
Abstract
Objective:
African Americans in the USA experience a disproportionate burden of chronic disease. Healthy lifestyle promotion programmes can help decrease this disease risk. This study determined the feasibility of using dyadic peer support to augment an existing healthy lifestyle programme in African American churches.
Design:
A prospective pre-post design was used with 80 participants from three churches in the southeastern USA over an 18-week period.
Methods:
Participants attended 9 weeks of group nutrition classes followed by 9 weeks of a dyadic peer support programme. Feasibility was measured by recruitment, acceptability, ability to collect peer support data, ability to implement the peer support component and preliminary health outcomes. Descriptive statistics and multilevel models were used to analyse the data.
Results:
Seventy-eight percent of participants completed group classes and peer support activities. Over 95% of participants would work with a partner again. Lay leaders and educators felt they had the resources and participant support to implement a dyadic peer support intervention. Participants achieved small but significant average increases of 1.1 fruit servings per day (p = .001) and 1.2 days of physical activity per week (p = .01) post-intervention. Significant changes in weight (−2.6 pounds, 95% confidence interval [CI] = −4.18, −1.1; p = .001) and vegetable intake (0.681 servings, 95% CI = 0.122, 1.241; p = .017) achieved during the first 9 weeks of the programme were maintained during the second 9 weeks.
Conclusion:
Dyadic peer support can successfully be used to augment existing healthy lifestyle promotion programmes within African American churches. Studies using control groups are needed to test the effectiveness of dyadic peer support on health outcomes more rigorously.
Introduction
Chronic diseases such as hypertension, cancer, obesity and diabetes significantly impact the quality of life, cost trillions of dollars to manage and treat and are becoming more prevalent in the USA (Raghupathi and Raghupathi, 2018). Nearly half of all adults in the USA are living with a chronic health condition, with African Americans sharing a disproportionate burden of disease (National Center for Chronic Disease Prevention and Health Promotion, 2021). High blood pressure is diagnosed in 45% of African American adults compared to 31% of White American adults (Aggarwal et al., 2021). In 2017, African American adults were 1.6 times more likely to be diagnosed with diabetes than White Americans and twice as likely to die from it (Office of Minority Health, 2019).Finally, obesity is 1.3 times more prevalent among African Americans than White Americans (Office of Minority Health, 2020).
Federally funded research and national and state health policies have aimed to address the higher disease burden among African Americans by integrating programmes into communities and delivering them through culturally relevant organisations (Office of Disease Prevention and Health Promotion, 2020). Healthy lifestyle and disease prevention programmes can decrease disease risk, but existing programmes have lower retention rates and smaller results for African Americans (Carr et al., 2020; Samuel-Hodge et al., 2014; Whitt-Glover et al., 2013) compared to White Americans. New and more innovative programmes are needed to prevent disease and promote healthy lifestyles.
Peer support, especially that provided by peer support dyads, is an effective health promotion strategy (Aschbrenner et al., 2016; Sorkin et al., 2014) and has been recommended for use with African American populations (Wolfe, 2004). The purpose of this study was to determine the feasibility of using dyadic peer support to augment an existing healthy lifestyle promotion programme in African American churches.
Dyadic peer support
Dyadic peer support, also referred to as mutual peer support (Valenstein et al., 2016) or reciprocal peer support (Heisler et al., 2010), occurs when two people who have the same health condition(s) work together to achieve similar health goals (Leahey and Wing, 2012). Dyadic peer support has been used successfully in numerous disease management and health promotion studies. Aschbrenner et al. (2016) achieved high participant satisfaction and retention (100%) in a small dyadic peer support healthy lifestyle intervention for people with serious mental illness. Family dyads in healthy lifestyle studies show improved dyadic communication, nutrition and weight loss (Samuel-Hodge et al., 2017; Sorkin et al., 2014). A programme for diabetic African American family members found a 5-kg difference in weight loss between primary participants with and without a peer partner (Samuel-Hodge et al., 2017). In another study to improve diabetes management, acquaintance dyads also reported better diabetes control compared to their baseline controls (Heisler and Piette, 2005). Over 70% of participants stated their partner helped them improve behaviours like making healthier food choices. Furthermore, in a weight loss study comparing different categories of support partners, the outcomes achieved from peer support dyads were comparable to those achieved from professional support (Leahey and Wing, 2012). Following a 6-month intervention, participants paired in dyads lost nearly as much weight as those being coached by a professional. Importantly, peer dyads may allow for more sustainable changes because they can reinforce each other’s skills and knowledge (Travis et al., 2010).
In African American healthy lifestyle promotion programmes, churches often rely on some form of social support, such as pastors providing health-related sermons and group health classes. Qualitative studies with African American churchgoers show a desire for peer support at all levels (e.g. pastoral, ministerial, leadership, membership) (Boltri et al., 2006; Shanks, 2017). However, no programmes, to our knowledge, have leveraged the potential power of dyadic peer support to augment existing health promotion programme delivery. We report the feasibility of a prospective multi-method 18-week pilot trial as part of an existing healthy lifestyle promotion programme in three African American churches in North Carolina.
Methods
Participants and setting
Faith communities in North Carolina were approached and recruited to the study between May and November 2018 via email, their Facebook sites, phone, community organisation board meetings and face-to-face visits. The study was implemented in collaboration with three North Carolina Cooperative Extension Nutrition Educators. The inclusion criteria for churches were faith communities with predominantly African American members in one of the three counties assigned to the nutrition educators. Participation was open to all church members or regular churchgoers (i.e. those who attended church most Sundays of the month or who were active in a church programme or activity), who were 18 years or older, able to engage in moderate physical activity, interested in health improvement (no specific medical diagnosis) and identifying as African American. The programme was advertised through word of mouth and church announcements. Churches in each county were selected based on their availability to host the programme within the study timeframe.
Study design
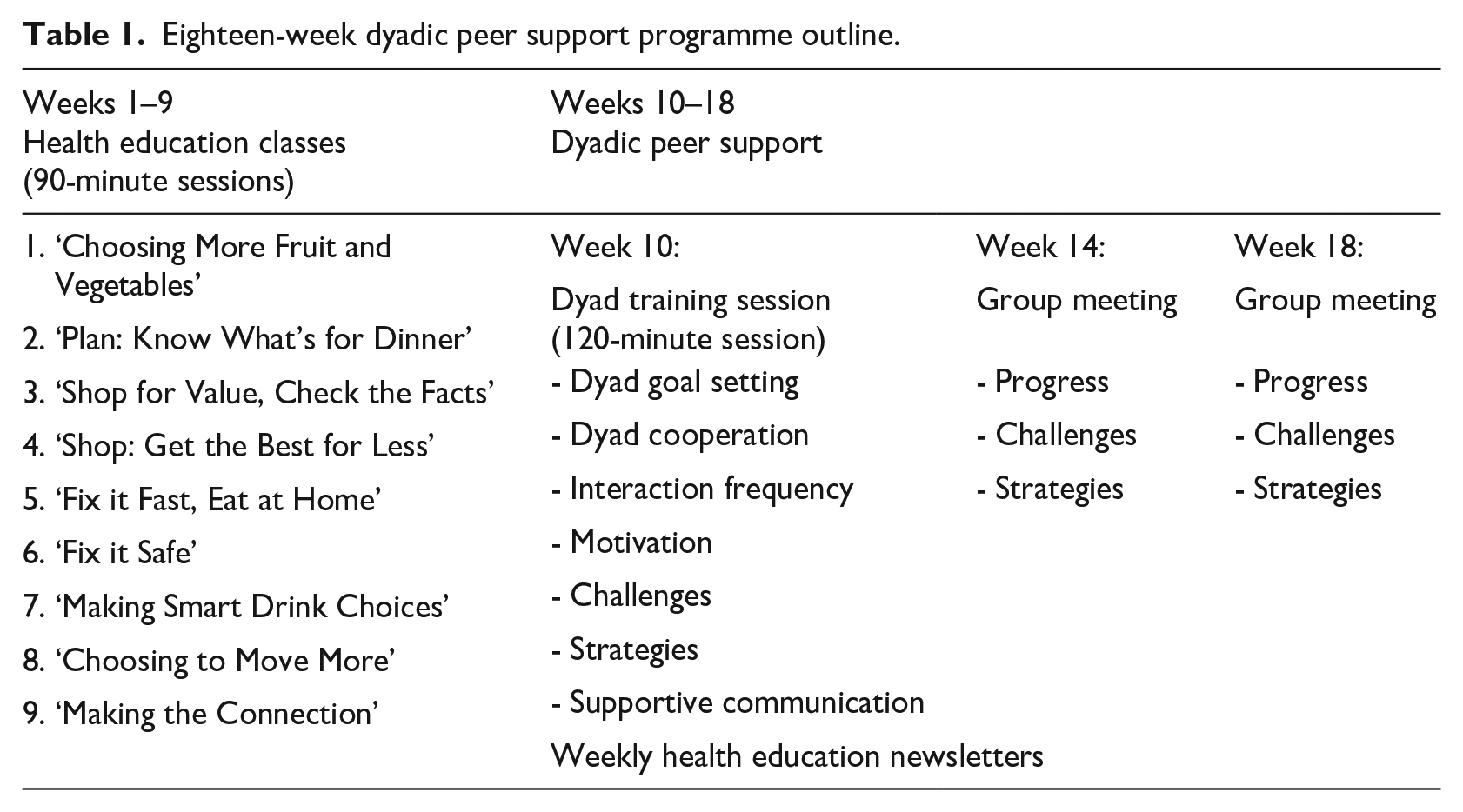
This was a prospective feasibility study. The 18-week intervention included 9 weeks of group health education classes in the faith communities, a dyadic training session and 9 weeks of dyads working independently to achieve their health goals (Table 1). Participants reconvened in the middle and at the end of a second 9-week period to share progress. Biometric, physical activity and dietary assessments were completed at baseline, 9, 14 and 18 weeks. Before starting, the study’s principal investigator (CC) and nutrition educators (AH, YB, AJ) explained the programme to all potential participants. The principal investigator read the consent form, provided potential participants time to review it independently and then gained the consent of members interested in participating. Duke University Institutional Review Board approved the study. Participants who completed the programme received a US$25 gift card for their time. Other church health promotion studies have used randomised control groups to test programme effectiveness (Newton et al., 2018), but for the purpose of this small feasibility study, each of the faith communities involved was provided with the programme.
Eighteen-week dyadic peer support programme outline.
Theoretical approach
This study was guided by existing theories of goal setting and social support among dyads (Fitzsimons et al., 2015; Johnson, 2003; Lewis et al., 2006). When individuals join a dyad, their goal attainment becomes intertwined. Mutually agreed upon goals are more likely to be attained within the dyadic relationship due to a desire to raise the other person, and the pair as a whole, to a better health status (Fitzsimons et al., 2015; Johnson, 2003; Lewis et al., 2006).). In this study, dyadic peer support training included discussions about goal setting and approaches for partners to communicate with and provide support to their partner (Table 1). Participants’ perception of being helped by their partners was assessed by means of a post-intervention feasibility survey.
Intervention
Existing healthy lifestyle promotion programme
Faithful Families Thriving Communities (FFTC) is a healthy lifestyle promotion curriculum implemented in faith communities across the state of North Carolina for the past 14 years (Hardison-Moody and Yao, 2019). The programme comprises nine weekly 90-minute group health education classes delivered by an experienced nutrition educator. Church lay leaders co-led the programme by adapting elements of the class curriculum and presentations to the needs of their community and integrating spiritual elements. Lay leaders at each site (including a nurse, members of the health ministry and the pastor’s wife) met with the principal investigator initially to learn about the programme. After speaking with their church leadership, if the faith community decided to host the programme, lay leaders volunteered to co-lead the programme. Before starting work, the lay leaders met individually with nutrition educators for an hour to review the programme logistics and curriculum and provide suggestions for lesson customisation. Programme content focuses on nutrition and physical activity (e.g. Choosing to Move More Throughout the Day) and included healthy cooking demonstrations and/or food tastings.
New dyadic peer support component
Data indicate leveraging dyadic peer support may improve the adoption and sustainability of new health behaviours after formal health education classes end (Aschbrenner et al., 2016). After attending one 120-minute dyadic training session, dyads worked together for 9 weeks (weeks 10–18) to meet national recommendations for fruit and vegetable consumption (⩾6 servings/day), physical activity (⩾30 minutes of moderate 5 days/week) and achieve any other health goals they considered important (e.g. less sugar, more sleep and increased water).
In other peer support studies, participants signed up to participate with a support person they chose before the study started (Aschbrenner et al., 2016; Samuel-Hodge et al., 2017), or were assigned a partner during the study (Leahey and Wing, 2012; Travis et al., 2010). In this study, programme participants chose a partner during the final group class or were assigned a partner based on observed interactions. Formative interviews with 11 nutrition educators and lay church members were completed by the principal investigator before designing the peer support component. Interviewees agreed church members would be interested in choosing an ‘accountability partner’ to work with and indicated it would be important to have a structured programme, set specific goals together and communicate in supportive and non-judgmental ways.
The 120-minute dyadic peer support training session was delivered by the Principal Investigator who has 20 years experience working in health education. Session topics were dyad goal setting, dyad cooperation and supportive communication. Topics were based on the behaviour change literature (Hooker et al., 2018) and the dyadic peer support literature, both of which emphasise frequent communication, listening and supportive feedback (Fitzsimons et al., 2015; Kowitt et al., 2017; Lewis et al., 2006). Dyads discussed their goals, how their partners could best support them, how often they would like to communicate and preferred mode of communication. Dyads were encouraged to maintain weekly contact with their partners, and track how often they communicated.
After the training session, dyads committed to working on health goals for the next 8 weeks. The PI provided communication tracking sheets to participants and asked them to record the frequency of communication with their partner about health goals each week. As suggested in peer support literature (e.g. Peers for Progress, n.d.), dyads reconvened at their faith communities after 4 weeks of independent dyadic work (week 14) to share their progress and challenges. Dyads were also sent weekly newsletters, developed and used previously by FFTC, encouraging continued physical activity and nutrition. The principal investigator and nutrition educator attended group classes and dyadic support sessions to maintain continuity.
Measures and data analysis
Programme feasibility
The main study outcome, feasibility of using dyadic peer support to augment an existing programme, was determined by recruitment, data collection, acceptability, implementation and preliminary intervention outcomes (Orsmond and Cohn, 2015).
Recruitment
Recruitment capability was assessed by tracking the number of churches contacted, reached and interested in hosting the programme. Our goal was to recruit one church from each of the three counties represented by the nutrition educator. Data from qualitative interviews generally reach information saturation between 10 and 15 interviews (Guest et al., 2006). Thus, a sample size of 20 dyads or 40 participants was planned to ensure saturation and account for a potential attrition rate of 30% (Lemstra et al., 2016). Recruitment patterns were analysed using descriptive statistics.
Data collection
Ability to collect relevant data was analysed using descriptive statistics of participants’ self-reported weekly communication with their partner and the proportion able to submit their nutrition and physical activity logs. We considered at least twice weekly communication between members of a dyad an indication of feasibility (Heisler and Piette, 2005).
Acceptability
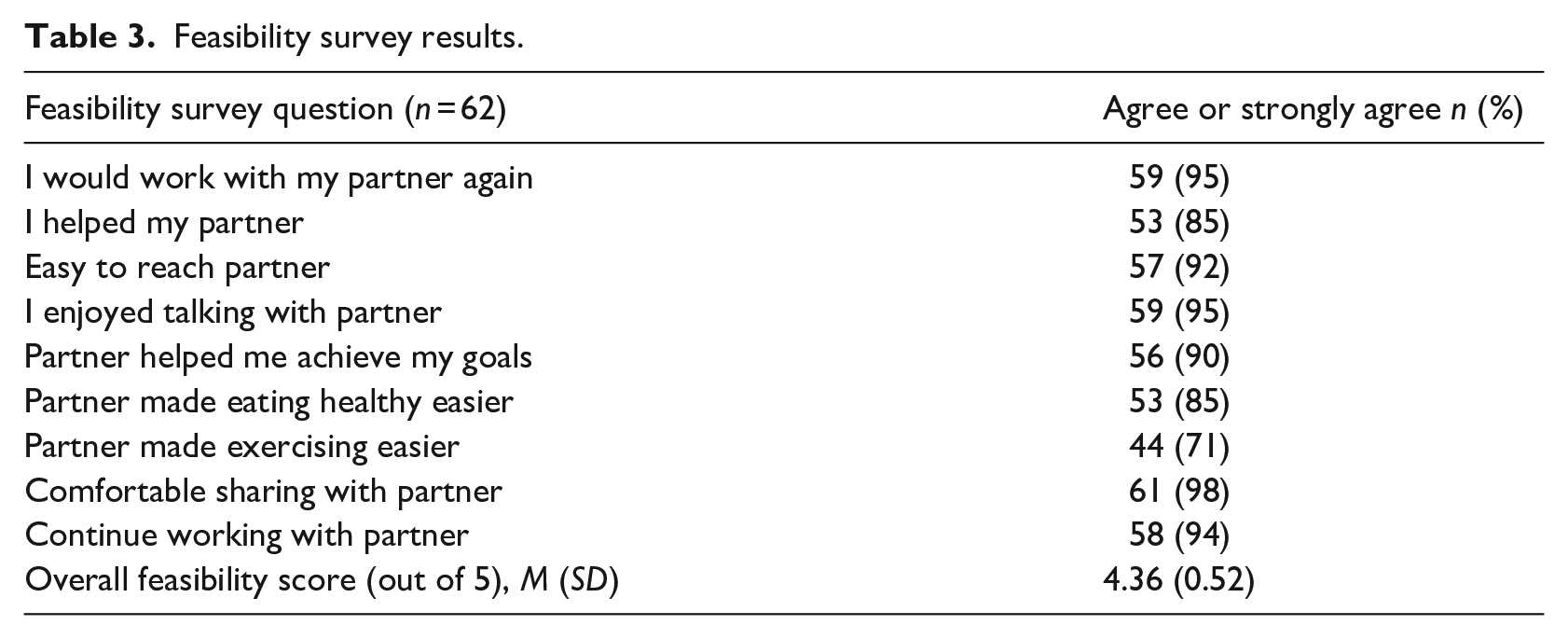
We assessed the acceptability of the programme using a nine-item post-intervention feasibility survey, as well as by tracking class attendance and retention. The feasibility survey was adapted from one used with adult friend dyads (Heisler and Piette, 2005). Survey questions included ‘My peer support partner helped me do things to improve my eating habits’ and ‘I helped my partner achieve their goals’. The survey consisted of 5-point Likert-type items from 1 = strongly disagree to 5 = strongly agree. Cronbach’s alpha for the survey was .87. Acceptability was analysed using descriptive statistics relating to participant attendance and retention, and average feasibility survey scores. Frequency of choosing ‘agree’ or ‘strongly agree’ was also calculated for each item. A multilevel model (participants nested in dyads) was used to determine whether dyad relationship type (i.e. family, friend, acquaintance) was associated with higher feasibility scores. Previous study results using the feasibility scale found at least 90% of participants agreed or strongly agreed their partners were helpful in achieving their health goals (Heisler and Piette, 2005). Therefore, the intervention was considered acceptable if at least 90% of survey respondents agreed their partners were helpful.
Implementation
We assessed nutrition educators’ ability to implement the programme and any suggestions for improvement through post-intervention semi-structured interviews with nutrition educators and lay leaders. Interviewees were asked, ‘What was your overall experience with the programme?’ and ‘What do you think can be changed to improve the peer support component?’. Interview transcripts were entered into NVivo (version 10) and analysed using content analysis (Hsieh and Shannon, 2005) and inductive coding. Transcripts were reviewed by the principal investigator to identify concepts and themes and by a co-author to compare themes, resolve discrepancies and interpret results.
Preliminary health outcomes
Preliminary evaluation of intervention outcomes was assessed through changes in clinical measurements and nutrition and physical activity survey results. The study principal investigator, who was a nurse, measured weight, blood pressure and body mass index (BMI) at week 1 (beginning of programme), week 9 (end of health education classes/beginning of dyadic component), week 14 (middle of dyadic component) and week 18 (end of programme). Participants entered a private area in the church and sat for 5 minutes before having blood pressure measured using an Omron electronic cuff (or Welch Allyn manual blood pressure cuff if measures could not be obtained electronically). Tanita digital scales were used to measure weight in a private area in each church and height was self-reported.
Fruit and vegetable intake and physical activity were measured at three time points, weeks 1, 9 and 18, using the 20-item FFTC survey developed by the US Department of Agriculture Expanded Food and Nutrition Education Program (Bradford et al., 2010). The FFTC survey measures dietary intake via a 24-hour food recall and two items asking about the average number of fruit and vegetable servings consumed each day. Cronbach’s alpha of the two survey items was .60 at baseline, .70 at week 9, .60 at week 18 and .80 between all three time points, showing acceptable internal consistency.
Participant characteristics obtained at baseline were analysed using descriptive statistics. T tests were used to identify any differences between participants who completed versus those who did not complete the programme. Analysis of variance (ANOVA) and Fisher’s exact tests were used to identify any significant differences in baseline characteristics between participants at different church locations. A three-level mixed model (participants nested within dyads over time) was used to assess changes in weight, BMI, systolic blood pressure, fruit and vegetable intake and physical activity. Both unadjusted and adjusted models were run. Church site, dyad relationship (i.e. friend, family or acquaintance), dyad assignment (whether dyads chose or were assigned their partner) and participant characteristics (age, sex, education) were added as model covariates. The potential influence of working with a partner during the second 9 weeks was accounted for by creating a dichotomous variable to separate measurements taken before and after participants were paired. Descriptive statistics were used to assess clinically significant changes in blood pressure and weight. Any participant improvements in clinical, nutrition or physical activity outcomes were an indicator of feasibility.
Results
Recruitment
Churches (N = 62) in three North Carolina counties were approached and contact was made with 36 churches to introduce the programme. Of the seven churches who were interested in doing so, three were ready to begin immediately and selected to start the programme. Other churches cited lack of time due to previously scheduled programmes, holidays or school starting as reasons for not participating.
Data collection
Dyads reported communicating on average 2.5 times per week. Forty-two of the 63 (67%) participants who completed the programme recorded and submitted their nutrition and physical activity logs.
Acceptability
Enrolment was open to all adult members of each church who fit the inclusion criteria. Eighty church members across the three church sites (Ns = 18, 24 and 38) consented to participate and were enrolled. Their mean age was 64 years (SD = 11.79) (Table 2), ranging from 18 to 87 years. Forty-three percent of participants had completed or had received some high school education. All self-identified as African American and 84% were women. Participants were affiliated with Baptist (67%) and African Methodist Episcopal (23%) denominations.
Baseline demographics and preliminary health outcomes.
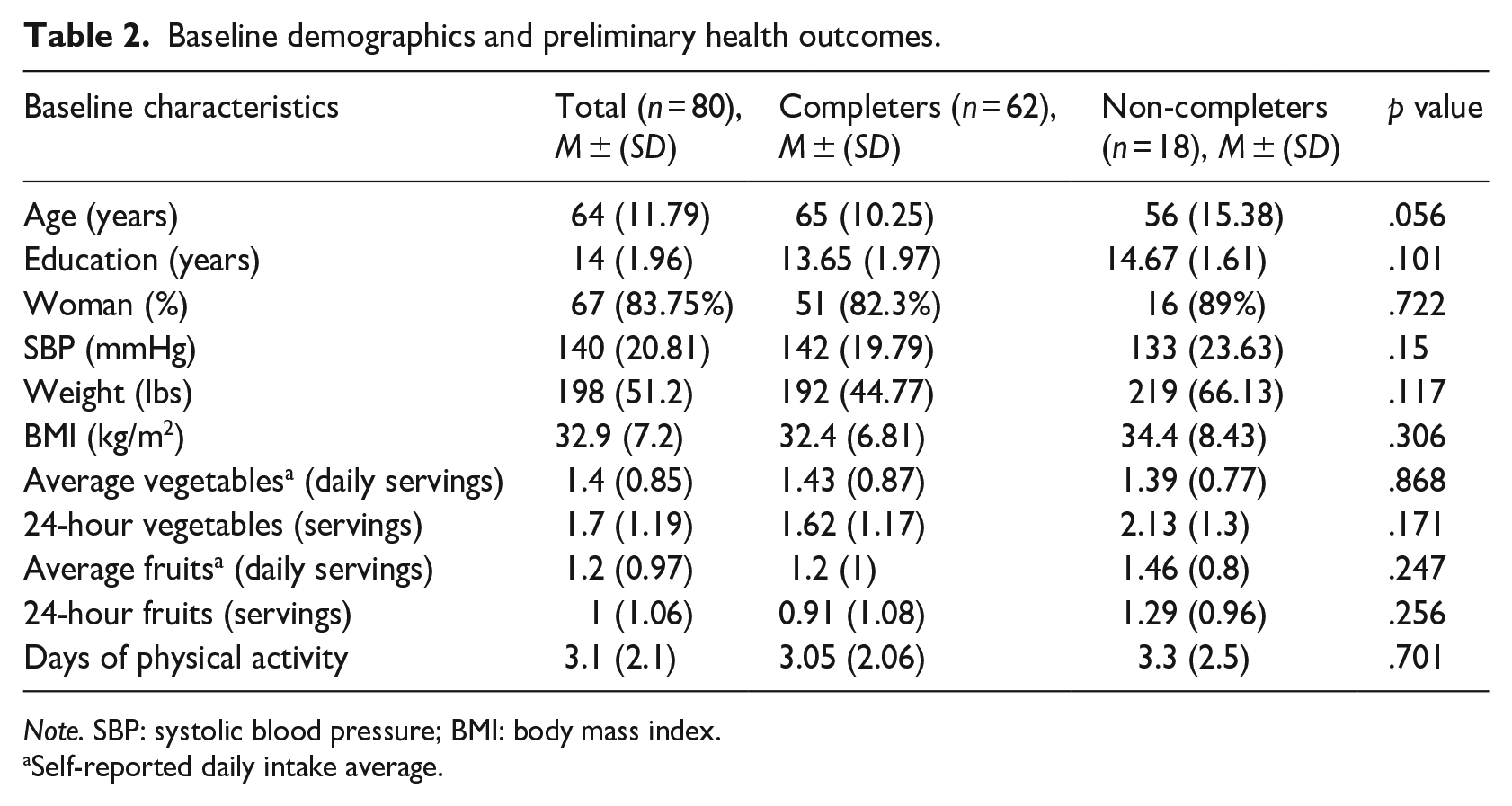
Note. SBP: systolic blood pressure; BMI: body mass index.
Self-reported daily intake average.
Sixty-two (78%) of the 80 participants completed the entire 18-week programme. Completers were defined as those who participated in group and dyad activities, worked with a partner and attended the programme’s final class. Sixty-eight (85%) participants completed the 9 weeks of education classes and 65 (96%) of those continued to the 9-week dyadic peer support component. All dyads attended the dyad training session. Of the 12 total classes (nine health education classes, one dyad training session, one dyad group meeting, final programme class), the mean number of classes attended was 9 out of 12 (SD = 1.3).
Thirty-one dyads and one triad (to account for odd number of participants) were created. Sixteen were friend pairs, 12 were family pairs and 4 were assigned acquaintances. Mean feasibility score was 4.36 out of 5 (Table 3). Most participants (95%) agreed or strongly agreed they would work with their partner again and 90% agreed or strongly agreed their partner helped them achieve their goals. Predictors of higher feasibility scores were friend dyadic relationships (0.846 points; 95% confidence interval [CI] = 0.394, 1.298; p = .001) and family dyadic relationships (0.606 points; 95% CI = 0.183, 1.029; p = .006).
Feasibility survey results.
Implementation
Ability to implement the peer support component
Lay leaders expressed positive experiences with the dyadic peer support component. The most time-consuming activities were booking rooms for the programme and sending out announcements about meeting times. During the dyadic peer support component, lay leaders were rarely called upon to provide additional support to dyads. Nutrition educators also felt it was feasible to add the dyadic peer support component. Their biggest concern was potential difficulty recruiting churches and maintaining participant interest for the programme duration. However, each reported higher than average, sustained attendance compared to previous classes. They attributed this increase to a variety of differences including the programme being introduced as a formal class, enthusiasm of church leadership, clinical measurements taken and participants wanting to be good partners.
Resources to implement the peer support component
Lay leaders all stated their congregants enjoyed gathering in groups for class. Lay leaders at two of the churches felt they would have liked to taper to monthly classes before moving directly to independent dyads. One leader stated she would have been comfortable running the classes on her own. Each lay leader also stated they had the internal resources, either a health ministry or healthcare professionals, to run the programme independently.
Suggested improvements to peer support implementation
Nutrition educators and lay leaders stated partnering earlier in the programme might have made it easier for participants to work with a partner on achieving health goals. Lay leaders also talked about the need for additional log sheets and the challenges related to paperwork.
Preliminary health outcomes
Baseline health status
Descriptive statistics at baseline revealed no significant differences in demographic characteristics, biometrics, fruit and vegetable intake or physical activity between those who completed the programme (n = 62) and those who did not (n = 18) (Table 2). Therefore, all the analyses focus on programme completers.
Changes in health outcomes from baseline to 18 weeks
Small but significant changes in fruit intake and physical activity were observed from baseline to week 18 (Table 4). Daily average fruit intake increased an average of 0.06 servings (95% CI = 0.027, 0.093; p = .001) for each week of the programme, which was an average increase of 1.1 servings from weeks 1 to 18. Fruit consumed in the last 24 hours also increased by an average of 0.06 servings (95% CI = 0.013, 0.098; p = .0113) each week of the programme, which was an average increase of 1.1 servings from weeks 1 to 18.
Fixed effects for preliminary health outcomes from weeks 1 to 18 (n = 62).
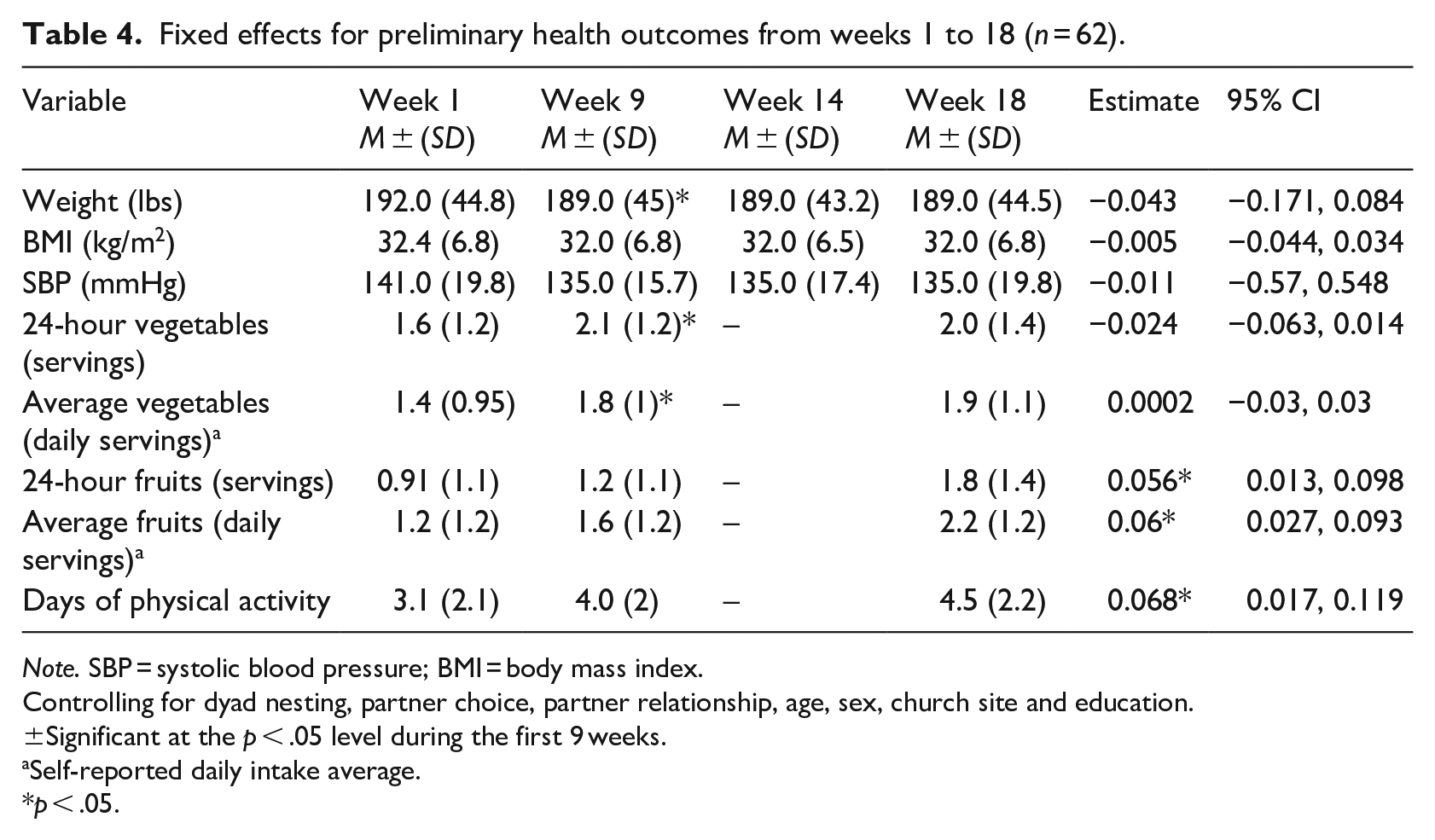
Note. SBP = systolic blood pressure; BMI = body mass index.
Controlling for dyad nesting, partner choice, partner relationship, age, sex, church site and education.
±Significant at the p < .05 level during the first 9 weeks.
Self-reported daily intake average.
p < .05.
Activity level increased significantly by 0.068 days of 30 minutes of activity per week (95% CI = 0.017, 0.119; p = .01), which was an average increase of 1.2 days of exercise from weeks 1 to 18. There were no significant changes in weight, systolic blood pressure, BMI or vegetable intake from baseline to 18 weeks. Eight (21%) of the 39 participants classified as obese at the beginning of the programme had lost at least 5% of their body weight by week 18.
Changes in health outcomes during the first 9 weeks compared to the second 9 weeks
Results showed small but significant increases in vegetable intake and decreases in weight during the first 9 weeks that were maintained during the second 9 weeks. The average number of daily vegetable servings was 0.545 more (95% CI = 0.143, 0.939, p = .008) on average during the first 9 weeks compared to the second. On average, there was a significant 2.6-lb decrease (95% CI = −4.18, −1.1; p = .001) in weight for participants during the first 9 weeks compared to the second 9 weeks. Post hoc analyses indicated that small but significant changes in vegetable intake and weight during the first 9 weeks were maintained during the second 9 weeks.
Discussion
The purpose of this multi-method 18-week prospective study was to evaluate the feasibility of using dyadic peer support to augment an existing healthy lifestyle programme in African American churches. Results indicate participants can improve health outcomes while working with a partner, and it is feasible to implement a dyadic peer support programme to augment an existing health promotion programme within an African American church.
Although only a small number of churches expressed interest, there was no clear indication of dyadic peer support focus affecting recruitment. Although there was concern the programme would be too long and deter faith community members from participating, this was not the case. The biggest challenge cited by faith communities was being unable to accommodate additional programmes. Researchers have documented difficulties in church recruitment for reasons like those stated by organisations in this study (Whitt-Glover et al., 2016). Thus, it is important to be aware of the best timing to start a programme based on the faith community’s calendar. Communities that express a need for the programme should be prioritised.
In terms of data collection feasibility, participants were able to discuss health topics with their partner and track how often they communicated. Similarly, they successfully logged their nutrition and physical activity. While 67% of participants submitted all their logs, lay leaders mentioned sometimes having to make extra copies due to participants misplacing them. Anecdotally, some participants stated they were already tracking their ‘steps’ on their phone or watch, which they found easy and convenient. Thus, providing alternate means of tracking and turning in data may improve future data collection.
Participant retention outcomes corresponded to other health promotion programmes (Lemstra et al., 2016). Programme completion rate for this study was 78%, and the average number of classes attended was 9 of 12 (75%) (Williams et al., 2015). Most participants (95%) who were part of a dyad completed the programme, which is comparable to completion rates seen in other dyadic healthy lifestyle studies (Aschbrenner et al., 2016; Leahey and Wing, 2012; Samuel-Hodge et al., 2017). This may be due to having additional accountability while working with a partner, or reflect only the most dedicated participants remained after the first 9 weeks.
Feasibility surveys showed, as in other dyadic studies (Aschbrenner et al., 2016; Heisler, 2007), participants enjoyed having a partner and found it easy to work with a partner. Pairs were able to communicate at least twice weekly on average and 67% tracked and turned in their logs. Pairing with a friend, compared to a family member or acquaintance, was associated with a higher feasibility score. Practitioners implementing church-based peer support programmes should consider encouraging participants to think about pairing with friends over family members.
Importantly, nutrition educators who regularly implement health education programmes in faith communities felt adding dyadic peer support was feasible and helpful. One recommendation by educators and lay leaders was to create dyads earlier in the programme to start working on goals earlier, an approach other dyadic studies have taken (Heisler, 2007; Sorkin et al., 2014).
Existing studies demonstrate peer support helps participants improve physical activity (Baruth et al., 2013) and fruit and vegetable consumption (Thomson et al., 2014). Similarly, in this study, participants made ongoing improvements in both physical activity and fruit intake over the whole 18 weeks. Changes in fruit serving intake were small (0.4–1 servings) but significant and reflective of other church-based health promotion programmes (Allicock et al., 2013; Resnicow et al., 2004). In this study, weight loss was small, but significant (−2.89 lbs, p < .05) during the first 9 weeks. Changes in weight, as well as improvements in vegetable consumption achieved during the first 9 weeks, were maintained during the second 9 weeks. Therefore, it is possible augmenting programmes with a dyadic peer support component may also improve maintenance and should be explored in future randomised controlled studies.
Notably, participant engagement was high and translated into clinically significant results in weight loss, nutrition and physical activity. For instance, a 5% or more decrease in body weight was achieved by 21% of obese participants, which reduces the risk of insulin resistance and cardiometabolic disease (Swift et al., 2016).
Limitations
There were several limitations to this study. This was a feasibility study and did not utilise control groups. Changes may have occurred regardless of whether an intervention or dyadic peer support component was implemented. However, results from other studies suggest a dyadic peer support component may help maintain behaviour change when used to augment time and labour-intensive health promotion programmes (Tang et al., 2014). To fully explore dyadic peer support’s potential to help participants maintain or improve health behaviours, additional studies including control groups are needed.
This study took place in three different faith communities with different nutrition educators. These differences could have influenced outcomes and perceptions of feasibility. However, church site was controlled for in analysis of biometric, diet and exercise outcomes. In addition, participant interview results were similar across locations, indicating no difference in perceptions of feasibility despite different educators or church communities.
Third, this study relied on self-reported measures of physical activity, dietary intake and height. To decrease recall bias, participants were encouraged to track activity and intake daily. The principal investigator also measured weight and was able discuss any height estimates that appeared inaccurate. Finally, restricting the study to churches in North Carolina limits the ability to generalise results to other geographic areas.
Conclusion
More effective community-based healthy lifestyle promotion programmes targeting African Americans are needed. Approaches incorporating dyadic peer support, an accessible community resource, may help. This study leverages existing relationships and resources within the church community, which may reduce the technical and financial assistance needed for programme implementation, support programme sustainability and, ultimately, optimise health outcomes. This study indicates dyadic peer support is a feasible approach to support healthy lifestyle promotion and chronic disease prevention. Another study with a larger sample size and the inclusion of control groups could further elucidate the value of peer support for improving and sustaining outcomes.
Footnotes
Acknowledgements
The authors acknowledge the community partners, nutrition educators and faith communities who participated in this study.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: this study was supported by an F31 Training Grant from the US National Institutes of Health, National Institute of Nursing Research.