
Abstract
Objective
Review the use of physiological measurement in team settings and propose recommendations to improve the state of the science.
Background
New sensor and analytical capabilities enable exploration of relationships between team members’ physiological dynamics. We conducted a review of physiological measures used in research on teams to understand (1) how these measures are theoretically and operationally related to team constructs and (2) what types of validity evidence exist for physiological measurement in team settings.
Method
We identified 32 articles that investigated task-performing teams using physiological data. Articles were coded on several dimensions, including team characteristics. Study findings were categorized by relationships tested between team physiological dynamics (TPD) and team inputs, mediators/processes, outputs, or psychometric properties.
Results
TPD researchers overwhelmingly measure single physiological systems. Although there is research linking TPD to inputs and outputs, the research on processes is underdeveloped.
Conclusion
We recommend several theoretical, methodological, and statistical themes to expand the growth of the TPD field.
Application
Physiological measures, once established as reliable indicators of team functioning, might be used to diagnose suboptimal team states and cue interventions to ameliorate these states.
Keywords
Unobtrusive measurement in the applied cognitive and organizational sciences has surged in recent years (Hill, White, & Wallace, 2014), along with new capabilities enabled by advanc-es in a variety of sensor technologies and analytic techniques (Luciano, Mathieu, Park, & Tannenbaum, 2018; Markowetz, Błaszkiewicz, Montag, Switala, & Schlaepfer, 2014). Applied research increasingly makes use of measures of individual physiology (Ganster, Crain, & Brossoit, 2018; Nofal, Nicolaou, Symeonidou, & Shane, 2018). Physiological measurement may be well suited to help address the general call for more dynamic and unobtrusive measures of team processes and performance in the human factors and organizational psychology literature (Funke, Knott, Salas, Pavlas, & Strang, 2012; Kozlowski & Chao, 2018; Salas, Cooke, & Rosen, 2008). Team physiological dynamics (TPD), defined here as the continuous assessment of individual team members’ physiological states while performing as a team, holds promise as an approach to understand relationships between team members’ unobtrusively measured physiological dynamics, and team inputs, processes, emergent states, and outcomes. The sampling rate requirement for “continuous” measurement is not formally defined, but all studies included in this review sample physiological functioning at least once per second. The main distinction is between single point measures (e.g., salivary cortisol levels) and measures that capture high-frequency (1 Hz or greater) data representing dynamics (change over time). The measurement and study of TPD can potentially advance team theories and organizational interventions through more scalable and dynamic measurement methods (Rosen, Dietz, Yang, Priebe, & Pronovost, 2014). Such interventions could include selection and composition of teams and provide performance feedback and tools for real-time management of teams in training and job settings.
This review aims to answer fundamental questions about the state of the science in TPD. First, we examine how researchers use physiological measures in team research. This includes reviewing which physiological systems are measured, in what types of teams, and through which methods. Second, we review how physiological measures are theoretically and operationally related to team constructs. Third, we evaluate what types of validity and reliability evidence exist for physiological measurement in team settings. Fourth, we provide recommendations and future directions based on an analysis of the state of the existing literature.
Background and Rationale
This section introduces the key concepts and framework used to review, synthesize, and critique the existing literature on physiological measurement in team settings. As our goal is to inform the use of TPD measures to better understand and ultimately improve team functioning, our approach draws from the fundamental concepts in the science of teams (cf. human physiology) described later.
Teams, Teamwork, and the Input–Mediators–Output–Input (IMOI) Framework
We adopt commonly used definitions of teams (i.e., two or more individuals working interdependently toward shared and valued goals; Salas, Dickinson, Converse, & Tannenbaum, 1992), task work (i.e., performance behaviors related to individual team members completing their work; Baker & Salas, 1992), teamwork (i.e., performance behaviors associated with team member interactions; Crawford & LePine, 2013), team performance (i.e., the combination of task work and teamwork; Salas, Stagl, Burke, & Goodwin, 2007), and team effectiveness (i.e., the degree to which the team’s performance outcomes meet goals and expectations; Salas et al., 2007).
Two interrelated features of these definitions hold particular significance to this review. First, drawing on concepts from the broader science of complex systems (e.g., Anderson, 1999; Arrow, McGrath, & Berdahl, 2000), team performance is viewed as a multilevel phenomenon involving both top-down contextual influences on behavior in lower level components of the system, and bottom-up emergent processes originating from the interactions of lower level system components (Kozlowski, 2015). Conversely, physiological dynamics are measured only at the individual level. Consequently, to understand these phenomena within a team setting requires answering key conceptual and methodological questions about levels of analysis and aggregation. Second, team performance is dynamic. It unfolds over time and levels. Because physiological dynamics can be measured at a high sampling rate (e.g., 1 Hz and greater), these approaches can help address calls for more dynamic empirical studies of team processes (Kozlowski, Chao, Grand, Braun, & Kuljanin, 2013, 2016). To do so, it is first necessary to answer key questions about how TPD can be represented, associated with team processes or emergent states, and used to test theory-driven hypotheses.
In the absence of an overarching theory or framework for TPD, this review adopts the IMOI framework (Ilgen, Hollenbeck, Johnson, & Jundt, 2005) from the science of teams. The IMOI framework has served as an organizing heuristic for the science of teams for decades. Team inputs are relatively stable attributes of the team, its task, and context (e.g., team composition, interdependence structure, organizational setting; Bell, 2007; Stewart, 2006). Team mediators include process behaviors typically classified as action, transition, or interpersonal processes (LePine, Piccolo, Jackson, Mathieu, & Saul, 2008; Marks, Mathieu, & Zaccaro, 2001), and cognitive (e.g., shared situation awareness; Wildman, Salas, & Scott, 2014) and affective (e.g., team mood, stress; Lehmann-Willenbrock, Meyers, Kauffeld, Neininger, & Henschel, 2011) emergent states that fluctuate over a team’s performance episode. Outputs are the results of team interaction and typically include team effectiveness, efficiency, viability, and learning. The IMOI framework was chosen to organize this review because it is a very high-level organizational framework capable of classifying aspects of a variety of more bounded theories (e.g., around a specific physiological system like team neurodynamics, Stevens et al., 2013; or a pattern of observations like synchrony, Guastello & Peressini, 2017) as well as atheoretical empirical studies. This review aims to summarize literature across a wide-ranging literature from diverse disciplines. Although the IMOI framework does not necessarily facilitate advancement of highly bounded theories within the broad field of TPD (e.g., physiological system or pattern-specific theories), it does enable integration of these research streams into the team research community.
Physiological Measurement in Team Settings
The study of physiology in dyads and larger groups has a long history, including parent and child dyads, therapists and clients, romantic couples, and groups of friends and performers (Palumbo et al., 2017). For example, the work of John Gottman in the area of marital dynamics employed continuous measures of physiology, communication analysis, and self-report of emotional valence throughout conversations to predict long-term outcomes for relationships (Gottman, 2005). In addition, the broad multidisciplinary field of social neuroscience seeks to uncover biological and neurological processes underlying social behavior (Cacioppo & Cacioppo, 2013) and has provided new insights into social-psychological phenomenon (e.g., Social Identity Theory; Scheepers & Derks, 2016). These complex and diverse literatures indicate that physiological patterns between dyads and groups reflect meaningful changes in social processes (e.g., the presence of physiological synchrony [PS] relates to the health of an interpersonal relationship; Palumbo et al., 2017). However, much of this work has focused on individuals in social settings or nontask performing groups and is disconnected from the extensive research on work teams. Studying TPD in the context of work teams can help understand potentially unique relationships between physiological processes and tasks and variables that are relevant to work teams (e.g., metrics of team productivity).
Following Palumbo and colleagues’ (2017) definition of the more general concept of interpersonal autonomic physiology as “the general methodology for studying temporal interactions in physiological processes between multiple people” (p. 100), the current review and definition of TPD focuses on the measurement of physiological dynamics over time of team members captured during team performance episodes (i.e., while team members are interacting interdependently toward shared goals). Consequently, TPD occurs concurrently with team interaction processes and emergent states. In this review, we consider how TPD relates to team constructs broadly represented by the IMOI framework introduced earlier.
As illustrated in Figure 1, overlaying the IMOI and team member physiological processes yields four broad categories of potential research questions or conceptual relationships, and related practical applications. First, research can test relationships between team inputs and physiological dynamics of team members. This could include the use of team composition variables (e.g., different aggregations of individual difference variables; Mathieu, Tannenbaum, Donsbach, & Alliger, 2014) or manipulations of task, technology, or team design (e.g., task-induced workload; Toppi et al., 2016) to predict aspects of physiological dynamics in teams. Once established, these team input-to-TPD relationships could be used in team selection or composition systems (e.g., adding predictive validity to traditional trait measures important for team members), diagnostic competency assessment systems within intelligent tutoring systems (e.g., diagnosing different levels of skill proficiency within the team), or to evaluate the impact of different technologies or other structural interventions on team functioning.

Integrating the inputs–mediators–outcomes model with team physiological dynamics.
Second, research can test relationships be-tween TPD and team processes or emergent states. Here, the goal is to understand how physiological signals can be used to understand how certain team processes (e.g., communication patterns; Gorman et al., 2016) or emergent states unfold within a team over time. If validity evidence exists for these TPD measures, they can help to remove resource barriers (e.g., time to manually code team process behaviors) currently hindering more research on dynamic team processes and resulting applications. Understanding how patterns in physiological dynamics relate to team processes and emergent states can also contribute to real-time team management tools (e.g., team interaction analytics and displays to aid team reflexivity and self-correction or leader-driven interventions) or the design of interactive and synthetic agent systems (e.g., driving more responsive and effective models for artificial agents as team members).
Third, research can test relationships between TPD and team outcomes. This includes task (e.g., error rate, completion time; Henning, Boucsein, & Claudia Gil, 2001; Henning & Korbelak, 2005), affective (e.g., group potency, mutual trust), and team learning outcomes. With TPD patterns associated with output variables, predictive aids can be developed to use TPD signals to prompt the team to potential failures. Given the cyclical nature of the IMOI framework, this can include relationships between patterns of physiology within teams and future performance episodes of that team.
Fourth, in addition to TPD relationships with aspects of the IMOI framework, researchers can focus exclusively on the physiological measurements without further connection to the IMOI model. These studies could explore the psychometric properties of TPD, just as studies focus on the reliability or internal structure of other measurement methods within teams, or relationships between measures of different types of physiological dynamics (Strube & Neuman, 2007). Psychometric evaluation studies could include, for example, evaluating the impact of different instrumentation, pre-processing, or data aggregation and analysis techniques on physiological signal quality.
Method
Search Strategy
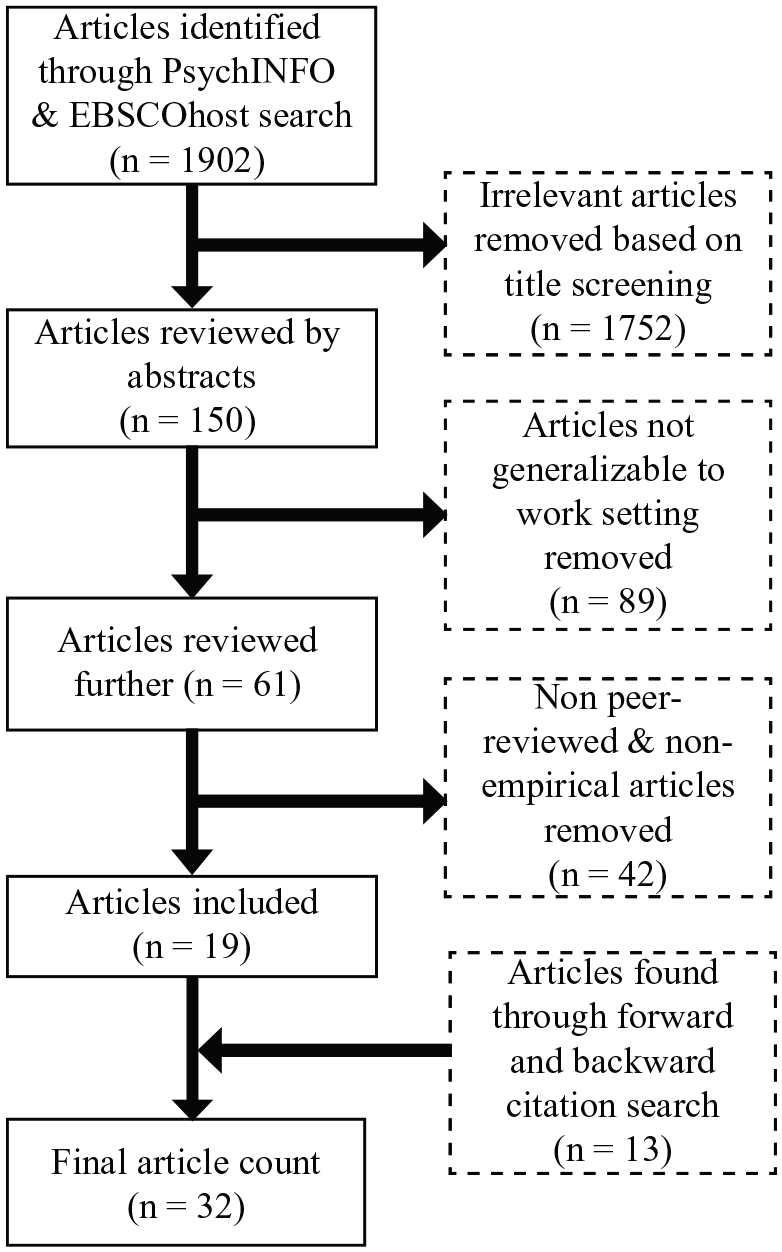
We searched the PsycINFO and EBSCOHost databases with search terms related to teams, physiological measurement systems, and teamwork constructs (see Appendix A for details under each search term). The search was first conducted in February 2017 and updated in December 2017 and December 2018. Our inclusion criteria included (1) peer-reviewed journal articles, (2) teams comprising members who were unrelated to each other (i.e., excludes mother–child or romantic relationships), (3) team tasks and processes that could be generalizable to work settings (e.g., constructing objects, process control, flight simulation, etc.), and (4) TPD measurements obtained when team members were engaged in team tasks.
Figure 2 illustrates the screening process. The initial search in February 2017 produced a total of 1,902 hits. After title and abstract review and limiting to empirical peer-reviewed articles, we retained 19 articles. Forward- and backward-citation searches from these articles produced an additional 13 articles. After further culling articles that were not generalizable to work settings or that had not obtained physiological measurements while participants were engaged in team tasks, our final article count was 32.
Article search strategy.
Coding
Coding methodology was iteratively developed. First, we extracted characteristics of teams that were judged as potentially influencing the development and maintenance of TPD, including team size, mutual familiarity of team members, and the context of measurement, including the team task, task setting, sample expertise, collaboration duration, and times at which measurements were taken.
Next, we coded study findings using the four categories rooted in the IMOI framework as illustrated in Figure 1: inputs, mediators (i.e., processes or emergent states), outputs, and psychometric factors. The intent of this coding was to extract common features relevant to team research from studies originating from diverse disciplines. Examples of psychometric variables included the timing of physiological measurements (e.g., Ahonen, Cowley, Hellas, & Puolamäki, 2018) and attempts to decompose the source of the variance underlying TPD (e.g., shared task demands, co-location; Fusaroli, Bjørndahl, Roepstorff, & Tylén, 2016; Strang, Funke, Russell, Dukes, & Middendorf, 2014). Owing to the wide variation in methodology and reporting of results, including establishment of individual and team physiological baselines, task structures, and the exact nature of experimental manipulations, it was difficult to extract covariates to enable conducting a meta-analysis.
Results
How Do Researchers Use Physiological Measurement in Team Settings?
We characterize how researchers use physiological measures to detect team phenomena, including the types of physiological systems measured, characteristics of teams studied, and methodological details.
What physiological systems are measured?
Figure 3 lists the variables measured within each physiological subsystem. Researchers measure both the central nervous system (CNS; for example, Stevens, Galloway, Wang, & Berka, 2012; Toppi et al., 2016) and the peripheral nervous system (PNS; for example, Chanel, Kivikangas, & Ravaja, 2012; Fusaroli et al., 2016; Henning & Korbelak, 2005).

Classification of physiological systems and their respective measures.
Measures of PNS activity primarily focus on the autonomic nervous system. Cardiac measures reflect activity of the sympathetic and parasympathetic nervous systems and were the most commonly used indicator of physiological activity, accounting for more than half (n = 18; 56%) of the articles. The electrodermal system (n = 11; 34%), in contrast, is a pure reflection of sympathetic activation because it measures the activity of eccrine sweat glands innervated by the sympathetic nervous system alone. Finally, facial electromyography (EMG; n = 5; 16%), a measure of somatic nervous system activity, was used to detect affect through zygomaticus major (ZM; that is, smiling), corrugator supercilli (CS; frowning), and orbicularis oculi (OO; frowning, stress) muscle activity during team events. Ten (31%) studies measured CNS activity using the electroencephalogram (EEG).
A majority of the articles (n = 23; 72%) measured only one system of physiological activation. Of these, cardiovascular measures were the most common (n = 10), followed by EEG (n = 8), electrodermal activity (EDA; n = 4), and facial EMG (n = 1). Simultaneous measurement of multiple systems can help inform the robustness of TPD and the generalizability of findings. Six (19%) articles measured at least two physiological systems or subsystems; of these, four articles measured cardiac activity and EDA. Only two (6%) studies measured both CNS (EEG) and PNS (cardiac, facial EMG) activity. Finally, only three articles (9%) measured multiple subsystems of the PNS: cardiac activity, EDA, and facial EMG activity.
How is individual-level physiological data treated at the team level?
In understanding TPD, it is important to consider how signals from individual team members are aggregated to the team level. Three main types of aggregation strategies were employed: (1) overall activation or arousal levels, (2) synchrony, and (3) organization or stability of patterns of activation. First, researchers used some form of overall arousal levels for individuals (e.g., averaging activation levels over some time) in multivariate analyses or created a team-level measure (e.g., averaging individual scores for the team). Four studies used an overall physiological arousal or activation measure, referred to as physiological activation (PA) in the following sections, including averages (Kivikangas, Kätsyri, Järvelä, & Ravaja, 2014) and magnitude of change in physiological responses compared with a baseline (Sariñana-González, Romero-Martínez, & Moya-Albiol, 2017, 2019).
Second, researchers used various forms of linear and nonlinear synchrony across team members’ physiological dynamics (for a review, see Guastello, 2017), referred to as physiological synchrony (PS) hereafter. These measures capture the degree of similarity over time between TPD but not overall activation levels. Nineteen studies used some form of PS measure, for example, cross-correlation and signal matching, making PS the most common TPD aggregation method.
Third, researchers used methods based in dynamical systems approaches (e.g., recurrence analysis; Knight, Kennedy, & McComb, 2016) to characterize the relative stability, organization, or disorganization (e.g., entropy) of patterns of activation within the team over time. Thirteen studies used some form of stability or organization metric, referred to as physiological organization (PO) hereafter, including cross-recurrence quantification analysis (CRQA) and multidimensional recurrence quantification analysis and cross-fuzzy entropy. Table 1 defines the most common statistical methods that are used for aggregating physiological data within each of these three categories, and the number of papers that use each method.
Definitions of Aggregation Methods Used in TPD
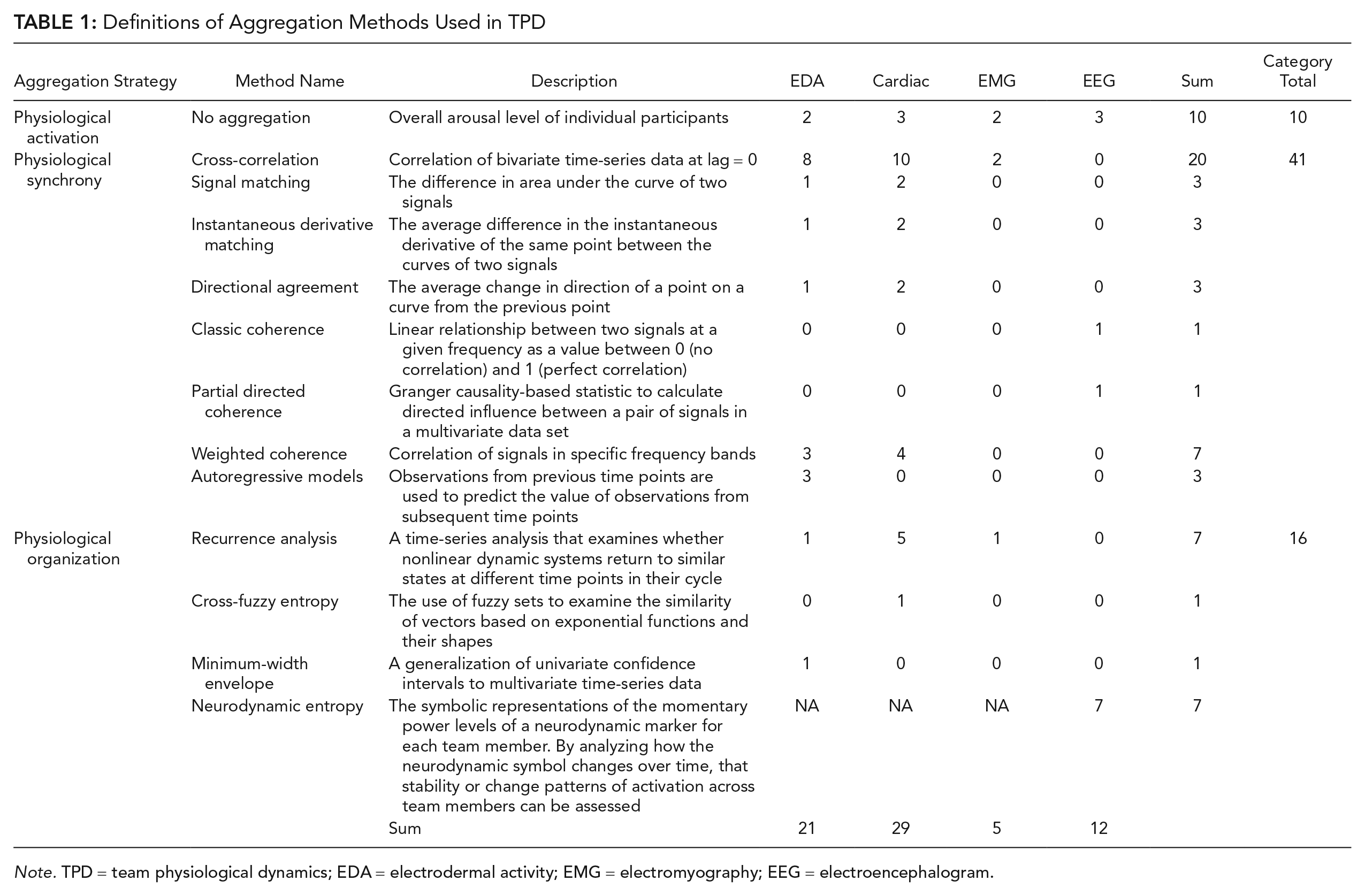
Note. TPD = team physiological dynamics; EDA = electrodermal activity; EMG = electromyography; EEG = electroencephalogram.
It is important to distinguish between measures of TPD that preserve temporal information or characterize sequence or order effects in physiological dynamics, and those that do not. Measures of PS and PO represent temporal dynamics in different ways (e.g., synchrony vs. entropy, respectively) whereas measures of PA aggregate physiological data in a way that much of the temporal information is lost (e.g., a mean level of activation over a performance period includes no information about trends over time or interrelationships between team members). Therefore, PS and PO measures represent either within-person or team changes over time, and PA measures collapse observations across time.
What are characteristics of teams studied?
Three main categories of team characteristics were reviewed based on their known relationships to team functioning (Stewart, 2006) and potential to impact TPD: team size, team task and team member familiarity, and timespan of research.
Team size
Depending on task structure, it is possible that smaller teams engender more frequent or closer interactions with team members, which may affect the level of TPD. Therefore, we reviewed the size of teams. We found that teams largely comprised dyads (n = 19, 59%). In the remaining studies, team size ranged from 3 to 12 members (e.g., Elkins et al., 2009; Håkonsson et al., 2016; Likens, Amazeen, Stevens, Galloway, & Gorman, 2014; Stevens et al., 2012). In these larger teams, however, team size considered for data analysis occasionally differed from the actual size of the team, or the size from which data were collected, for two main reasons. First, researchers sometimes collected data from a subset of the team (e.g., Stevens et al., 2012, collected data only from six members of 12-person teams). Second, data loss due to instrumentation problems meant that researchers had to limit analysis to the subset of team members that produced usable data (e.g., Elkins et al., 2009). The predominance of two-person teams, either by design or because of limitations in data collection, suggest that most findings may be generalizable to teams of dyads.
Team tasks and team member familiarity
Prior familiarity of team members with each other and with the experimental task may influence physiological arousal and, consequently, the development of TPD relationships. Most studies using EEG (n = 8, 25%) were conducted in simulations of job-relevant tasks such as submarine (e.g., Gorman et al., 2016; Likens et al., 2014; Stevens & Galloway, 2016; Stevens et al., 2012; Stevens et al., 2013), health care (Stevens, Galloway, Halpin, & Willemsen-Dunlap, 2016), flight deck (Toppi et al., 2016), and process control (Sciaraffa et al., 2017) operations. Participants in most of these studies were experts or had some level of prior knowledge about and experience with the task (e.g., trainees), which may have influenced their overall arousal levels when engaging with their team members and with the task. Most laboratory studies, in contrast, used college students to study teamwork in video games (e.g., Chanel et al., 2012; Järvelä, Kivikangas, Kätsyri, & Ravaja, 2014) or other tasks such as Lego building (Fusaroli et al., 2016) or origami construction (Håkonsson et al., 2016; Mønster, Håkonsson, Eskildsen, & Wallot, 2016). Lack of familiarity or specialized knowledge in performing these latter types of tasks may affect participants’ understanding of and engagement with the tasks, and thus affect physiological arousal patterns.
A plurality of studies (n = 13; 41%) did not provide information about prior mutual familiarity of team members. In the remaining studies, five (15%) teams comprised friends, nine (28%) consisted of classmates, and five (15%) teams were unfamiliar with each other. A history of interacting with someone may result in faster activation or longer persistence of pre-established physiological arousal patterns. Future research should investigate how TPD fluctuates in response to engaging with novel tasks and unfamiliar team members, perhaps through the establishment of baselines.
Timespan of research
TPD may develop and show fluctuations over a period of time. A majority of the studies (n = 25; 78%) investigated TPD only during a single session. Seven studies (22%) spanned several sessions, which enables a comparison of TPD fluctuations over sessions. However, of these seven studies, five (Gorman et al., 2016; Likens et al., 2014; Stevens & Galloway, 2016; Stevens et al., 2012; Stevens et al., 2013) appeared to use the same sample. Ten studies (31%) lasted 1 hr or less, and the duration of 11 studies (34%) was more than 1 hr, with the range being just over an hour (Wallot, Mitkidis, McGraw, & Roepstorff, 2016) to 2½ hr (Spapé et al., 2013).
Engaging in team-based tasks may influence individual physiological dynamics not only during the team task, but even after completion of the task, which has implications on persisting effects of team engagement on individual health. Twenty-two (69%) studies measured physiology only during team interactions. Most other studies had combinations of evaluation periods before, during, and after team interaction. One study measured physiology only prior to team interaction, which was used to predict task outcomes based on the level of TPD (Elkins et al., 2009). Only two studies measured physiology before, during, and after team interaction (Sariñana-González et al., 2017, 2019).
What Relationships Exist Between Physiological Measures and Team Constructs?
Research has explored relationships between TPD and all three categories of team variables described by the IMOI model as well as a variety of psychometric factors. Appendix B presents summarized findings about specific variables investigated under each general teamwork variable. Findings are organized under three categories to correspond to whether findings about the specific variables are unequivocal, equivocal, or fail to establish a relationship with TPD. Team input and outcome variables dominate the literature. Psychometric variables concern aspects of study design and measurement, and influence the interpretation of the nature of the relationship between TPD and many team input and output variables. Consequently, we report results of the main psychometric factors investigated before summarizing findings for team inputs, mediators, and outputs.
Psychometric Variables
The majority of psychometric evaluations have focused on measures of PS and PO and sought to understand the impact of different statistical methods for detecting synchrony or organization in TPD (e.g., linear vs. nonlinear methods, differences in lag lengths for cross-correlations). Psychometric variables also consider contextual or task factors influencing the magnitude of PS or PO. Three main categories of psychometric variables were identified in the literature: (1) measurement time, (2) aggregation method, and (3) differentiating shared task demands, co-presence, and team-specific or team-generic processes.
Measurement time
The time at which physiological measurements are taken (e.g., early vs. late in the performance episode) interacts with how long team members have collaborated and may influence the development of TPD. The effects of measurement time are reflected in interactions with multiple input variables (e.g., gender, Sariñana-González et al., 2019; role type, Ahonen et al., 2018) and outputs variables (e.g., subjective workload, Ahonen et al., 2016; task outcomes, Ahonen et al., 2018). For example, with regard to an output variable, objective task outcome, Ahonen et al. (2018) found that programmer and commenter dyads in dyads that succeeded in a paired programming task had higher phasic EDA PA before task completion compared with dyads from unsuccessful pairs who showed higher phasic EDA PA after task completion. This variable illustrates how a continuous measurement of TPD not only helps understand the relationship between task outcomes and TPD but also changes in TPD at different time points.
Aggregation method
Researchers often test different aggregation methods for TPD against one another in the same study. Such comparative evaluations help illustrate the sensitivity of aggregation methods in detecting changes in TPD in tasks with a variety of interaction patterns (e.g., simultaneous vs. turn-taking tasks), and inform their validity in predicting relationships between physiological systems, and between physiological dynamics and psychological constructs. Most researchers compare linear aggregation methods (e.g., cross-correlation, signal matching, etc.; Henning et al., 2001; Montague, Xu, & Chiou, 2014); a handful (e.g., Strang et al., 2014) also compare linear and nonlinear aggregation methods. Cross-correlation is a frequently used linear aggregation method that is sensitive to detecting PS aggregated through linear statistical methods in cardiac and EDA systems in studies using simultaneous (Chanel et al., 2012) and turn-based activity (Järvelä et al., 2014). However, Strang et al. (2014), using a task with differentiated roles, found cross-correlation to be less robust than the nonlinear aggregation method of CRQA and cross-fuzzy entropy in detecting cardiac TPD.
Guastello and colleagues compared aggregation methods in their ability to determine optimal lag lengths, that is, the time that elapses before time-series data from two sources align, on EDA PS. Smaller lag lengths (i.e., 1 s) resulted in the highest EDA PS in four- to five-person teams playing an emergency response game (Guastello et al., 2016). In contrast, a larger lag length of 20 s accounted for the greatest proportion variance of EDA PS in a two-person team performing a dual vigilance task (Guastello, 2016). This shows that lag length may depend on the nature of the task, as well as team size. In addition, nonlinear aggregation models were more robust to withstanding lag differences between team members in the dual vigilance task (Guastello, 2016).
Shared task demands, co-presence, and team-specific or team-generic processes
Researchers also attempt to separate sources of variance in TPD by using techniques similar to the nominal group technique used in team idea generation research (e.g., Mullen, Johnson, & Salas, 1991). Specifically, “real teams” of interacting individuals are compared with aggregates of individuals working in isolation. Measures of TPD can then be generated from (1) real interacting teams, (2) nominal groups comprising individuals who completed the task in a dyad but are not from the same dyad, and (3) nominal groups comprising individuals who completed the task in isolation.
Fusaroli and colleagues (2016) used this approach to investigate the effect of shared task demands and collocation on level and duration of cardiac PO in a joint construction task by using CRQA. They found no difference in the level of cardiac PO between dyads comprising real interacting team members versus nominal dyads formed by combining individuals who completed the task in different dyads. This shows that similar task demands, rather than interaction when physically working together, affected cardiac PO. However, Fusaroli and colleagues also found that real interacting teams showed more stable PO during collectively performed activities, showing some influences of interaction on cardiac PO.
In a task with differentiated roles, Strang and colleagues (2014) found cardiac PO in real dyads to be greater than chance, indicating that some proportion of PO could be attributable to shared task and teamwork. At the same time, however, PO in real collaborating dyads was higher than that in nominal dyads formed by pairing individuals working on the task by themselves, indicating the role of interpersonal interaction in PO. Finally, linear aggregation revealed that PO in real dyads was higher than that in nominal dyads comprising members drawn from different teams. However, because nonlinear aggregation methods did not replicate the latter result, Strang and colleagues (2014) concluded that their task required interpersonal dynamics that were not unique to individual teams but instead were common in all teams.
Team Inputs
Existing research primarily explores three categories of team input constructs: individual differences in team composition, team role and task structure, and team task demands.
Individual differences in team composition
Four studies investigate relationships between TPD and trait variables. Higher cardiac PS has been associated with fewer differences in participants’ empathy on a simultaneous action task (Chanel et al., 2012), and higher EMG (OO) PS has been associated with higher empathy in a turn-based action task (Järvelä et al., 2014). Together, these findings suggest that higher levels of empathy are related to cardiac and OO PS. However, findings connecting EDA TPD and empathy are mixed (Guastello, 2016; Järvelä et al., 2014) and may be attributed to differences in task interaction structure and task demands. Other trait variables such as emotional intelligence, coping flexibility, (Guastello, 2016), and hostility (Kivikangas et al., 2014) have not been linked to EDA or EMG TPD.
Another individual difference variable, expertise, has only been examined using EEG. Experienced submarine operator teams show more diverse neural PO during team performance episodes, which may be indicative of greater cognitive flexibility within the team (Gorman et al., 2016; Stevens et al., 2013). In addition, shifts in communication patterns within experienced submarine operator teams precede changes in team neural PO (Gorman et al., 2016), suggesting that shifts in TPD are at least partly driven by reactions to patterns of communication within the team.
Gender’s effects have been investigated in three studies with other types of input variables using cardiac, EDA, and EMG measures. Sariñana-González and colleagues (2017, 2019) measured EDA and cardiac PA in a Lego-based construction task in which participants either compete with each other to simultaneously construct their models or cooperate in a turn-based fashion or construct models by themselves. The effects of gender depended on the physiological system that was measured, the experimental condition, and the time of measurement: Women had lower phasic EDA PA in the cooperation condition before and after the task, but men showed lower phasic EDA PA only after the task (Sariñana-González et al., 2017). In a follow-up experiment measuring cardiac PA, men who experienced failure on the task had higher cardiac PA when they were cooperating on the task than when they were working alone.
Kivikangas and colleagues (2014) also investigated gender differences in competitiveness through distinct tasks in two experiments in which they varied whether interaction structure was simultaneous or turn-based. Simultaneous competition resulted in higher cardiac PA in men, but gender did not have an effect on cardiac PA in turn-based competition. However, men showed higher positive affect through EMG (ZM and OO) PA in both simultaneous and turn-based play. Although there was no evidence of equivocal findings related to gender, two of the three studies failed to detect effects in women on cardiac PA for task outcome, measurement time (Sariñana-González et al., 2019), and cardiac and EMG (ZM and OO) PA for level of competitiveness (Kivikangas et al., 2014).
Team task structure
Researchers measure task structure variables, including team member role type, level of competitiveness, task-induced workload, structure of team task interdependence, awareness about team member actions, and environmental variables such as task location. The effect of a team member’s specific role within the team and TPD has been investigated in four studies, and may depend on the physiological system measured and task characteristics. Stevens and colleagues (2012; Stevens & Galloway, 2016) did not find any effect of team role in a submarine navigation task on shifts in neural PO. However, other researchers have found that participants in more active roles have higher and faster phasic EDA PA (e.g., in programmers who were responsible for designing and actively entering the code in a computer programming task; Ahonen et al., 2018) and higher cardiac PO (e.g., in participants in charge of flying in a flight simulation task; Toppi et al., 2016) compared with participants in relatively inactive roles. Finally, Ahonen and colleagues (2018) found that both members of a programming team had higher phasic EDA PA before task completion and before receiving information about task outcome, but programmers from losing teams had higher phasic EDA PA after task completion compared with commenters from losing teams, thus demonstrating the joint influence of team role and task outcome on PA.
Two research groups have conducted six studies to investigate the effect of level of competitiveness (i.e., cooperation vs. competition) on cardiac TPD and electrodermal PA. Four studies (Chanel et al., 2012; Järvelä et al., 2014; Kivikangas et al., 2014; Spapé et al., 2013) test TPD in different combinations of levels of competitiveness and team members (i.e., human vs. synthetic team member). These studies have consistently found higher ZM and OO PS during human competition in both simultaneous (Chanel et al., 2012) and turn-based tasks (Spapé et al., 2013). Kivikangas and colleagues (2014) also found this pattern in ZM and OO PA in both simultaneous and turn-based tasks, but only in men. Furthermore, although there was higher cardiac PA in men during simultaneous play, there was no effect of gender on cardiac PA during turn-based play (Kivikangas et al., 2014), signaling to potentially different patterns of arousal of the cardiac and EMG systems during different types of interactions. The other research group investigating levels of competitiveness (Sariñana-González et al., 2017, 2019) have found higher EDA PA in cooperation compared with competition (Sariñana-González et al., 2017), and higher cardiac PA in cooperation compared with playing alone. This suggests that levels of competitiveness may have different effects depending on the physiological system in which it is measured.
Finally, interpreting the effect of level of competitiveness also requires accounting for the specific measure of TPD. For example, cardiac PS can be measured in the time domain (e.g., variability in interbeat interval) and the frequency domain (e.g., based on the power spectrum level of heart rate: very low, low, and high). Chanel and colleagues (2012) found differing results with time and frequency domain metrics: Participants had higher cardiac PS in the time domain during human competition but higher cardiac PS in high-frequency cardiac domain during cooperation in a simultaneous play task. In contrast to Chanel’s findings in the frequency domain, Järvelä et al. (2014) found higher cardiac PS in the high-frequency domain during human competition in a turn-taking task. Sariñana-González et al. (2019) also found differences in results from time versus frequency domain measures of cardiac PA. These seemingly different findings not only illustrate the complexities in interpreting physiological signals through a psychological lens but also offer clues about how to add nuance to the interpretation through a consideration of variables that influence physiological activity (e.g., structure of interaction, measurement time, etc.).
Team task demands
Task-induced workload has been investigated by eight studies, making it the most frequently studied variable. Seven studies investigate neural TPD in task-induced workload, of which five studies have been conducted by the same research group (Gorman et al., 2016; Stevens & Galloway, 2016; Stevens et al., 2016; Stevens et al., 2012; Stevens et al., 2013). This research group has found neural PO in submarine operators and health care workers to be sensitive to changes in task-induced workload. However, findings from other research groups are mixed. Sciaraffa and colleagues (2017) found lower neural interconnective density during a high workload condition in the Multi-Attribute Battery (MAT-B) task with naïve participants in contrast to Toppi and colleagues (2016) who found higher neural interconnectivity density during high workload/high cooperation conditions in a flight simulation with experienced commercial pilots.
Toppi and colleagues (2016) also found higher cardiac PA during periods of high workload. Findings on cardiac PS, however, are mixed, and depend on the specific method of aggregation. Montague and colleagues (2014) found higher cardiac PS during higher workload periods on the MAT-B task when aggregating through weighted coherence but were not able to replicate this finding through cross-correlation, signal matching, instantaneous derivative matching, and directional agreement. Montague and colleagues also failed to find any relationship between task-induced workload and EDA PS. These findings indicate the need to consider the effect of variables that can modify the influence of task-induced workload (e.g., participant and task characteristics) on TPD while continuing to refine study design to reliably capture task-induced workload.
One study each has investigated the structure of team task interdependence (Wallot et al., 2016) and awareness about team member actions (Henning et al., 2001) but did not find any significant effects. The two studies investigating playing location have been unable to replicate each other’s findings on cardiac or EMG (ZM or OO) TPD (Chanel et al., 2012; Kivikangas et al., 2014), suggesting the need for future research on these variables.
Team Mediators
Two categories of team mediator variables dominate the relatively small extant research connecting TPD to team mediators: affective emergent states and team process behaviors.
Affective emergent states
The existing research on TPD and affective team emergent states relies on interventions designed to induce specific team affects. Engaging in a trust-building activity is associated with higher cardiac PA and PO in a joint construction task (Mitkidis, McGraw, Roepstorff, & Wallot, 2015). Håkonsson and colleagues (2016) investigated the effects of induced emotions (i.e., priming positive or negative emotional states in individual team members) on EMG (ZM, CS), EDA, and cardiac PA in a task resembling a production assembly line. The same group of researchers (Mønster et al., 2016) then reanalyzed the data to investigate PO and found higher EDA PO before teams were given a choice to adopt a new production routine, and higher ZM PO before the teams decided against adoption of the new production routine, but only in teams that had been induced with positive emotions. Findings around ZM TPD were complex: Håkonsson et al. (2016) found higher ZM PA in members of teams induced with positive emotions, but Mønster et al. (2016) found higher ZM PO in teams induced with negative emotions.
Team process behaviors
Researchers have measured many aspects of behavior toward team members during the task, including how team members coordinate their actions, their ability to work together, team communication effectiveness, and quality of communication in relation to cardiac TPD. Fusaroli and colleagues (2016) found higher level cardiac PO to be associated with higher coordination in physical activity (i.e., behavioral coordination), and with higher and more stable coordination in speech activity between team members in a construction activity.
Other self-reported process behaviors are associated with mixed findings. Henning and colleagues investigated the effect of different patterns of speech activities (e.g., simultaneous vs. turn-taking in speech activity) on perceptions of team process behaviors in six dyads. Associations between cardiac PS during speech activity and perceptions of quality of communication and ability of the team to work together were only found for one of the six dyads, indicating limited generalizability of the findings. Furthermore, although Järvelä and colleagues found self-reported team task interdependence during the task to be associated with cardiac PS, they failed to find any relationship to EDA PS in a turn-based task.
Team Outputs
TPD studies cover four main types of team outputs: objective task performance, perceived workload, team affective outcomes, and team learning outcomes. Team learning outcomes (i.e., likelihood of adopting new production routines) have been discussed in relation to induced emotions, so this section will focus on the first three team output variables.
Objective task performance
Seven studies investigate objective task performance in relationship to TPD, making it the second most frequently studied variable after task-induced workload. TPD studies include task performance measures such as error rates, completion time (e.g., Elkins et al., 2009; Henning, Armstead, & Ferris, 2009), or success versus failure (Ahonen et al., 2018). Many studies have found higher cardiac and neural TPD to be significantly associated with better task performance. For example, higher cardiac PS predicted task completion time (Henning et al., 2001), and higher cardiac PS before experiencing a change in control dynamics was associated with fewer errors (Henning & Korbelak, 2005) on a team tracking task. Higher neural PO is also associated with better performance on a submarine operations task (Stevens & Galloway, 2014).
The effect of task performance on EDA is complex and depends on measurement time and role. Higher EDA PS before task completion was associated with task success, but there was higher EDA PS after task completion in dyads that failed in a programming task (Ahonen et al., 2018). Furthermore, Ahonen and colleagues also found that in dyads that failed the programming task, the participant in the more active role (programmer) had higher EDA PS compared with the participant in the relatively inactive role (commenter). In a dual vigilance task, Guastello (2016) found that having turbulence in EDA PO and greater sensitivity to EDA influences from the coworker were associated with worse performance.
Some researchers have found limited influences of TPD on team performance. For example, Walker, Muth, Switzer, and Rosopa (2013) found that a team indicator of cardiac PA accounted for only 3% of team error in contrast to 10% that was accounted by individual cardiac sympathetic nervous system PA in a process control task. Other researchers have demonstrated differences in effects of task performance on cardiac (Elkins et al., 2009; Strang et al., 2014; Walker et al., 2013) and EDA (Henning et al., 2001; Montague et al., 2014) TPD depending on the methods of data aggregation. These mixed findings help inform the predictive validity of aggregation methods while also testing the robustness of the relationship between teamwork variables and TPD.
Perceived workload
Perceived workload has been investigated by four studies. Guastello and colleagues (2016) found higher fluctuations in electrodermal PS associated with higher perceived workload in an emergency response task, and EDA PS to be associated with physical, temporal, and mental demand, and effort on a dual vigilance task (Guastello, 2016). Ahonen and colleagues (2018) also found that cardiac PA was negatively associated with perceived temporal demand on a computer programming task, but was positively associated with perceptions of performance on a programming task. However, Montague and colleagues (2014) did not find perceived workload on a monitoring and vigilance task to be related to either cardiac or EDA PS that was aggregated through cross-correlation, directional agreement, instantaneous derivative matching, and signal matching. The diversity of study designs, task demands, and aggregation methods may account for the varied nature of findings on subjective workload.
Team affective outcomes
Seven studies in-vestigate the relationship between affect toward the team and TPD. The findings depend on dynamics of the team task, the specific affective variable, and the aggregation method. Higher feelings of negative affect have been associated with higher cardiac PS in both simultaneous (Chanel et al., 2012) and turn-based tasks (Järvelä et al., 2014), higher EMG (CS) PS in simultaneous tasks, lower EMG (ZM and OO) PS in turn-based tasks (Spapé et al., 2013), and higher EDA PO in a production assembly line task (Mønster et al., 2016). However, Järvelä and colleagues (2014) were unable to establish a relationship between negative affect and EDA PS in a turn-based task. Findings on team cohesion also depend on aggregation method. Strang and colleagues (2014) found higher cardiac TPD to be associated with higher cohesion, but only when aggregated through cross-fuzzy entropy, but not cross-correlation or CRQA.
Discussion and Recommendations
The study of physiology in groups has spanned diverse settings: romantic couples, friends, parents and their children, and even therapists and their patients (Palumbo et al., 2017). Extending this line of research to the physiological dynamics of members of collaborative task performing work teams is not new (e.g., Henning et al., 2001). However, research in this area has expanded considerably in recent years. The results of this review indicate a small but promising set of research on measuring physiology in team settings. In the following section, we describe key findings and themes emerging from this review, and suggest recommendations to develop future research, ranging from conceptualization of TPD, study design, data acquisition and processing, and statistical analysis.
Develop a Theory-Driven Approach to TPD
The TPD field may benefit from teamwork frameworks and theories to formulate research questions and testable hypotheses, and teamwork researchers may benefit from exploring more bounded theories of physiology in groups and dyads not yet applied to work team research. For example, examining the current research in terms of the IMOI framework makes it apparent that TPD has focused primarily on team inputs and outputs. The study of mediators and processes is underdeveloped. Existing studies linking process variables such as communication with TPD are promising (Gorman et al., 2016), and may help in developing predictive aids to diagnosing maladaptive team states and cue appropriate interventions or countermeasures. Theoretical conceptualizations of TPD can be improved by specifying the evolution of TPD over time (Luciano et al., 2018). Team process behaviors are conceptualized as emerging through two types of processes: compositional or compilational (Kozlowski & Klein, 2000). Compositional emergence is characterized by convergent dynamics (i.e., people within a team become more homogeneous over time on some dimension; for example, trust increases, a shared mental model develops). A compositional form of emergence in TPD could include increasing similarity in measures of cardiac functioning as a team progresses through a task. Compilational emergence involves divergent dynamics (i.e., people within a team become more heterogeneous over time; for example, specialized skills or knowledge for different team roles are developed as the team interacts). These dynamics may show fluctuations over time, within-team variability, and different growth trajectories (Kozlowski, 2015). In the case of TPD, it is important to understand what types of emergence have been observed in the literature and what these dynamics indicate about the team.
In the current literature, TPD is most commonly treated as a compositional emergent phenomenon (PA, PS) and sometimes as a compilational phenomenon (PO), but rarely as both within the same study unless they are being compared with one another. There is evidence that composition and compilation conceptualizations can be differentially appropriate based on the situation. For example, using linear methods for generating metrics of PS may be appropriate for tightly coupled teams where all members share similar task demands (e.g., Järvelä et al., 2014). Conversely, nonlinear methods may be more appropriate for teams with more diverse collaboration patterns (e.g., Fusaroli et al., 2016). Characterizing the entire performance period through a single process ignores the potential of TPD to vary and evolve over time within the same team (Kozlowski, 2015). We need a better understanding of situations under which either or both conceptualizations of TPD are appropriate.
An increasingly large set of theories and streams of research outside of the traditional work team literature can help inform the development of theory for work team TPD. For example, work in joint action (Sebanz, Bekkering, & Knoblich, 2006), interpersonal coordination (Marsh & Richardson, 2009), interactive alignment (Garrod & Pickering, 2009), and mirroring and coupled dynamics (Hassan & Firth, 2016) from basic cognitive science research address related phenomenon. These research streams do not necessarily focus on work teams as a context but do explore physiology and interpersonal interactions in ways that can inform TPD research in work teams. Expanding studies in the process/mediators domain can also help inform conceptualizations of teams as complex systems (Arrow et al., 2000), and dynamic theories of team interaction such as Interactive Team Cognition (ITC; Cooke, Gorman, Myers, & Duran, 2013). The ITC theory proposes that team cognition is an activity that emerges from interactions between team members. Team cognition can be understood by considering patterns of communication and coordination within the context of work. Using dynamic theories of team cognition as a theoretical lens can help TPD researchers answer a variety of questions, including the reciprocal effect of team-level interactions on individual- and team-level physiological dynamics, evolving trajectories of multiple dynamical phenomena (i.e., individual physiological dynamics and TPD, communication), and patterns of overlap in these trajectories.
Operationalize Physiological Signals in Terms of Team Constructs
Physiological signals within team settings should be operationalized in terms of the team construct of interest. Operationalization should also include clarification of the measurement context, including occurrence of convergent and/or divergent work processes during the measurement period. This is especially important for physiological dynamics because the same phenomenon (e.g., elevated heart rate variability) can have competing interpretations. Using a “measure fit” process (Luciano et al., 2017), including defining the team construct (e.g., team affect, cognition, behavior, workload) and features of the measurement method and context, can help in aligning the theoretical construct with its appropriate measure.
Cacioppo, Tassinary, and Berntson’s (2007) three dimensions of psychophysiological relationships can also guide operationalization. First, researchers should consider generality, or whether psychophysiological phenomena are dependent on the measurement context. It is possible for the same phenomenon (e.g., elevated heart rate) to occur during different measurement contexts (e.g., manipulation of psychological stress vs. manipulation of task engagement). Specificity is concerned with whether a physiological phenomenon can be mapped to a single team variable or whether many-to-one mappings exist. Sensitivity concerns the degree of change required to occur in a psychological variable to be reflected as a change in a physiological process. Appropriate operationalization in terms of the measurement context can help successfully describe how physiological data represent manifestations of specific team constructs.
Develop Methodological and Reporting Standards in TPD
There is wide variability in study methodologies and reporting of key variables, which makes it difficult to not only interpret the findings of individual studies but also establish the reliability and validity of the field in general. Therefore, it is critically important for the TPD field to establish standards to guide the study of physiology in teams. This entails extracting best practices from the fields of physiological dynamics and team research for study design, data collection, and technical reporting on variables affecting teamwork and the development of TPD. For example, there is inconsistency in reporting teamwork and task work variables affecting TPD. Based on current findings, we recommend reporting prior familiarity between team members, whether team members have a history of shared work experiences, and familiarity with the task and the setting.
There is also a need to improve baseline measurement of individual physiological dynamics and TPD. When establishing baselines, it may be helpful to consider the sources of variance attributable to shared team physiology. At the most basic level, we can consider the baseline physiology of individual team members. To control for the effects of social interaction, it may be advisable to measure baselines of individual team members at rest and in isolation. Another source of variance, the effect of others’ presence on individual physiology, can be obtained through simultaneous measurements of individual team members who are collocated but not interacting. In the next step, the effect of nontask interaction can be obtained by having collocated individuals engaged in conversation while measuring their individual physiologies. Finally, the effect of task work and teamwork on baseline physiology can be measured during practice trials in which team members collaborate to accomplish the task.
Researchers should also follow best practice guidelines for statistical processing and analysis. This begins with using standard methods to detect and remove artifacts from physiological data. If linear statistical analyses (e.g., correlation coefficient) are planned then the appropriate transformations (e.g., converting nonstationary data to stationary) should be performed on the data. Developments in statistical analysis software (e.g., LedaLab, Physioscripts; Christie & Gianaros, 2013) on different types of programs (i.e., MATLAB, R, Python) have automated many steps. During statistical analyses, it is important to be mindful of Type I errors by adjusting the alpha value by the total number of desired tests. This statistical correction is rarely computed or reported in the current literature (see Järvelä et al., 2014; Montague et al., 2014).
Expand TPD Beyond Measures of Single Systems
Cardiovascular measures, either by themselves or in conjunction with other measures, are the most commonly used indicator of TPD. It is relatively rare for researchers to simultaneously measure more than one subsystem under the PNS, and rarer still for measurements to span across the CNS and PNS. However, due to the complex nature of interpersonal physiology, studies that only use a single measure of physiology may not capture a meaningful representation of general patterns in TPD.
The simultaneous analysis of multiple signals offers many benefits. First, it can help establish the relative sensitivity of different physiological systems to team research manipulations (e.g., lag differences in inter-physiological measurement in detecting team phenomena) and can improve predictive power. Second, it is a conceptually robust approach as human responses naturally involve multiple interacting physiological and psychological subsystems. However, it is a difficult undertaking, as it involves parsing intra-individual variability across time within the same measure and different measures, while also capturing this variability across the team.
There are two general approaches to combine information across sensors: across subjects and within subjects. Couplings between physiological parameters within subjects is rare but could generate new insights. Inter-parameter coupling might change, for example, under stressors of various kinds. Individual parameters might stay within their normative bounds while their interactions might deviate from these bounds; this could provide additional discriminatory information.
Extending measurements across multiple physiological subsystems can also add to contextual information that helps clarify the nature of the team construct. For example, knowing that there has been excitation in EDA without further context makes it unclear if the excitation is representing a positive or negative emotional response. To address this, Håkonsson and colleagues (2016) used two measures of facial EMG, indicating smiling and frowning, to show that heighted EDA was associated with positive emotions. In addition, use of multiple measures can help advance inter-measure reliability in capturing psychological and sociological phenomena.
One challenge to multiphysiology measurement is contending with the highly obtrusive nature of measures. Such measures of physiological activity typically impose physical constraints by limiting mobility. The use of newer technology, such as higher quality physiological wrist sensors, and emerging methods of contactless measurement of physiological states (Wei et al., 2018) present great promise to the field because they allow for the unobtrusive collection of multiple physiological measurements.
Develop Methods of Statistical Modeling and Aggregation of TPD
Currently, there are three main strategies of data aggregation (PA, PS, and PO). PS is the most frequently used aggregation strategy and characterizes compositional TPD. In addition to the extant approaches in PS, statistical advances in modeling physiological patterns in dyads can also help understand compositional patterns in TPD (Gates & Liu, 2016; Liu, Zhou, Palumbo, & Wang, 2016). The stability and influence model (Thorson, West, & Mendes, 2018) uses multilevel modeling approaches to model dependencies between repeated measures of data within the same individual (i.e., stability), and influences from partners. Helm, Miller, Kahle, Troxel, and Hastings (2018) describe three patterns of dyad dynamics. Trend synchrony describes a pattern in which physiological dynamics of both members of a dyad fluctuates around similar statistical trends (i.e., linear, quadratic, cubic) across time. Concurrent synchrony is concerned with a micro level of temporal analysis and investigates moment-to-moment de-trended changes in dyad dynamics. Lagged synchrony is also de-trended and examines the direction of dynamic influence between dyad members.
In general, there is the need for analysis and modeling methods that naturally incorporate and visualize multidimensional data. Some of the PO-based nonlinear dynamics approaches (e.g., Guastello et al., 2016; Stevens et al., 2016) that use attractors in high-dimensional state spaces could be helpful. Such methods have been used to examine nonlinear properties such as fractal representations (Likens et al., 2014), and system entropy or complexity (e.g., Gorman et al., 2016). Recurrence analysis (Knight et al., 2016) is another PO-based approach that has been used to uncover and model the temporal structure of data from two or more time-series over time, understand when systems return to similar states (e.g., Fusaroli et al., 2016), and reveal the predictability of temporal patterns (e.g., Mønster et al., 2016). Nonlinear forecasting is another type of nonlinear method in which future points are predicted based on nearest neighbors in the state space. These are model-free methods.
Model-based methods driven by specific hypotheses derived from known individual physiology and team dynamics would be more powerful. Structural Equation Modeling (SEM) embodies a structure or a hypothesis-driven model, and naturally incorporates latent or unobserved variables. This could be especially useful in the realm of TPD as the data produced by physiological sensors are not necessarily the variables that are of most interest (i.e., psychosocial and team constructs). SEM can also incorporate cofounding variables such as environmental factors (time of day, lighting level, etc.), contextual factors (e.g., interaction dynamics), or physical state of team members (fatigue, nutritional status, etc.) that are known to affect individual and team physiology.
Some aggregation approaches draw from both PS and PO (e.g., Guastello, 2016; Guastello et al., 2016) making the boundaries between these types of analysis and conceptualizations of TPD less discrete. This is an opportunity to expand research on clarifying the nature and construct of TPD, including understanding its primary dimensions.
Advance Study and Methods of Psychometric Evaluation in TPD
The TPD field has already made an encouraging start in understanding the sources of variance underlying TPD. For example, Strang and colleagues (2014) demonstrate the contribution of variables such as common task demands and collocation on TPD. By shedding light on nonteam factors (e.g., similar physical and cognitive demands induced by engaging in the same task) that may contribute to PA, such research can inform consideration of control variables in future studies on team physiology. Generalizability theory (Shavelson, Webb, & Rowley, 1989) involves identification and quantification of sources of systematic and error variance underlying behavioral measurements, and can be applied to TPD research to inform understanding of facets (e.g., team role) that drive variance in team-level data.
Multitrait multimethod measurement using time-series data can also help advance psychometrics in TPD. Robust methods of data collection should be used to capture a broader range of variables across the IMOI spectrum. Levenson and Gottman (1983) established the validity of cardiovascular, vascular, muscle, and skin conductance activity in measuring marital satisfaction by comparing them against communication content and self-reported valence. Establishing the construct and criterion validity of physiological measures in team research is critical and can be similarly established by comparing them against more traditional measures of teamwork constructs including observational forms, self-report surveys, or other organizational outcomes. Once physiological measures have been established as reliable and valid indicators of team states and processes, they can then be used in place of other measures of team constructs that require intensive coding, for example, communication.
Move TPD Research From the Lab to the Field
Historically, physiological measurement required extensive instrumentation and limited participant mobility. Consequently, a majority of the research on TPD is conducted in the laboratory. Although laboratory studies afford experimental control, they also have drawbacks. First, tasks used in laboratory research typically either have low realism and fidelity, or fail to embody critical features about work settings that may influence teamwork. Second, the sample pool of a typical participant in a laboratory experiment (i.e., college students) may not have access to strategies and work processes of experts, thus limiting the generalizability of research to work settings. A third cost is the relative expense of establishing experiments or simulations with expert samples compared with instrumenting them in field settings.
Advances have been made in studying TPD of experts such as submarine operators, pilots, and health care workers in simulated work settings using EEG (e.g., Stevens et al., 2016; Stevens et al., 2012; Toppi et al., 2016). There is a need to expand TPD research to field settings by also studying other autonomic nervous system processes. Unobtrusive and wearable sensors provide the opportunity to study teamwork in situ. The ability to freely ambulate in the environment can also enable greater diversity in the types of tasks and teams that could then be brought under the scrutiny of systematic physiological research. In addition, it can also allow for better understanding of the influence of the physical environment on emergent processes such as task restructuring, formation of subgroups, team collaboration, and strategy use. In addition, study setting is an important moderator of relationships between other team constructs and performance with effect sizes being larger in field studies (e.g., Bell, 2007).
Replicate Studies in TPD
At the present time, it is challenging to make conclusive statements about the relationship between physiological variables and team constructs. One reason is that there are insufficient studies investigating the link between specific team variables and TPD. In addition, diversity in task structure, measurement processes, and analysis and reporting standards make it difficult to compare results across studies, even for the same construct. Increasing research focused on disambiguating these findings is important.
Some research groups appear to use the same sample across multiple studies (e.g., Gorman et al., 2016; Kivikangas et al., 2014; Stevens et al., 2012; Spapé et al., 2013). It is essential to replicate these studies with different samples to investigate the generalizability of findings. Replication studies can also enrich the field by establishing reliability of findings across different types of samples and across different physiological systems, and test for boundary conditions of TPD, for example, by varying interaction structures.
Conclusion
There is a small but growing literature on TPD. The findings are encouraging, but widely varied, as are the experimental designs, methods of data acquisition, processing, and analysis. Maturing the field of TPD provides unique opportunities to advance the science of teams with more dynamic and unobtrusive methods of interaction analysis that are scalable and feasible to implement in field settings. However, much work is needed in conceptualizing TPD, grounding TPD in theories of team interaction, and formalizing methods of measurement and analysis. Addressing these challenges will require transdisciplinary approaches drawing from psychology, engineering, physiology, and informatics.
Key Points
We critically reviewed the use of physiological measurement in team settings to investigate how researchers related physiological measurement to theoretical team constructs, and whether there was validity evidence supporting the use of such sensors.
After reviewing 32 articles that measured CNS and PNS activity of participants who engaged in team-based tasks, we found that researchers tended to limit measurements to single physiological systems, and favored testing relationships between team physiology and team inputs and outputs.
We recommend several strategies to better connect the field of TPD to theoretical concepts in teams research, improve practices in measuring team-based phenomena through physiological sensors, and expand statistical methods to analyze these complex data.
Footnotes
Appendix
Summarized Results Depicting Relationships Between Physiology and Team Input, Mediator, and Outcome Variables

| Variable Name | Studies | Significant Findings—Unequivocal | Significant Findings—Equivocal | No Relationship |
|---|---|---|---|---|
| Trait variables (I) | 1. Chanel, Kivikangas, and Ravaja (2012)
2. Järvelä, Kivikangas, Kätsyri, and Ravaja (2014) 3. Kivikangas, Kätsyri, Järvelä, and Ravaja (2014) 4. Guastello (2016) |
1. Higher cardiac PS in the time domain was associated with fewer differences between participants’ empathy in a turn-based task (Järvelä et al., 2014) 2. Higher facial EMG (OO PS) was associated with higher empathy in a simultaneous action task (Chanel et al., 2012) |
1. Being lesser influenced by co-workers EDA arousal levels was associated with higher empathy (EDA PS) and anxiety levels (EDA PO) in a vigilance task (Guastello, 2016), but Järvelä et al. (2014) did not find any effect of EDA PS on empathy in a turn-based task | 1. EDA PS and PO and emotional intelligence and coping flexibility (Guastello, 2016) 2. Facial EMG (CS PA) and hostility (Kivikangas et al., 2014) |
| Expertise (I) | 1. Gorman et al. (2016)
2. Stevens et al. (2013) |
1. Experienced submarine operator teams had higher levels of neural PO and greater task success (Gorman et al., 2016, Stevens et al., 2013) 2. Communication by experienced submarine operators precedes team neural PA (Gorman et al., 2016) |
||
| Gender (I) | 1. Kivikangas et al. (2014)
|
1. Higher cardiac PA in time domain in women in a construction task (Sariñana-González et al., 2019) |
1. Cardiac PA in the time domain in women and time of measurement (before, during, and after a construction task, Sariñana-González et al., 2019) |
|
| Role (I) | 1. Ahonen, Cowley, Hellas, and Puolamäki (2018)
|
1. Higher and faster phasic PA in programmers than commenters (Ahonen et al., 2018) |
1. Neural PO of team and team roles (Stevens & Galloway, 2016; Stevens et al., 2012) | |
| Level of competitiveness (competition vs. cooperation; I) | 1. Chanel et al. (2012)
|
1. Higher facial EMG (ZM and OO) PS in human competition during simultaneous (Chanel et al., 2012) and turn-based play (Spapé et al., 2013) |
1. Higher cardiac PA in the time domain in men during human competition in simultaneous play, but no effects of gender on cardiac PA in turn-based play (Kivikangas et al., 2014) |
1. Cardiac PA in the time domain and facial EMG (ZM and OO) PA and level of competitiveness in simultaneous and turn-based play in women (Kivikangas et al., 2014) |
| 5. Sariñana-González et al. (2019) found higher cardiac PA in the time domain during turn-based cooperation compared with working alone when measured pre-, during, and post-test, but higher low-frequency cardiac PA in the frequency domain pre-test when working alone compared with cooperation | ||||
| Task-induced workload (I) | 1. Stevens et al. (2012)
|
1. Neural PO is sensitive to major task changes (Gorman et al., 2016; Stevens & Galloway, 2016; Stevens et al., 2016; Stevens et al., 2012; Stevens et al., 2013), and occurrence of unexpected events (Stevens & Galloway, 2014; Stevens et al., 2016; Stevens et al., 2012)2. Neural PO entropy reduces when problems are encountered, but increases as they are resolved (Stevens & Galloway, 2014) |
1. Higher cardiac PS in the high-frequency domain (Montague et al., 2014) in higher workload conditions when aggregated through weighted coherence, but not replicated with aggregation methods of cross-correlation, signal matching, instantaneous derivative matching, and directional agreement |
1. EDA PS and task-induced workload (Montague et al., 2014) |
| Structure of team task interdependence (I) | 1. Wallot, Mitkidis, McGraw, and Roepstorff (2016) | 1. Cardiac PS in the time domain and structure of team task independence (Wallot et al., 2016) | ||
| Playing location (home vs. laboratory; I) | 1. Chanel et al. (2012)
|
1. Chanel et al. (2012) found higher cardiac PS in the low-frequency domain when playing at home in a simultaneous play task, but Kivikangas et al. (2014) did not find any relationship between playing location and cardiac PA in the time domain |
||
| Real-time visual feedback on team member actions (I) | 1. Henning, Boucsein, and Claudia Gil (2001) | 1. Cardiac PS in the time and frequency domains and EDA PS and real-time visual feedback on team member actions (Henning et al., 2001) | ||
| Induced emotion (positive vs. negative; M) | 1. Håkonsson et al. (2016)
|
1. Higher EDA PO in teams induced with positive emotions before being provided a choice to adopt a new production routine. There was no effect of negative emotion induction on pre- vs. post-choice EDA PO activity (Mønster et al., 2016) |
1. Higher facial EMG (ZM) PA in individual team members with induction of positive emotions in a production assembly line task (Håkonsson et al., 2016), but a re-analysis of the same dataset showed higher facial EMG ZM PO in team members after induction of negative emotions (Mønster et al., 2016) | 1. Induced emotion and cardiac PA and PS and facial EMG (CS) PA in a production assembly line task (Håkonsson et al., 2016; Mønster et al., 2016) |
| Communication (M) | 1. Stevens et al. (2012)
|
1. Transitions in team neural PO correspond to changes in topics under discussion by the submarine team (Stevens et al., 2012) |
||
| 2. Changes in neural PO of experienced submarine operators during a submarine navigation team task occur after communication exchanges between the members (Gorman et al., 2016) | ||||
| Trust induction: Self-reported team interaction vs. trust building activity (M) | 1. Mitkidis, McGraw, Roepstorff, and Wallot (2015) | 1. Higher cardiac PA and PO in the time domain in teams who engaged in trust building activity compared with teams that completed self-report on team interaction in a joint construction task (Mitkidis et al., 2015) | ||
| Coordination in construction activity (i.e., simultaneous construction activity; M) | 1. Fusaroli, Bjørndahl, Roepstorff, and Tylén (2016) | 1. Higher cardiac PO in the time domain associated with higher simultaneous construction activity (Fusaroli et al., 2016) | ||
| Coordination in speech activity (i.e., simultaneous speech activity; M) | 1. Fusaroli et al. (2016) | 1. Higher cardiac PO in the time domain associated with more stable speech coordination; more stable cardiac PO associated with higher and more stable speech coordination (Fusaroli et al., 2016) | ||
| Objective task performance (O) | 1. Henning et al. (2001)
|
1. Higher neural PO was associated with better task performance (Stevens & Galloway, 2014) |
1. Walker et al. (2013) found cardiac indicators in the time domain of SNS activity of individual team members to be more robust predictors of team error than team SNS and parasympathetic indicators: |
|
| 5. Stevens and Galloway (2014)
|
2. Higher cardiac PS in the time domain before experiencing a change in task control dynamics was associated with fewer errors, but did not have an effect on other performance measures (e.g., collision severity (Henning & Korbelak, 2005) |
a. Individual indicators of cardiac SNS activity in the time domain have different patterns of relationship with team error in a process control task: Lower individual LVET in both participants was associated with lower team error. However, higher PEP in the participant who controlled the first tank in the process control activity, but lower PEP in the participant who controlled the second tank was associated with lower team error |
||
| 3. Higher cardiac PS in the high-frequency domain (logE RSA) when aggregated through cross-correlation and directional agreement, and in the time domain (mean IBI) aggregated through direction agreement during training for a physical building clearing friend vs. foe task was associated with higher team performance during the task. However, other combinations of aggregation methods and dependent measures spanning both time and frequency domains (e.g., cross-correlation of mean IBI and RSA, and directional agreement of RSA) found no relationship between cardiac activity and team performance (Elkins et al., 2009) |
||||
| 7. Higher EDA PS was associated with worse performance on a resource management subtask of a process control task when aggregated through signal matching but not directional agreement, instantaneous derivative matching, cross-correlation, or weighted coherence (Montague et al., 2014) | ||||
| Self-report behavior toward team member(s): behavioral involvement (interdependence between team members’ actions), team communication effectiveness, quality of communication, ability to work together (O) | 1. Henning, Armstead, and Ferris (2009)
|
1. Higher cardiac PS in the time and frequency domains was associated with higher team members’ mutual interdependence, and fewer differences between team member’s self-reported mutual interdependence (Järvelä et al., 2014) | 1. Higher cardiac PS in the time domain during highly correlated speech between team members associated with lower quality of communication, but only for one (of six) dyad (Henning et al., 2009) |
1. EDA PS and self-reported team interdependence (Järvelä et al., 2014) |
| Subjective workload (O) | 1. Montague et al. (2014)
|
1. In an emergency response task, Guastello et al. (2016) found higher perceived effort to be associated with steadier EDA PA, higher perceived physical demand to be associated with being lesser influenced by co-workers’ EDA PA, higher perceived mental demand to be associated with lower Lyapunov exponents, and higher perceived temporal demand to be associated with higher Lyapunov exponents and EDA PO being lesser influenced by co-workers’ PA (Guastello et al., 2016) |
1. Subjective workload on a process control task and cardiac PS in the time domain and EDA PS (Montague et al., 2014) | |
| 2. In a programming task, cardiac PA in the time domain negatively predicted 20% to 50% of variance in perceived temporal demand with one dependent measure, and positively predicted 4% of variance in perceived performance for one dependent measure at shorter time scale (Ahonen et al., 2016) | ||||
| Adoption of new taskwork strategy (O) | 1. Håkonsson et al. (2016)
|
1. Higher facial EMG (ZM) PO prior to being provided a choice to adopt a new production routine resulted in greater likelihood of deciding to adopt the new routine in an assembly line task (Mønster et al., 2016) |
1. Decision about adoption of new production routine had no effect on facial EMG (ZM and CS PA, Håkonsson et al., 2016); however, Mønster et al. (2016) found lower facial EMG (ZM) PO after adoption of new production routine | |
| Self-report affect toward team member(s): negative feeling, trust, collective competence, relatedness to group, team cohesion (O) | 1. Chanel et al. (2012)
|
1. Higher cardiac PS in the frequency domain was associated with higher negative feelings toward team members in a simultaneous play task (Chanel et al., 2012), and fewer differences in negative feelings between team members in a turn-based task (Järvelä et al., 2014) |
1. Higher cardiac PO in the time domain associated with higher perceived team cohesion and team trust when aggregated through cross-fuzzy entropy in a cooperative team task with differentiated roles. However, when aggregated through cross-correlation (PS) and cross-recurrence quantification analysis (PO), there was no relationship between team cardiac activity and team cohesion or team trust (Strang et al., 2014) |
1. EDA PS and negative feelings toward team members in a turn-based task (Järvelä et al., 2014) |
| 3. Higher facial EMG (ZM) PO was associated with higher self-reported team cohesion (relationship orientation and positive affect toward team members) in a production assembly line task (Mønster et al., 2016) |
2. Higher cardiac PO in the time domain was associated with higher expectation of material return on investment in a public goods game (a proxy for team trust), but actual material investment in the game was not associated with cardiac activity (Mitkidis et al., 2015) | |||
| Cognition about team: comprehension (mutual understanding of team members), team productivity (O) | 1. Henning et al. (2009)
|
1. Higher cardiac PS in the frequency domain associated with higher comprehension in a turn-based task (Järvelä et al., 2014) | 1. Higher cardiac PS in the time domain during highly correlated speech between team members associated with lower team productivity, but only for one (of six) dyad (Henning et al., 2009) | 1. EDA PS and comprehension in a turn-based task (Järvelä et al., 2014) |
Note. PS = physiological synchrony; EMG = electromyography; OO = orbicularis oculi; EDA = electrodermal activity; PO = physiological organization; CS = corrugator supercilli; PA = physiological activation; ZM = zygomaticus major; SNS = sympathetic nervous system; LVET = left ventricular ejection time; PEP = pre-ejection period; PNS = peripheral nervous system; RSA = respiratory sinus arrhythmia; IBI = interbeat interval.
Acknowledgments
This work was supported by a grant from the National Aeronautics and Space Administration (#NNX17AB55G; PI: MA Rosen). Michael A. Rosen is also affiliated with Johns Hopkins University, Baltimore, Maryland, USA.
Sadaf Kazi was a human factors specialist at the Armstrong Institute for Patient Safety and Quality at the Johns Hopkins University School of Medicine. She received a PhD in engineering psychology from the Georgia Institute of Technology in 2016. She is a research scientist at the Medstar National Center for Human Factors in Healthcare where she conducts research on the influence of complex adaptive systems on cognitive work.
Salar Khaleghzadegan is a senior research program coordinator at the Armstrong Institute for Patient Safety and Quality at the Johns Hopkins University School of Medicine. He received a BS in biological sciences at the University of Maryland Baltimore County (UMBC) in 2014 and is pursuing a Master of Public Policy with a concentration in Health Policy at UMBC.
Julie V. Dinh is a doctoral student in the Department of Psychological Sciences at Rice University. She received an MA in industrial/organizational psychology from Rice University in 2018.
Mark J. Shelhamer is an associate professor in otolaryngology at the Johns Hopkins University School of Medicine and conducts research on sensorimotor adaptation, human spaceflight, and complex systems. He received an ScD from the Massachusetts Institute of Technology in 1990. From 2013 to 2016, he served as chief scientist of the NASA Human Research Program.
Adam Sapirstein is an associate professor in the Department of Anesthesiology and Critical Care Medicine at the Johns Hopkins University School of Medicine. He received an MD from the Penn State College of Medicine in 1988, and completed his residency and fellowship in Anesthesiology and Critical Care Medicine from Massachusetts General Hospital in 1992 and 1993, respectively.
Lee A. Goeddel is an assistant professor in the Department of Anesthesiology and Critical Care Medicine at the Johns Hopkins University School of Medicine. He received an MD from the Johns Hopkins University School of Medicine in 2011, completed his residency in anesthesiology from the University of Alabama Hospital in 2015, and fellowships in Cardiothoracic Anesthesiology and Anesthesiology and Critical Care Medicine from the Johns Hopkins University School of Medicine in 2016 and 2017, respectively.
Nnenna O. Chime is a post-doctoral fellow in Pediatric Critical Care Medicine at the Johns Hopkins University School of Medicine. She received an MD from the University of Nigeria and received an MPH from the Johns Hopkins Bloomberg School of Public Health.
Eduardo Salas is professor and chair of the Department of Psychological Sciences at Rice University where he conducts research on team effectiveness, teamwork, and team training. He received a PhD from Old Dominion University in 1984.
Michael A. Rosen is an associate professor at the Armstrong Institute for Patient Safety and Quality and the Department of Anesthesiology and Critical Care Medicine at the Johns Hopkins University School of Medicine with joint appointments at the Bloomberg School of Public Health and the School of Nursing at Johns Hopkins University. He received a PhD in applied experimental and human factors psychology from the University of Central Florida in 2010.