
Abstract
Objective:
In a driving simulation, we investigated the efficacy of galvanic cutaneous stimulation (GCS) provided during curves or intermittently during the whole circuit to mitigate simulator syndrome (SS).
Background:
The literature on how GCS decreases SS, although scarce, has demonstrated the effectiveness of this technique. Stimulation with this and similar techniques has usually been provided in curves or continuously during the whole circuit but never intermittently. This stimulation method could generate a continued activation of processes related to GCS mitigating SS.
Method:
Fifteen drivers (8 men; mean age = 25.5 years) participated in this experiment. We compared the total scores of the Simulator Sickness Questionnaire (SSQ) across three stimulation conditions: (a) curve GCS condition, whereby GCS was provided in curves; (b) intermittent GCS condition, whereby GCS was provided intermittently during the whole circuit; and (c) no-stimulation condition, whereby no stimulation was provided (baseline condition).
Results:
The experimental outcomes revealed that GCS decreased SS in both the curve and intermittent stimulation conditions.
Conclusion:
We provide evidence that GCS is an effective countermeasure to decrease SS. It could be applied indifferently in curves or intermittently during the whole circuit.
Application:
For future interventions, we recommend the use of GCS to mitigate SS with similar intermittent stimulation programs. These programs have a crucial advantage as they are easily integrated into the simulator setup without the necessity of generating a complicated experimental design to stimulate during the curves.
Keywords
Introduction
Some drivers experience simulator sickness (SS), a condition in which symptoms similar to motion sickness (MS) are exhibited when driving in a simulator (nausea, disorientation, dizziness, headache, and difficulty focusing). This syndrome is a critical issue for the use of a simulator because it leads to population biases and data loss (Stanney, Mourant, & Kennedy, 1998). The literature on this topic has mainly addressed two issues: the nature and causes of SS and the study of countermeasures to mitigate SS.
The etiology of SS is not completely understood, as it involves different interactions between sensorial, perceptual, cognitive, and motor processes (Riccio & Stoffregen, 1991; Stanney et al., 1998). This not well-known etiology has generated several theories attempting to explain this syndrome and, more generally, MS (see Kennedy & Frank, 1986; Mollenhauer, 2004; and Reed-Jones, 2011, for an extensive review of SS). The aim of this research is not to address these theories but rather to study how it is possible to decrease SS.
For example, galvanic vestibular stimulation (GVS) has been tested as an effective tool for decreasing SS. GVS involves placing the electrodes over the mastoid process, which stimulates the eighth cranial nerve (Bent, McFadyen, Merkley, Kennedy, & Inglis, 2000; Reed-Jones, Vallis, Reed-Jones, & Trick, 2008). Reed-Jones, Reed-Jones, Trick, and Vallis (2007) and Reed-Jones, Reed-Jones, Trick, Toxopeus, and Vallis (2009) applied GVS during curves in fixed-simulator experiments. They found that GVS reduces SS and produces lower vehicular velocities.
Other electrical techniques that have been shown to decrease SS include galvanic cutaneous stimulation (GCS), which will be the focus of this research. GCS entails stimulating superficial cutaneous nerve fibers with a large diameter using an electric current with a relatively short-pulse duration and intensity below the motor threshold. Usually GCS is applied on the neck muscles (mainly the sternocleidomastoids), approximately 3 to 4 cm below the mastoid process (Reed-Jones et al., 2008). GCS impacts cardiovascular autonomic responses (Chu, Li, Juan, & Chiou, 2012; Sanderson et al., 1995), enhances visuospatial abilities and cognitive function (van Dijk, Scherder, Scheltens, & Sergeant, 2002), and more importantly, alleviates SS (Chu et al., 2012). Two studies have assessed the impact of GCS on SS. First, Chu, Li, Huang, and Lee (2013) showed how GCS mitigates SS and improves cognitive processing, such as attention, and performance. Second, Reed-Jones et al. (2009) failed to find a significant effect when comparing GVS, GCS, and no-stimulation groups, although they found an interesting trend toward a lower Simulator Sickness Questionnaire (SSQ; Kennedy, Lane, Berbaum, & Lilienthal, 1993) total score (TS) when GCS was provided. However, vehicular speeds during curves were better negotiated with GVS. They concluded that GCS could be a better technique to reduce SS, whereas GVS could be a better choice in more naturalistic driving tasks.
The first aim of this research is to investigate the advantages of GCS in mitigating SS and to add to the scarce literature demonstrating GCS as an effective countermeasure against SS. The second aim of this research is to provide an alternative to stimulation during curves (e.g., Reed-Jones et al., 2009). Stimulation during curves presents a crucial advantage, as maneuvering curves in the simulator is when the conflict between perception of static and dynamic situations is highest (Kemeny & Panerai, 2003). Nevertheless, experiments in which stimulation is applied during curves demand a difficult setup and a program to synchronize when the stimulation is provided in the circuit. Here, we want to test whether an intermittent stimulation program during the whole circuit could mitigate SS. To test this idea, we will compare SS in three conditions of stimulation: GCS applied during the curves, GCS applied intermittently during the whole circuit, and finally, a base condition whereby no stimulation is provided. It should be noted that we will use similar total times of GCS in the curve and intermittent conditions to rule out this temporal difference as an explicative factor.
An additional aim of this research is to investigate how GCS impacts different driving performance variables to add to the scarce literature on this topic. Previously, Reed-Jones et al. (2009) failed to find a significant effect in driving performance when GCS was provided. We hypothesized that GCS will mitigate SS in curves in line with previous research (Reed-Jones et al., 2009). Moreover, we also hypothesized a decrease in SS when the stimulation was delivered intermittently during the whole circuit.
Method
Participants
Prior to the experiment, possible participants were screened to determine if they had any predisposition to MS. They completed a French version of the Motion Sickness Susceptibility Questionnaire (MSSQ; Golding, 1998). For ethical reasons, we did not include in the experiment participants (only 1 participant) with MSSQ scores higher than 65 (percentile 75) because of the high susceptibility to sickness. The MSSQ mean score for our sample was 45.88 ± 10.52. The participants included 8 men and 7 women (mean age = 25.5 ± 3.2 years). We calculated this sample size using a statistical power analysis program (G*power) for one ANOVA of repeated measures (within factors) with a large effect size, setting statistical significance to α = .05 and a power of .90. In addition, to be included in this study, volunteers should have driven at least 3,000 km the previous year, should not have a pacemaker or a hearing aid, should never have experienced vestibular vertigo, and finally, should not be taking medicines that affect driving. All participants reported normal or corrected-to-normal vision and normal tactile perception. Participants were instructed to refrain from the use of medication, alcoholic substances, and caffeinated drinks for 24 hr before the experiment. Participants were unaware of the purpose of the experiment, received €60 in return for their participation, and gave their signed informed consent. This study was performed in accordance with the ethical advisory internal committee of the research center (the French Institute of Science and Technology for Transport, Development, and Networks [IFSTTAR]).
Apparatus and Stimuli
GCS was delivered using a linear stimulus isolator device (STMISOL; Biopac, Goleta, CA). Stimulation was applied through electrodes (2.5 cm2) placed bilaterally on the neck on the top of the sternocleidomastoid muscles (Reed-Jones et al., 2008).
The study was carried out in an instrumented full-cab fixed-base simulator (Peugeot 308) with sensors on the pedals, wheels, and gearbox. The road scene was projected, in the front, on five screens (220 × 165 cm, 1,024 × 1,280 pixels) representing a 180° horizontal field of view (FOV) and a 40° vertical FOV. The simulator was also equipped with SIM2 virtual reality–based software, which relies on the ARCHISIM traffic model. SIM2 includes tools for creating various experimentation components (databases and files) needed to describe the environment and progress of experiments. A quadraphonic audio system reproduces the sounds related to the vehicle’s instruments (engine, bearing, starter) and the noise outside. This simulator was built by the Laboratory for Road Operations, Perception, Simulators, and Simulations (LEPSIS-IFSTTAR). Driving performance data were captured at 60 Hz (temporal display resolution) from the original equipment. The simulator was also equipped with a CAN-bus system to send/receive information to/from the dashboard.
The virtual environment simulated driving a 7.5-km flat route through an urban environment. The simulated road represented a paved surface with a double lane each way and no median. Each lane was 3.6 m wide with a 2-m sidewalk on both sides. There were buildings (around 20 m high) around the whole circuit on both sides of the sidewalk. Participants negotiated 18 curves (nine lefts and nine rights). The turns consisted of either a gradual 90° turn or a sharp 90° turn. The gradual turns consisted of a 70-m lead-in, a 140-m-long curve, and a 70-m lead-out. The sharp turns were modelled on a T intersection and consisted of a 40-m lead-in with a 40-m-long curve immediately transitioning back into the next roadway. The straight sections of the circuit had a distance between 200 and 300 m. In addition, 40 road marks and 17 traffic signals indicating the direction to follow were presented.
Procedure
Participants performed a driving session to become familiar with the car at the beginning of the experiment. The duration of this urban virtual scenario was about 5 min. After this familiarization, the sternocleidomastoids were swabbed with alcohol to remove dead skin. Electromyography electrodes were applied 3 to 4 cm below the mastoid process, on the cutaneous skin over the sternocleidomastoid muscles. The anode electrode was placed in the right sternocleidomastoid and the cathode electrode in the left sternocleidomastoid. Current output was adjusted to each participant’s threshold to the stimulus, assessed at a range of 0.6 to 1.25 mA following a similar procedure described by Reed-Jones et al. (2008, 2009). More concretely, threshold testing started at 0.05 mA and was increased in increments of 0.05 mA until the threshold was reached. Threshold determination was based on verbal reports of sense of movement and the investigator’s visual observance of very small movement toward the anode electrode. If a particular stimulus level produced an unclear or unsure response, the experimenters increased the level by 0.05 mA and then reduced it again to help confirm the presence and severity of the disturbance. For each participant, the stimulation applied was adjusted to twice the determined threshold. Reed-Jones (2011) pointed out that this procedure provided a comfortable and suitable stimulation strength that produced an effect for GVS in line with previous research (Bent et al., 2000) and replicates the GCS procedure used by Reed-Jones et al. (2008).
The participants were asked to drive in the right lane, to not exceed 90 km/h, and to reduce their speed during curves in order to perform this maneuver efficiently. The participants drove through the simulation three times, corresponding to the three experimental conditions. These experimental conditions (counterbalanced between participants to compensate for any learned behavior) were the following: (a) no stimulation condition, whereby no stimulation was delivered (baseline condition); (b) curve GCS condition, whereby GCS was delivered from 40 m before the curve to the end of the curve; and (c) intermittent GCS condition, whereby GCS was delivered following a program that provided stimulation intermittently in different parts of the circuit (either during curves or in straight sections of the road). This intermittent program was created by taking into account the use of similar total latencies of stimulation in the curve stimulation conditon in order to control for this factor as an alternative explanation to our pattern of data. We computed the time of stimulation for 5 participants in the curve condition during pilot testing. The mean time was 130 s of stimulation and 270 s of resting. Thus, in the intermittent stimulation condition, we applied these latencies of stimulation and resting divided into different temporal intervals assigned randomly per participant (range between 3 and 9 s for stimulation and between 15 and 21 s for resting).
It should be noted that the length of the circuit was 7.5 km, and the maximum velocity allowed was 90 km/h. This design means that if participants perform the circuit in less than 5 min, they do not receive the total 130 s of stimulation and the 270 s of rest time between them. Nevertheless, in the current study, all the participtans completed the circuit in all the conditions in more than 5 min (6.6 ± 1.3 min). Additionally, we analyzed the time of stimulation in both stimulated conditions to ensure that they had similar duration of total stimulation.
After each drive, participants exited the vehicle for a rest period of 5 min and completed their responses to the SSQ (Kennedy et al., 1993) whereby the severity of SS was measured. The questionnaire is composed of 16 symptoms that the participant has to rate on a scale from none (0) to severe (3). We analyzed the SSQ TS provided by the questionnaire in the three stimulation conditions.
Design
The different conditions for delivering the stimulation were manipulated as the independent variable (no-stimulation condition, curve GCS condition, and intermittent GCS condition). The SSQ TS revealed high variance across conditions in line with previous studies (Draper, Viirre, Furness, & Gawron, 2001; Moss & Muth, 2011; Sharples, Cobb, Moody, & Wilson, 2008). Thus, a square root transformation was performed to correct the heterogeneity of variance, using a method similar to Sharples et al. (2008) and Moss and Muth (2011). The resultant data were submitted to an ANOVA of repeated measures (within factor) and planned comparisons to compare the levels of SSQ TS under the different conditions of stimulation.
Driving performance variables were compared between the spatial intervals when participants received GCS in the curve and intermittent GCS conditions and the same spatial intervals in the no-stimulation condition. The driving performance variables measured were average speed, speed variability, steering variability, and lateral position variability. Speed variability was calculated through the standard deviation of speed (measured in km/h). Steering variability was calculated as the standard deviation of the angle of the steering wheel (measured in degrees). Finally, lateral position variability was calculated through the standard deviation of the lateral position of the vehicle with respect to the central axis of the road (measured in centimeters).
The data were submitted to a double analysis. The first assessed the driving performance variables in the curves of the curve stimulation condition versus the curves of the no-stimulation condition (comparison curve vs. neutral). The second compared the stimulated parts of the circuit in the intermittent stimulation condition versus the same segments of the circuit in the no-stimulation condition (comparison intermittent vs. neutral). A t test for related samples was performed for each driving variable per comparison. In order to decrease the overall probability of Type I errors, we included Bonferroni corrections of the significance level in each comparison. Thus, we declared a result to be significant when the p level is less than 0.05/4 = 0.0125 (4 was the number of t tests per comparison). As pointed out in the procedure, we added an additional t test for related samples whereby we compared the total time of stimulation in curve and intermittent stimulation conditions to rule out this factor as a potential explanation for our results.
Results
Table 1 shows the means and medians of SSQ TS (without a square root transformation) in the three conditions of stimulation. In addition, the number of sick participants under the three conditions of stimulation is presented. According to the criterion of Webb et al. (2009), SSQ scores greater than 20 (without a square root transformation) indicate that participants are sick. All the participants were sick under the no-stimulation condition, 10 participants were sick under the curve GCS condition, and 9 participants were sick under the intermittent GCS condition. These data will be considered in the discussion.
Simulator Sickness Levels by Stimulation Condition
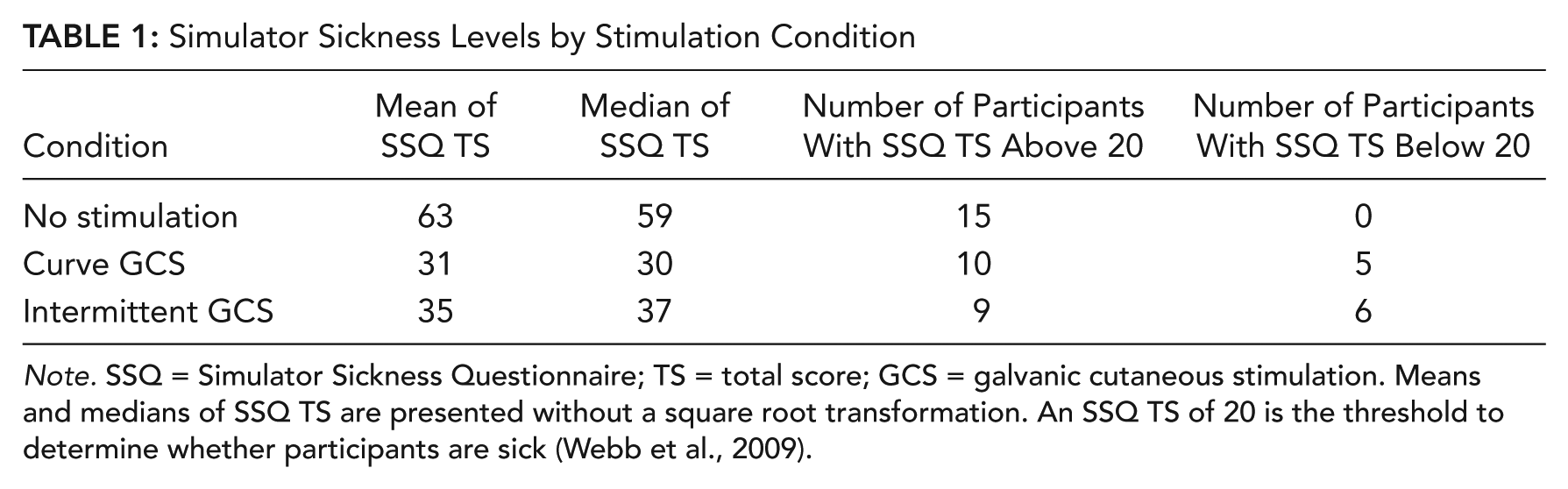
Note. SSQ = Simulator Sickness Questionnaire; TS = total score; GCS = galvanic cutaneous stimulation. Means and medians of SSQ TS are presented without a square root transformation. An SSQ TS of 20 is the threshold to determine whether participants are sick (Webb et al., 2009).
For SSQ TS (after a square root transformation; see Figure 1a), a significant effect for the experiment condition was found, F(2, 28) = 11.3890, p = .0002, η2 = .67, with significantly higher scores in the no-stimulation condition (7.7) compared to the curve GCS condition (4.9; p = .0009) and intermittent GCS condition (5.5; p = .0032). There were no differences between curve GCS condition and intermittent GCS condition (p = .2993).
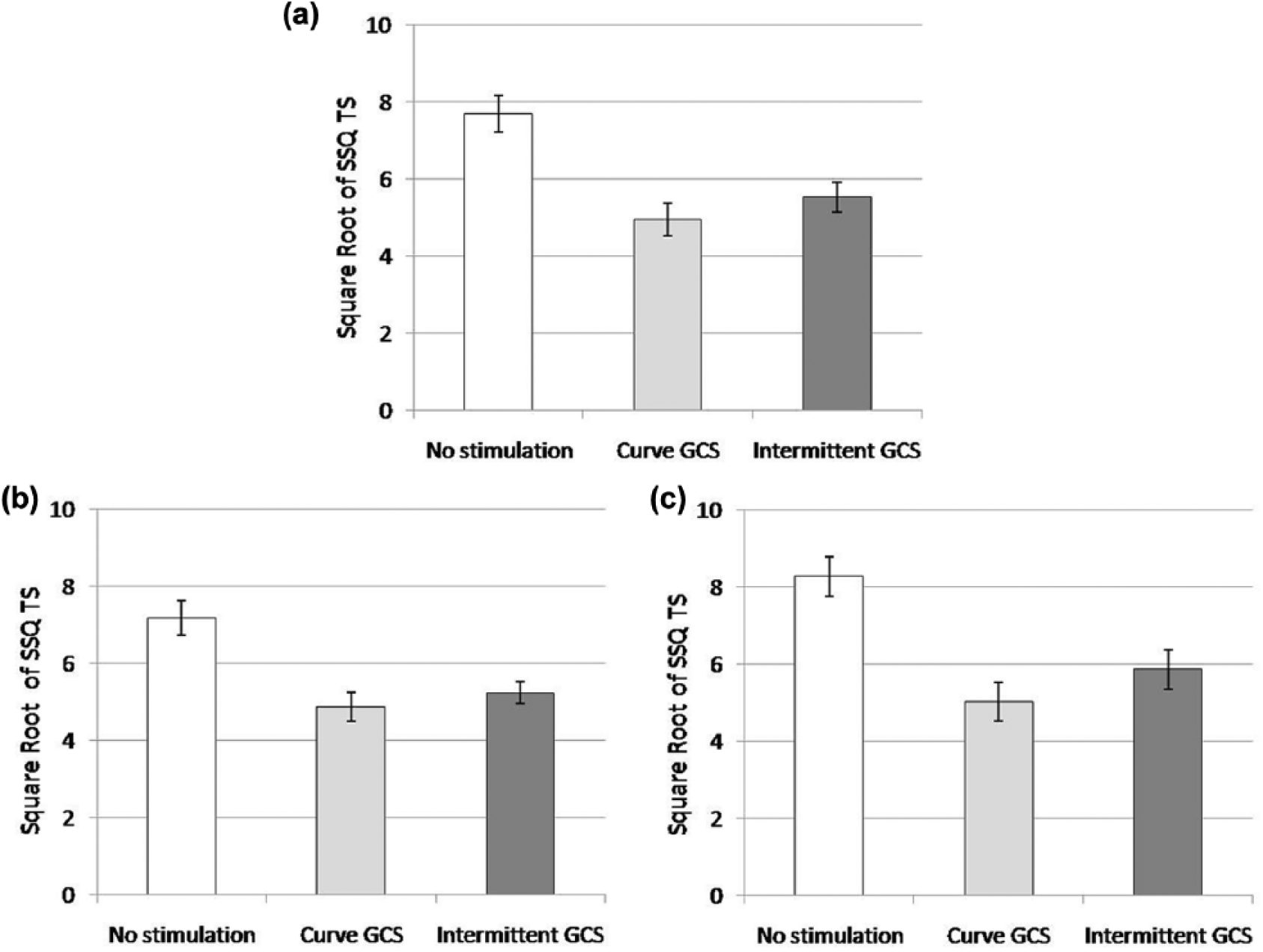
Means and standard errors of Simulator Sickness Questionnaire total score after a square root transformation in the three conditions of stimulation. The maximum possible score after a square root transformation is 15.35. Standard errors have been corrected for within-subject studies (Morey, 2008). (a) Total sample. (b) Male sample. (c) Female sample.
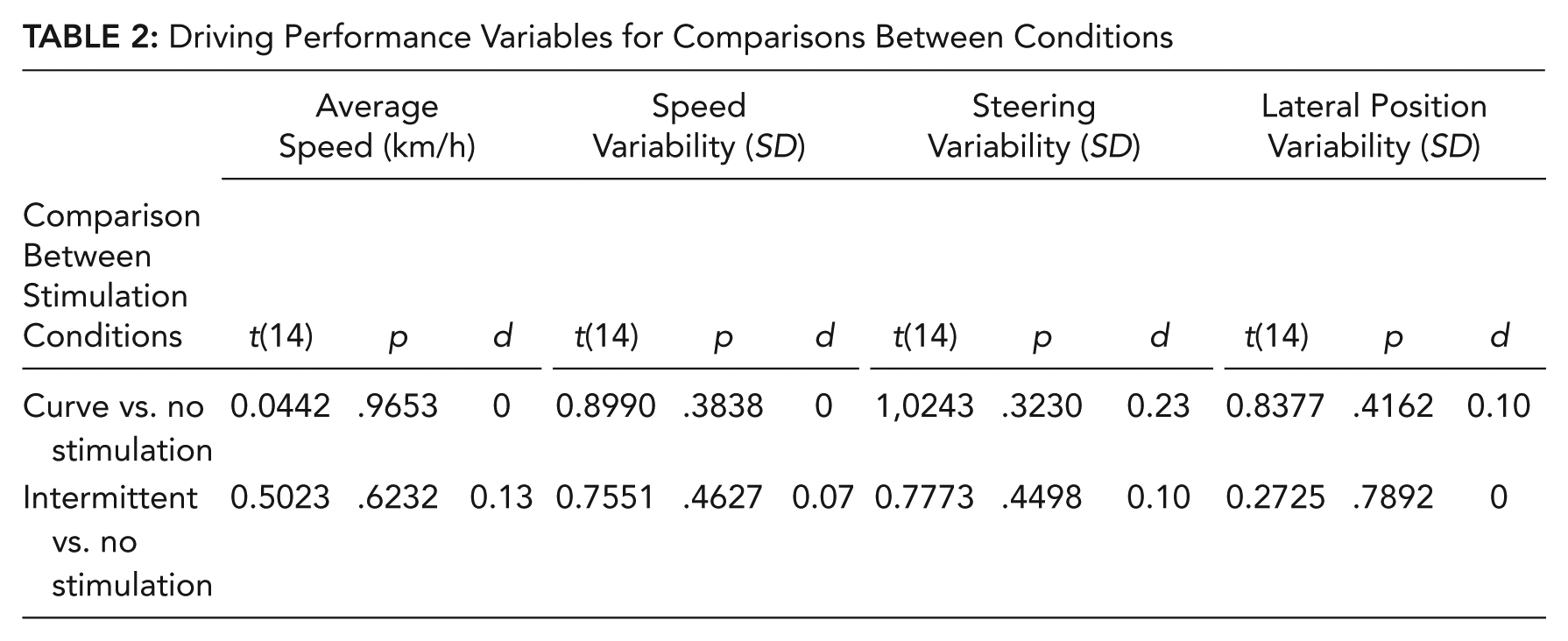
When comparing the duration of stimulation across curve (122 s) and intermittent GCS conditions (120 s), we did not obtain any differences in stimulation, t(14) = 0.22, p = .8274, d = .08. The data for driving performance are presented in Table 2. We did not find any differences in the curve versus no-stimulation conditions and the intermittent versus no-stimulation conditions regarding average speed, speed variability, steering variability, or lateral position variability (see Table 2).
Driving Performance Variables for Comparisons Between Conditions
Discussion
This research had two aims. First, we wanted to test the efficacy of GCS as a countermeasure to decrease SS in line with previous research (Chu et al., 2013; Reed-Jones et al., 2009). Second, we wanted to ascertain whether intermittent stimulation during the whole circuit could mitigate SS due to continued activation of mitigation processes related to GCS. In addition, we wanted to investigate how GCS impacts different driving performance variables.
The results confirmed that GCS mitigates SS. The decrease of SSQ TS is in line with some previous research. For example, Chu et al. (2013) found significant differences in SSQ TS, whereas Reed-Jones et al. (2009) failed to find a significant effect when comparing GVS, GCS, and no-stimulation groups, although they found a trend toward lower SSQ TS with GCS. Nevertheless, this research demonstrates a mitigation of SS whereby SSQ TS was around 32% lower when GCS was applied. Importantly, this finding does not mean that the participants were not sick in the stimulated conditions. According to Webb et al. (2009), SSQ scores greater than 20 indicate sufficient discomfort (see Table 1), and in our experiment, SSQ TS was above 20 (without the square root transformation) for 10 participants in the curve GCS condition and for 9 in the intermittent GCS condition, whereas under the no-stimulation condition, the 15 participants reported SSQ TS above 20. This finding means that the total sample of participants presented SS symptoms when no stimulation was provided, and although GCS mitigated the SS symptoms, they did not disappear for a considerable percentage of the participants Nevertheless, it should be noted that in any case, a reduction in SSQ TS was found when GCS was applied.
Interestingly, we found that the SSQ TS was higher in our experiment than in previous work with GCS (e.g., Reed-Jones et al., 2009). A possible factor influencing our high SSQ TS could be that participants were driving an urban circuit. Drivers usually present higher SS symptoms in urban rather than in rural circuits due to the number of curves (Edwards, Creaser, Caird, Lamsdale, & Chisholm, 2003; Mourant, Rengarajan, Cox, Lin, & Jaeger, 2007; Park, Allen, & Fiorentino, 2006) and the presentation of more objects in peripheral view (Chrysler & Williams, 2005). One other point that could explain our high SSQ TS is the speed. Mourant and Thattacherry (2000) found that drivers experienced higher SS when they drove at 96 km/h than when they drove at 40 km/h. This result indicates that higher speed leads to higher SS. In our experiment, the participants were asked not to exceed 90 km/h, (although the participants were requested to reduce their speed during curves), driving at a mean of 65.12 km/h across conditions. Thus, this speed could be considered as a high speed for an urban circuit and could have had an impact on the SS symptoms.
It should be noted that there are no other variables in our experiment that affect SS symptoms. For example, some studies have shown that women are more prone to SS (e.g., Allen, Park, Cook, & Rosenthal, 2003; Freund & Green, 2006; Jaeger & Mourant, 2001; Rizzo, Sheffield, Stierman, & Dawson, 2003) but not all (e.g., Kolasinski & Gilson, 1998; Mourant et al., 2007). Our sample was almost equal regarding gender (8 men and 7 women), and thus this factor can be ruled out in explaining the high SS scores. Nevertheless, as seen in Figures 1b and 1c, there was a trend toward higher SSQ TS for women in the no-stimulation and intermittent GCS conditions (we did not perform inferential statistics because the sample was small). This finding could suggest that women could be more prone to SS in line with the aforementioned literature (e.g., Allen et al., 2003).
We found that SSQ TS in the curve and intermittent GCS conditions reduced SS. This finding corroborates our hypothesis that decreasing SS with an intermittent but continued activation during the whole circuit of the process could mitigate SS. These processes could be activated in curves, which is considered the maneuver that produced the greatest discomfort in a simulator, or intermittently but continuously during the whole circuit to reduce SS. However, even when GCS was provided randomly in the intermittent GCS condition, participants could have been stimulated fortuitously with a higher percentage during the curves. We have rejected this possibility, however, because participants received only 7.2% of the total GCS time during the curves in the intermittent condition; in other words, they received 92.8% of the total stimulation time during straight sections of the circuit.
The driving performance variables showed no difference between the no-stimulation condition and the curve GCS condition or intermittent GCS condition. This finding is in line with previous literature that did not show any significant differences in driving performance variables when GCS was applied (Reed-Jones et al., 2009). In any case, it is important to note that GCS did not adversely affect any driving variable; this is a fundamental point for the recommendation of GCS for future interventions reducing SS. Finally, we want to remark that although participants had lower SS, they drove no better. New studies must be done to explore this finding.
The current study has several limitations due to its novelty. We strongly believe that further research must be performed to replicate and generalize our results and conclusions across different populations, cohorts, scenarios, and simulators.
In conclusion, this research has provided evidence regarding the benefits of using GCS to mitigate SS without any negative effects on driving performance, and we thus recommend its use in future experiments. The beneficial effects of GCS should aid researchers when implementing best practice for their participants receiving simulator-based training. Future interventions involving this technique could apply GCS directly in curves or intermittently during the whole circuit. Nevertheless, intermittent GCS has an advantage in that it does not necessarily require synchronization between the stimulation and the simulator. In fact, the current GCS apparatus has different functions for selecting the interval program, so that it could be easily integrated into the setup of the simulator experiment. In addition, some of this apparatus is relatively inexpensive (some models cost less than $200), and the electrical administration is easy to deliver (the level of intensity can be directly selected in some models). Although contraindications to GCS are few and mostly hypothetical, it should be noted that researchers should be cautious when providing GCS to some groups, such as those with epilepsy, people with pacemakers, and pregnant women. Additionally, it must not be applied internally (e.g., in the mouth) or over areas of broken or damaged skin (see chapter 5 of Johnson, 2014, for an extensive revision of the hazards and contraindications for the use of GCS).
Key Points
Some drivers experience simulator syndrome (SS), a condition that may result in nausea, disorientation, dizziness, headache, and difficulty focusing when driving in a simulator. This syndrome is a critical issue in the use of simulators because it leads to population biases and data loss.
Galvanic cutaneous stimulation has been tested as an effective countermeasure to mitigate SS, but due to the scarce literature, this study is essential for corroborating the effectiveness of the technique.
Stimulation has usually been provided in curves, because it is considered the most likely maneuver for developing SS, or during the entire circuit. In this study, we have tested whether intermittent stimulation can provide the same benefit as direct stimulation in curves.
We suggest the use of intermittent stimulation programs for future interventions as they have easy experimental setup and programming.
Footnotes
Acknowledgements
This research was supported by two postdoctoral grants from the French Institute of Science and Technology for Transport, Development, and Networks and the Spanish Ministry of Education. Thanks to D. Ndiaye and S. Gauthier for the programming and analysis of the data. Thanks to M. Lavin, Matt Sassman, and F. Tornay for their insightful comments.
Germán Gálvez-García is a researcher at the Laboratory of Ergonomics and Cognitive Sciences Applied to Transport (LESCOT), a part of the French Institute of Science and Technology for Transport, Development, and Networks (IFSTTAR). He received his PhD in experimental psychology and behavioural neurosciences from Granada University in 2009.
Marion Hay is a PhD student at Laboratory of Ergonomics and Cognitive Sciences Applied to Transport (LESCOT), a part of IFSTTAR, and at the Laboratory INSERM U1075 COMETE (Mobility: Orientation, Attention and Chronobiology). She received her master’s degree in neuroscience from Rouen University in 2011.
Catherine Gabaude is a senior researcher at Laboratory of Ergonomics and Cognitive Sciences Applied to Transport (LESCOT), a part of IFSTTAR. She received her PhD in cognitive sciences from Lyon University in 2001.