
Abstract
In today’s unstable and uncertain economy, middle-class and professional workers are expected to participate in employability activities, such as ongoing higher education and obtaining additional credentials. These activities are expected by employers, protect workers against layoff, and help to advance workers’ careers. In this article, we argue that the expectations of employability are increasingly being placed on lower-level workers by their employers, in partnership with educational institutions. We draw on 20 case studies of career development programs in a variety of health care settings across the United States. We found that through the development (and requirement) of credentials and partnerships with educational institutions, employers encouraged low-level employees to be continually considering their employability and career pathways. However, while the career development programs in our sample use many of the same employability practices seen among middle-class and professional workers, there were often minimal financial or educational rewards for low-level workers. Career programs that focused on established credentials (e.g. surgical technicians, registered nurses), though, were able to provide substantial upward social mobility for workers.
The expectation of employability, or the need for the individual to develop one’s personal and professional capacity to maximize one’s employment potential, is pervasive in today’s uncertain and unstable economy (Clarke and Patrickson, 2008; Cremin 2010; Kanter, 1995; Kossek, 2000). Research on employability largely focuses on the behaviour of middle-class and professional workers (Baldry et al., 2007; Barley and Kunda, 2004; Di Tomaso, 2001; Smith, 2010), as they pursue human, cultural and social capital that will help them to secure employment and promotions in today’s ever-shifting labor market (Dwyer, 2013; Holzer and Lerman, 2009; Kalleberg, 2011; Mishel et al., 2012; Osterman, 2000). However, in this article we argue that the expectations of employability, which we conceptualize as the pursuit of credentials and participation in higher education, are increasingly being placed on lower-level workers, often from their own employers (Dill et al., 2012; Smith, 2010).
In this article, we examine how employer organizations use the expectation of employability to encourage low-level workers to improve their performance and productivity, drawing on case studies of career development programs in the US health care sector. Through the development (and requirement) of credentials and partnerships with external educational institutions, employer organizations encourage employees to be continually considering their employability and career pathways. However, while the career development programs in our sample use many of the same employability practices seen among middle-class and professional workers, the rewards to workers for participating in such activities often do not match those received by their better-educated peers. While some career programs can provide substantial upward social mobility for workers, there are often minimal financial rewards for low-level workers who choose to participate in career development programs that enhance their employability.
This study aims to make two contributions to the literature on employability and low-level workers. First, we analyze specific ways in which employers of low-level health care workers encourage workers to participate in employability activities, including gaining credentials and participating in higher education, while accommodating the resource-limitations of low-level workers. Most studies of employability have focused on middle-class and professional workers (Smith, 2010); this study aims to understand employer expectations of employability in the context of entry level work. Second, we examine how different types of career development programs and employability practices contribute to the social mobility and employment opportunity of workers. While past research has explored the limitations of career development programs for entry level workers (Ducey, 2009), this study expands on previous studies by examining how different types of career development programs constrain—and sometimes support—employability and upward career mobility for workers.
The context: Career development for us entry level health care workers
In this study, we focus on career development programs for low skill workers in US health care settings, which we refer to as entry level health care workers. Entry level health care workers are those that provide a high degree of hands-on care or care support in health care settings, have a low threshold to entry (typically less than a college degree), and make relatively low wages (generally under $40,000 per year) (Schindel et al., 2006). Entry level health care workers range from care support (e.g. housekeepers and dietary staff) and direct care workers (e.g. nursing assistants, patient care technicians), to administrative workers (e.g. medical records technicians, unit clerks) and entry level allied health workers (e.g. respiratory therapists, medical technicians). Many of these entry level occupations are among the fastest growing jobs in the United States (US Department of Labor, Bureau of Labor Statistics 2016) and the UK (Bach et al., 2012).
There are more career development programs for low-skill workers in the United States in health care than in any other industry (Fitzgerald, 2006), and there are a number of reasons for this enthusiasm. First, health care organizations face competition to recruit and retain the best workers, and established patterns of upward mobility within an organization may be a draw to potential workers (Lepak and Snell, 2002; McBride, 2011; MacLean et al., 2014; May et al., 2006; Rother and Lavizzo-Mourey, 2009). Second, increased pressure to demonstrate high quality of care at all levels of the organization has contributed to efforts of workforce development for entry level health care workers (Ducey, 2009; Fitzgerald, 2006; Folbre, 2006; Morgan and Farrar 2015; Pindus et al., 1995). Finally, some health care organizations may be motivated to train entry level health care workers to work at the ‘top of their licensure’ to reduce costs (Dower et al., 2013; Grumbach and Bodenheimer, 2004). There is some overlap in the skills that workers in different occupations are allowed to perform as determined by professional regulating bodies (often referred to as an occupation’s ‘scope of practice’). Consequently, health care organizations are motivated to train low- or mid-level workers to perform skills within their scope of practice that might otherwise be performed by a more qualified, more expensive worker (Shipman and Sinsky, 2013), a practice that is common in health care systems outside of the US as well (Bach et al., 2012; Currie et al., 2009).
Conceptualizing employability for low-level workers
The term ‘employability’ has a range of meanings, most simply having the skills and willingness to be employed (Gazier 2001; McQuaid and Lindsay, 2005). Since the 1980s, the term employability has largely referred to the understanding articulated by Kanter (1995), where individuals actively accumulate human, cultural, and social capital to maintain and find employment in today’s unstable economy (Beck, 2000; Kanter, 1995; Lippman, 2008; Smith, 2010), or what Gazier (2001) would term ‘initiative employability’ (Chertkovskaya et al., 2013). These employability activities include undergoing training and acquiring skills and credentials (Adams and Demaiter, 2008; Kalleberg, 2011), identity work (Chapple, 2006; Sharone, 2007; Ybema et al., 2009), and networking and unpaid labor, such as volunteering or internships (Edgerton and Mullan, 2008; Taylor, 2004).
Organizations now expect workers—especially middle-class and professional workers—to participate in employability activities. Indeed, Chertkovskaya et al. (2013) point out that not only is employability now viewed as being key for one’s own well-being in the labor market, it is also now the very condition for employment. That is, if one does not pursue employability activities, one may not be employable (Andersen, 2007; Heelas, 2002). Of course, employers benefit from employees who are ever seeking opportunities to refine and sharpen their skills, as do educational institutions (Arthur and Rousseau, 2001; Brown et al., 2003).
Smith (2010), in her review of employability, argues that the expectations of being an ambitious, self-starting and continuously-learning employee have spread to low-skill, working class employees and their employers. As an example, we can look at Ariel Ducey’s (2009) critique of many workforce development efforts in health care organizations. Ducey demonstrates that entry level workers recognize that they need additional education to gain employability—which is typically communicated to them by their employers—but do not necessarily have the skills or knowledge to navigate a complex educational system. Workers then end up accumulating many low-level credentials, but these credentials do not move them any closer to a credential that could provide significant upward mobility. Thus, Ducey argues that many workforce development or career programs provide ‘false promises’ of upward social mobility. Indeed, Chertkovskaya et al. (2013) argue that positive language around employability overlooks differential ability to reap the benefits of employability activities.
Organizations arguably provide some support for low-skill workers to participate in employability activities, largely because low-skill workers frequently lack the resources, skills and cultural capital to pursue these activities on their own (Cooper, 2008; Kossek, 2000). For example, low-skill workers may lack resources (e.g. tuition, transportation, childcare) and time to pursue additional education or training, as many need to work full-time to support a family or hold multiple jobs (Clawson and Gerstel, 2014; Kazis and Miller, 2001). However, workers are still responsible for part of their employability activities, whether it is time outside of work to attend classes, or the cost of forgone wages to complete a clinical rotation. For this reason, employability practices are often referred to as the ‘externalizing’ of careers because workers are largely responsible for these activities (Cappelli, 1999; Clarke and Patrickson, 2008; Jacoby, 2001; Osterman, 2000; Smith, 2010). Vallas and Prener (2012: 343) use the term ‘responsibilization,’ where workers are expected to ‘assume the obligation of perfecting themselves, and of bringing out the full value of their human capital’.
In this article, we focus on two specific dimensions of employability: credentials and participation in higher education. The expansion of human and social capital through training and credentialing are central activities in improving one’s employability (Smith, 2010). In the US health care sector, the context of this study, credentials have historically been required of mid-level and professional health care workers (e.g. registered nurses and physicians) (Abbott, 1988; Friedson, 2001), but credentials are increasingly required of low-level and paraprofessional employees in health care organizations (Kleiner and Krueger, 2010; Nancarrow and Borthwick, 2005). Unfortunately, most credentials within the health care industry do not build on each other in terms of advancing one’s career (e.g. earning a certificate to become a certified nursing assistant does not contribute credit towards earning a nursing degree) (Ducey, 2009; Glazer, 1991).
To encourage employees to become credentialed, employers frequently partner with external educational institutions (Manley et al., 2009; Pindus et al., 1995), which have embraced—if not expanded—the values of employability (Boden and Nedeva, 2010; Tomlinson, 2012). Indeed, pursuing employability typically means being involved in higher education, which benefits from this cradle-to-grave approach to self-development (Perlin, 2012). Involving an external training institution increases the legitimacy of a training program (Dill et al., 2014) and may be more likely to make employees feel that they are engaged in employability activities, as compared with routine internal training within the organization (Morley, 2001; Tomlinson, 2012). However, such involvement with external educational institutions may, in some cases, also give workers a false sense of career advancement with few meaningful rewards, particularly if career structures are not in place within employment settings to reward workers for skill acquisition (Ducey, 2009).
The most basic reward of employability is the maintenance of employment. In today’s turbulent and unpredictable economy, gaining additional training and credentials helps employees to update their skills and protect against job loss (Smith, 2010). Employability can also be a pathway to upward social mobility. In this article, we conceptualize upward social mobility as an increase in wages and other forms of compensations (e.g. stipends), as well as career opportunity or potential (Andersson et al., 2005; Gautie and Schmitt, 2010). Most entry level health care jobs can be described as ‘bad jobs,’ meaning they have low wages and limited opportunities for advancement (Kalleberg, 2011; Ribas et al., 2012). A reward of employability may be gaining the potential to obtain a more lucrative position or move up a career ladder. For low-skill workers, a reward of employability may also be gaining additional responsibility and autonomy in one’s position, and thus gaining a greater sense of status or prestige (Fitzgerald, 2006; Kalleberg, 2011).
Summary and research questions
In this study, we expand on previous research on employability by analyzing how employer organizations use the practices of employability to encourage low-level workers to improve their skills and productivity, and we examine the rewards that low-level workers receive for participating in employability activities. Drawing on 20 case studies of career development programs within US health care organizations, we have two main research questions we aim to answer in our analysis:
First, how do organizations encourage—and sometimes require—employability practices and activities for low-skill workers? As discussed in the literature review, most research on employability activities has been on middle-class and professional workers. We analyze how organizations develop (and require) credentials and create partnerships with educational institutions to encourage employability, specifically among low-skill and paraprofessional workers, and we explore tensions that arise for organizations and workers when organizations implement these practices.
Second, what are the rewards for workers in terms of social mobility when they participate in different types of career development programs that incorporate employability practices? We categorize and describe different types of career development programs and assess the potential to provide workers with improvements in wages and job quality. Past research has focused on the limitations of career programs for low-skill workers in terms of social mobility (Ducey, 2009); we aim to expand on this research by looking at variation in types of programs and outcomes.
Methods
Research design
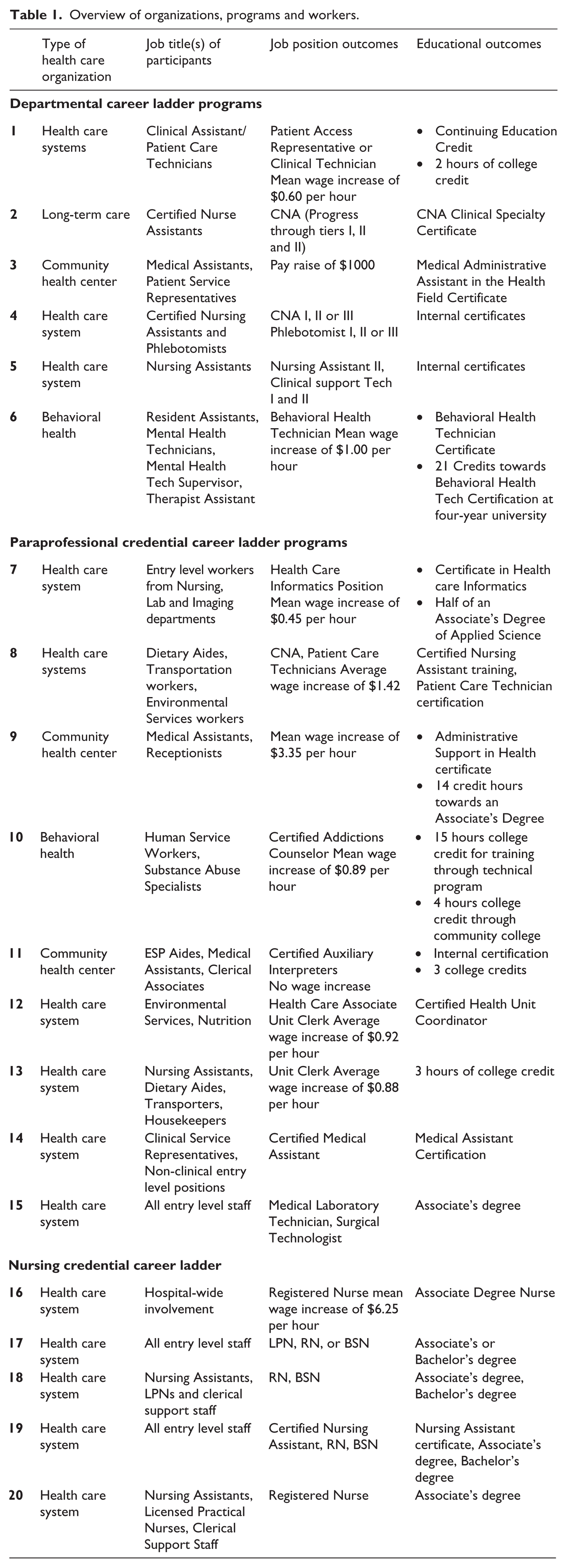
This study is based on case studies of career programs in 20 health care organizations including large health systems, community health centers, behavioral health centers and long-term care organizations. A health system in the United States is an organization that is usually anchored by an acute care hospital, but also often includes primary care practices, specialty practices, rehab facilities, urgent care facilities, and so forth. Health care organizations included in the sample either received grant funding to implement career development programs aimed at entry level worker career advancement or were identified as having successful programs targeting entry level workers retrospectively. Types of entry level workers that participated in career programs included direct care (e.g. nursing assistants), entry level (e.g. dietary, housekeeping) or administrative workers (e.g. unit clerks). Table 1 summarizes the types of organizations included in the sample, the career outcomes and the types of workers targeted.
Overview of organizations, programs and workers.
Interviews and focus groups were conducted between 2005 and 2012. An overview of the number interviews and focus groups conducted is included in Table 2, and a description of types of interviews conducted is included in Table 3. For sites where data was collected prospectively as the organizations implemented the career development programs, interviews were conducted three times over a three-year period (labeled T1, T2 and T3 in Table 2). Often, the same people were interviewed over time unless the position turned over during the intervening period. For sites where the data were collected retrospectively, only one set of interviews was conducted (T1 in Table 2).
Number of interview and focus group participants.
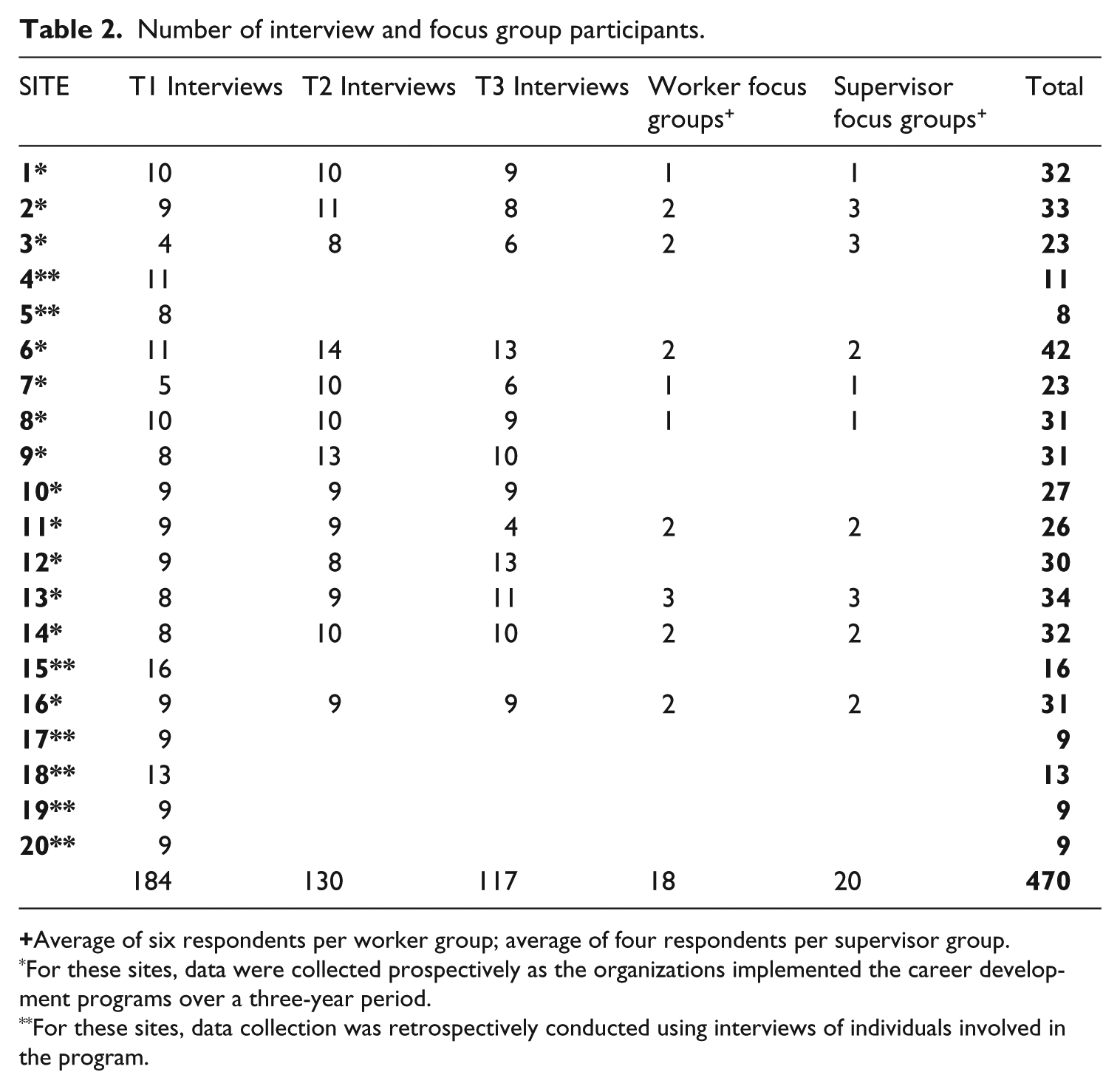
Average of six respondents per worker group; average of four respondents per supervisor group.
For these sites, data were collected prospectively as the organizations implemented the career development programs over a three-year period.
For these sites, data collection was retrospectively conducted using interviews of individuals involved in the program.
Percentage of interviews by type.

In interviews with administrators and managers, we gathered information about their motivations for implementing career programs, the challenges they faced during the implementation process, and details about the programs they developed. We also heard from entry level supervisors and entry level workers about working and staffing conditions, challenges that entry level workers face in moving up within the organization, and how they had experienced the career program that had been implemented at their place of employment. Interviews and focus groups were also conducted after the career program had been implemented, and participants were asked to recall their experiences in developing and participating in the career program. Finally, at some sites where data were collected prospectively, we were able to gather wage data on workers participating in the career program from the employer organization. The mean pay raise (when available) for workers who completed the career program is shown in Table 1.
Data gathering
Semi-structured interviews and focus groups were conducted with entry level health care workers, supervisors and administrators to gather in-depth information about the implementation process of the career program and the work experiences of the entry level health care workers. We conducted 431 semi-structured key informant interviews (e.g. administrators, middle managers and HR personnel), 18 focus groups with entry level health care workers, and 20 focus groups with direct supervisors of entry level health care workers. In the cases developed using retrospective data collection, each set of key informant interviews included someone who could speak to organizational strategy (e.g. Chief Executive Officer), someone familiar with the organizational budget (e.g. Chief Financial Officer), a department head of the area where the program was being implemented, the program coordinator, supervisors (usually two) and frontline workers (usually two) who had participated in the workforce development program. Key informants from the grant-funded cases included those informants mentioned above and an educational informant, a workforce intermediary informant as relevant and an HR representative to speak to workplace policy related to education. We give an overview of the number and type of interview and focus group participants for each site in our sample in Table 2. This triangulation of source data avoids an over-reliance on senior administrators, who often are not familiar with the daily challenges that are faced during the development process.
The interviews took place either in person at the respondent’s place of work or over the phone. Interviews typically lasted about one hour; focus groups lasted about an hour and a half. Respondents were encouraged to talk freely about their experiences of the career programs. The interviews were recorded and transcribed.
Data analysis
Interview and focus group transcripts were coded for themes using NVivo. Coders, which included the authors and additional graduate students, were trained to apply codes consistently. Each transcript was coded twice; discrepancies between codes were discussed until consensus was achieved. Primary level thematic coding was completed to understand the breadth of policy and practice changes implemented to support entry level worker career advancement.
Findings
The practices of employability
In this section, we analyze how career programs within health care organizations encourage—and sometimes require—employability practices and activities for low-skill workers, with an emphasis on credentialing and participation in higher education. The requirement that workers earn a credential is sometimes necessitated by industry regulatory frameworks and professional bodies, but not all health care occupations require certification or licensure. In seven cases in our sample, the health care organization developed their own credential that became required for workers to move into new jobs, creating a new formal expectation of employability for workers. For example, one community health center (case #11 in Table 1) in our sample that served a very diverse patient population needed workers with the ability to assist as interpreters. The community health center developed a certificate reflecting proficiency in interpretation through the local partnering community college. However, many workers were already informally helping as interpreters within the health care organization, so the interpreter credential simply formalized the training and certification that these workers had to have to perform the job task.
Credentials were also intended to signal to workers that the career programs could improve their career potential and give workers a sense of accomplishment (and induce workers to participate in the program). Managers routinely commented that a credential would make workers feel like they were advancing their careers and improving their employability, just as middle-class and professional workers advance their careers by obtaining credentials. For example, in the quote below, a program manager (case #2 in Table 1, T3) describes how earning a certificate will mean so much to these low-level workers because it will improve their employability, something that they have not been able to achieve in the past:
I think just knowing that these 15 people have earned that certificate. I mean that’s something that no one will ever be able to take away from them and they probably never thought it was possible before they had participated in this program. I mean we’re talking about people who were single moms or are single moms who you know got divorced in the middle of this program. Oh my gosh, can you imagine? These are not highly educated people. They don’t make a lot of money. Some of them you known barely completed high school and so to give them that confidence. I think it’s about those individuals and they can take that with them regardless of where they work.
In addition to obtaining credentials, the health care organizations encouraged or required low-skill workers to participate in higher education, another expectation of employability. To facilitate worker participation in higher education, all of the health care organizations in our sample partnered with an external educational institution—typically a community college—to create or provide training and credentials for low-skill workers. In some of our sample cases, health care organizations worked closely with an educational institution to develop a new program, track, or certificate that would address needed firm-specific skills at the health care organization; workers would then be directed towards the new program as part of the career program. In one example (case #7 in Table 1), a large health system in the western region of the US realized that they needed workers that were experts in the electronic medical record system at the health system and general IT but were also proficient in medical terminology and basic patient care. They worked with the local community college to develop a certificate of Health Care Informatics that would require that students take courses in both IT and medical care; the certificate involved 50 credits, about the equivalent of half of an Associate’s Degree. In many cases, the educational institution would provide classes at the health care organization for workers, reducing transportation and travel barriers.
Health care organizations were eager to form partnerships with educational institutions to facilitate higher education for their workers. While the administrators within the health care employers and educational institutions would often describe these partnerships as a ‘win-win-win’ situation, indicating that health care organizations, educational institutions and workers benefited from the arrangements, these partnerships sometimes contributed to confusion for workers and undermined employability and social mobility (Dill et al., 2014). Bureaucratic logistics at both the educational institution and the health care organizations frequently frustrated partners in our case studies and sometimes resulted in a lack of outcomes for workers. For example, workers were sometimes promised some college credit for courses that they completed on-site at their place of work, but ultimately the educational institution, after a lengthy curriculum review process, would refuse to award credit for the course or would award ‘continuing education’ credit, which does not count towards a degree. In one case, workers still received some college credit but it was only acknowledged as course credit if they enrolled in the new degree program with several additional requirements for an associate’s degree. Alternatively, educational institutions would try to accommodate the needs of health care organizations by offering a course on on-site at the workplace, only to face resistance from mid-level managers who had direct control over workers’ schedules.
Health care organizations in our sample assumed some of the costs and risks of the employability practices that they expected of their workers. For example, many of the health care organizations implemented tuition remission policies, where the health care organization would pay the tuition up entry level directly to the educational institution so that workers would not be responsible for any initial costs. Another example of an HR policy that assumed some of the risk of training was the use of educational release time, which allowed entry level workers to use some of their work time for studying or class. However, in all cases, the workers themselves were expected to also carry some of the burden of gaining credentials and training, from covering part of tuition costs to time required outside of work hours. For some workers, the risk of pursuing employability activities resulted in substantial career mobility, but for many workers, as we will discuss below, their investment did not result in meaningful career rewards.
Employability and career development programs
In this section, we examine the rewards for workers in terms social mobility when they participate in different types of career development programs that incorporate employability practices. The different types of career programs within the health care organizations we have identified in our sample include: departmental career ladders, paraprofessional credential programs and nursing credential programs. The three types of career programs we have identified are based on the outcome of the career program for workers, which we describe in more detail below, and are loosely based on the schema used by Fitzgerald (2006). We discuss the expectations of employability placed on the workers and the rewards to workers in the three types of career programs. Table 1 includes descriptions of the career programs in each organization by type.
Departmental career ladders largely focused on providing incremental advancement within a single occupation (cases #1–6 in Table 1). As workers gained additional skills, typically demonstrated through participation in higher education and credentials, they were able to move up within their department. For example, several of the organizations in our sample created career ladders that consisted of differentiations in the occupation of nursing assistant, labeled Nursing Assistant I, Nursing Assistant II and Nursing Assistant III (cases #2, 4 and 5 in Table 1). Depending on the organization, levels were differentiated by increased clinical skills, duties related to peer mentoring or training new hires and leadership roles that included managing schedules on certain floors or within certain organizational units (e.g. floors, units). Most departmental career ladders were firm-specific, meaning that the different levels of achievement were not constant across employers; however, earning a nationally- or state-recognized certification was often a part of climbing a departmental career ladder, which would be recognized by other employers.
In all the cases in our sample, departmental career ladders were limited in scope, typically providing workers with minimal upward mobility. Workers would gain small wage increases as they progressed up the career ladders, but these gains did not usually amount to more than an extra dollar per hour raise, even after earning certification (see cases #1 and #6 in Table 1). Despite these minimal gains, however, program managers and administrators would frequently use the language of upward social mobility when talking about the program, invoking middle-class conceptions of employability. For example, administrators and workers alike would comment on how the career ladder would help them to achieve their ‘career goals.’ For example, in the quote below a department manager (case # 5 in Table 1, T1) describes how creating a departmental career ladder for workers in patient care will enable people who ‘want more’ to ‘achieve their goals,’ which will help with worker retention:
So what we want to do is provide an opportunity for people to stay. If I have people who are in housekeeping and patient care or dietary and they really want to do more with their career . . . I want to provide them an opportunity so they don’t have to leave me or go someplace else to achieve those goals.
Administrators would also talk about how the career ladder would allow workers to have more autonomy and responsibility in their jobs, which they thought would improve worker satisfaction. Workers were, in many cases, eager for more responsibility and recognition of their skills, but they also commented that they felt that their employer took advantage of them by giving them additional responsibilities without a commensurate increase in pay. In the quote below, a Medical Assistant (MA) in a large health system (case #14 in Table 1, T3) describes how she is climbing a career ladder for MAs and now has earned her MA certification (MAs do not have to have to be certified to be employed in the US). Unfortunately, she did not receive much of an increase in pay after completing her credential, but she quickly brushes off her disappointment by explaining that she did it ‘for the education’:
I did I get my [MA] certification. There wasn’t very much of an increase in pay, which I really didn’t do it for the pay. I did it for the education. But yeah, it wasn’t what they said I was going to get bumped up to which was kind of confusing for me because I was told one thing before I started the program and it was not anything close to what they told me after I had gotten my increase but once again I, you know I didn’t really do it for the money. I did it for advancing my knowledge in the medical field and hoping to continue with medicine.
The most common type of career program in our sample organizations was one that culminated in earning a paraprofessional credential (cases #7–15 in Table 1). In these programs, workers received training through higher education and credentials to move into a new occupation. The credentials earned by the workers varied in the amount of time to completion and career advancement; some culminated in a nationally- or state-recognized certification, while others were firm-specific credentials. For example, many dietary and housekeeping workers were eager to earn credentials to move into a clinical position, which they viewed as a step towards becoming a nurse or other allied health professional. Unfortunately, in most cases, moving into a clinical position does not in fact help workers progress towards becoming a midlevel worker, like a nurse or allied health professional, but we found that workers were frequently unclear about the pathways they need to take to reach their career goals. Further, the involvement of external educational institutions and the use of credentials often gave workers ‘false promise’ that they were moving towards a career goal or outcome (Ducey, 2009). Unfortunately, since most health care credentials do not build on each other, most of the departmental career ladders provided little training or credentials that would help workers move towards a midlevel health credentials. In the quote below, an individual with her CNA certification and other paraprofessional credentials (#5 in Table 1, T1) expresses her frustration that her experience does not help her move towards a career in nursing:
Why did I have so much stuff before we get in if, if we’re experienced in it why just, why can’t we, why can’t we use our CNA credentials, and why can’t I use well, I have CNA, I have medication aide and I have an associates. You tell me that’s not good enough to get into a nursing school? And not just with that but I mean we have the heart. My heart is, my passion is nursing. I want to do nursing but it’s so hard to get in. You don’t have this grade point average, we don’t have this, we don’t have that.
However, some paraprofessional certificates can provide substantial upward mobility for workers. For example, one organization in our sample (case #15 in Table 1) gave all entry level staff within the health system an opportunity to earn an associate’s degree that would allow them to work as a surgical technologist. The median pay for surgical technicians is about $42,000 per year, or about $20 per hour, a substantial increase for many entry level health care workers.
The occupational credentials offered in our sample of organizations were also sometimes untraditional and reflected the changing health care context and workforce. For example, as described above, one health system in our sample developed a Certificate of Health Care Informatics (case #7 in Table 1). The limitation of these more non-traditional credentials, however, is that they tend to be firm-specific, making the credential less marketable to other employers, at least in the early stage of development. Indeed, the organization that built a career ladder around the Certificate in Health Care Informatics found that owing to the economic recession, they were unable to hire many of the workers for the positions for which the workers had trained.
We found that paraprofessional credential programs were often what have been termed career lattice programs. Career lattices offer multiple pathways to jobs that are both lateral and vertical in an attempt to improve career opportunities for workers and meet emerging workforce needs of health care organizations (Sporing et al., 2012; Stone, 2007). For example, a health system might choose to train entry level or supervisory housekeeping staff as certified nursing assistants. The completion of the certified nursing assistant credential (continuing education class and competency exam) might result in a lateral move to the nursing department, but this may be useful to the worker as there is a career ladder for CNAs (e.g. CNA 1, CNA 2, Shift Lead), where there is no such ladder in housekeeping department. However, attaining the certified nursing assistant credential may only result in marginal immediate compensation benefits for the worker. Below a project manager (case #12 in Table 1, T2) describes how a career lattice works for workers:
We’ve quickly realized we don’t have a ladder. We have a lattice. You know, if I am a dietary worker maybe I do want to go be a direct patient care person I can do that. Or if I’m already in direct patient care, maybe if I’m a CNA I and I want to be a II. That might be the path for somebody but somebody else says well, you know I want to be a CNA III and then I want to go specialize in obstetrics or urology or cardiac or, so the matrix was it’s all over.
The last type of career program we describe that was adopted by seven organizations in our sample was a traditional nursing credential program (cases #16–20 in Table 1). The nursing career ladders that we discuss in the article are developed for entry level health care workers to move into nursing positions. Such programs have been used extensively in health care organizations to train (and then retain) low-level employees to be nurses (Cheung and Aiken, 2006; Goldberger, 2005; Hassmiller and Cozine, 2006). In nursing credential programs, the employer organizations would typically assist entry level health care workers in earning a credential to become a Licensed Practical Nurse (LPN), followed by earning an associate’s degree in nursing and becoming a Registered Nurse (RN). Most organizations in our sample then supported workers in the pursuit of a Bachelor’s of Nursing (BSN), and sometimes even a graduate degree in nursing. Not all workers would complete all levels of the career ladder, naturally, but the credential programs allowed workers who were interested in upward social mobility assistance in a stepwise progression through the credentialing process.
In one example, a western health system in our sample had an arrangement with the local community college where hospital employees who met the standards for admission into the nursing program were considered for slots set aside for the health system and did not have to compete for acceptance in the general applicant pool. After employees had completed an Associate’s Degree in Nursing (ADN) through the community college, hospital employees were eligible to obtain a Bachelor’s of Science in Nursing (BSN) through a local four-year university. All but 10 elective credits were taught onsite at the hospital, and employees attended class once a week for three years, allowing them to work full-time or nearly full-time while completing their degree.
A clear advantage of traditional nursing credential programs is that they can provide substantial upward social mobility for workers. The median wage for Certified Nursing Assistant—which would be the lowest rung of the nursing hierarchy—is less than $12 per hour (US Department of Labor, 2017b). Registered Nurses (RN), on the other hand, earn a median wage of about $30 per hour. Further, a nursing credential is extremely portable and highly valued by all health care employers, an asset for workers that may want or need to switch jobs. Among our case studies, nursing credential programs appeared to be the most effective in providing workers with substantial upward mobility; for example, at case #16 in Table 1, hospital workers were able train to become RNs, resulting in an average increase in pay of $6.25 per hour. We interviewed many managers at these sites that had ‘climbed the ranks’ of the organization by becoming an LPN, then an RN, and then typically earning a BSN, all with significant financial and time investments from their employer.
However, it should be noted that building a career program that supports workers as they earn nursing credentials requires significant investment from organizations, and consequently, nursing credential programs were only present in large health systems that employ thousands of workers. Smaller organizations or settings where RNs are used less (e.g. long-term care or behavioral health) would not necessarily benefit from investment in nursing credentials. Earning nursing credentials also requires substantial commitment on the part of the worker: completing a nursing degree (while also working) takes years of classes and clinical rotations and may not be an option for many entry level health care workers.
Discussion
The purpose of this study was to analyze how employer organizations place expectations of employability on low-skill workers, and to examine the rewards that low-level workers receive for participating in employability activities. Our first research question focused on how organizations encourage—and sometimes require—employability practices and activities for low-skill workers. We found that employers in our sample applied the practices of employability typically seen among middle-class and professional workers to their lowest level workers, a finding that supports Smith’s (2010) claim that the expectations of employability have spread to low-skill workers. For example, all of the organizations in our sample included the receipt of a credential by participating workers, even if it was an internal or newly developed credential. Credentials were sometimes required for workers to move into new positions (e.g. registered nurses, surgical technicians), but frequently credentials were incorporated to formalize work that was already being done. Such requirements reinforce Chertkovskaya et al.’s (2013) argument that employability has now become a requirement for employment, even for low-level employees.
Health care organizations largely drew on outside educational institutions to legitimize the credentials that were awarded as part of a career ladders and used a variety of HR policies and practices to reinforce partnerships with educational institutions, which shifted some of the risk from workers to employers. The adoption of some of the risks of training by health care organizations, such as paying costs of tuition or allowing workers to complete training during work hours, stands in contrast to the literature on externalization or ‘responsibilization,’ where workers are largely responsible for their own career development (Vallas and Prener, 2012). Employers in our study recognized the limitations of low-wage workers to engage in employability activities, but because conditions in the health care sector such as the demand for high quality of care, health care organizations have increasingly decided to invest in training for low-level workers (Fitzgerald, 2006). Unfortunately, as we discuss in the findings section, workers in all organizations were still required to take on some of the risks of training and often did not receive meaningful rewards for their efforts.
Our second research question focused on the rewards for workers in terms of social mobility when they participate in different types of career development programs that incorporate employability practices. We found that top-level administrators, managers and even the workers used the language of upward social mobility and career progression when describing their career programs, even when the rewards to the workers for participation were minimal. However, our findings suggest that the type of workforce development that workers participated in made a substantial difference in their potential upward social mobility. In general, we found that department career ladders provided only limited upward social mobility for workers, despite the fact that administrators frequently used the language of employability and upward social mobility to describe worker opportunities. Paraprofessional credential programs varied in their ability to provide workers with upward social mobility; some programs—typically programs that worked with the established occupational structure in health care—could lead to jobs that would boost workers into the middle class, such a surgical technologist position. The career programs that consistently helped workers to gain upward social mobility were nursing credential programs, which enabled low-level workers to move into licensed nursing positions.
For those workers who do not experience much upward mobility as a result of employability activities, Ducey (2009) largely places the blame for ‘false promises’ of employability and upward mobility on health care organizations, who want to have a highly trained low-level workforce but do not reward workers for their training. However, the structure of educational institutions also contributes substantially to a lack of upward social mobility among workers, despite workers’ efforts of increasing their employability. As discussed above, the health care organizations in our sample all partnered with an educational institution, usually a community college, to provide training and award a credential as part of a career program. We found that students were often given little guidance in terms of how to accomplish their goals and were confused by pre-requisite courses needed for entering a degree program, developmental educational credits, which are often awarded but do not count towards a degree, and the required courses needed for the credential they hope to achieve (see Goldrick-Rab’s (2010) review of challenges that students face in navigating the community college system). Consequently, entry level health care workers would often spend years taking courses that provided little in the way of progress towards a meaningful credential or degree. This lack of ‘stackable’ credentials and intra-occupational courses means that the risks workers take in gaining training and increasing employability rarely is accompanied by meaningful rewards.
We found that workers in these low-level health care occupations were largely aware that they needed to obtain additional training in order to move up within the health care sector, and they were often eager to participate in any training programs that were made available to them. In other words, they were aware of the expectations of employability. Many had career goals of moving into mid-level health care occupations (such as nursing or allied health), but the barriers to achieving those goals were too high (e.g. no time for classes, too expensive, nursing programs too academically competitive, etc.). Consequently, when training was made available with lower barriers, they were hopeful that it would provide them with career opportunities. We found that low-wage workers in health care settings sought to improve their employability through additional training (Smith, 2010), which they viewed as essential to upward mobility. Unfortunately, in many cases in our sample, these efforts to improve their employability did not lead to meaningful changes in their income or job prospects. Where meaningful changes were realized, occupational and educational structures were well-established, navigable and corresponded to career ladders.
While we have focused on the role of the organization in the requirement of credentials in career programs, frequently it is professional organizations that are pushing for workers to have required credentials. As occupations aim to secure a monopoly over a knowledge jurisdiction (Abbott, 1988), professional organizations often seek to use certification and/or licensure to limit competition and raise wages (Kleiner, 2011). However, research suggests occupational certification and licensure largely does not raise wages, particularly for women or minorities (Redbird, 2017). While we did find that workers that became licensed nurses experienced the most substantial upward mobility in our sample, occupational certification often did little to secure higher wages for workers.
Conclusion
Our findings and those of scholars like Ducey (2009) demonstrate that there is no ‘quick fix’ for promoting upward social mobility in the health care sector. Because of required credentials, workers need to invest years of training, both in the classroom and on-the-job, to obtain substantial upward social mobility. When organizations have the expectation of employability for their low-level workers—along with some logistical support—it can be a welcome opportunity for workers to gain additional credentials and skills with some needed assistance from their employer. In other words, the expectation of employability on the part of workers and employers can lead to meaningful opportunities and rewards for low-skill workers, who typically lack opportunities for advancement (Kalleberg, 2011). However, we found that the activities of employability for low-level workers, such as participating in higher education and earning credentials, were too often ‘false promises’ (Ducey, 2009) and provided few rewards for workers’ efforts.
Our findings indicate that policymakers and funders of workforce development and job training programs should support programs that have demonstrated outcomes for workers; in the health care sector, established, nationally recognized credentials in nursing and allied health provide the most potential for upward mobility for workers. Our findings also suggest educational reforms, such as creating classes and credentials that build or ‘stack’ together towards a degree, may help workers to avoid accumulating many low-level credentials that lead to only limited increases in compensation. Future research can expand on our study by investigating whether there are expectations of employability being placed on low-level workers in other industries and sectors, and whether employability activities provide opportunities for upward mobility for low-skill workers across industries.
Footnotes
Acknowledgements
The authors would like to acknowledge Thomas R Konrad, Emmeline Chuang, Brandy Farrar and Kendra Jason for their help in collecting and coding the data used in this project and the many employers and frontline workers who shared their time and insights with us across the two projects. We would also like to thank Associate Editor Kim Hoque and three anonymous reviewers for their guidance in shaping this article.
Funding
This research was supported by funding from the Hitachi Foundation (grant number: 5-40680) and the Robert Wood Johnson Foundation (grant number: 59245).