
Abstract
Objective
This study examined a system-level perspective to investigate the changes in the whole trunk and head postures while sitting with various lower extremity postures.
Background
Sitting biomechanics has focused mainly on the lumbar region only, whereas the anatomy literature has suggested various links from the head and lower extremity.
Method
Seventeen male participants were seated in six lower extremity postures, and the trunk kinematics and muscle activity measures were captured for 5 s.
Results
Changes in the trunk-thigh angle and the knee angle affected the trunk and head postures and muscle recruitment patterns significantly, indicating significant interactions between the lower extremity and trunk while sitting. Specifically, the larger trunk-thigh angle (T135°) showed more neutral lumbar lordosis (4.0° on average), smaller pelvic flexion (1.8°), smaller head flexion (3.3°), and a less rounded shoulder (1.7°) than the smaller one (T90°). The smaller knee angle (K45°) revealed a more neutral lumbar lordosis (6.9°), smaller pelvic flexion (9.2°), smaller head flexion (2.6°), and less rounded shoulder (2.4°) than the larger condition (K180°). The more neutral posture suggested by the kinematic measures confirmed significantly less muscular recruitment in the trunk extensors, except for a significant antagonistic co-contraction.
Conclusion
The lower and upper back postures were more neutral, and back muscle recruitment was lower with a larger trunk-thigh angle and a smaller knee angle, but at the cost of antagonistic co-contraction.
Application
The costs and benefits of each lower extremity posture can be used to design an ergonomic chair and develop an improved sitting strategy.
Introduction
Modern society routinely forces people to sit and work for long periods. The rate of seated work has increased significantly due to the increase in the computer-based tasks (Park et al., 2000; Workineh & Yamaura, 2016). As a result, people assimilated into modern technology suffer from pain and discomfort symptoms in the lower back, neck, and upper back (O’Sullivan et al., 2006; Williams et al., 1991; Womersley & May, 2006).
Many studies on sitting biomechanics have focused on the lower back and pelvis to understand the development process of lower back pain (LBP). They commonly examined the effects of the postural variables and chair design variables on various biomechanical responses of LBP and non-LBP participants (Curran et al., 2015). Those studies have commonly pointed out the negative impacts of prolonged sitting on the symptoms of LBP (Womersley & May, 2006), but no study has examined the effect of the lower body posture on trunk kinematics.
Some evidence on the system-level interaction has been presented in that the sitting posture naturally rotates the pelvis backward (i.e., hip flexion) and flattens the lower back (Claus et al., 2009; De Carvalho et al., 2010; Dunk et al., 2009; Park et al., 2013). In detail, the hip flexion causes pelvic extension (i.e., posterior tilt), and the lumbar and sacral vertebrae connected to the pelvis move together (i.e., more lumbosacral flexion) to lose the lumbar lordosis. A study measured the intervertebral joint angle of the lumbosacral spine quantitatively in the sitting, standing, and full flexion postures and showed that the pelvic extension while sitting upright drives the L5-S1 intervertebral joint to flex approximately 60% of its range of motion (Dunk et al., 2009). In addition to the kyphotic changes in the low back while sitting, the change in the intervertebral joint angle in the low back influences the adjacent vertebra motion directly through the surrounding passive tissues (e.g., lumbodorsal fascia, supraspinal ligament, capsular ligament, intervertebral disc, anterior and posterior longitudinal ligament) and the vertebral arch (e.g., spinous process and two transverse processes). Consequently, lumbar kyphosis could influence the thoracic and cervical spine posture. For example, recent studies reported that the sitting posture had more significant head flexion than the standing posture (Lee et al., 2015; Weston et al., 2017). Moreover, there was a strong correlation between increased thoracic kyphosis, forward head posture, and rounded shoulder (Park et al., 2014; Singla & Veqar, 2017). These biomechanical linkages could provide a path to reflect the lower extremity posture on the whole trunk posture, particularly on the lower back.
Previous studies investigated how the chair design changes the pelvic extension angle and hamstring length. Bendix and Biering-Sørensen (1983) tested the forward inclined seat angles (0°, 5°, 10°, and 15°; similar to the knee chair posture), and reported that lumbar flexion is closer to the neutral standing posture as the tilting angle of the seat-pan is increased. In other words, a larger seat-pan tilting angle may lead to a longer hamstring length (i.e., loosen hamstring), and the resulting less pelvic extension could give better lumbar lordosis (Bendix et al., 1988). Bridger et al. (1989) also compared five sitting postures and reported a more lordotic lumbar posture in the forward-sloping chair (or kneeling chair) and a more kyphotic lumbar posture in the semi-squatting posture. In particular, the pelvis extension increased with increasing tightening of the hamstring, leading to a kyphotic lumbar posture (Bendix, 1984; Claus et al., 2009; De Carvalho et al., 2010; Dunk et al., 2009; Keegan, 1953; Mandal, 1983; O’Sullivan et al., 2012; Vaucher et al., 2015). In summary, although these studies only investigated the seat design variables and focused on the lower back, they suggested a possible pathway between the lower extremity and trunk (e.g., lower back, upper back, and neck) while sitting.
Few previous studies have suggested the effects of the knee angle on the low back. To measure the lumbar and pelvic postures quantitatively, Bridger et al. (1992) tested nine sitting postures with an inclinometer and confirmed that the posterior trunk-thigh muscle (e.g., hamstring and iliopsoas) plays a significant role in changing the lumbar shape. They suggested that the knee flexion might also alter the pelvic extension angle and influence the lumbar curvature. Two possible mechanisms for the interaction between knee flexion and trunk postures could be hypothesized. First, a direct change in the tightness of the hamstring throughout the biomechanical linkage on the tibia (i.e., the insertion point of the muscle) could change the possible range of motion of the pelvis significantly while sitting. Second, the trunk posture may have an indirect influence throughout continuous efforts to maintain balance by moving the trunk and head posture, so the center of pressure (CoP) of the sitting posture could be modified depending on the transition of the foot location, accompanied by a change in the knee angle. Collectively, a system-level perspective considering the effects of the lower extremity posture on the whole trunk posture, not only the lumbar part, may provide a new viewpoint to understanding the sitting biomechanics at the whole-body level.
Significant anatomical linkages assist the interactions between the trunk and lower extremities. The trunk and lower extremities are connected directly or indirectly throughout various tissues, such as bones, muscles, ligaments, and fascia, to have remarkable biomechanical influence. First, the lumbardorsal fascia, extending from the iliac crest and sacrum to the thoracic cage and covering the paravertebral musculature, transmits the load from the lower extremity to the trunk during flexion and extension of the lower body and trunk (Snijders et al., 1993; Vleeming et al., 1995). Second, the hamstring, known as two-joint muscles, crosses from the knee joint to the hip (i.e., pelvis) and is recruited in hip extension and knee flexion. Consequently, these muscles influence the lumbosacral interaction and pelvifemoral interaction while sitting and standing (Sihvonen, 1997). Third, the psoas major, originating from the thoracic and lumbar vertebrae, passing through the pelvis, and inserting into the lesser trochanter, directly connects the lower extremity and trunk as a hip flexor and spine stabilizer (Bogduk et al., 1992). Overall, these connections have a significant biomechanical influence on each other. Therefore, a quantitative investigation of the role of these connections on the sitting biomechanics is worthwhile.
The above literature review supports the new viewpoint proposed in the current study that the proper head, upper back, and lower back postures can be guided by controlling the lower extremity posture, particularly the knee and hip joint angles. No studies have investigated how the lower body posture changes the pelvic, lumbar, thoracic, cervical, head, and shoulder postures directly and indirectly while sitting on a chair. In particular, a system-level perspective, considering the lower body and the upper body simultaneously, may provide a new viewpoint to understanding the biomechanical system recruited for the sitting postures. This study hypothesized that a smaller knee angle and a larger trunk-thigh angle might positively influence lumbar lordosis, cervical lordosis, head posture, and shoulder posture while sitting.
Methods
Participants
Seventeen male participants were recruited from the student population of Pusan National University (average age 26.8 [SD 4.25] years, height 175.6 [SD 5.0] cm, and weight 70.1 [SD 9.6] kg). The exclusion criteria were current or chronic troubles (e.g., pain or discomfort) in the lower back, upper back, or shoulder. All experimental procedures were approved by the institutional review board (IRB) at Pusan National University, which complied with the tenets of the Declaration of Helsinki. Written informed consent was obtained from each participant before data collection.
Apparatus
The kinematic measures were recorded using an OptiTrack motion capture system (Model Prime 13, NaturalPoint, OR, USA), collected at 120 Hz. Fourteen reflective markers were attached directly to the skin of the bony markers, including the right and left tragus (LTR, RTR), right and left acromion (LAC, RAC), C7, T6, T12, L3, L5, S2, right and left posterior superior iliac spine (LPSIS, RPSIS), and right and left head of the fibula (LF, RF). Each marker position was used to calculate the body angle, such as the lumbar flexion angle, pelvic tilting angle, head flexion angle, and rounded shoulder angle (For more detail, see “Data Processing => Kinematic data”).
The muscle activation level was captured using a bipolar surface electromyography (EMG) system (Model Bagnoli, Delsys, Boston, MA, USA) with a 1 cm spacing (fixed inter-sensor distance by Delsys), collected at 1200 Hz. Five EMG sensors were attached to the unilateral side (right) of the lumbar erector spinae (LES), thoracic erector spinae (TES), cervical erector spinae (CES), rectus abdominis (RA), and upper trapezius (UT), because the sitting postures tested in the current study were symmetrical.
A round chair without a backrest and arm supporters was used during the experimenter trials to embody all six postures with a chair and measure body kinematics and muscle activation simultaneously.
Experimental Design
Independent variables
This study included two independent variables: two trunk-thigh angles (TRUNK: 90°, and 135°) and three knee angles (KNEE: 45°, 90°, and 180°) to control the lower extremity posture. The two independent variables were fully crossed to develop the following sitting conditions: (1) T90K45 (TRUNK 90°, KNEE 45°); (2) T90K90 (TRUNK 90°, KNEE 90°); (3) T90K180 (TRUNK 90°, KNEE 180°); (4) T135K45 (TRUNK 135°, KNEE 45°); (5) T135K90 (TRUNK 135°, KNEE 90°); (6) T135K180 (TRUNK 135°, KNEE 180°; Figure 1). Each sitting posture was repeated five times, giving 30 trials tested randomly for each subject. The seat height was adjusted from the floor to the popliteal fossa minus 1 cm to provide the same conditions for each subject; this is an average of the proposals made in previous studies (Bendix, 1984; Keegan, 1953).

Six sitting postures developed by the combination of two trunk-thigh angles (TRUNK: 90°, and 135°) and three knee angles (KNEE: 45°, 90°, and 180°). Note. T90K45 = trunk-thigh angles 90° and knee angle 45°; T90K90 = trunk-thigh angles 90° and knee angle 90°; T90K180 = trunk-thigh angles 90° and knee angle 180°; T135K45 = trunk-thigh angles 135° and knee angle 45°; T135K90 = trunk-thigh angles 135° and knee angle 90°; T135K180 = trunk-thigh angles 135° and knee angle 180°.
Dependent variables
The dependent variables included four kinematic measures (lumbar flexion angle, pelvic tilting angle, head flexion angle, and rounded shoulder angle), five normalized EMGs (LES, TES, CES, RA, and UT), and co-contraction index (CCI; for more detail, see “Data Processing => CCI data”). The kinematic measures reflected the changes in the trunk postures according to the lower extremity posture: (1) average lumbar flexion angle, (2) average pelvic tilting angle, (3) average head flexion angle, and (4) average rounded shoulder angle. All kinematic measures were standardized based on the neutral standing posture captured before the experimental trials. The EMG measures were an average of the normalized EMG (NEMG) within each trial. The NEMG was standardized by the maximum voluntary contraction (MVC) of each muscle (i.e., used as a denominator in NEMG).
Tasks and Procedure
After obtaining written informed consent, the purpose and procedure of the current study were explained thoroughly by an experimenter, and the agreement of the participant was acquired. The participants then performed a pre-experimental session to become familiar with the six sitting postures. The experimenter showed the correct posture first. The participant was then asked to follow the posture, during which the correct posture was advised by the experimenter after measuring the posture using a goniometer. During the training session, the popliteal height was acquired and used to adjust the seat-pan height. EMG sensors were then attached to the appropriate locations of the selected muscles after shaving and swabbing the skin with alcohol cotton. The locations of the electrodes were as follows: (1) LES, 4 cm horizontally from the L4 spinous process; (2) TES, 4 cm horizontally from the T4 spinous process, (3) CES, 2 cm horizontally from the C4 spinous process; (4) RA, 5 cm above the umbilicus and 3 cm lateral to midline; (5) UT, 10 cm left from the vertebral midline at the C7 or T1 level. After attaching the electrodes, the MVC was measured before starting the experiment to normalize the EMG data. During the trials, a series of isometric contractions against the static resistance provided by two experimenters were performed with each muscle for 3 s (two replications). To capture the MVC of the LES, the participants laid on a fixed bench in the prone position. Their trunk was extended approximately 10° to push against the static resistance. To achieve the MVC of the trunk flexor, the participant laid in the supine posture. They then flexed their trunk approximately 20° to push against the static resistance on their shoulder. Similarly, the MVCs of the neck extensors were captured while pushing against the static resistance of the back of the head in the prone posture. Finally, the MVC of the UT was performed using the static resistance on the arm with the shoulder in a 70° abduction posture. These MVC data were used as a denominator of the NEMG.
After the MVC trials, fourteen reflective markers were attached to the skin of the bony markers, such as LTR, RTR, LAC, RAC, C7, T6, T12, L3, L5, S2, LPSIS, RPSIS, LF, and RF. The neutral standing posture was then captured while standing in a comfortable upright posture. The standing measurements were used as a baseline of the kinematic changes observed in the six sitting postures. In the subsequent experimental trials, six sitting postures were repeated five times, giving 30 trials conducted in random order. In all sitting postures, the participants sat on a round chair without a backrest and arm supporters for 5 s and were asked to gaze straight ahead and place their hands on the thigh. While capturing each posture, the correct posture was advised continuously by the experimenter. The seat heights were determined by the height of the popliteal fossa of each participant, minus 1 cm (Bendix, 1984). Between the experimental trials, the participants were required to stand up and sit again for the subsequent trial. After the final trial, the reflective markers and electrodes were removed, and the participants were free to leave.
Data Processing
The raw data, including the 3D position of the reflective markers and unprocessed EMG, were exported from the Motive Tracker software, transferred into MATLAB (MathWorks, version R2014B), and processed to calculate the dependent variables. Each kinematic and EMG measure was processed independently with the following details.
Kinematic data
All kinematic measures were simply the mean of each sitting posture for 5 s. First, the lumbar flexion angle was calculated by the included angle between the line formed by the markers on T12 and L3 and the line formed by the markers on L3 and L5 in the sagittal plane (Figure 2). Second, the head flexion angle was calculated from the forward tilting angle of a virtual plane, developed by C7, LTR, and RTR, taken from the global vertical plane in the sagittal plane. Third, the pelvic tilting angle was calculated from the forward tilting angle of a rigid body, developed by three markers on LPSIS, RPSIS, and S2. Finally, the rounded shoulder angle was calculated by the included angle between the line formed by the markers on LAC and C7 and the line formed by the markers on C7 and RAC in the horizontal plane. All kinematic dependent variables were standardized from the upright standing posture captured before the experimental trials to reveal the changes from the neutral standing trunk posture. In other words, the closer to zero degrees, the more neutral the standing posture was, which means lumbar lordosis, thoracic kyphosis, cervical lordosis, and neutral shoulder posture.
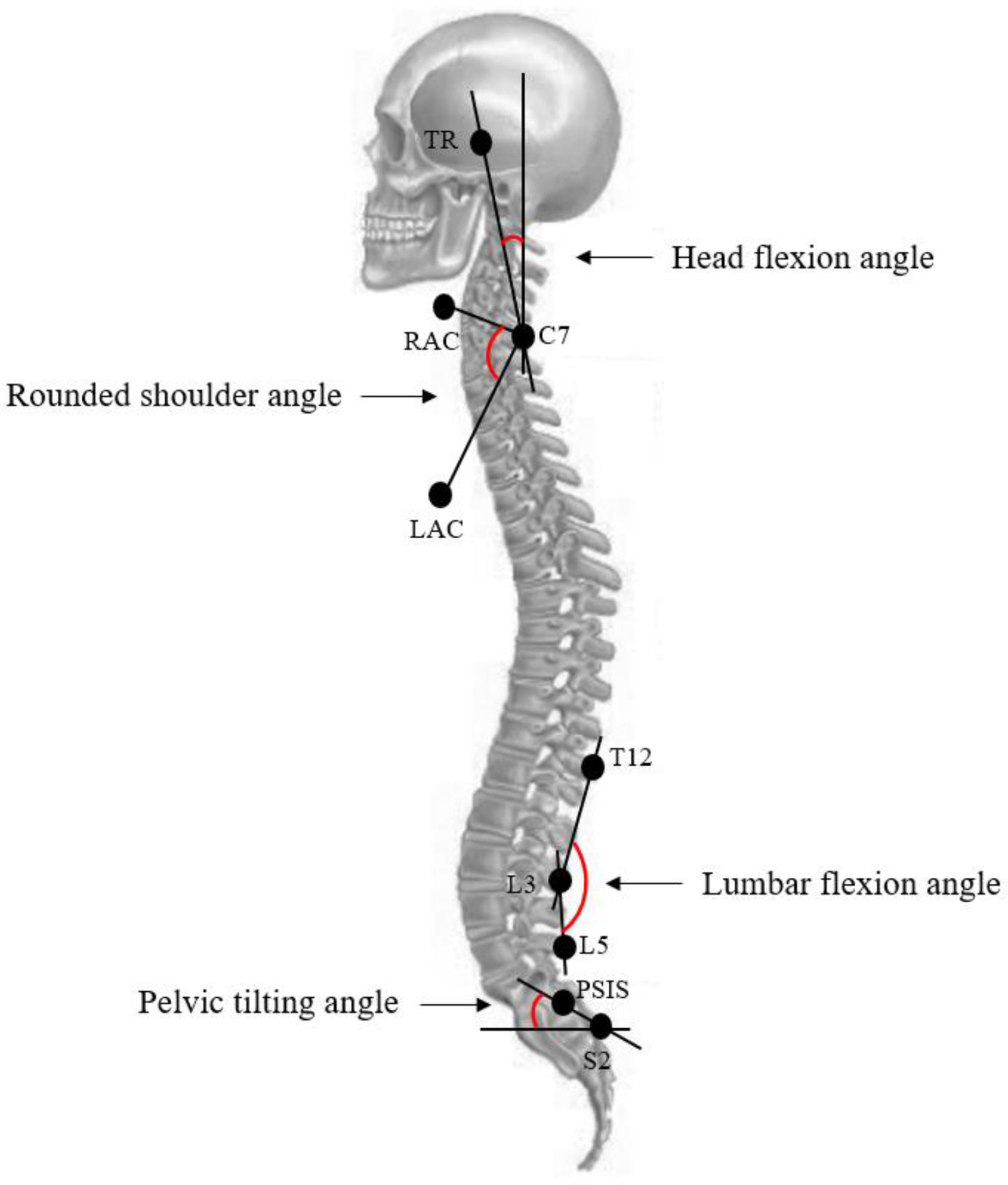
Definition of the head flexion angle, lumbar flexion angle, pelvic tilting angle, and rounded shoulder angle. Note. TR = tragus; LAC = left acromion; RAC = right acromion; PSIS = posterior superior iliac spine.
EMG data
The unprocessed EMG data were filtered (high-pass filter at 10 Hz, low-pass filter at 500 Hz, and a notch filter at 60 Hz) and full-wave rectified. For the MVC data, the filtered signals were averaged into 1/8 s moving windows to calculate the maximum value of each muscle. The peak value was used as a denominator to normalize the EMG data captured during the experimental trials. For the EMG data collected during the experimental trials, the filtered signals were averaged over each sitting posture for 5 s and used as a numerator to calculate the NEMG.
CCI data
The CCI was calculated using Eq. (1) to investigate the spinal stability (Lewek et al., 2004; Nelson-Wong & Callaghan, 2010). EMGlow and EMGhigh denote less or more activated muscles in the agonist and antagonist. The NEMGs of LES and RA in each experimental trial were used as CCI inputs (e.g., EMGlow: RA; EMGhigh: LES).

Statistical Analysis
The SAS and Minitab packages were used in all statistical analyses. Before performing the ANOVA procedure, the statistical model assumptions, including the homoscedasticity and normality, were tested. The dependent variables that violated the assumptions were transformed until they satisfied the assumptions (Montgomery, 2005). The log scale transformation or Johnson transformation was applied in this procedure. Two-way ANOVA with repeated measures was used for all dependent variables, and the post-hoc test using the Bonferroni method was employed where appropriate. Simple effect analysis was conducted where a significant interaction existed. A p value <.05 was considered significant.
Results
Trunk Kinematics
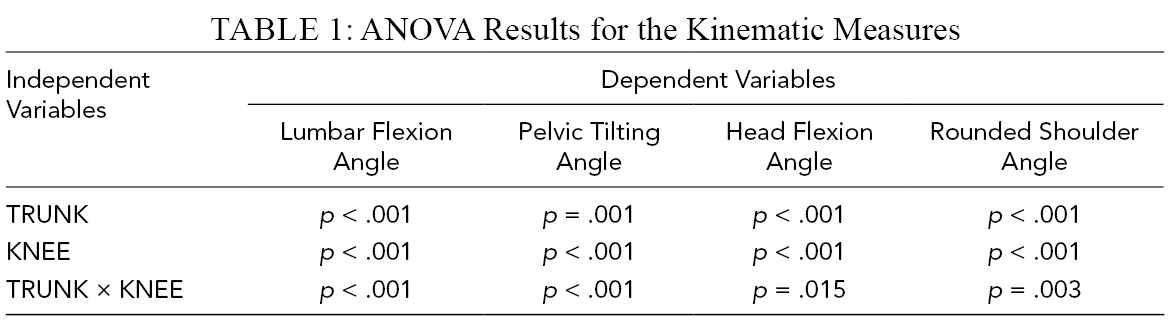
ANOVA revealed significant interaction effects between TRUNK and KNEE on all kinematic measures (Table 1). First, in the lumbar flexion angle, the T135K45 condition (i.e., largest TRUNK and smallest KNEE) has a significantly smaller change from the standing lumbar posture (12.6°) compared to the other conditions (Figure 3). In contrast, the increase in lumbar flexion (24.3°) of the T90K180 (i.e., smallest TRUNK and largest KNEE) was almost double that of the T135K45 condition (i.e., kyphotic lumbar curvature). Second, in the pelvic tilting angle, the standing posture changes were similar to those in the lumbar flexion angle (Figure 4). On the other hand, K45 and K90 showed similar changes from standing, but K180 showed significantly larger pelvic flexion, particularly in the T90 condition. Third, in the head flexion angle, the changes were similar to the lumbar flexion angle, as discussed above (Figure 5). In particular, the T135K45 condition had no difference with the upright standing posture in the head flexion angle (−.1°). As with the other kinematic measures, the T90K180 condition showed the largest change from the standing posture (6.2°). Fourth, in the rounded shoulder angle, the T135K45 condition was also similar to the standing posture (−3.8°), and the T90K180 condition showed a significantly larger rounded shoulder angle than the other postures (−6.0°; Figure 6). Overall, the smaller KNEE and larger TRUNK indicated a more neutral lower and upper back posture (i.e., closer to a neutral standing posture).
ANOVA Results for the Kinematic Measures
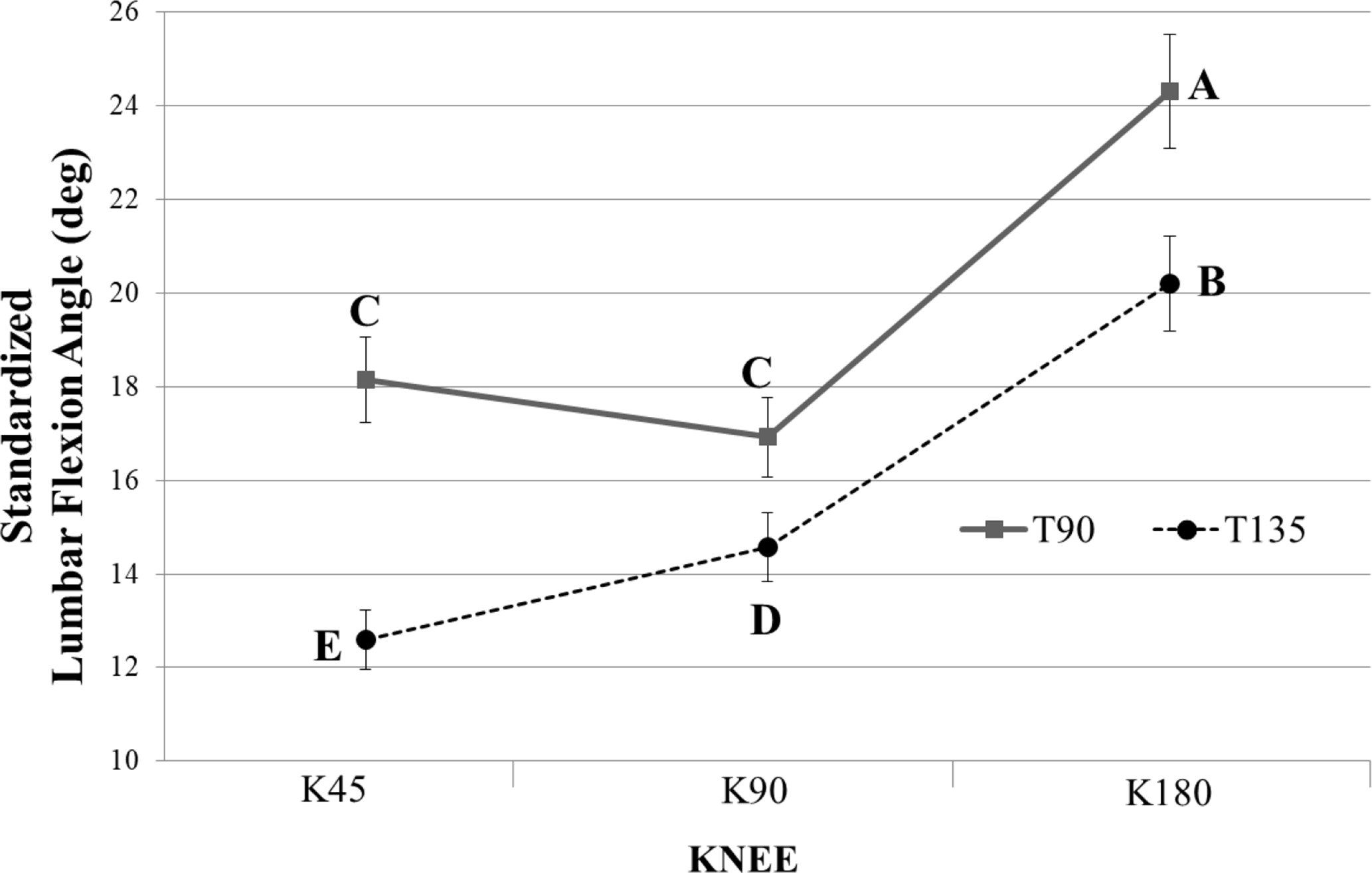
Lumbar flexion angle while sitting with the six lower extremity postures. Note. The values represent an average change from the standing posture. The letters “A,” “B,” “C,” “D,” and “E” represent the results of the post hoc tests. The average lumbar flexion angle with the same letter indicates that they are not significantly different. T90 = trunk-thigh angle 90°; T135 = trunk-thigh angle 135°; K45 = knee angle 45°; K90 = knee angle 90°; T135K180 = knee angle 180°. The error bars show standard error.
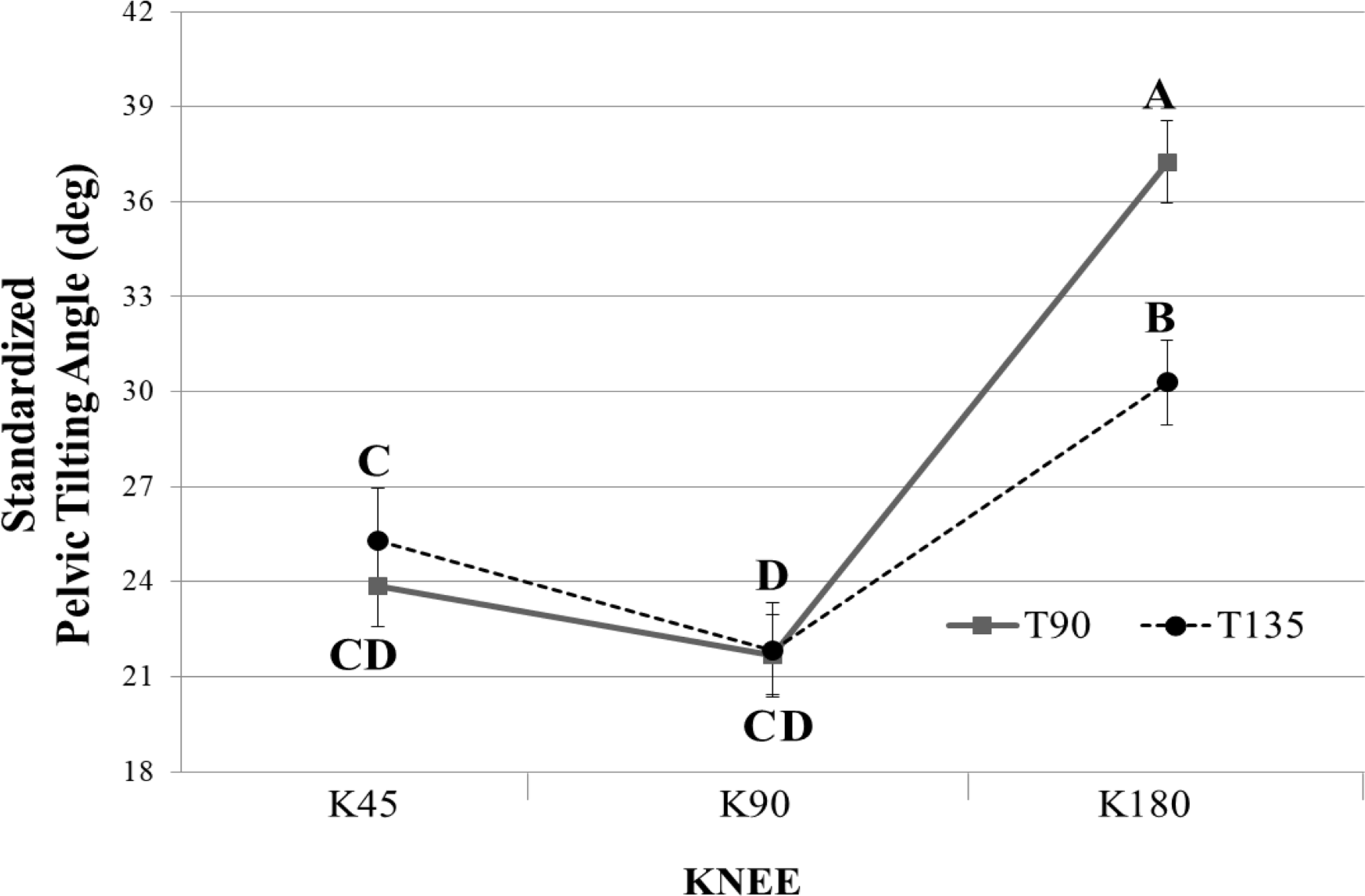
Pelvic tilting angle while sitting with the six lower extremity postures. Note. The values represent an average change from the standing posture. The letters “A,” “B,” “C,” and “D” represent the results of the post hoc tests. The average pelvic tilting angle with the same letter indicates that they are not significantly different. T90 = trunk-thigh angle 90°; T135 = trunk-thigh angle 135°; K45 = knee angle 45°; K90 = knee angle 90°; T135K180 = knee angle 180°. The error bars show the standard error.
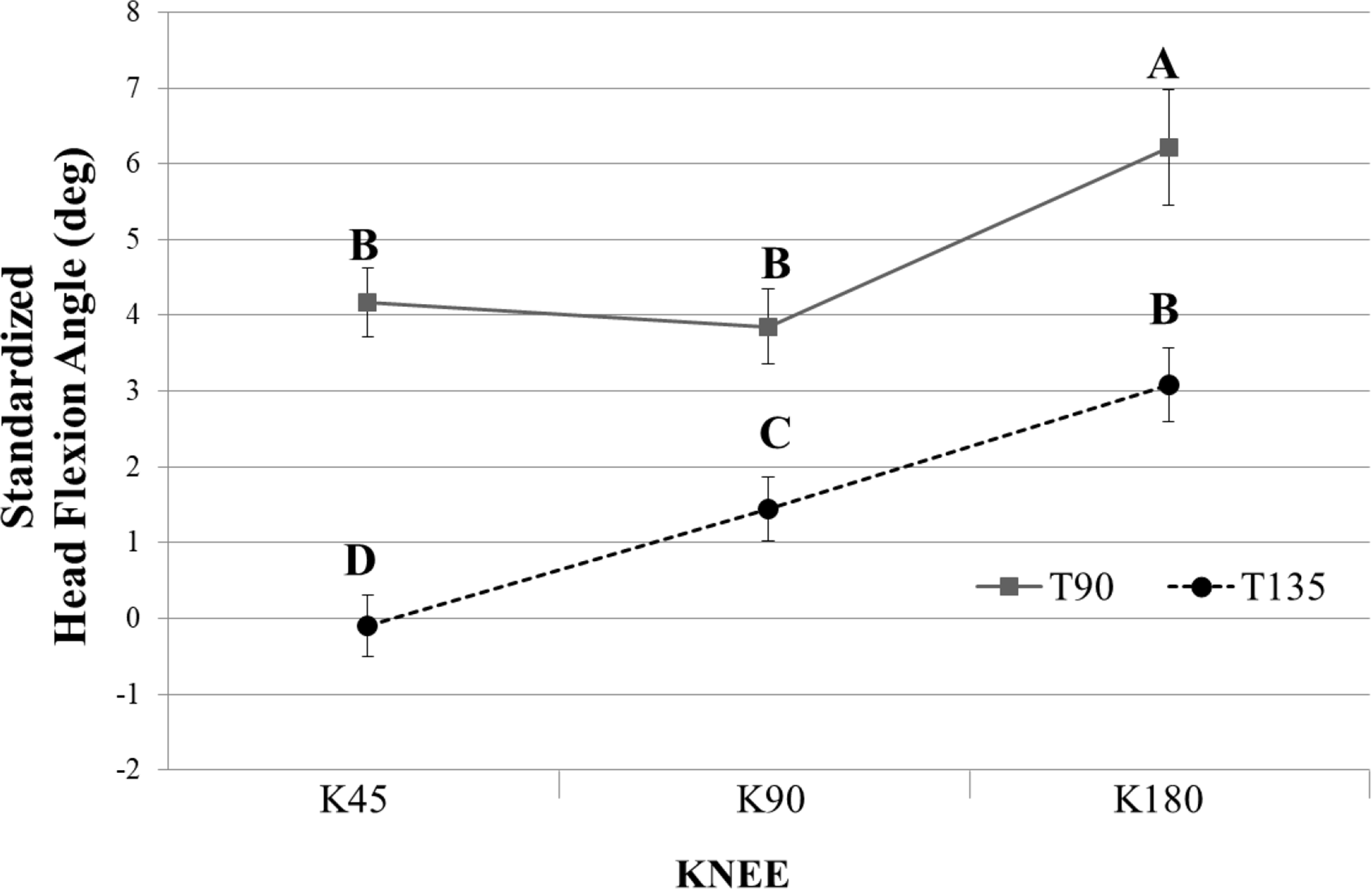
Head flexion angle while sitting with the six lower extremity postures. Note. The values represent an average change from the standing posture. The letters “A,” “B,” “C,” and “D” represent the results of the post hoc tests. The average head flexion angle with the same letter indicates that they are not significantly different. T90 = trunk-thigh angle 90°; T135 = trunk-thigh angle 135°; K45 = knee angle 45°; K90 = knee angle 90°; T135K180 = knee angle 180°. The error bars show the standard error.
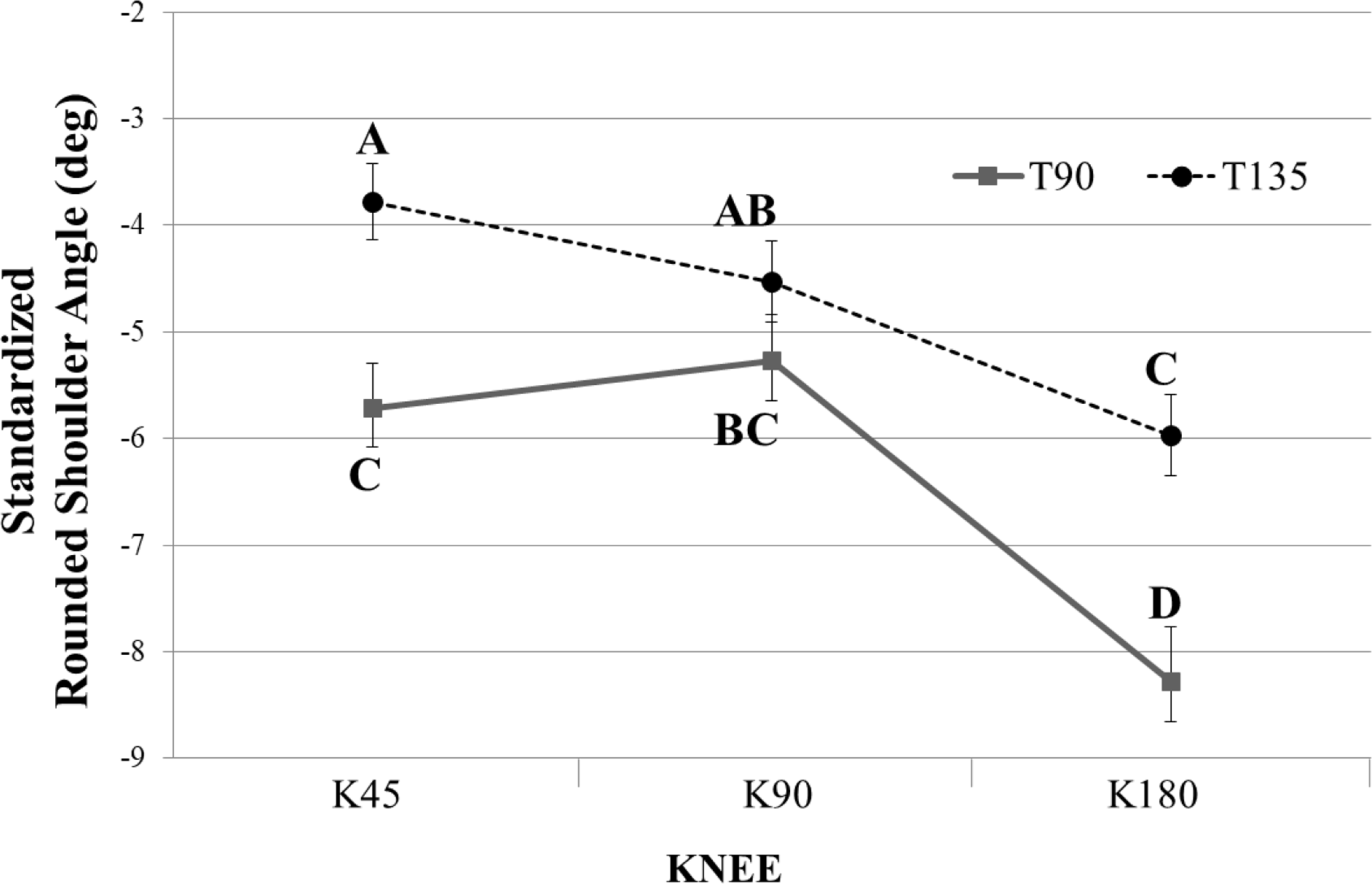
Rounded shoulder angle while sitting with the six lower extremity postures. Note. The values represent an average change from the standing posture. The letters “A,” “B,” “C,” and “D” represent the results of post hoc tests. The average rounded shoulder angle with the same letter indicates that they are not significantly different. T90 = trunk-thigh angle 90°; T135 = trunk-thigh angle 135°; K45 = knee angle 45°; K90 = knee angle 90°; T135K180 = knee angle 180°. The error bars show the standard error.
Muscle Activation Patterns
ANOVA of LES revealed significant effects of TRUNK and KNEE, but there was no interaction between them (p = .195; Table 2). The following post-hoc tests showed that T135 had significantly less LES activation than T90 and that K45 and K90 showed significantly more LES activation than K180 (Figure 7). In RA, ANOVA revealed a significant effect of an interaction between TRUNK and KNEE (Table 2). The following post-hoc tests showed significantly greater muscle activation in T135K45 and T90K180 than in the other conditions (Figure 8). On the other hand, ANOVA of the CCI showed that the T90K180 condition has a significantly larger CCI than the other sitting postures (Figure 9).

Effect of TRUNK and KNEE for lumbar erector spinae NEMG. Note. The error bars represent the standard error of the sample mean. NEMG values (%MVC) with the same letter indicate that they are not significantly different. EMG = electromyography; NEMG = normalized EMG; T90 = trunk-thigh angle 90°; T135 = trunk-thigh angle 135°; K45 = knee angle 45°; K90 = knee angle 90°; T135K180 = knee angle 180°. The error bars show the standard error.

Interaction plot between TRUNK and KNEE for the average NEMG of the rectus abdominis. Note. The error bars represent the standard error of the sample mean. NEMG values (%MVC) with the same letter indicate that they are not statistically significantly different. EMG = electromyography; NEMG = normalized EMG; T90 = trunk-thigh angle 90°; T135 = trunk-thigh angle 135°; K45 = knee angle 45°; K90 = knee angle 90°; T135K180 = knee angle 180°. The error bars show the standard error.
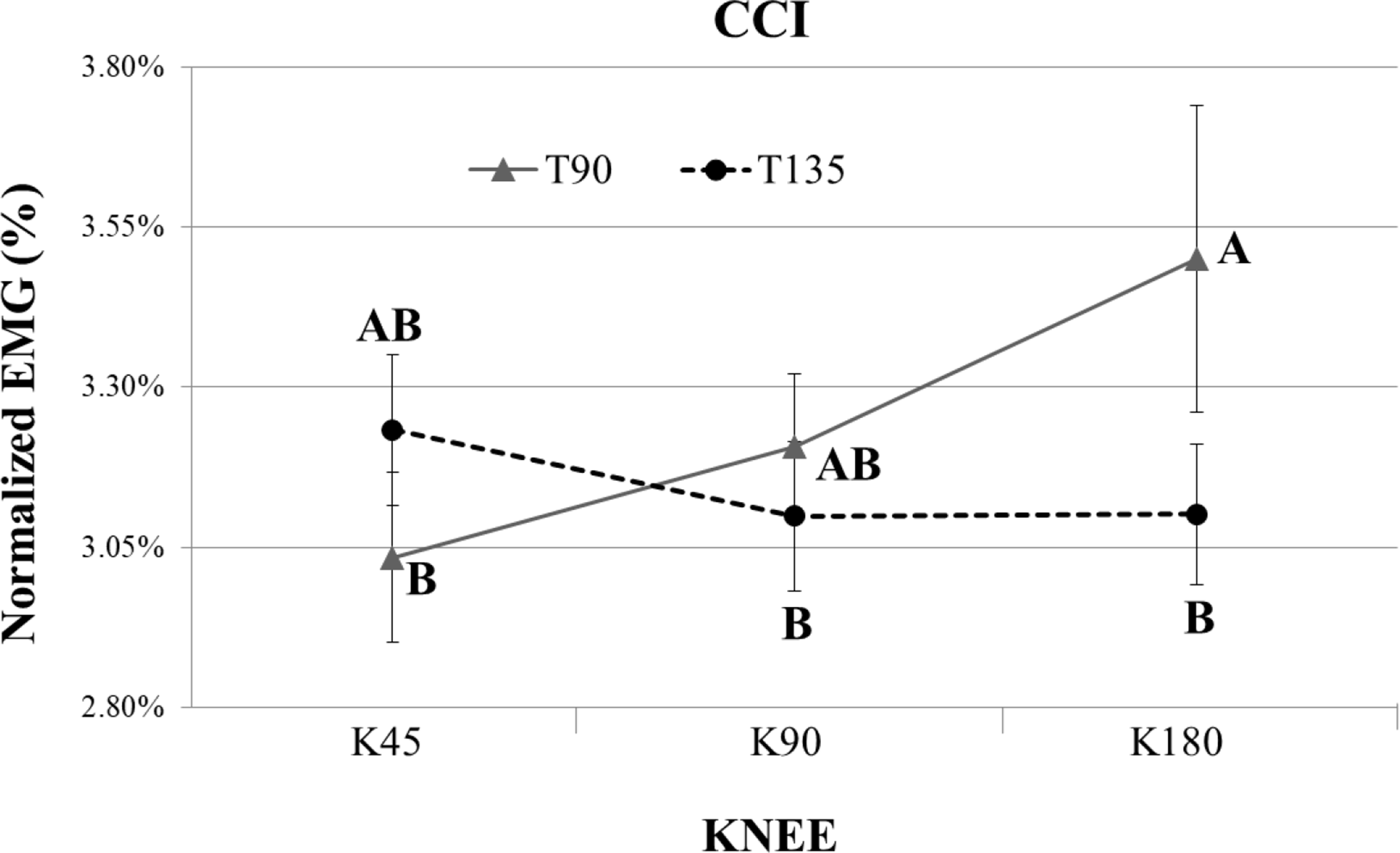
Interaction plot between TRUNK and KNEE for the average CCI. Note. The error bars represent the standard error of the sample mean. CCI values with the same letter indicate that they are not significantly different. EMG = electromyography; CCI = co-contractionindex; T90 = trunk-thigh angle 90°; T135 = trunk-thigh angle 135°; K45 = knee angle 45°; K90 = knee angle 90°; T135K180 = knee angle 180° (for more detail, see “Data Processing => CCI data”). The error bars show the standard error.
ANOVA Results for the EMG Measures
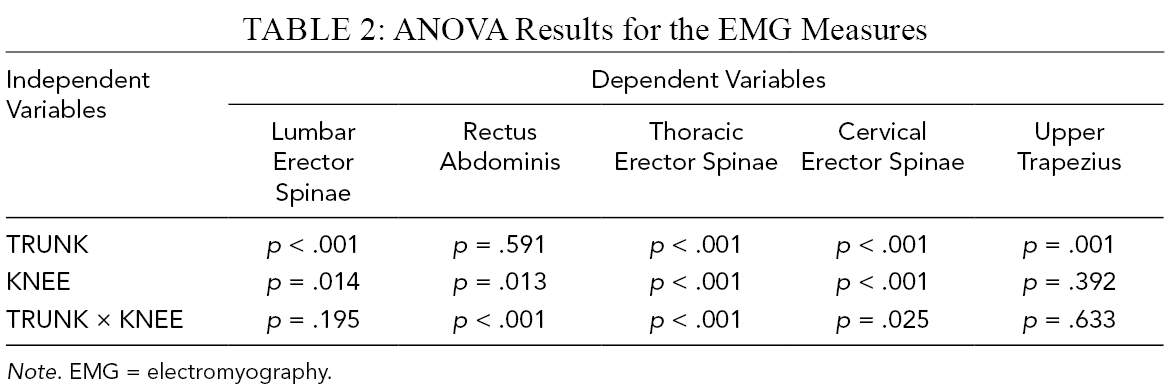
Note. EMG = electromyography.
ANOVA on TES revealed a significant interaction, and the following tests showed that the T90K45 and T90K90 conditions required significantly more TES activation compared to the other conditions (Figure 10). In CES activation, ANOVA revealed the significant effect of an interaction between TRUNK and KNEE (Table 2). The T135K45 condition showed a smaller activation level among the six sitting postures, and the T90K180 condition showed a larger activation level, following the result of the head flexion angle (Figure 11). Finally, in the UT activation, ANOVA showed that only TRUNK exerted a significant effect (Table 2). The post-hoc test showed that T135 had significantly lower UT activation than T90 (T135 = 1.1%, T90 = 1.4%).

Interaction plot between TRUNK and KNEE for the average NEMG of the thoracic erector spinae. Note. The error bars represent the standard error of the sample mean. NEMG values (%MVC) with the same letter indicate that they are not significantly different. EMG = electromyography; NEMG = normalized EMG; T90 = trunk-thigh angle 90°; T135 = trunk-thigh angle 135°; K45 = knee angle 45°; K90 = knee angle 90°; T135K180 = knee angle 180°. The error bars show the standard error.
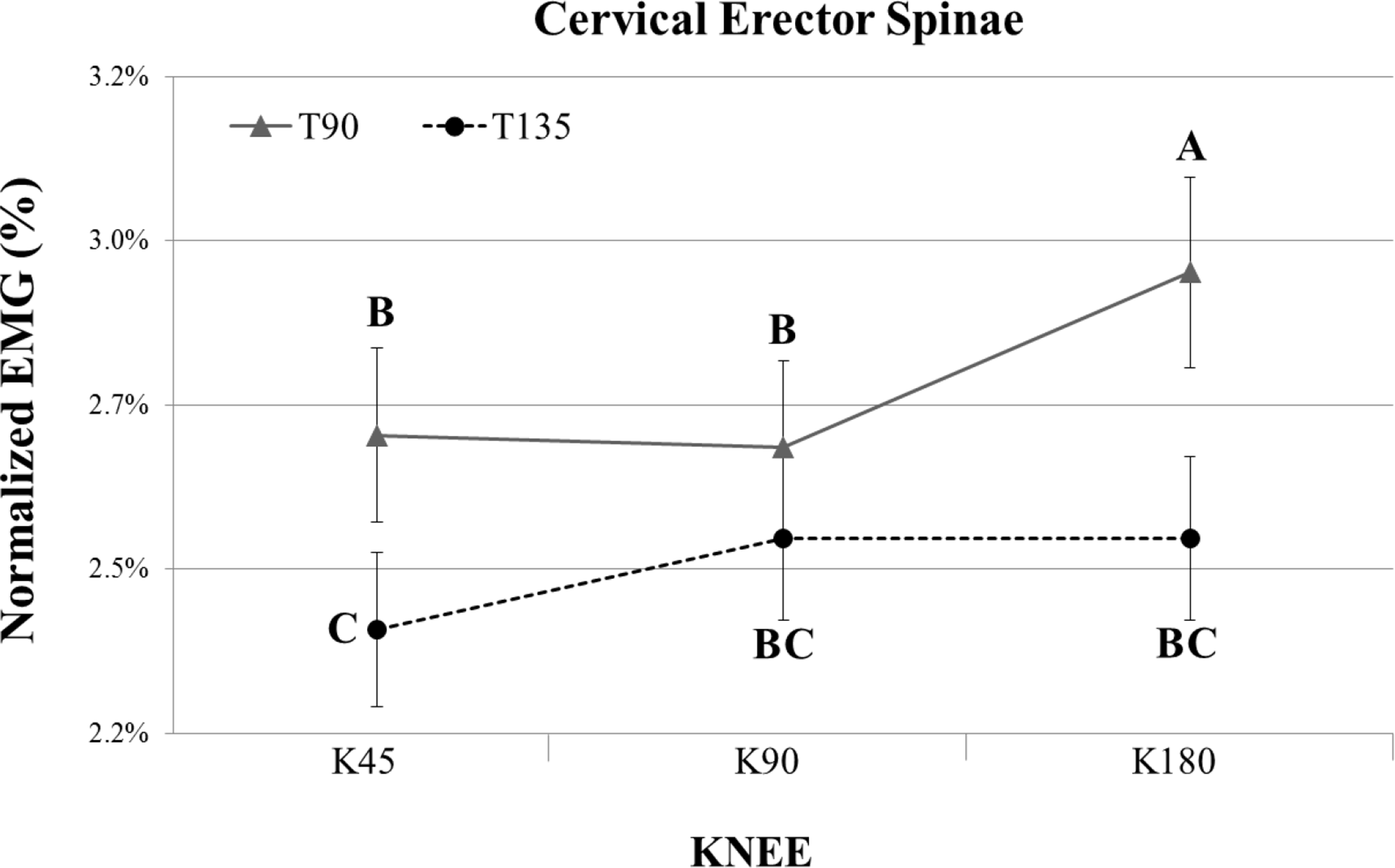
Interaction plot between TRUNK and KNEE for the average NEMG of the cervical erector spinae. Note. The error bars represent the standard error of the sample mean. NEMG values (%MVC) with the same letter indicate that they are not significantly different. EMG = electromyography; NEMG = normalized EMG; T90 = trunk-thigh angle 90°; T135 = trunk-thigh angle 135°; K45 = knee angle 45°; K90 = knee angle 90°; T135K180 = knee angle 180°. The error bars show the standard error.
Discussion
The current in-vivo study examined the change in the trunk and head postures and muscle recruitment patterns while sitting with various lower extremity postures. The results showed that changing the trunk-thigh and knee angle affected the trunk and head postures significantly, which suggested a significant system-level interaction while sitting. In particular, a larger trunk-thigh angle and a smaller knee angle (i.e., T135K45) could provide a more neutral posture while sitting and reduce back muscle activation.
From a collective perspective, the kinematic analysis in this study confirmed a significant biomechanical interaction between the upper body and lower body throughout the direct and indirect actions on the pelvis while sitting with various lower extremity postures. These results showed that a change in the trunk-thigh angle (i.e., hip angle) and the knee angle significantly influence all trunk postures, including pelvic extension (i.e., pelvic tilting angle), lumbar lordosis (i.e., lumbar flexion angle), cervical lordosis (i.e., head flexion angle), and rounded shoulder angle. An increase in trunk-thigh angle may lead the hamstring to loosen, resulting in less pelvic extension and more neutral lumbar lordosis (Bendix & Biering-Sørensen, 1983; Bridger et al., 1989). Previous studies showed that the intervertebral joint angles in the lower back range from 4.9 to 8.0°, 6.7 to 10.2° and 4.6 to 7.0° for the L3/4, L4/5, and L5/S1, respectively (Andersson et al., 1979; Lin et al., 2006; Makhsous et al., 2003). Hence, the lumbar flexion angle (approximately 12° change) observed in the current study could be interpreted as a noticeable change. Moreover, the current study also showed that a larger trunk-thigh angle consistently improves the upper back posture, including a smaller head flexion angle (but relatively minor) and less rounded shoulder angle. This could be related to the more neutral lumbar lordosis that may lead to thoracic kyphosis and cervical lordosis. Because the change in the intervertebral joint angle influences the adjacent vertebra motion directly through the surrounding passive tissues (e.g., supraspinal ligament, capsular ligament, intervertebral disc, and anterior and posterior longitudinal ligament) and the vertebral arch (e.g., spinous process and two transverse processes), the neutral lower back posture observed in the larger trunk-thigh angle may induce a more neutral upper back posture.
The biomechanical interaction was also affected significantly by the change in knee angle. The results showed that a smaller knee angle consistently provides more neutral trunk postures, as confirmed by all four dependent measures. As discussed in the literature review, the hamstring length can be controlled by the knee angle, in that the hamstring comprises two-joint muscles inserted into the tibia. Regarding the observations in the current study, the straightened knee (K180 condition) could experience tight hamstring and pelvic extension, and the lumbosacral interaction acting directly on the lumbar vertebrae may lead to lumbar kyphosis (De Carvalho et al., 2010; O’Sullivan et al., 2012). The upper body posture, including the rounded shoulder angle and head flexion angle, also confirmed the significant role of the knee posture while sitting. This may be an unexpected observation because those two body segments are too far apart to have a direct influence. On the other hand, serial impact between adjacent body structures could have a significant consequence on the upper back throughout the biomechanical linkages: (1) knee extension, (2) tight hamstring, (3) pelvic extension, (4) lumbar kyphosis, (5) hyper thoracic kyphosis, (6) cervical kyphosis, (7) rounded shoulder, and (8) head flexion. In addition, a significant posterior transition of the CoP can indirectly change the head position and upper back posture as a counter-balancing mechanism, which is usually observed in whole-body balancing (Gupta, 2001). In the T135K45 posture in Figure 1, the participants have been trying to keep their overall balance by locating the head posteriorly and opening the shoulders. In other words, the trunk posture may have an indirect influence throughout the continuous efforts to maintain balance by moving the trunk and head posture, so the CoP of the sitting posture could be modified depending on the foot location, accompanied by a change in the knee angle. Overall, the kinematic observation showed that the lower body posture changes the pelvic, lumbar, cervical, head, and shoulder postures directly and indirectly while sitting on a chair. This in line with the hypothesis that a larger trunk-thigh angle and smaller knee angle, the more neutral the lower and upper back posture are.
Although the kinematic measures suggested more neutral trunk postures with a larger trunk-thigh angle and a smaller knee angle, no conclusion can yet be made on the best posture. Therefore, the muscle recruitment pattern was analyzed to investigate the lower extremity sitting postures. In general, the NEMG also supported a significant interaction between the trunk and lower extremity, even if the changes were minor. The kinematic measures indicated that a larger trunk-thigh angle and a smaller knee angle (e.g., T135K45) are better for achieving a more neutral posture. Overall, the T135K45 posture confirmed the smaller muscular recruitments in the lumbar erector spinae, thoracic erector spinae, and cervical erector spinae, except for significant trunk muscle co-contractions. Previous studies suggested the role of excessive antagonistic co-activation to maintain a stable posture (Cholewicki et al., 1998; Gardner-Morse & Stokes, 1998; Granata & Marras, 2000; Granata & Orishimo, 2001). The significant co-contraction may be due to the lower activation levels in the muscles around the spinal column (i.e., local muscle system suggested by Bergmark, 1989) and the reactional recovery to hold the trunk system by the co-contraction mechanism of the global muscle system (e.g., abdominal muscles). In summary, a larger trunk-thigh angle and a smaller knee angle could provide a more neutral trunk posture while sitting and reduce the back muscle activation levels at the cost of an antagonistic co-contraction.
In addition, a discrepancy was observed between postural measures and muscular activation in the lower back muscle activity while changing the knee angle. The smaller knee angle revealed a more neutral trunk posture in the kinematics, but the lower back muscle activation was more significant in the smaller knee angle. The results were in line with a previous study showing that the lower back muscle activity was also smaller in the slumped posture (e.g., K180 in the current study, see Figure 1) than in thoracic upright sitting (e.g., T135K45; O’Sullivan et al., 2006). This may have been caused by the use of passive moment generated by the intra-abdominal pressure (IAP) and the passive tissues in the lower back while sitting with a slouched posture under the K180 condition (Figure 1; Cresswell et al., 1994; Marras & Mirka, 1996). Cholewicki et al. (1999) reported that the co-activation level in the antagonist could control the IAP. The current study also supported the observation by showing a significant increase in the rectus abdominis while sitting in the slouched posture (e.g., T90K180 condition). Interestingly, both the best posture (T135K45) and the worst posture (T90K180) showed significant recruitment of the rectus abdominis for different reasons. Collectively, the slouched posture with a larger knee angle may not be advocated, even with the smaller muscle activation in the lower back.
The muscle recruitment level in the current study design was modest because of the sedentary sitting nature. On the other hand, the NEMG suggested an interesting co-activation strategy according to the change in sitting biomechanics and generally supported the kinematic measures. The more neutral posture observed with a larger trunk-thigh angle and smaller knee angle was required to have an antagonistic co-contraction, even with the lower activation levels in the spinal musculatures. Nevertheless, although the co-contraction increased the spinal compression load, the negative impact of the antagonistic co-activation observed in the current study could be minimal (Hughes et al., 1995; Marras & Granata, 1997). First, the amplitude of the antagonistic co-activation level was 2.5%–2.9% in NEMG because of the nature of the sedentary sitting (Mörl & Bradl, 2013). Second, co-contraction is a cost-beneficial strategy in that a 34%–64% increase in trunk stability can be achieved by only a 12%–18% increase in compression force (Granata & Marras, 2000). In this manner, the antagonistic co-contraction while sitting with a larger trunk-thigh angle and a smaller knee angle could be advocated.
In the lumbar biomechanical model developed by Bergmark (1989), only the active component of the trunk system was included as a spine stabilizer and moment generator. The conceptual model classified the active system into a local system (i.e., all muscles have their origin and insertion at the vertebrae) controlling the spinal curvature and a global system (i.e., trunk muscles connect the thoracic cage and pelvis) generating the required moment to hold the trunk. Based on Bergmark’s work, two recent studies took the conventional model one step further by focusing on the system-level perspective (Jin & Mirka, 2015a, 2015b). The previous studies gathered data to reveal an interaction between the lower body and trunk during trunk flexion-extension and revealed the role of “a superglobal system,” including the active and passive tissues that directly or indirectly influence the trunk biomechanics through their actions on the pelvic girdle. The current empirical work focused on collecting data while sitting with various lower extremity postures. The results revealed a significant interaction between the super-global system in the lower body and the upper body.
In addition, the current study revealed a significant interaction from the knee to the head while sitting and has provided important insights into more neutral sitting postures. These results could be used to design a chair controlling the lower extremity postures and develop a sitting strategy comprised of a periodic posture change for equalizing the load between body parts. This study had several limitations that limit the generalizability of the results. First, the effects of sitting postures on EMG and some kinematic variables were relatively modest because of the characteristics of the tested trials (i.e., quiet sitting), even though the previous studies and the kinematic results of the current study are in line (O’Sullivan et al., 2012; Wong et al., 2019). Therefore, the changes could be biologically insignificant in the viewpoint of the spinal loading. Further study, including prolonged sitting, may provide a better understanding of this issue. Second, only healthy and fit males participated in the current experiment. The results might have been biased because males and females differ in their pelvic anatomy (females have a broader and denser pelvis than males). Dunk and Callaghan (2005) showed that men sat with a more posterior rotated pelvis than women, which causes more lumbar flexion while sitting. A future study should consider both genders and age groups representing the broader public. Finally, the chair used in the current study had no backrest or armrest. Therefore, care should be taken while translating the results in a more common situation using a chair with a backrest. Further study will be needed to test a combination of various sitting strategies, including backrest, armrest, and knee support.
Conclusion
This study evaluated the effects of the lower extremity posture on the angle of the pelvis-lumbar-thoracic-head. A smaller trunk-thigh angle and a larger knee angle resulted in more lumbar lordosis lost, greater head flexion, and more rounded shoulders. The results confirmed that a change in trunk-thigh angle and knee angle had a significant effect on the upper extremity posture.
Key Points
Data were collected while sitting with various lower extremity postures to demonstrate a significant interaction between the lower body and the upper body
Kinematic observations showed that the lower body posture directly and indirectly changes the pelvic, lumbar, cervical, head, and shoulder postures.
A larger trunk-thigh angle and a smaller knee angle could provide a more neutral lower and upper back posture while sitting and reduce the back muscle activation.
A significant interaction from the knee to the head while sitting was demonstrated, and important insights into controlling the trunk and head postures throughout the lower extremity posture were provided.
Footnotes
Acknowledgments
This research was supported by the Basic Science Research Program through the National Research Foundation (NRF) of Korea, funded by the Ministry of Education (NRF-2020R1I1A306953611). This research was also supported by the MSIT (Ministry of Science and ICT), Korea, under the Grand Information Technology Research Center support program (IITP-2020-0-01791), supervised by the IITP (Institute for Information & communications Technology Planning & Evaluation).
Author Biographies
Seulgi Kim holds a BSc degree in industrial engineering from Dongseo University and is currently a PhD candidate in industrial engineering at Pusan National University.
Ilseok Lee holds a BSc degree in industrial engineering from Pusan National University and is currently an MSc candidate in industrial engineering at Pusan National University.
Sang Hyeon Kang holds a BSc degree in industrial engineering from Pusan National University and is currently an MSc candidate in industrial engineering at Pusan National University.
Sangeun Jin is a director of the Human & Safety Engineering laboratory and an associate professor of industrial engineering at Pusan National University, South Korea. He received his PhD in industrial and manufacturing systems engineering in 2011 from Iowa State University, Ames, USA.