
Abstract
Objective:
We aimed to determine if serum biochemical and MRI biomarkers differed between high volume (≥ 230 texts sent/day; n = 5) and low volume (≤ 25 texts sent/day; n = 5) texters. A secondary aim was to ascertain what correlations between the biochemical and imaging biomarkers could tell us about the pathophysiology of early onset tendinopathies.
Background:
Text messaging has become widespread, particularly among college-aged young adults. There is concern that high rates of texting may result in musculoskeletal disorders, including tendinopathies. Pathophysiology of tendinopathies is largely unknown.
Method:
Ten females with a mean age of 20 were recruited. We examined serum for 20 biomarkers of inflammation, tissue degeneration, and repair. We used conventional MRI and MRI mean intratendinous signal intensity (MISI) to assess thumb tendons. Correlations between MISI and serum biomarkers were also examined.
Results:
Three high volume texters had MRI tendinopathy findings as did one low volume texter. Increased serum TNF-R1 was found in high volume texters compared to low volume texters, as were nonsignificant increases in MISI in two thumb tendons. Serum TNF-R1 and TNF-α correlated with MISI in these tendons, as did IL1-R1.
Conclusion:
These results suggest that early onset tendinopathy with concurrent inflammation may be occurring in prolific texters. Further studies with larger sample sizes are needed for confirmation.
Application:
High volume texting may be a risk factor for thumb tendinopathy in later years. Multidisciplinary research using biochemical and imaging biomarkers may be used to gain insight into pathophysiological processes in musculoskeletal disorders.
Keywords
Introduction
Text messaging and data transmission through mobile devices have dramatically increased worldwide. In the United States, between December 2006 and June 2008, the number of text messages sent increased more than 400% to 75 billion text messages per month (CellSigns, 2009). In the third quarter of 2011, text messaging services were most commonly used among 13- to 17-year-olds (3,417 texts/month), and to a lesser extent among 18- to 24-year-olds (2,842 texts/month; Nielsen Company, 2011).
The global rapid adoption of text messaging has raised concern that high volumes of this activity could lead to musculoskeletal disorders (MSDs). A growing number of case studies have identified tendonitis, tenosynovitis, and first carpometacarpal arthritis among individuals sending a high volume of text messages (Menz, 2005; Ming, Pietikainen, & Hanninen, 2006; Storr, de Vere Beavis, & Stringer, 2007). Several small-scale studies have shown associations of neck, shoulder, or hand symptoms with daily number of text messages sent or duration of manual mobile device usage (Berolo, Wells, & Amick, 2010; Gold, Kandadai, & Hanlon, 2009).
However, little is known about the pathophysiology of MSDs, particularly in tendon disorders. Several studies have detected biomarkers of inflammation in serum of patients that are newly diagnosed with MSDs (Carp, Barbe, Winter, Amin, & Barr, 2007; Rechardt et al., 2011). It would be of interest to identify biomarkers of MSDs early during their development so that individuals could take preventative measures against possible progression.
Pathology in tendon disorders may be visualized in magnetic resonance images (MRI) through the quantitative measure of increased intratendinous signal intensity, as compared with tendons in control subjects (Berquist, 2000). Signal intensity correlates with a qualitative (conventional) MRI grading system of tendinopathy severity (Khan et al., 2003). In a validated technique based on MR images (Shalabi, Movin, Kristoffersen-Wiberg, Aspelin, & Svensson, 2005), mean intratendinous signal intensity was found to be greater in the symptomatic Achilles tendon than in the asymptomatic contralateral tendon (Gardin, Bruno, Movin, Kristoffersen-Wiberg, & Shalabi, 2006). An increase in mean intratendinous signal is a result of the presence of fluid in the tendon. It is not known whether this represents inflammatory exudate, neovascularization, or both. Intratendinous signal has also been interpreted as mucoid degeneration and granulation tissue (Potter et al., 1995; Williams et al., 2001).
By examining serum biomarkers of inflammation and degeneration and quantitative MRI parameters, simultaneously, we may glean information as to the origin of increased mean intratendinous signal intensity in MRI studies of tendinopathy. Therefore, we applied quantitative MRI techniques to two thumb tendons involved in texting, specifically, the flexor pollicus longus (FPL) and extensor pollicus longus (EPL). We hypothesized that the high volume texters would show elevations in serum inflammatory cytokines. We further hypothesized that high volume texters would be more likely than low volume texters to be in the early stages of tendinopathy, and would demonstrate MRI-detectable increases in mean intratendinous signal, and that MRI findings would correlate with serum findings. Hence, our objective was to determine if the following differed between high and low volume mobile phone texters in college-age subjects: (a) serum biomarkers of inflammation, repair, and tissue degeneration; (b) conventional qualitative MRI findings for the FPL and EPL; and (c) mean intratendinous signal intensity of the FPL and EPL, as determined through MRI. Last, correlative statistics between serum biomarkers and quantitative MRI parameters were gathered to gain insight into pathomechanisms of early tendinopathy.
Method
Participant Recruitment and Selection
The Temple University Institutional Review Board approved this study protocol, and all eligible study subjects signed informed consent forms prior to the onset of the study. Potential subjects responded to email and poster solicitations by filling out a web-based questionnaire. Subjects were divided into high and low volume texters based on their answer to the question, “On an average day, how many text messages do you send from a mobile device (e.g., cell phone or PDA)?” Those sending 230 or more texts/day were regarded as high volume texters, whereas those sending 25 or fewer texts/day were considered low volume texters. Also for inclusion, subjects were required to use their right thumb in texting. Potential subjects were asked how long they had been using a mobile device to send text messages.
Respondents with the following were excluded from further consideration to avoid confounding factors for the serum markers of inflammation and degeneration, and for safety assurance in the MRI procedure: musculoskeletal injury or surgery within the past 4 weeks, a diagnosis of rheumatoid arthritis, tendonitis in regions other than in the hand or wrist, autoimmune or metabolic disorders, cancer, cardiovascular or pulmonary disease, pregnancy, and the presence of any metallic foreign bodies. In addition, potential participants were excluded if they reported continuous pain in the shoulder, wrist, or hand and/or musculoskeletal discomfort greater than 3 on a 1–10 pain scale to avoid enrolling subjects with more than mild MSDs.
Individuals who fulfilled these selection criteria were contacted and asked to bring their latest phone bill to investigators to verify their texting volume status. Five high volume texters were recruited to the study. Five low volume texters, matched on age and gender, were also recruited. Subjects were advised to restrict their intake of any anti-inflammatory medications to 3 days prior to their scheduled MRI/blood draw appointment.
Serum Biomarkers
Seven ml of blood was taken from an antecubital vein on the left arm of the subject by a certified phlebotomist. Blood samples were coded with a participant ID number, placed on ice, and transported to Dr. Barbe’s laboratory by an investigator trained to transport blood samples by Temple University’s Environmental Health and Radiation Safety Office. Each sample was centrifuged at 1,000 revolutions per minute for 20 minutes at 4°C. Serum was transferred to cryovials, flash-frozen, and stored at −80°C until analyzed. After collection of samples from all subjects, the samples were assayed undiluted as well as at 1:2 dilutions using customized multiplexed enzyme-linked immunosorbent serologic assays (ELISA) made by Aushon Searchlight Biosystem (Billerica, MA) for the following 20 analytes: (a) six proinflammatory cytokines and receptors: interleukin (IL)-1β, IL-8, IL-R1, tumor necrosis factor (TNF)-α, TNF-R1, and osteoprotegerin (OPG; a member of the TNF-α receptor superfamily); (b) two inflammatory chemokines: monocyte chemotactic protein (MCP)-1 and macrophage inflammatory protein (MIP)-1a; (c) two cytokine inhibitors: IL-1RA and IL-RII; (d) one inflammatory mediator: cyclooxygenase (COX) 2; (e) three repair markers/growth factors: fibronectin, vascular endothelial growth factor (VEGF), and TGF-β1; and (f) five markers of tissue degradation: matrix metalloproteinase (MMP) 2, MMP3, MMP8, MMP13, and capthesin D. Also, one neurotransmitter associated with mediation of pain, substance P, and the chemokine, MIP2, were tested in Barbe’s laboratory using undiluted samples on single-plex ELISA (Invitrogen Biosource), according to the manufacturer’s directions. All samples were analyzed on the Aushon Searchlight Biosystem multiplex kit, as well as on the single plex ELISA kits from Invitrogen Biosource, in single batches to reduce potential interassay variability, as well as in duplicate, in a blinded fashion. Results of the duplicate analyses were averaged to also reduce potential interassay variability, as part of standard practice for ELISA assays. Results of the undiluted sample assays as well as the assays using 1:2 dilutions were compared to determine if there were matrix effects for the multiplex ELISA kits. A matrix effect for anti-TNFalpha was observed; therefore, the 1:2 results for anti-TNFalpha was used for the statistical analyses. For each set of ELISA kits, signal outcomes were compared to known standards that consisted of known amounts of each protein being assayed, as well as standards for water and for the buffers used, for a total of 12 standards tested per kit. Curve fitting math was used to match signal outcome to these standards, and then to an extrapolated pg/ml value of the analyte of interest to determine validity of the detected signals. The LLOQ (lower limit of quantitation) was determined, and samples at or below the LLOQ were considered as undetectable values and were regarded as 0.00 in data analysis. Data are presented as median pg of analyte per ml of serum ± interquartile range (IQR).
MRI Protocol
A Verio 3 Tesla MRI scanner (Siemens Medical Solutions USA, Inc., Malvern, PA) was used to obtain images of the participants’ right hand and wrist. A 12-channel coil routinely used for clinical imaging was used for imaging the hand and wrist. Sagittal images were obtained with the following pulse sequences: T1-weighted spin-echo sequence (repetition time [TR] = 700 ms, echo time [TE] = 21 ms, field of view [FOV] = 130 mm, scan time = 2:12 min, pixel size: 0.4 × 0.3 × 3.0 mm), T2-weighted fast spin echo (TR = 4500 ms, TE = 85 ms, FOV = 130 mm, scan time = 3:40 min, pixel size: 0.4 × 0.3 × 3.0 mm), and PD (proton density)-weighted spin-echo (TR = 1300 ms, TE = 37 ms, FOV = 160 mm, scan time = 6:51 min, pixel size: 0.6 × 0.5 × 0.6 mm). The PD image was utilized for quantitative MRI analysis, since it has been shown to be the most reliable protocol for measuring mean intratendinous signal intensity (Shalabi et al., 2005). Three to five sequential sagittal images were acquired to cover the entire tendon widths of the EPL and FPL tendons.
MRI Qualitative Analysis
A board-certified musculoskeletal radiologist (S.A.) with experience in interpreting musculoskeletal MRIs reviewed the MR images for tenosynovitis, tendinitis, joint effusion, muscular strain, carpal tunnel syndrome, arthritis, myocitis, and ligamentous sprain, according to standard clinical practices. Mild, moderate, or severe and the digit affected (where appropriate) was specified. The radiologist was blinded to subject exposure and symptom status. The number of findings per subject were summed.
MRI Quantitative Analysis
All MR images were transferred to a computer with Analyze software (Biomedical Imaging Resource, Mayo Clinic, Rochester, MN). This software was used to calculate EPL and FPL mean intratendinous signal intensity based on a region of interest (ROI) drawing on PD-weighted images. Two blinded researchers separately defined the ROI using a semiautomatic segmentation algorithm. First, the tendon location was demarcated from the tendon insertion to the level of the mid-metacarpal on the PD image. Then, tendon segmentation was accomplished through a 3D seed growing technique. A board-certified musculoskeletal radiologist (S.A.) independently reviewed the ROI across all slices and made manual adjustments as necessary to refine the location of the EPL and FPL tendons (Figure 1). Once the ROI was established, the mean intratendinous signal intensity was automatically calculated by the Analyze program.

A sagittal proton density weighted MRI image of the thumb showing regions of interest drawn around the flexor pollicis longus (FPL) tendon (short arrows), and the extensor pollicis longus tendon (long arrows). The regions of interest are drawn from the mid-metacarpal to the tendon insertion on the distal phalanx.
Noise was measured using a circular ROI (area = 350 mm2) drawn outside the FOV of the image (air area). The MISI (mean intratendinous signal-to-noise ratio) was determined by dividing the mean intratendinous signal intensity by the standard deviation of the noise. For each of the EPL and FPL MISI parameters, the average of the two researchers’ calculated values was used in data analysis.
Statistical Analysis
Results are reported as median and IQR. The Wilcoxon rank sum test was utilized to evaluate mean differences in the non-normally distributed variables of interest between high and low volume texters. To determine if there was a difference in number of MRI findings between texting groups, the Fisher’s exact test was used. Correlation between serum biomarker concentrations and MISI in each of the tendons was assessed with the Spearman rank correlation coefficient. A p value less than or equal to .05 was regarded as statistically significant.
Results
Subject Demographics
Ten females were recruited to the study, with a mean age of 20 years (range = 18–22). For high volume texters (n = 5), the median number of text messages sent/day was 356 (range = 236–506). Low volume texters (n = 5) sent a median of 19 text messages/day (range = 10–25). All reported using a mobile device to send text messages for 5 or more years. Two of the subjects were left-hand dominant.
Serum Biomarkers
Serum TNF-R1 levels were higher in high volume texters than low volume texters (Wilcoxon rank sum test, p = .05; Table 1). Although not statistically significant, IL-1β showed a trend toward being higher in low volume texters (p = .09), whereas IL1-R1 and IL1-RA showed a trend toward being higher in high volume texters (p = .08, each; Table 1). MCP-1 was also higher in high volume texters, though not significantly (p = .11). All other analytes tested were either not significantly different between the two groups or were below levels of detection.
Serum Biomarker Concentrations in High and Low Volume Texters (n = 10)
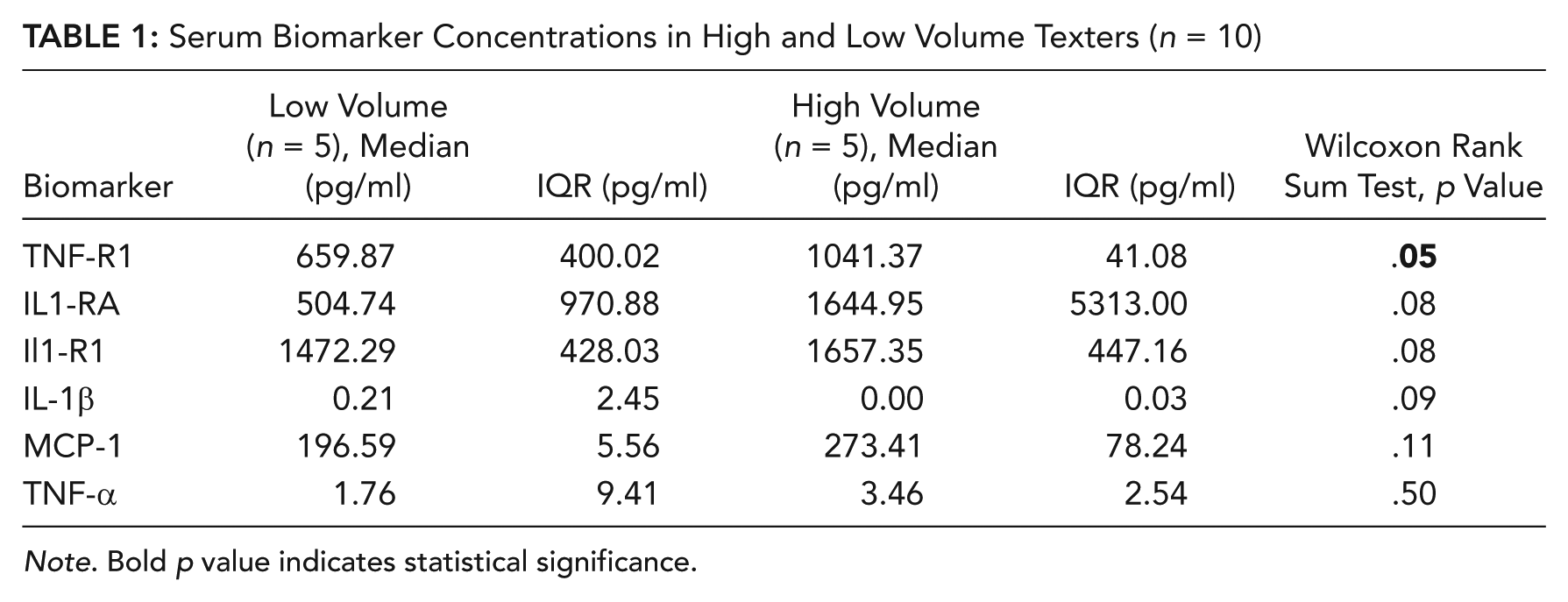
Note. Bold p value indicates statistical significance.
MRI Qualitative and Quantitative Findings
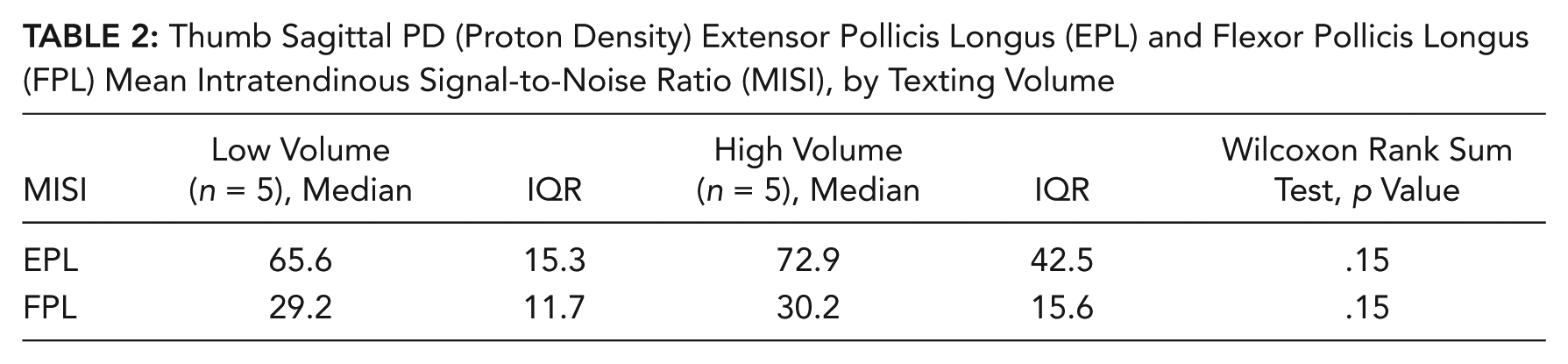
Four of the ten subjects (40%) had MRI findings of tendinopathies. Three of five (60%) of the high volume texters had findings of tendinopathy, as did one of the five (20%) low volume texters. However, the difference in number of findings between the two groups was not statistically different (Fisher’s exact test, p = .26). Specifically, the 3 high volume texters exhibited mild FPL tenosynovitis, as did the one low volume texter with findings of tendinopathy. One high volume texter was scored as having mild tenosynovitis in their extensor carpi radialis brevis (ECRB), extensor carpi radialis longus (ECRL), and flexor pollicis longus (FPL). The mean intratendinous signal-to-noise ratio was greater in the EPL and FPL tendons of high volume compared to low volume texters. However, these differences were not statistically significant (Table 2; Figure 2).
Thumb Sagittal PD (Proton Density) Extensor Pollicis Longus (EPL) and Flexor Pollicis Longus (FPL) Mean Intratendinous Signal-to-Noise Ratio (MISI), by Texting Volume

Coronal fat-saturated fast spin echo (FSE) T2-weighted MRI image of the thumb showing the flexor pollicis longus (FPL, black arrow) and tenosynovitis around that tendon (white arrows).
Correlations Between Serum Biomarker Concentrations and MRI Quantitative Findings
Serum levels of TNF-R1 were positively correlated with EPL MISI (Spearman rank correlation coefficient = .70, p = .03), and with FPL MISI (Spearman rank correlation coefficient = .62, p = .05). EPL MISI was also positively correlated with serum levels of IL1-R1 (Spearman rank correlation coefficient = .62, p = .05) and TNF-α (Spearman rank correlation coefficient = .66, p = .04). In contrast, MISI EPL was negatively correlated with TGF-B1 (Spearman rank correlation coefficient = –.065, p = .04). No other correlations between serum biomarker and quantitative MRI variables had a p value < .05.
Discussion
In this pilot study, we hypothesized that high volume texters would show elevated serum levels of inflammatory biomarkers, MRI-detectable tendinopathy, as well as increased mean intratendinous signal in thumb tendons. Increased serum levels of TNF-R1, a receptor for TNF-α, were found in high volume texters compared to low volume texters of college age. Nonsignificant increases in mean intratendinous signal-to-noise ratio, particularly in the EPL tendon, were present in high volume texters compared to low volume texters. In addition, serum TNF-R1 and TNF-α correlated with the mean intratendinous signal-to-noise ratio in EPL and FPL tendons. IL1-R1 also correlated with EPL MISI.
Our serum findings of increased TNF-R1 in high volume texters provide evidence of an early inflammatory phase in these subjects. We also observed trends toward increased IL-1RA and IL-1R1 in high volume texters. These findings are similar to a recent study where increased serum IL-1RII was found in association with newly diagnosed upper extremity MSDs (Rechardt et al., 2011). They also observed increased serum IL-18 in association with newly diagnosed MSDs, a serum analyte that was not available for testing through our commercial testing source. We did not find an increase in serum IL-1RII in either group in our study, perhaps because our subjects were asymptomatic or comparatively less symptomatic than the subjects with increased IL-1RII in the Rechardt et al. (2011) study, each of which had sought medical advice for either a symptomatic upper-limb disorder or for nonspecific upper-limb pain.
The significant increase in TNF-R1, but lower increase in TNF-α compared to its receptor, is likely a result of the difference in clearance kinetics of cytokines as compared to their receptors (Bemelmans, van Tits, & Buurman, 1996). TNF is cleared rapidly from the blood stream, as a result of binding to TNF receptors (Bemelmans et al., 1996; Bemelmans, Gouma, & Buurman, 1994). TNF receptors are responsible for neutralizing circulating TNF and aid in its rapid clearance via the kidney (Bemelmans et al., 1996; Terlizzese, Simoni, & Antonetti, 1996). In contrast, soluble TNF receptors are continuously released and shed into the circulation, and have increased retention periods in the blood stream (Bemelmans et al., 1994; Terlizzese et al., 1996). Similarly, Rechardt and colleagues (2011) observed increased concentrations of an IL-1ß receptor, the soluble IL-1RII, yet not of IL-1ß itself in MSD patients.
Of interest, we observed nonsignificantly increased levels of serum IL-1β in the low volume texters in our study. If one assumes that we adequately restricted our study population to eliminate other potential conditions that would cause elevated serum IL1-β, and that our subject groups only differed on texting status, we can infer that low volume texting also produces an inflammatory response. It is hard to infer more, however, because of the small number of subjects in this study and the low level of serum IL1-β detected.
A high MISI indicative of fluid in two right thumb tendons was associated with higher serum levels of two inflammatory receptors (IL1-R1 and TNF-R1), one inflammatory cytokine (TNF-α), and lower levels of a tissue repair protein (TGF-β1). These increased serum inflammatory markers in association with increased MISI suggests that the increase in the latter is reflective of edema caused by inflammation, although we cannot rule out the possibility of concurrent hyperplasia. The inverse correlation with TGF-β1 suggests that a repair and adaptation process had down-regulated, perhaps because of the concurrent inflammatory response, which was most evident in high volume texters. We hypothesize that there was sufficient recovery time after exposure in the low volume texters for any repair mechanism involving TGB-β1 to operate satisfactorily. However, in the high volume texters, the recovery time appeared to be insufficient, at least in the current study.
Although mild FPL tenosynovitis was a finding in three of the five high volume texters and in one of the low volume texters, none of the ten subjects exhibited EPL tendinopathy in conventional MRI analysis. The correlations that we found between EPL tendon MISI and serum biomarkers were observed using quantitative MRI measures. Perhaps the changes were too small in the EPL tendon in these young, asymptomatic or mildly symptomatic subjects, to detect with conventional MRI analysis. Inclusion of subjects meeting a case definition or diagnostic criteria for tenosynovitis in future studies could better address this question.
One strength of this study was our multidisciplinary approach. To our knowledge, we are the first group to combine serum biomarker analysis with quantitative and qualitative MRI analyses for the assessment of MSD pathophysiology. Also, the study exposure (number of text messages sent per day) was verified objectively, using a potential subject’s phone bill to confirm exposure status. Third, we are reasonably confident that we excluded potential subjects with medical conditions that would have influenced the outcome variables that we examined. Furthermore, the levels of TNF-a, IL-1b and IL-1RA observed in this study are comparable with previously published levels for healthy adults with no signs of hypertension, and an absence of trauma (Carp, Barr, & Barbe, 2008; Carp et al., 2007; Nieman et al., 2006; Panagiotakos, Pitsavos, Yannakoulia, Chrysohoou, & Stefanadis, 2005; Ridker, Cushman, Stampfer, Tracy, & Hennekens, 1997; Svoboda, Kantorova, & Ochmann, 1994). This suggests that the increases observed are unlikely to be attributable to these factors.
However, there are several limitations as well. Our small sample size in this pilot study restricted our ability to detect variable differences between low and high volume texters. In addition, since other hand-intensive exposures (such as conventional computer and laptop use, and video game playing) and other thumb-intensive exposures (such as pipetting) were not ascertained in study subjects, it is possible that the changes observed cannot be solely attributed to the daily volume of text messages sent. Although the latency in serum of several of the biomarkers that we examined has been investigated in response to high level exercise (e.g., Marklund et al., 2013; Peake, Nosaka, & Suzuki, 2005; Suzuki, Nakaji, Yamada, Sato, & Sugawara, 2002), there is little known about biomarker generation and associated latency after low level activity such as texting. Subjects were not asked to send texts within a specified period before the testing, nor was the period since last text known. We can only speculate that the time since last text was shorter in high volume texters than low volume texters, but as this is not known, it is a potential source of variability in the data. Last, in this cross-sectional study, we cannot be certain that the increased biomarker concentrations and increased MISI in high volume texters did not precede the texting exposure.
In conclusion, we found significant associations between serum TNF-RI and IL-1R1 levels and MRI mean intratendinous signal increases in thumb tendons of texters. The results of this pilot study support the need for further research examining the pathophysiological effects of intensive texting. It would be useful for such future studies to include a comprehensive exposure assessment of hand- (and particularly thumb-) intensive activities, perhaps matching on exposure levels in asymptomatic and symptomatic subjects.
Even though the number of subjects was quite small, we found significantly higher serum levels of an inflammatory receptor, TNF-R1, in college-age texters sending 230 or more messages per day. This increase correlated with an increase in the mean intratendinous signal-to-noise ratio in two right thumb tendons (the EPL and FPL). Increased mean intratendinous signal in these tendons was also directly correlated with serum levels of TNF-α and IL-1R1. These findings support the need for further studies with larger sample sizes to confirm these findings.
Key Points
College students texting at high volumes (≥ 230 texts sent/day) had increased serum TNF-R1, a marker of inflammation, as compared to low volume texters (≤ 25 texts sent/day).
Three of five high volume texters exhibited mild flexor pollicis longus tendinitis MRI findings as did one of five low volume texters.
Inflammatory biomarkers TNF-R1, TNF-α, and IL1-R1 correlated with mean intratendinous signal in thumb tendons, suggesting that early onset tendinopathy with accompanying inflammation is occurring in these texters.
Our multidisciplinary approach (serum and imaging biomarkers) appears promising for MSD pathophysiology assessment.
Footnotes
Acknowledgements
The authors would like to thank Evan McClennan and Indu Dornadula for their assistance with the quantitative MRI measurements. Paul Fisher performed several serum biomarker analyses. We would also like to thank phlebotomists Sheara Williamson and Kohei Kishimoto, and Nadja Thomas and Tanushree Chakravarty for research assistance. Last, we would like to thank Mamta Amin for her management of the serum samples. This work was supported by Temple University funds to Judith Gold and Mary Barbe.
Judith E. Gold is a guest researcher at the Centre for Musculoskeletal Research at the University of Gävle in Gävle, Sweden. She earned her ScD in occupational epidemiology from the University of Massachusetts Lowell in 2003.
Feroze B. Mohamed is a biomedical MRI physicist and associate professor in the Department of Radiology at Temple University. He serves as the associate director of the Functional Magnetic Resonance Imaging Center at Temple University. He earned his PhD in biomedical engineering from Drexel University in 1996.
Sayed Ali is a musculoskeletal radiologist and assistant professor in the Department of Radiology at Temple University. He is the Musculoskeletal Radiology Fellowship Program director at Temple University Hospital. He completed his fellowship in musculoskeletal radiology at Indiana University in 2002, and is certified by the American Board of Radiology.
Mary F. Barbe is a professor in the Department of Anatomy and Cell Biology at Temple University School of Medicine in Philadelphia, Pennsylvania. She earned her PhD in anatomy from Bowman Gray School of Medicine of Wake Forest University in 1987.