
Abstract
Objective:
We aimed to build upon the state of knowledge about the impacts of sleep disruption into the domain of complex cognitive task performance for three types of sleep disruption: total sleep deprivation, sleep restriction, and circadian cycle.
Background:
Sleep disruption affects human performance by increasing the likelihood of errors or the time it takes to complete tasks, such as the Psychomotor Vigilance Task. It is not clear whether complex tasks are affected in the same way. Understanding the impact of sleep disruption on complex cognitive tasks is important for, and in some instances more relevant to, professional workers confronted with unexpected, catastrophic failures following a period of disrupted sleep.
Method:
Meta-analytic review methods were applied to each of the three different areas of sleep disruption research.
Results:
Complex cognitive task performance declines over consecutive hours of continuous wakefulness as well as consecutive days of restricted sleep, is worse for severely restricted sleep (4 or fewer hours in bed), is worse during the circadian nadir than apex, and appears less degraded than simple task performance.
Conclusion:
The reviews suggest that complex cognitive task performance may not be impacted by disrupted sleep as severely as simple cognitive task performance.
Application:
Findings apply to predicting effects of sleep disruption on workers in safety-critical environments, such as health care, aviation, the military, process control, and in particular, safety-critical environments involving shiftwork or long-duration missions.
Introduction
It is widely recognized that sleep disruption, which includes sleep restriction (SR) and the circadian desynchrony that typically accompanies total sleep deprivation, affects human performance by increasing the likelihood of errors or the time it takes to complete tasks, such as the Psychomotor Vigilance Task (PVT; Dorrian, Rogers, & Dinges, 2005). However, it is not clear whether more complex tasks are affected in the same way as simple tasks, such as the PVT.
Much has been learned about the general influences of sleep disruption on professional workers in safety-critical environments, such as health care (e.g., Barger et al., 2006; Landrigan, 2005; Landrigan et al., 2004; Reed, Fletcher, & Arora, 2010; Tucker, Whitney, Belenky, Hinson, & Van Dongen, 2010), aviation (Braude, Goldsmith, & Weiss, 2011; Caldwell et al., 2003), the military (Angus & Heslegrave, 1985; Krueger, 1989), and process control (Australian Council of Trade Unions, 2000; Bahner, Elepfandt, & Manzey, 2008). Although much of the information regarding the effects of sleep disruption on performance is contained in single studies addressing a targeted population (e.g., physicians, pilots), a number of meta-analyses have provided aggregated information from many of these studies (e.g., Blagrove, Alexander, & Horne, 1995; Drummond, Gillin, & Brown, 2001; Griffith & Mahadevan, 2006; Horne, 2012; Koslowsky & Babkoff, 1992; Lim & Dinges, 2010; Philibert, 2005; Pilcher & Huffcutt, 1996). The data from both individual and meta-analytic studies have been incorporated into models, such as the Sleep, Activity, Fatigue, and Task Effectiveness model (SAFTE) and the Fatigue Avoidance Scheduling Tool (FAST) that is based on the SAFTE model, which in turn is based principally on the effect of sleep disruption on PVT performance (Hursh, Balkin, Miller, & Eddy, 2004; see http://www.ibrinc.org/index.php?id=112).
In this paper, we explicitly attempted to go beyond the existing meta-analyses in several important respects. Five prior meta-analyses were located that examined sleep deprivation effects (Griffith & Mahadevan, 2006; Horne, 2012; Koslowsky & Babkoff, 1992; Lim & Dinges, 2010; Philibert, 2005; Pilcher & Huffcutt, 1996). All of these share some, but not all, features with the current work and hence provide complementary information to this work. The distinctions with the current work are as follows:
Because of our exclusive focus on complex tasks, we incorporate new literature in our meta-analyses. The two meta-analyses reported here address collectively data from 34 articles (including multiple data points per article). Of these 34 articles, only 11 were included in previously conducted meta-analyses by Lim and Dinges (2010), Alhola and Polo-Kantola (2007), Philibert (2005), Griffith and Mahadevan (2006), and Pilcher and Huffcutt (1996). Hence, we are including data points from 23 unique articles.
None of these articles examined SR. Although Alhola and Polo-Kantola (2007) extensively reviewed the literature on SR, they did not formally submit these effects to a meta-analysis. They also concluded that the effects of restriction may be more pronounced than those of total deprivation but did not provide a common metric upon which the two could be compared.
Only Lim and Dinges (2010) considered the role of the circadian cycle as a possible moderator variable for deprivation effects; however, they did not report its effects, leaving the reader to assume that it was insignificant.
Only Koslowsky and Babkoff (1992), Pilcher and Huffcutt (1996), and Philibert (2005) presented data that informed the progressive loss in performance with more sleep deprivation. However, Kozlowski and Babkoff did not differentiate task type, and Pilcher and Huffcutt and Philibert showed conflicting results, with Pilcher and Huffcutt showing a more rapid loss with simple than with complex tasks but Philibert showing the opposite.
Pilcher and Huffcutt (1996), Philibert (2005), and Lim and Dinges (2010) all made systematic comparisons of the overall effect size of deprivation between simple and complex tasks. However,
Pilcher and Huffcutt and Lim and Dinges restricted their consideration of complex cognitive tasks to studies on only reasoning (two paradigms; Baddeley, Ravens tests) rather than the more complex real-world tasks of decision making and problem solving addressed in the comprehensive review by Harrison and Horne (2000; these additional complex tasks are considered here). The results were conflicting: Philibert reported an equal or greater effect size decrement for the real-world complex task involving clinical judgment (–1.5), compared with simple information-processing tasks (–1.3); Lim and Dinges reported a smaller decrement for complex (reasoning) tasks (–0.2) than for simpler tasks (–0.87; although the results for the former were highly variable), and Pilcher and Huffcutt reported a considerably greater decrement for complex (–1.55) than for simple tasks (–0.87).
Finally, our approach to aggregating data was different from those in prior meta-analyses. Instead of collapsing the time dimension to provide a single standardized estimate of difference between more and less sleep disruption, we converted the raw data to ratios of performance. These ratios identified the proportion of performance degradation as a function of accumulated sleep disruption (deprivation or restriction), that is, disrupted performance relative to baseline performance. The ratio approach offered three benefits: (a) Each study that was examined potentially offered many different ratios at many different levels of sleep disruption. (b) The performance ratio was a quasistandardized method of comparing the magnitude of disruption at any given amount of accumulated time across studies. It allowed us to compare performance degradations across studies that used different tasks and measures. (c) The pool of performance ratios from across studies allowed us to meta-analytically regress performance degradation onto hours of accumulated sleep disruption or days of degradation, thus providing estimates of the percentage performance loss as a function of time. This method has not been used in previous sleep-related meta-analyses.
Our reason for focusing on complex tasks is to better appreciate the role of sleep disruption and fatigue when an unexpected emergency occurs (e.g., Chernobyl, Three Mile Island, Deep Water Horizon, Fukushima; Flin, Slaven, & Stewart, 1996; Rubinstein & Mason, 1979). Under such circumstances, operators must respond quickly and perform complex cognitive tasks, including failure diagnosis and fault management. These cognitive tasks make demands well beyond the demands of the relatively simple tasks, such as PVT, that have dominated sleep disruption research and may extend beyond the basic reasoning tasks examined by Lim and Dinges (2010). Furthermore, they often require concurrent performance of complex decision-making tasks (i.e., multitasking). We examine the extent to which the effects of sleep disruption on performance of complex tasks are different from the pattern observed in other studies for simple tasks, an issue for which data remain conflicting.
In addition to focusing on complex tasks, where possible, we examined the joint effects or interactions of three categorical types of sleep disruption:
Total sleep deprivation (TSD; i.e., more than 16 hr of consecutive wakefulness prior to complex cognitive performance assessment).
SR (i.e., several consecutive day-night cycles with relatively small amounts of sleep per cycle; typically less than 6 hr). This category is representative of the sleep patterns for the medical intern or a new parent.
Circadian cycle performance during the circadian day/night (i.e., morning/afternoon vs. the period from 10:00 p.m. to 6:00 a.m.). Note that circadian cycle was evaluated in conjunction with TSD only, because of the absence of studies examining circadian cycle interaction with SR.
We examine these three factors in consort because (a) combinations may come into play in the unexpected emergency response scenario, (b) there may well be interactions between them, and (c) each may affect performance on complex cognitive tasks in very different ways.
As noted earlier, we present the results of our meta-analyses in the nontraditional form of the percentage decrement in complex task performance as a function of the sleep disruption manipulation, rather than the more traditional Pearson r, Hedges g, or Cohen’s d′ effect size measures (Rosenthal, 1991; Borenstein, Hedges, Higgins, & Rothstein, 2009). We do so because of the paucity of studies that reported the data necessary to compute those traditional effect sizes, particularly in a manner conducive to identifying the standardized effects over time inherent to sleep disruption performance assessment. Commonly, the performance-over-time data are reported in graphical format only. In addition, the emphasis on percentage decrement highlights the actual expected performance decline as a result of the disrupted sleep.
Sleep Disruption Research
General Meta-Analytic Methods
Two types of searches were performed to identify potential papers for review. First, keyword searches were conducted in scientific and public databases (DTIC, Academic Search Premier, CINAHL, ERIC, PsycARTICLES, PsycINFO, Applied Science and Technology Abstracts, and Google Scholar) targeting the following terms: fatigue, sleep, sleep loss, sleep restriction, circadian disruption, circadian desynchronization, sleep disruption, sleep deprivation, underload, boredom, routine tasks, low task demand, and low task loading. In addition, several other keywords were used in conjunction with the fatigue-related terms to build more focused search strings (e.g., multitasking, routine, attention, arousal, task management, performance). Second, “ancestry” (Cooper, 1982, p. 295) searches of the reference lists were performed on research reports, reviews, and meta-analyses to further identify potential papers.
We initially reviewed a broad scope of the scientific literature to identify and organize research and review papers related to the effects of sleep variables on performance on a wide variety of tasks. The fatigue-related sleep variables of interest were TSD, chronic and short-term SR, and circadian phase/circadian desynchronization. We identified 247 papers that specifically addressed the effects of the sleep variables on performance of complex tasks.
Several criteria were established for inclusion of a research paper in our meta-analyses. Studies included in each of the meta-analyses are identified in Appendix A. To be included, studies had to meet the following requirements:
Include performance data for complex cognitive experimental or actual work tasks; these included decision making, multitasking, tasks that burdened working memory, and team performance tasks. Decision-making tasks that were included were defined as those tasks requiring “convergent, rule-based skills of logical, critical, and deductive reasoning but also can involve unique and unfamiliar circumstances, necessitating a range of divergent skills” (Harrison & Horne, 2000, p. 238); Multitasking demanded concurrent performance of two or more tasks; Working memory tasks involved retention of information concurrently with another cognitive operation (e.g., keeping track); and, Team performance included tasks requiring team communication, group information seeking/sharing, and group decision making. Studies that evaluated simple cognitive tasks (e.g., declarative knowledge tasks, simple mental arithmetic, visual search, reaction time, routine driving, PVT, and Stroop tasks) were excluded from this analysis. Appendix B lists the specific tasks used by investigators whose data were included.
Report (numerically or graphically) measures of task- or test-related performance data (accuracy or speed).
Include (and report data in accordance with) a control condition. Three control types were identified for our purposes:
Between participants at equivalent time points, Within participant at equivalent time points, or Within participant at initial (baseline) performance.
Report time-based performance data in such a way that performance in the sleep-disrupted condition relative to a control condition could be attributed to a specific number of hours of continuous wakefulness or days of sleep restriction.
Data were extracted from graphs, tables, and text. At a minimum, the following data were collected: the number of hours of continuous wakefulness or the number of hours of sleep in each 24-hr period, performance when sleep deprived/restricted, and control group performance. Where necessary, performance measures were inverted (e.g., error measures converted to accuracy) so a higher number always represented better performance. Therefore, trends less than 1 always indicate superior performance for the control group relative to the sleep-deprived group. Conversely, trends more than 1 indicate performance cost for the control group relative to the sleep-deprived group. Note that this difference in trend lines above and below 1 is true for the data plots of both accuracy and time to perform a task; lower scores indicate worse performance (e.g., longer task times). Our search did not constrain the starting date but terminated in 2013.
Meta-Analysis 1: TSD and Circadian Cycle Research
Twenty-eight papers met our criteria for inclusion in the meta-analysis of TSD research findings and yielded a total of 447 performance ratios (the large number of ratios from relatively fewer studies was the consequence of extracting numerous data points over time from each study). These studies are listed in Appendix A. TSD research designs (Hutchins, Laux, Wickens, & Sebok, 2013; Wickens, et al., 2013) focus on assessing performance over extended periods of continuous wakefulness, “generally for 24–72 hours” (Alhola & Polo-Kantola, 2007, p. 554). Data collection from the acute TSD research targeted continuous time-based data rather than acute total (maximum deprivation vs. control). In our meta-analysis of the effects of TSD on performance, we coded three primary variables: hours of continuous wakefulness, performance outcome over time awake, and circadian cycle. Hours of continuous wakefulness was treated as a continuous variable with whole hour increments. The performance outcome variables were coded as time to perform and accuracy. The circadian cycle was included in this meta-analysis, rather than treated in a separate analysis, because of the profound influence of cycle on the effect of TSD (i.e., its prominent role as a moderator variable). This variable was coded as circadian day or circadian night (10 p.m. to 6 a.m.). The coding for circadian cycle resulted in 99 performance ratios for circadian night and 212 performance ratios for circadian day.
To elaborate on this third moderator variable, research designs targeting circadian cycles (Hutchins et al., 2013; Wickens et al., 2013) measure the individual’s circadian period, when the probability of falling asleep is naturally highest, and compare performance to that period when the propensity toward staying awake is naturally highest (May & Baldwin, 2009; Williamson et al., 2011). Consequently, a cycle of circadian day and circadian night is determined based on when the individual would naturally be awake or asleep. On earth, this is typically coupled to solar night and day. In unusual environments (e.g., in a submarine, on a space exploration mission, during Antarctic winter), the two cycles can become decoupled.
In order to assess when an individual would naturally be asleep, commonly a dim light melatonin onset (DLMO) measurement technique was used. DLMO measures melatonin levels from saliva samples to indicate the time of natural onset of melatonin excretion in the body. Melatonin is naturally excreted by the body to induce sleepiness. By tracking the rise and drop of melatonin, researchers are able to capture the body’s natural sleep/wake cycles (Mollicone, 2008). In order to code for circadian day versus circadian night at each point of performance measurement, time-based boundaries were needed that defined the range of daily hours that coincided with the two circadian cycles. To establish these hour-based boundaries, a sample of studies using the DLMO measurement technique was reviewed (Angus & Heslegrave, 1985; Bratzke, Steinborn, Rolke, & Ulrich, 2012; Lo et al., 2012; Mollicone, 2008; Monk, Buysse, Billy, Kennedy, & Willrich, 1998; Scheer, Shea, Hilton, & Shea, 2008). Across the six studies, the average time of onset was approximately 2200 and the average time of return to normal levels was approximately 0600.
TSD meta-analysis data analysis
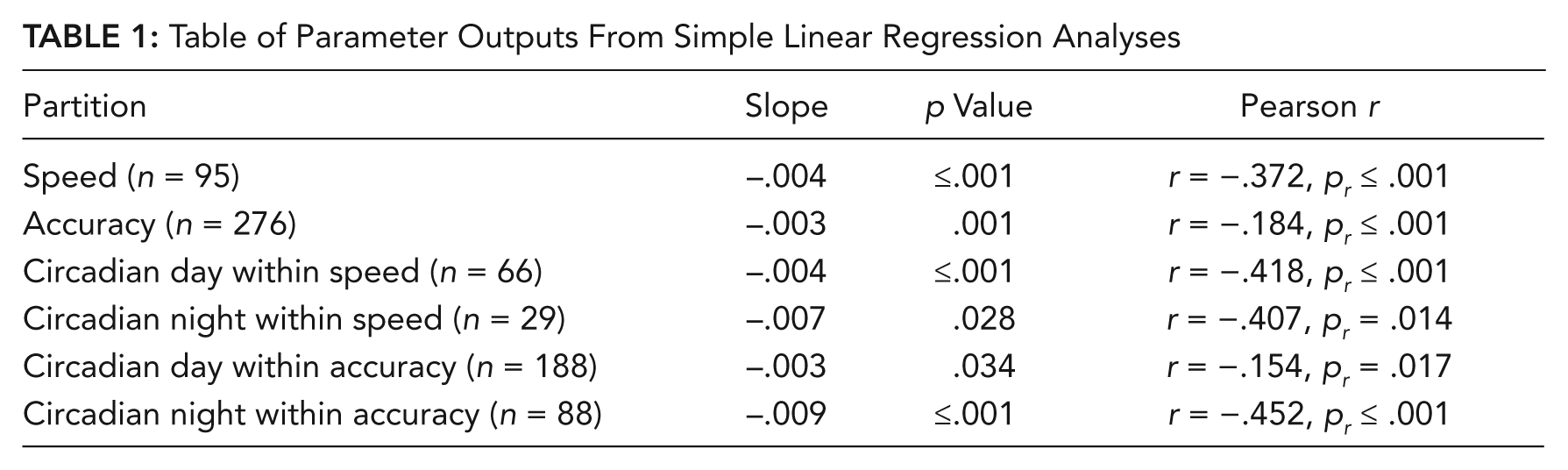
Analysis of the time-based performance ratio data included two levels of data partitioning and analysis: a partition of the 447 performance ratios by speed and accuracy, and a partitioning by circadian day and night within speed and accuracy. Data partitioning allowed simple linear regression models to be fit to each data subset (e.g., speed, accuracy, circadian day, night). We made the assumption that at a time of no sleep deprivation, the performance in the control groups and “treated” groups was equal. Therefore, the y intercept was forced to a value of 1.0, which represents a point of no performance degradation. The slope of the line over time indicates change in performance ratio for each added hour of sleep deprivation. We also provide standardized measures of Pearson r and its associated p value. These standardized measures are not in raw units, but the slope value (i.e., β1) is in raw units. Analyzed in this way, slope coefficients represented a straightforward percentage change in rested versus TSD performance for each hour of continuous wakefulness, for example, PR = −0.05 translates to a 5% decrement in TSD performance relative to control performance for each hour of continuous wakefulness, PR = −0.005 translates to a 0.5% decrement, and so forth.
A criterion of three standard deviations was used to identify outlying values within each outcome distribution. Rather than removing outlying data points from the analysis, outliers were replaced with data points that met the three–standard deviation criterion for the mean. For the sleep deprivation data, all speed data fell within three standard deviations, and for the accuracy data three data points were bound at the criterion. Three standard deviations in the distribution of accuracy TSD performance ratios was equal to a ratio of 2.7.
Results of TSD meta-analysis: Regression analysis
Figures 1a and 1b show the overall TSD data regressions for time to perform and accuracy, respectively; the regression lines are shown overlaying the raw data points. The regression analyses for these two data sets are presented in the top two rows of Table 1. As is evident from the table, both variables showed significant declines of roughly the same magnitude (slope), corresponding to a loss of about 10% of performance per day. The last four rows of Table 1 also show the same data, now broken down by circadian night and day. Figures 2a and 2b depict these data for time to perform, with slopes of −0.004 for day and −0.007 for night. Particularly for accuracy (last two rows), the differences between day and night are profound, and these differences are illustrated in Figures 3a and 3b, respectively. The TSD-related accuracy decline is approximately 3 times as great at circadian night than during the day.
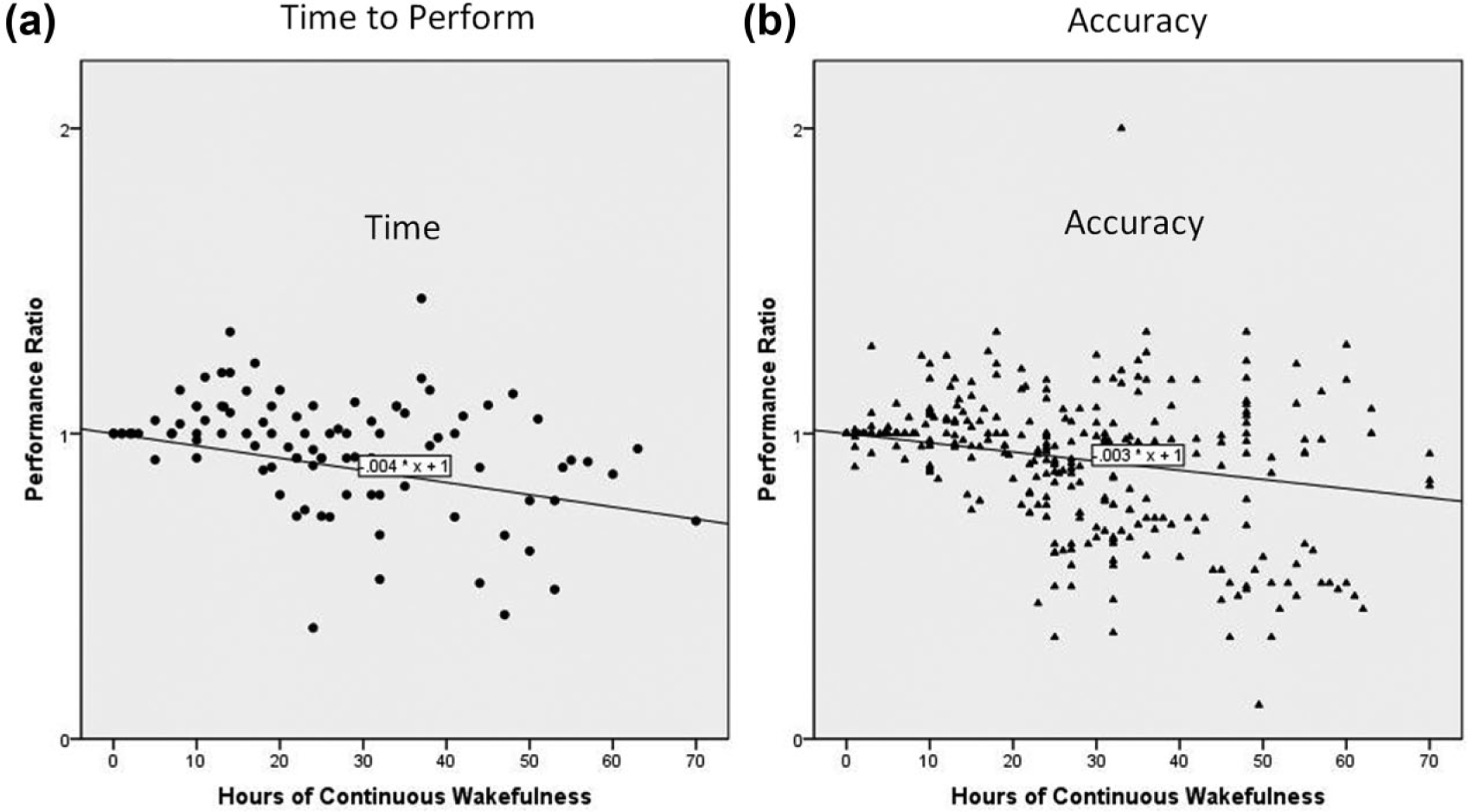
Overall total sleep deprivation data: (a) time, (b) accuracy.
Table of Parameter Outputs From Simple Linear Regression Analyses
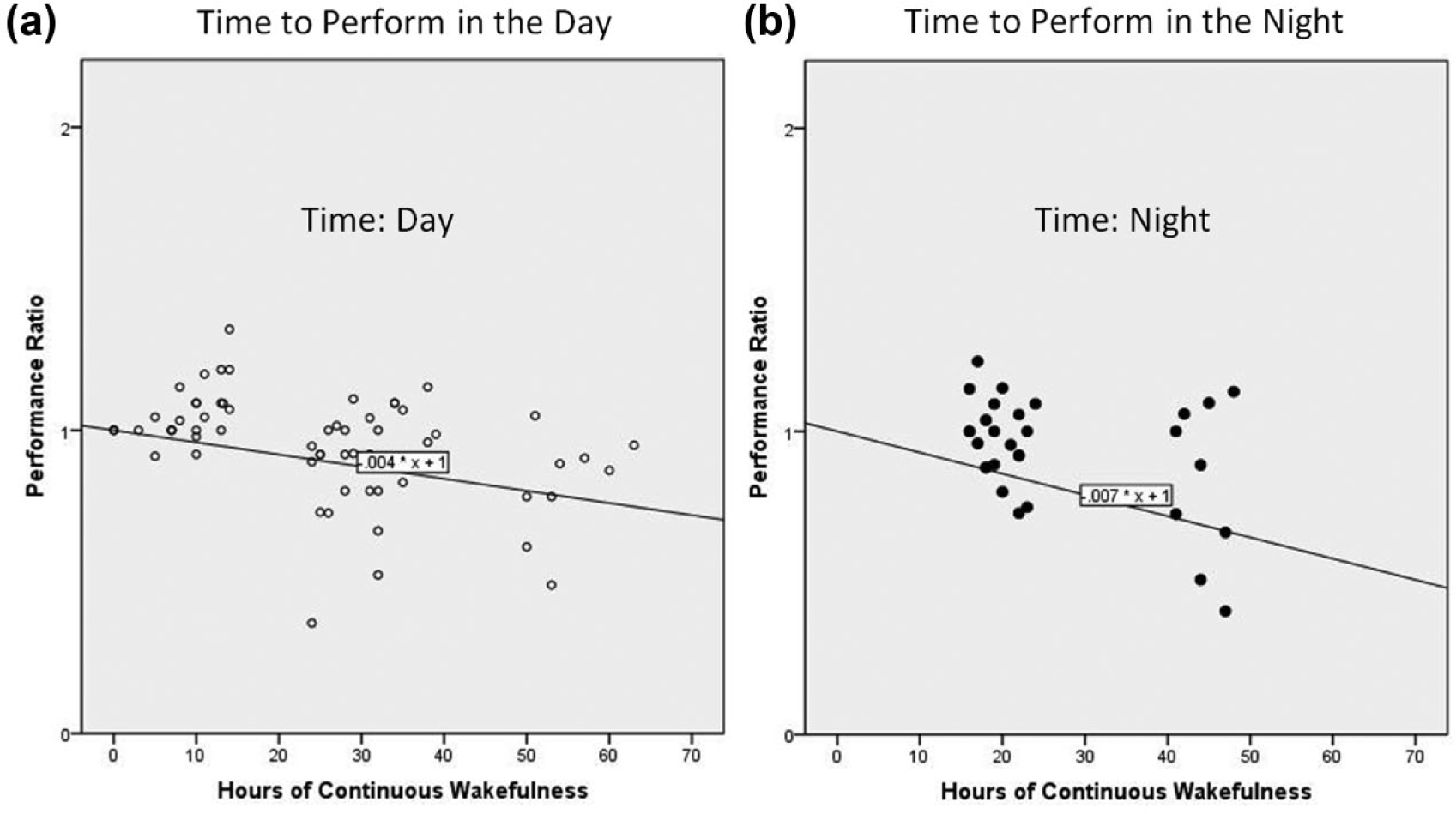
Total sleep deprivation time by circadian phase: (a) day, (b) night.
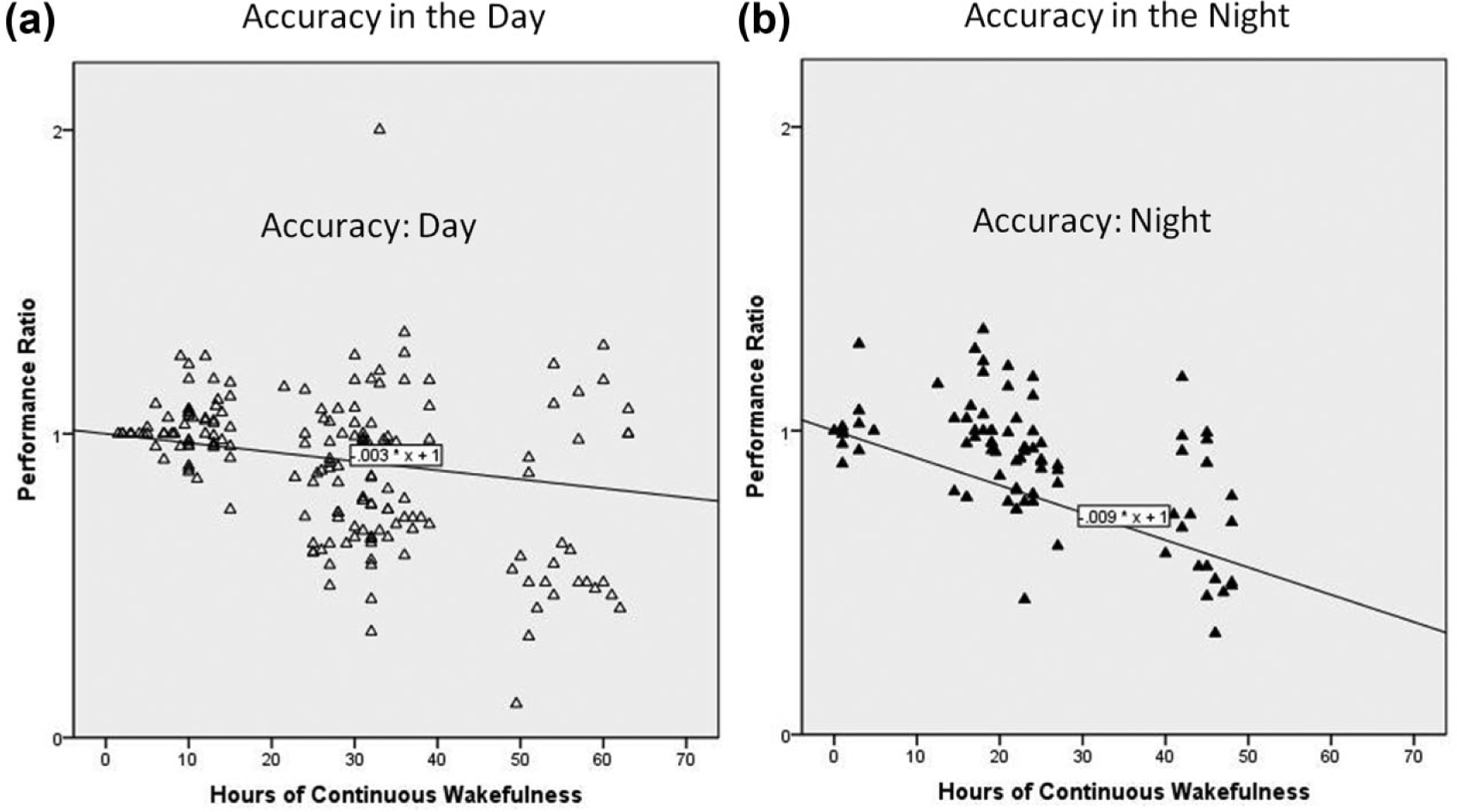
Total sleep deprivation accuracy by circadian phase: (a) day, (b) night.
TSD meta-analysis discussion
Overall, complex cognitive performance was substantially worse for sleep-deprived groups than their respective control counterparts. The loss in complex cognitive performance when sleep deprived is consistent with other findings in the literature on TSD (e.g., Lim & Dinges, 2010). The circadian analyses strongly suggest that complex cognitive performance (both speed and accuracy) over hours of continuous wakefulness differs between the circadian night and the circadian day. On average, the complex cognitive performance decrement was twice as large during the circadian night, and the effect at circadian night for accuracy was extremely high: 0.009, or 21.6% loss in accuracy per sleepless day.
Of further significance is the different pattern of effects between the simple and complex tasks emerging from the literature on sleep deprivation. The slope values observed here for complex cognitive tasks (mean speed, −.004; mean accuracy, −.003) can be compared with data derived from representative studies using simple vigilance and reaction time (RT) tasks. For example, from data presented in Angus and Heslegrave (1985), we can derive a slope estimate of approximately −.01 for both accuracy of auditory vigilance and speed of serial RT. That is, in the latter case, the decline over sleepless days of these simpler tasks is about 2 to 3 times greater than observed in this analysis of complex tasks.
Consistent with the aforementioned conclusions of smaller effects for more complex tasks, the meta-analysis by Lim and Dinges (2010) demonstrated that simple attention measures, primarily comprised of PVT, had the largest decrease in performance over 24 to 48 hr of sleep deprivation across all cognitive measures, including simple attention, complex attention, processing speed, working memory, short-term memory, and measures of crystallized intelligence and reasoning. Specifically, in this study, in which those authors used Hedges’ g as an effect size measure, simple attention showed a much larger Hedges’ g of −.762 (p ≤ .001) for lapses (i.e., errors of omission) and −.732 (p ≤ .001) for reaction time. In contrast, crystallized intelligence and reasoning (including problem solving and other measures analogous to the complex cognitive category in the current analysis) showed a Hedges’ g of −.125 for accuracy. In summary, then, our results confirm the essential findings of Lim and Dinges regarding the greater sleep deprivation disruption of simpler tasks while contrasting with the findings of Pilcher and Huffcutt (1996) and the ambiguous findings of Philibert (2005). We discuss the possible interpretation of this finding below.
Meta-Analysis 2: SR Research
SR, or partial sleep deprivation, is associated with sleep deficits in nightly sleep as opposed to the complete lack of sleep and continuous wakefulness of sleep deprivation. Similar to sleep deprivation, the inadequate sleep of SR is also found to result in declines in performance (May & Baldwin, 2009). At a minimum, SR can be the result of as little as 1 hr less sleep per night (Williamson et al., 2011); however, it is commonly explored as a restriction to less than 5 hr (Pilcher & Huffcutt, 1996) or 4 hr (Williamson et al., 2011) in bed within a 24-hr period.
The chronic SR studies examined here evaluate performance either daily during or following several consecutive nights of restricted sleep (Alhola & Polo-Kantola, 2007; Williamson et al., 2011). Because individuals sleep varying amounts per night naturally, it is difficult to experimentally reduce everyone’s sleep by a constant amount. Consequently, as a research manipulation, restricted sleep is achieved by controlling the amount of time participants spend in bed each night; therefore, SR is achieved by limiting time in bed to a constant number of hours as opposed to reducing sleep by a constant number of hours (Wickens et al., 2013). We have dichotomized SR into severe (time in bed of 3-4 hr) versus mild (time in bed of 5-6 hr).
We sought to quantitatively synthesize change-over-time data from the literature examining performance on complex cognitive tasks over consecutive days of restricted sleep. In contrast to the case with sleep deprivation, the literature on the impacts of SR on complex cognitive performance was much sparser. Only five papers met our criteria for inclusion in the meta-analysis of SR research findings and yielded a total of 66 accuracy performance ratios, with SR extending to seven consecutive nights (Appendix A). Data were extracted from graphs, tables, and text. Days of restricted sleep were coded as a discrete numeric value. Time in bed was coded as dichotomously as severe or mild restriction. The outcome variable coded measures of score and error, where score represented scores on task or test performance and error included measures of incorrect action, such as procedural errors in a test, accidents in a driving simulator, and so on. There were inadequate data available to derive slope measures for speed or separate measures for circadian day and night.
SR meta-analysis data analysis
Analysis of the time-based performance ratio data included simple linear regression modeling of the performance trends. Similar to the rationale for the analysis of the sleep deprivation data, the descriptive linear models were forced to intercept the y axis at 1 (i.e., β0 = 1) so that all rates of change over days of restricted sleep departed from a common starting point equivalent to a performance ratio of 1.
Results of Meta-Analysis 2: Days of SR
Overall, a negative slope was fit to the performance data over days of sleep restriction (β1 = −.026, p ≤ .1), describing a gradual decline in complex cognitive performance over days of restricted sleep. However, as shown in Figure 4, there was a profound difference in performance deterioration between mild (>4 hr per night) and severe (≤4 hr) sleep restriction conditions. The mild restriction condition showed almost no cost, yet the severe sleep restriction condition showed a significant slope of −0.067 (p < .01), corresponding to a 7% loss in performance with each night of restriction equal or less than 4 hr.
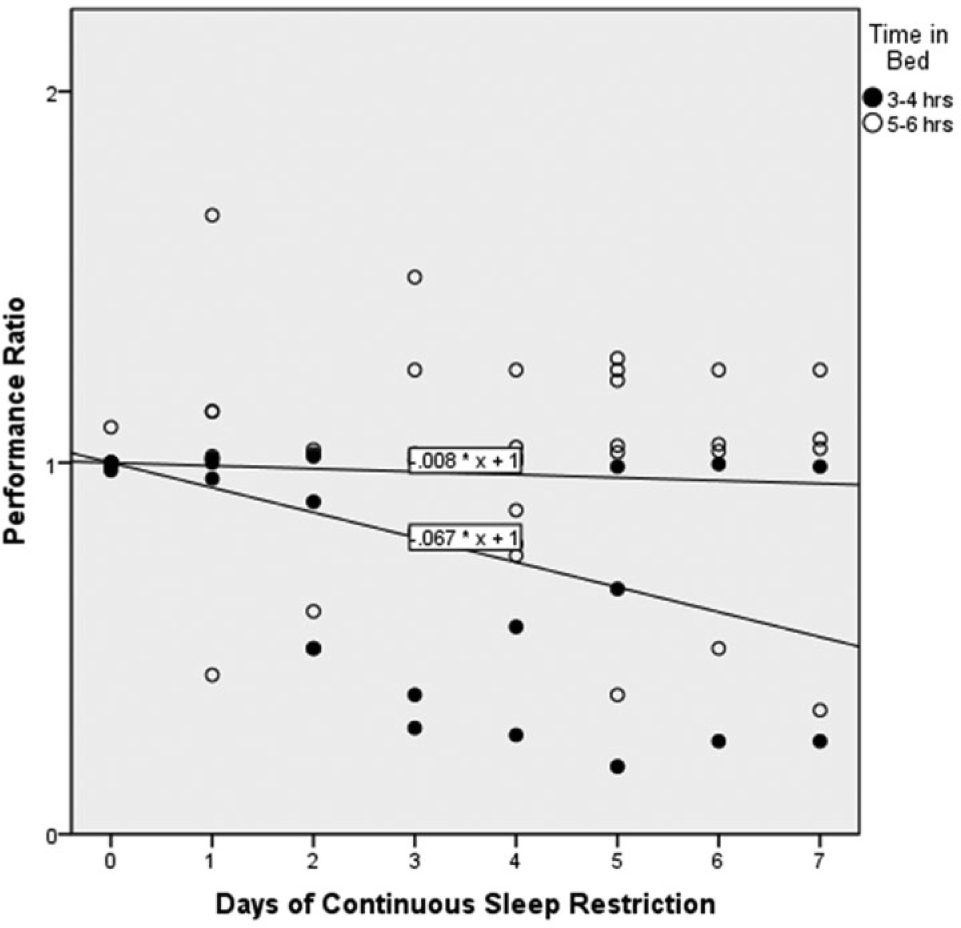
Accuracy performance for mild and severe restricted sleep over consecutive days of restricted sleep. Any given study may have included as few as one sleep-restricted data point.
SR effects on performance speed
Although none of the research reports we reviewed relating SR to performance included an assessment of the effect of SR on time to perform a task (speed), Van Dongen, Maislin, Mullington, and Dinges (2003) provided data from which we could derive the slope representing the effect of SR on performance speed over days. Van Dongen et al. (2003) report differences in performance for participants restricted to 4 hr in bed per night for 14 days, compared to performance at baseline (no SR) and to performance of participants sleeping 8 hr per night. The tests they used included the Digit Symbol Substitution Test (DSST), a test of working memory. Based on data from Laux and Lane (1985), participants who are not sleep deprived and who are otherwise similar to the Van Dongen et al. participants could be expected to complete 68.4 items in 90 s, or spend an average of 1.32 s on each item. Using change per day data from Van Dongen et al., time per item could be calculated for each day of SR (i.e., after 7 days of SR, Van Dongen et al. reported that participants were performing 5 items fewer than at baseline, or 63.4 items per 90 s, which means they were spending 1.42 s per item, or .10 s more than if not sleep restricted). When these numbers are converted to time in seconds per item, it is clear that as the days of SR increase, participants take longer and longer to complete the items on the DSST despite the practice effect, which is typically found to improve performance when testing is repeated multiple times. The practice effect was obvious for participants whose sleep was not restricted, who completed more items each day over the 14 days. When time per item is regressed on days of SR, the slope is significant at β1 = .012 (p < .001), meaning that time per item increased 1.2% per day.
Meta-Analysis 2 discussion
SR, much like sleep deprivation, appears to gradually degrade complex cognitive performance over consecutive days of restricted sleep. However, the decrement to complex cognitive performance over consecutive days of restricted sleep is strongly moderated by the degree to which sleep is restricted (i.e., the controlled time in bed). Restriction appears to have little effect when more than 4 hr of sleep is allowed (i.e., mild restriction), but a profound effect when less than 4 hr is imposed (Figure 4). Although studies of complex task performance were not located that might have revealed different degrading functions of circadian night versus day, we can infer from the data of sleep deprivation that similar trends would be found with restriction, that is, a greater effect of restriction when measured during circadian night than during day.
Discussion
In the current meta-analyses, we examined the sleep disruption effects of total sleep deprivation, SR, and circadian cycle on complex task performance. Not surprisingly, and consistent with the results of prior experiments and meta-analyses (e.g., Alhola & Polo-Kantola, 2007; Blagrove et al., 1995; Drummond et al., 2001; Griffith & Mahadevan, 2006; Horne, 2012; Koslowsky & Babkoff, 1992; Lim & Dinges, 2010; Philibert, 2005; Pilcher & Huffcutt, 1996), as well as with the data reviewed by Harrison and Horne (2000), all three factors produced performance decrements. Thus complex cognitive tasks, like their simple task counterparts, are degraded by sleep deprivation, restriction, and circadian night. However, the degradations imposed by these variables on complex task performance appear to be less severe than their effects on simple task performance (e.g., vigilance- and attention-switching-type tasks).
The conclusion that the performance degradation of sleep disruption on complex tasks is less than on simple tasks is reinforced by the differences found by Lim and Dinges (2010) in the meta-analysis of sleep deprivation effects on simpler versus more complex cognitive tasks, an effect that might be explained by the greater engagement required by (and therefore, greater stimulation afforded by) complex tasks. Such a finding is consistent with those of Matthews and Desmond (2002), who found that task-induced fatigue had greater impact on driving straight roadway segments (a simple task) than curved ones (a more complex task). One might speculate the possible reasons for this difference: The boredom and low arousal of simple tasks is amplified with sleep loss, and tasks with complexity provide an increase in arousal that can compensate for this loss, in a manner predicted by Hockey’s (1986) analyses of stressor interactions.
The current examination of the literature on sleep disruption is complementary to other reviews in the domain—for example, Lim and Dinges (2010); Harrison and Horne (2000); Angus and Heslegrave (1985); and Gunzelmann, Gross, Gluck, and Dinges (2009)—supporting the differential effect of sleep disruption between simple and complex cognitive task performance. In this study, we focused exclusively on complex cognitive task performance and examined a diverse set of research studies that investigated sleep disruption effects on complex task performance. In addition, the current reviews also highlight the complexities and higher-order interactions likely to exist between the amount of sleep disruption and the time of day in which performance is required to be performed following sleep disruption. When considering the influences of these three factors on complex cognitive task performance, one may surmise that the ability of a professional to safely and effectively confront an unexpected, catastrophic failure following a prolonged period of sleep disruption is likely to be compromised. Further research is warranted to explore the compounded effects of sleep deprivation, SR, and circadian schedules on the type of complex cognitive task performance characteristic of real-world professional situations, particularly, emergency crisis management.
A final factor, not considered in the current paper but highly relevant to complex emergency response management, is sleep inertia, the degraded performance upon immediate awakening (Dinges, Orne, & Orne, 1985; Wickens et al., 2013; Wickens, Laux, Hutchins, & Sebok, 2014). In other research (Wickens et al., 2014), we have found that the degrading influence of sleep inertia on complex task performance is just as great if not greater than on simple task performance. This finding becomes highly relevant for emergency task management because, clearly, an unexpected emergency is just as likely to occur at night (when the performer is sleeping) as during the day.
Key Points
Complex cognitive task performance significantly declines over consecutive hours of continuous wakefulness.
The degrading influences of sleep deprivation on complex cognitive task performance are greater during the circadian night than during the circadian day. This difference is particularly pronounced for task accuracy.
Complex cognitive task performance shows a greater decrement over consecutive days of severely restricted sleep (i.e., 4 or fewer hours in bed) than mild sleep restriction (i.e., more than 4 hr in bed).
The general decrements on complex task performance caused by total sleep disruption appear to be smaller than those on simple task performance.
Footnotes
Appendix A
Appendix B
Acknowledgements
We wish to thank our project sponsors at NASA: Brian Gore, Jessica Marquez, and Sandra Whitmire. This work was funded under NASA Grant NNX12AE69G.
Christopher D. Wickens is a senior scientist at Alion Science and Technology Corporation, Micro Analysis and Design Operation, in Boulder, Colorado, a professor of psychology at Colorado State University, and professor emeritus at the University of Illinois at Urbana-Champaign. He earned his PhD in psychology from the University of Michigan in 1974.
Shaun D. Hutchins is a PhD candidate in research methodology at Colorado State University. He earned his MA in experimental psychology at New Mexico State University and his BA in psychology from the University of Maine at Farmington.
Lila Laux is a principal human engineer at Alion Science and Technology. She earned her PhD in industrial psychology from Rice University in 1986.
Angelia Sebok is a principal human factors engineer and program manager at Alion Science and Technology. She earned her MS degree in industrial and systems engineering from Virginia Tech in 1991.