspective.
In many healthcare-related careers (e.g. nutrition, medicine), weight bias exists and creates barriers to equitable patient care (Lawrence et al., 2021; Panza et al., 2018; Wu and Berry, 2018). Health and allied health professionals have been shown to focus on excess weight, even if consultations are not related to weight. An over focus on body mass index (BMI), which lacks a measure of central adiposity and has been used to draw arbitrary associations with morbidity and mortality, may be inappropriate for all individuals (Lee et al., 2017; Strings, 2019). Moreover, patients in larger bodies are often blamed for their lack of willpower and lifestyle choices, thus cultivating feelings of shame (Lawrence et al., 2021). These experiences can lead patients to opt out of future appointments due to negative interactions and inadequate healthcare related to weight-based biases.
Students following pre-health majors 1 also have documented weight biases (Fontana et al., 2013; Herzig et al., 2021; Phelan et al., 2015; Swift et al., 2013; Werkhoven, 2020; Zaroubi et al., 2021). Werkhoven (2020) identified low to medium anti-fat attitudes and fat stereotypes among pre-health majors, which were higher than non-pre-health majors. In a cross-sectional study among students in health-related majors, Swift et al. (2013) observed medium to high beliefs about persons in larger bodies using the Fat Phobia Scale (FPS). These scores pointed to stronger beliefs that weight is not controllable and to an endorsement of negative adjectives to describe persons in larger bodies. A sub-sample analysis revealed significantly higher scores among nutrition and dietetics students in the first year of their programme. It thus becomes critical that students pursuing healthcare-related professions are educated about weight bias and its negative consequences.
Recent interventions focused on reducing weight bias among college students pursuing healthcare-related degrees have yielded mixed results (Oliver et al., 2022; Rukavina et al., 2008; Werkhoven, 2021; Wijayatunga et al., 2019). Some studies have indicated mild improvements in bias reduction, while others have not. A few studies revealed minimal bias at pre-intervention, limiting the potential for change (Flint, 2015; Oliver et al., 2022; Poustchi et al., 2013; Werkhoven, 2021; Wijayatunga et al., 2019). Programmes, actions, and interventions have been evaluated primarily through quantitative surveys, with fewer including qualitative data to understand outcomes (Werkhoven, 2021). Future studies using mixed methods are needed to explore students’ quantitative attitude shifts as well as their perceptions and experiences of weight bias curriculum. interventions may be perceived differently by individuals of varying body sizes given individuals in larger bodies likely have firsthand experience of weight bias (Bessey et al., 2021). Therefore, it is important to consider body size when assessing the effectiveness of an intervention designed to address weight stigma.
Against this background, the overarching purpose of this mixed-methods study was to test the impact of a pedagogical intervention regarding weight-related biases among first-year experience students. Our main research question was how does implementing a weight bias awareness curriculum affect students’ anti-fat attitudes, fat phobia, and body appreciation? A secondary focus was to examine how intervention results differed depending on students’ self-reported BMI.
Method
Overall design and setting
The quasi-experimental design of our study introduced a weight-bias pedagogical intervention into a course designed for students in their first and second years at college. All participants were enrolled in a writing-intensive, social justice focused course created for students pursuing a major in health and social science. Intervention students were exposed to a 3-module weight bias curriculum, while students in the comparison classrooms did not receive a weight bias curriculum. Outcomes and reflections from the intervention group (three classrooms) and the comparison group (two classrooms) were analysed. A mixed-methods approach was employed to develop a more holistic understanding of the intervention’s effectiveness than might otherwise have been the case (Creswell et al., 2011). Validated quantitative surveys assessing anti-fat attitudes, fat phobia, and body appreciation were implemented pre- and post-intervention, while qualitative interviews exploring students’ perceptions of the curriculum were undertaken post-intervention.
Participants
Table 1 provides demographic information on participants, split by intervention classrooms (INT; n = 48) and comparison classrooms (COM; n = 33). Most participants were in their first or second year of college and identified as female. About half were majoring in a degree programme related to health and social sciences (e.g. pre-nursing, kinesiology), with the other half were majoring in degree programmes outside of the health and social sciences (e.g. biology, engineering). The largest number of participants identified as Asian, Latino/a/x, more than one ethnicity, or White. The distribution of BMI (calculated from self-reported height and weight) was similar between the two groups, with around 40% of participants in larger body categories (Nuttall, 2015). A smaller sample of INT students (n = 13) volunteered to participate in individual interviews (Table 2). These participants included various gender identities, ethnicities, majors, and years in school. We chose not to report individual level data for their BMI categorisations.
Participant demographics.
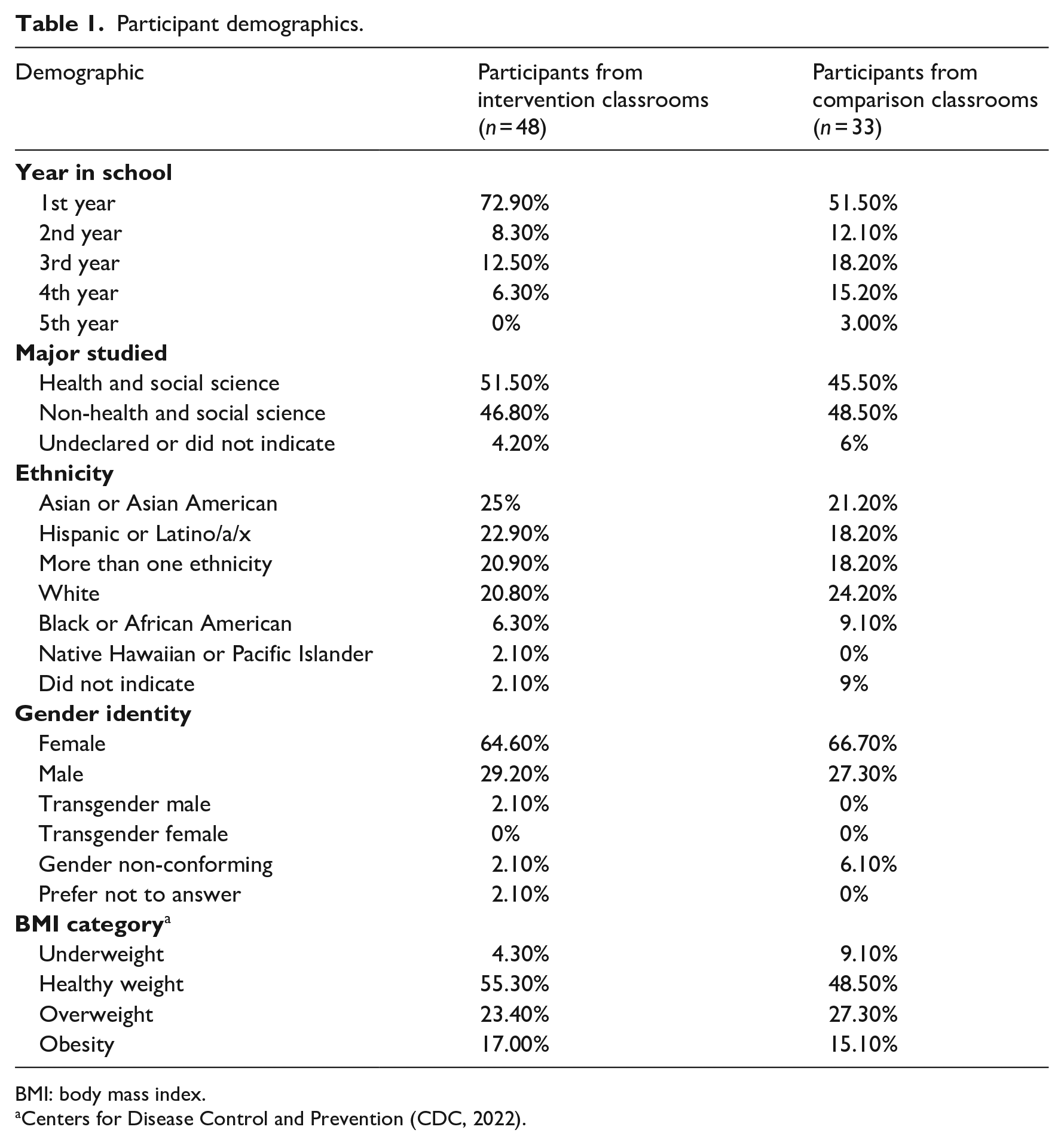
BMI: body mass index.
Centers for Disease Control and Prevention (CDC, 2022).
Individual interview participants from intervention classrooms (n = 13).

Quantitative measures
Anti-fat attitudes
The Anti-Fat Attitudes questionnaire (Crandall, 1994) is a 13-item tool that assesses three dimensions. The Dislike of Fat subscale has seven items and captures prejudice towards fat people (e.g. ‘I really don’t like fat people much’). The Fear of Fat subscale includes three items and represents personal concerns about weight ( ‘I worry about becoming fat’). The Willpower subscale is represented by three items and reflects beliefs about the controllability of weight and fatness (e.g. ‘Some people are fat because they have no willpower’). Participants responded to each item on a 9-point Likert-type scale from very strongly disagree to very strongly agree. Items on each subscale were averaged, with higher scores indicating greater anti-fat attitudes. Internal reliabilities for the scale in this study were as follows for Dislike of Fat (α = .86), Fear of Fat (α = .84), and Willpower (α = .72).
Fat phobia
The FPS (Bacon et al., 2001) includes 14 items reflecting a person’s thoughts and feelings towards persons considered to be in larger bodies. Respondents are given a pair of adjectives on opposite ends of a 5-point scale (1–5) and asked to indicate a score closest to the adjective that reflects their beliefs. Sample adjective pairs include lazy vs industrious, good self-control vs bad self-control, active vs inactive, and insecure vs secure. Half of the items were reverse scored and re-coded such that higher scores reflect greater fat phobia. Internal consistency was acceptable in this study (α = .71).
Body appreciation
The 13-item Body Appreciation Scale (Avalos et al., 2005) assesses the degree of an individual’s favourable perceptions of and respect for their own body, weight, and appearance. Participants rate each item on a 5-point scale (1 = never, 2 = seldom, 3 = sometimes, 4 = often, 5 = always) and scores are summed and averaged, with higher scores representing greater body appreciation. Sample items include ‘I feel good about my body’ and ‘Despite its flaws, I accept my body for what it is’. Internal consistency reliability scores from this study were high (α = .95).
Qualitative interview guide
An interview guide was created for semi-structured INT student interviews. Initial questions focused on participants’ backgrounds (e.g. major, future career goal) and general thoughts about their college experiences. Main questions focused on what students had learned about weight biases. Sample questions include “What, if anything, stood out to you when learning about weight stigma and anti-fat biases? and “Did you learn anything new related to weight stigma or anti-fat bias that you didn’t know already before you took the class?” The final questions captured anything else students wanted to learn or share about the topic.
Intervention
Researchers (G.G., N.B.) created a 3-module series, which included 20-minute, pre-recorded lectures with supplemental materials to accommodate student learning preferences and faculty collaborative pedagogy. The content utilised evidence-based research from 2006 to the present day regarding prevalence, impact, and intervention (Himmelstein et al., 2017; O’Brien et al., 2010; Pearl and Puhl, 2018). The module format was intended to be incorporated into an existing social justice first-year experience course. Module 1, entitled Awareness, described key aspects of weight stigma and bias, and their origins (Puhl and Brownell, 2003). The content included how weight is classified, causes of weight variability beyond an individual’s control, relationship of weight to health, weight bias in various professional and social settings, how weight bias impacts health and wellness, and how weight bias is an issue of social injustice. Module 2, titled Action, focused on changing the narrative through understanding what can be done. The content included potential actions to mediate social injustice and what students can do now (e.g. evaluate one’s terminology, communicate with others about experiences). Module 3, titled Appreciation, centered on applying weight bias information to participants’ own personal voice, lives, and environments to decrease self-stigma and also social injustice. The content included messages about how self-body appreciation can improve personal well-being as well as future patient/client interactions.
Procedure
After receiving institutional approval, three members of faculty who taught a first-year experience course were invited to participate in the study. Upon giving informed consent, faculty met with the researchers in two pre-semester sessions (1.5 hours each) to learn about the 3-modules and the supplemental syllabus for the INT. The syllabus included discussion guides, sample assignments, and student materials such as videos, podcasts, and readings. The training process was collaborative, as faculty provided feedback on the intervention materials, which were then modified. Faculty were asked to include at least two learning materials from the supplemental syllabus into each lesson module.
Instructors then delivered the modules during Weeks 4–9 of the 16-week semester. Two members of faculty taught both an INT and COM section, while one member of faculty taught one INT section. Researchers visited each classroom at the semester’s start to introduce the study and recruit participants to complete the pre-intervention survey. A Qualtrics link to the online survey was provided. The first page of the survey explained to participants that if they continued with the survey, that would indicate their consent to participate. Researchers returned at the end of the semester to distribute the post-intervention survey. At the end of the survey, students in INT classrooms indicated if they were willing to participate in an individual interview. We purposively selected and invited 19 students for an interview that represented a variety of majors, gender identities, and race/ethnicities from the list of 36 volunteers. Each student who responded to the request (n = 13) completed their semi-structured interview over Zoom with one of the two authors (G.G., N.B.). Surveys took on average 8 minutes to complete, while interviews averaged 36 minutes. Students received digital gift cards as compensation for their time ($20 per survey, $40 per interview).
Data analysis
Quantitative data were analysed using IBM SPSS Statistics 27. To answer the main research questions, a multivariate analysis of covariance (MANCOVA) was run with treatment (INT vs COM) as the independent variable, BMI as the covariate, and the five scales (Dislike of Fat, Fear of Fat, Willpower, Fat Phobia, and Body Appreciation) as dependent variables. A series of linear regressions were also run, separately for INT vs COM groups, to examine which predictors (ethnicity, gender identity, major, year in school, BMI) might explain participants’ anti-fat attitudes, fat phobia, and body appreciation scores. Statistical significance was set at p < .05.
Drawing from several qualitative approaches (Braun et al., 2016; Boyatzis, 1998; Joffe, 2011), qualitative data were analysed by means of thematic analysis. Six transcripts were initially read and coded independently (by G.G., N.B.), followed by collaborative discussion to identify agreed upon codes and preliminary themes. The same process was repeated for the eight remaining transcripts, after which the authors (G.G., N.B.) agreed upon a robust set of themes. Acting as critical friends, the remaining two authors (M.A., D.S.) reviewed themes for conceptual clarity, and confirmed or provided suggestions for modifications. Using multiple researcher viewpoints established credibility via crystallisation, whereby the final set of themes provided a complex and in-depth understanding of the data, rather than a singular truth (Tracy, 2010). To protect participants’ confidentiality, students provided their own pseudonyms during the interview, which were then used in writing up the results.
Results
Preliminary analyses
The final data set included responses from 81 participants (48 INT, 33 COM). Initial analyses revealed a small amount of missing data (1.6%), with the majority from the FPS. Missing data patterns suggested these omissions were random and likely caused by a misunderstanding of the Qualtrics sliding scale used. Four items were deleted from the scale that had > 5% missing data, which did not affect the reliability of the scale. Mean imputation was used for the remaining missing data points. Descriptive analyses suggested normal distributions for all continuous variables and acceptable reliability for all scales (Cronbach’s alpha > .7).
Post intervention comparisons
Table 3 displays the means and standard deviations for all five dependent variables at post intervention. On average, participants were unsure or agreed somewhat with having fear of becoming fat themselves, sometimes/often reported to appreciate their own bodies, strongly disagreed with disliking people who are in larger bodies, and disagreed with beliefs about people who are in larger bodies lacking willpower. MANCOVA results revealed BMI as a significant covariate (p = .017), with univariate analyses indicating BMI was only significantly related to participants’ Fear of Fat scores (p < .001, partial η2 = .153). There were no statistically significant differences between the treatment groups on anti-fat attitudes, fat phobia, or body appreciation after controlling for BMI, F(5, 73), p = .513, Wilks’Λ = .944, partial η2 = .056.
Pre and post means for intervention and comparison groups.
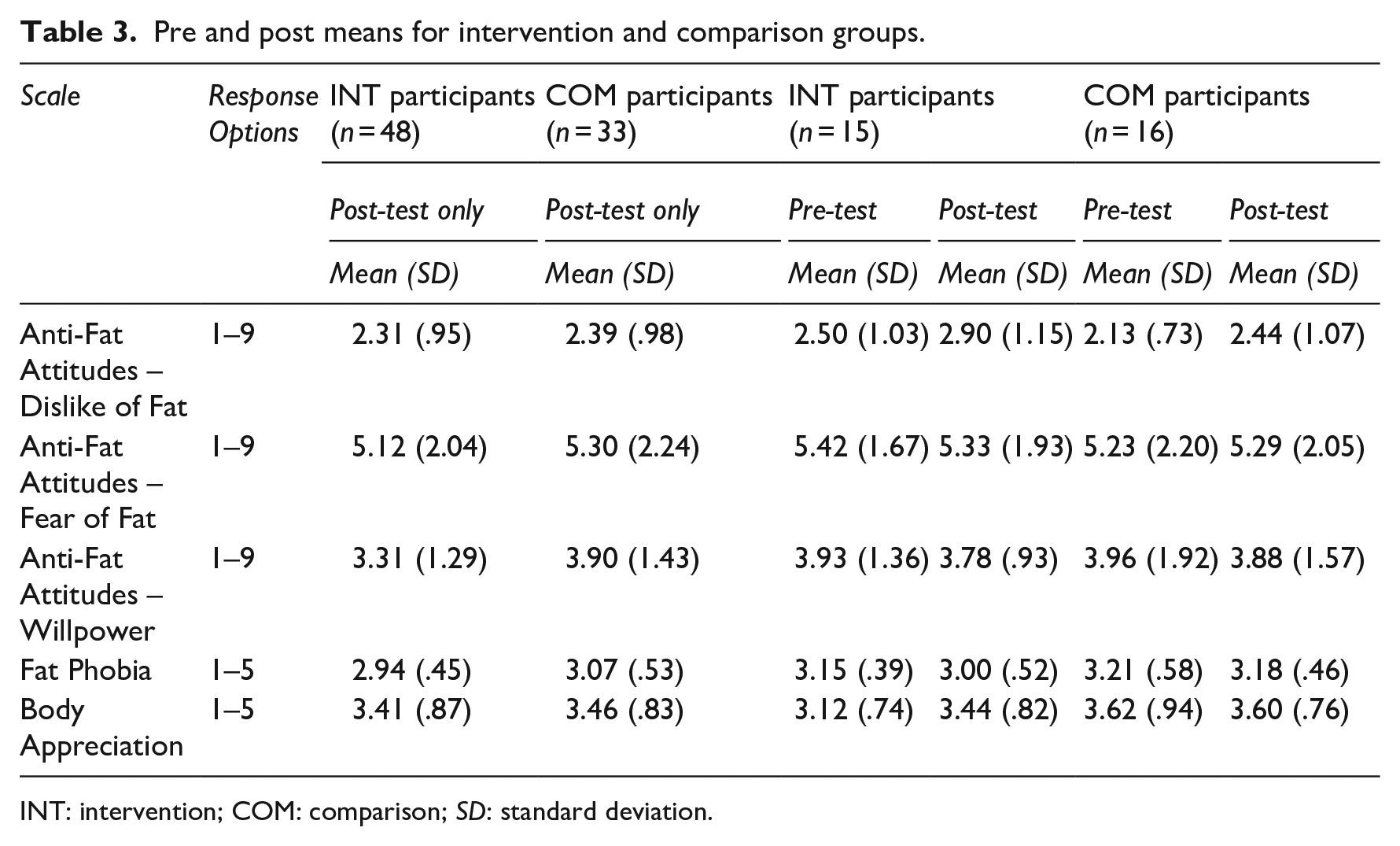
INT: intervention; COM: comparison; SD: standard deviation.
In the regression analyses, no significant predictors emerged for Dislike of Fat, Willpower, FPS, or Body Appreciation for either INT or COM participants. The combination of predictors explained 23.1% of the variance in Fear of Fat scores for COM participants, R2 = .231, F(5, 25) = 2.80, p = .038. BMI significantly predicted Fear of Fat scores, Beta = .452, t = 2.42, p = .023. That is, higher scores on participants’ reports of Fear of Fat were related to higher scores on BMI. This relationship between BMI and Fear of Fat scores was not significant for INT participants (p > .05).
Pre vs post intervention
A smaller number of participants from INT (n = 15) and COM (n = 16) classrooms completed the survey pre- and post-intervention (see Table 3). A series of paired samples t tests revealed no significant differences in pre- to post-test scores in either group (p > .05).
Qualitative findings
Five themes were developed from the data: (1) learned about weight stigma, (2) connected course material with personal experiences, (3) shifted perspective on weight stigma, (4) recognised application of weight stigma material to future career, and (5) valued learning about weight stigma. Below each theme is described and aligned with representative quotes using participants’ pseudonyms. Some disfluencies (e.g. utterances of ‘um’ ‘like’) have been removed from quotes to avoid detracting from participants’ meaning (Collins et al., 2019). To provide a sense of how many participants expressed each theme, the terms ‘a few’ for 3 or less participants, ‘some’ for 4–6 participants, ‘many’ for 7–9 participants, and ‘most’ for 10–13 participants, are used (Lewis et al., 2011).
Learned about weight stigma
Many participants reported learning factual information about weight stigma and weight biases from the intervention content. Students mentioned learning about discrimination in healthcare settings, such as gaslighting by doctors, and the potential misrepresentation of BMI as an independent marker of health. Theo said, ‘Or like the BMI scale, and how totally outdated that was. And I just kind of hadn’t thought about that. Because I was like . . . every single doctor uses that . . . it’s not accurate. It doesn’t actually work’. Rusty explained his discouragement after encountering the material, It was shocking . . . I have an altruistic view of people who work in healthcare and my wife’s a nurse and it’s just really disappointing to hear the statistics on like . . . doctors’ assumptions about people’s lifestyles and stuff based on their weight. . .demeaning them, demoralising them because of how they look . . . that seemed like the one place you might be able to go where someone’s going to hear you out thoroughly without judging you.
Students also mentioned learning about the multifaceted aetiology of health and weight, with environment, food availability, past trauma, and systematic racism having an influence beyond stereotypical patient-controlled diet and lifestyle choices. Ana explained an interesting visual her instructor had used, It [the visual] kind of explained all of the factors that go into obesity and it . . . showed how our society as a whole, we kind of focus on, oh it’s because of their laziness or lack of motivation and other really unimportant factors. And she explained how there are so many other ones that can affect someone’s weight . . . your genetics, your access to healthy food, your job, other inequalities in your life. Those often aren’t really focused upon and instead people just view weight as someone’s own choice and that’s not the case.
A few other students noted how they encountered a multifaceted definition of health and how the relationship between weight and health is often oversimplified. Claire reflected on her new understanding, Do you know the singer Lizzo? Okay so her performances are really dance heavy and she could play the flute . . . I play the Alto sax so I know it takes a lot to play an instrument and just like so much core strength. And . . . she’s like bigger, on the bigger side. So that just shows that you can be healthy and be really strong and then not look like the standard.
Connected course material with personal experiences
All but one student provided examples of how the course material was relevant to their personal experiences – either in terms of personal weight stigma discrimination or through the experiences of others (e.g. at work, with family members or friends). These connections reinforced feelings students already had about weight stigma and helped them develop more empathy for individuals who experienced it. Two students shared their family experiences: I grew up in a Filipino family and . . . they have a really negative outlook on people who are overweight and . . . when relatives are . . . leaning on the overweight side. They always talk bad about those relatives . . . and of course I think the same . . . when you see a fat person walking on the sidewalk, you’d have these negative thoughts about them because growing up, that’s how I grew up hearing’. – Pink My sister . . . a lot of the time when she goes to the doctor, she goes for asthma or things she’s dealt with her whole life and they just give her like a Tylenol. They’re just like, oh you’ll be fine, well. She is overweight, but . . . she used to play soccer so she has knee pain from the sport. And they’ll be like, Oh, maybe, if you lose some weight. – Pancha
A few students noted that they witnessed weight bias firsthand in their jobs. Monica, a medical assistant, said, ‘I’ve seen doctors actually say you know what, you need to lose a couple pounds and you’ll feel better but deep down, you know there’s something wrong’. Claire shared what she had noticed working in a women’s clothing store, I think it’s messed up. Like it’s really messed up . . . It’s [the store] mainly targeted towards black and brown minority women . . . and so I’ve witnessed the exact same style, colour of clothing, the plus size is always $4 more . . . everything plus size is so much more expensive than the petite junior side.
Shifted perspective on weight stigma
Most participants felt the material they encountered opened their eyes regarding the prevalence of weight stigma. Students acknowledged that beforehand they knew a little about the topic, but not how far reaching or impactful it is on those who experience it. Rafaela commented, That people go through that and feel that way. I obviously know to a certain extent that our society shames people, shames weight in general, but especially people that are bigger . . . but it was just a bigger eye opener, what more they have to go through like getting jobs . . . little things . . . people think they’re lazy.
Diego mentioned how his eyes had been opened to weight-based discrimination when he was scrolling through the news on his phone. He said, I saw the video about a woman needing to pay for two plane tickets . . . Why should she pay double just off of weight? I thought that was insane . . . when I’m on Apple news . . . I don’t stop for stuff like that. That was the first time I stopped for it and I was like huh, I’m changed.
Some students shared how the course material gave them an opportunity to reflect on their own weight biases. Light commented what stood out to her, ‘Recognising my own bias and how everyone kind of . . . has that, whether it be conscious or unconscious, and recognising that is important’. Violet elaborated, Right now, I’m struggling with an eating disorder and really struggling with my body image . . . when I was watching those videos, I was like inherently that’s wrong. I have a personal bias against my own weight and how much I weigh, and I obsess over that and I don’t want to be like that . . . when you’re talking to other people, it’s easy for that to come out and for that bias to be clear to those people as well as that you feel some type of way.
Recognised the application of weight stigma material to future career
Most students saw how their understanding of weight stigma and weight biases would be important in their future careers. Students pursuing careers in healthcare spoke about not assuming a person’s health issue was due to their weight. Monica discusses her approach in her career goal of physician’s assistant, in the profession I am now and once I get where I want to be . . . I will overlook the weight and not have it as the main reason . . . do blood work or go more in depth in it, and not just be oh it’s because of your weight. I . . . won’t have an opinion on somebody just because of their weight.
As a registered nurse, Pink planned to adopt a similar approach, Learning about weight stigma and the weight discrimination that’s been going around, especially in the healthcare field . . . just learning about it helps me control my own negative thoughts about you know my future patients who are a little on the heavier side.
Even students with careers plans beyond healthcare saw weight bias as an issue they could address in the future. Rafaela saw how she could address weight stigma while working for a clothing company. She explained, It’s not a secret that the fashion industry discriminates against people that are bigger. . . . I think a lot of it comes down to . . . brands. I remember I watched a video one time and said, why do we have to be labeled plus size? why can’t we just be a size? So just not having a separate section for . . . othering them and making them feel like they’re not a part of everyone else. We should just make size ranges bigger and more inclusive.
Valued learning about weight stigma
Most students mentioned how they liked learning about weight stigma, felt it was a valuable topic, and appreciated discussions about it in class. Sunflower said, ‘I’m just glad that you guys are talking about the weight stigma and bias, and trying to open up the conversation’. Pancha said, ‘It’s a chance to talk about something that . . . we seem to ignore a lot of the time’. Claire elaborated, I really liked learning about it . . . I think everybody should learn about it because they don’t teach you that in high school . . . We were always taught to go run or do this, do that, but never learned about weight stigma.
Upon learning that the weight stigma curriculum was a new part of the class, Monica commented, ‘I was just glad that it was added. . .I’ve experienced personally and through my profession, so I was glad that it was showing other people’. Violet also noted how important it was to discuss the topic, I really like the fact that we even addressed it because I feel like it’s not something that is talked about a lot . . . I think there’s a lot of intrinsic value in talking about this, and having a discussion about it, because, you know, you realise more about yourself and you realise more about the world around you.
Discussion
The primary intent of this mixed-methods study was to determine whether a brief pedagogical intervention focused on weight stigma and weight bias could shift students’ perspectives. On average, students in this study reported low to medium anti-fat attitudes, low to moderate fat phobia, and modest body appreciation. Our quantitative results did not reveal significant differences between students in the pedagogical intervention compared to those who were not, echoing previous research employing similar content and duration (Elboim-Gabyzon et al., 2020; Oliver et al., 2022; Usta et al., 2021; Werkhoven, 2020; Wijayatunga et al., 2021). However, self-reported BMI was a positive, significant predictor of students’ fear of becoming fat themselves, and this relationship was significant for students in the comparison, but not the intervention, classrooms. It is possible the intervention influenced students’ understanding that BMI and weight are not absolute indicators of health, which may explain the lack of relationship between BMI and Fear of Fat. Bessey et al. (2021) found that pre-dietitian students who identified themselves as being in a larger body felt their identities as dietetic students and as fat people were in conflict. Our findings additionally suggest an individual’s perception of their body may be important when designing and delivering a weight stigma intervention.
Qualitative findings provided more insight into how the intervention impacted students’ learning and awareness of weight stigma, further reinforcing the value of the mixed-methods approach. Students were able to cite specific content about weight stigma that was covered in the intervention, suggesting the retention of these ideas. One reason why students may have retained this knowledge is because they connected to the material personally and found it meaningful to talk about. Curriculum material is often easier to remember when it is relevant to one’s life (Royce, 2016). Given the high prevalence of societal weight stigma (Puhl et al., 2018), it is not surprising that students themselves experienced or knew someone who had encountered weight stigma.
Beyond simply learning facts, students noted how their perspectives on weight stigma changed. They became more aware of, and wanted to unlearn, their acknowledged biases. One explanation for this shift in perspective may be because faculty directly named and addressed the discriminatory impact and prevalence of weight stigma, perhaps for the first time for some students. As Royce (2016) states, ‘if fat hatred can be taught (at the societal level), calling it by name and engaging it in the classroom may just constitute a progressive step towards unteaching it’ (p. 28). Evidence-based recommendations by Schmidt and Brochu (2021) note that stigma is learned through subtle messaging, but unlearning must be undertaken with intent and directness. Our results support the idea of the classroom being a valuable environment in which to unravel false stereotypes through intentional pedagogy.
The fact that students saw weight stigma and weight bias as relevant to their future careers was a particularly encouraging finding, given the documented weight bias among pre-health professionals (Lawrence et al., 2021; Panza et al., 2018; Zaroubi et al., 2021). Responses from our sample echoed Schmidt and Brochu’s (2021) recommendation that students pursuing health profession careers adopt a more holistic and inclusive approach, beyond focusing only on patients’ shape and size. Interestingly, our data showed that even participants not pursuing health profession careers (e.g. fashion, history teacher) also saw how weight stigma could be relevant in their future jobs. This outcome suggests a wider applicability of this intervention to college curricula beyond health-related subjects.
Several reasons may explain why the intervention was not more impactful quantitatively, or at the classroom level. First, the small sample size limited statistical power to identify significant differences among INT vs COM groups, as well as between instructors or sections. Students also reported low to medium levels of weight bias, suggesting there was not a significant amount of weight bias to reduce in the first place. Interestingly, students reported the highest scores on measures related to their own bodies (i.e. Fear of Fat, Body Appreciation). Another explanation for why the intervention was not as impactful may relate to the duration and dose of the intervention itself. Modules were relatively brief and concentrated, limiting the exposure students had to the content and timing for deeper discussion. Moreover, we were unable to verify whether all students participated in all aspects of the modules (e.g. watching video recordings, participating in discussions). Although some previous research indicated brief interventions were successful (O’Hara et al., 2021), others did not (Wijayatunga et al., 2021). Instructors were also given flexibility in how they implemented the modules and which specific materials they incorporated into the existing curriculum. While this strategy strengthened the ecological validity of the study, this variability limited the ability to identify cause-and-effect.
Implications for future research
Directions for future studies should be noted. First, it seems important to have an interview guide that focuses on the intersectionality of weight stigma with gender and racial/ethnic identities (Himmelstein et al., 2017). In this study, participants discussed these identities in their responses to our questions to a varying degree. An important step in future research would be to explicitly explore social identities and weight stigma so as to more inclusively understand and deliver interventions. Second, we asked participants to self-report their own height and weight, which were then used to calculate their BMI and used as an indicator of body composition. Our purpose was descriptive and not meant to further stigmatise participants. However, students may have felt uncomfortable answering questions about height and weight. Future studies would benefit from a more inclusive and less stigmatising measure of perceived body composition or adiposity.
Third, our modules provided awareness of weight stigma, appreciation of various body shapes and sizes, and action tips about speaking out, but did not have a specific focus on standing up to the systematic structure of weight stigma. Schmidt and Brochu (2021) noted that framing fat stigma as a problem without providing alternative models of health led to little change. O’Reilly (2016) similarly suggests that only countering students’ myths about weight and the medicalisation of weight may not be an effective approach. She suggests adopting a more critical pedagogy, whereby students are given the skills to ‘question authority and power structures’ (p. 194), rather than simply countering myths about weight. It may be that a more direct emphasis on alternative models of health and critical pedagogy would lead to more impactful changes. Finally, we recommend future researchers similarly adopt a mixed-methods approach to data collection. Having both quantitative and qualitative data allowed us to more comprehensively understand how the intervention did or did not impact students, as well as identify areas for improvement.
Conclusion
Pedagogical interventions in college classrooms provide an opportunity to address systemic weight-stigma biases prevalent in society and among future health professionals. This study contributes additional knowledge about how to potentially shift students’ perspectives and become aware of how weight stigma is relevant in their future careers. The mixed-methods approach adopted was particularly valuable in obtaining students’ experiences, adding to our understanding of combatting weight biases. Although the quantitative results were not statistically significant, qualitative findings are encouraging in suggesting that a brief intervention integrated into an existing college course has the potential to engage students with this important social justice issue. This potential can be realised in future interventions that are longer term in duration and delivered more uniformly across classrooms, focusing on intersectionality, and including less stigmatising measures of body composition.
Footnotes
Acknowledgements
We would like to thank Jalen Sharp, Carolina Overton and Johana Duarte for implementing the interventions in their classrooms, and Valerie Nhan and Nakea Harrison for assisting with data collection.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: this work was supported by San Francisco Stateʼs Office of Research & Sponsored Programmes, Office of Faculty Affairs & Professional Development, and the Professional Development Council, SF State Research and Scholarly Activity Fund (Reference AY2020-2021).