
Abstract
How does engagement in multiple health behaviors consolidate into health promoting health lifestyles, and how does economic development provide a broadly shared living condition to enable participation in health promoting health lifestyles? To answer these questions, we harmonize information from the 2011 International Social Survey Programme and the 2014 European Social Survey to examine patterns of health lifestyles and subsequent associations with self-rated health in representative samples of 52 country-years nested in 35 countries, with repeated observations from 17 countries. We find individuals engage more frequently in health promoting behaviors in countries with higher levels of economic development. Moreover, we find a tighter connection between health lifestyles and health in countries with higher levels of economic development. Critically, we move health lifestyles research forward by testing the consequences of within country changes in economic development, finding that growth in economic development increases the engagement of health promoting health behaviors. Policy and theoretical implications are discussed.
How are health lifestyles informed by where people live, and where do these health lifestyles translate into positive health outcomes? 1 While many health lifestyle studies focus on a single country context (Burdette et al., 2017; Christensen and Carpiano, 2014; Saint Onge and Krueger, 2017) or a set of bordering and institutionally similar countries (Cockerham et al., 2004, 2006), recent cross-national research has underscored the importance of situating health inequalities as a function of macrolevel factors occurring between countries (Boyle et al., 2006). To that end, comparative health scholars have conceptualized unequal health outcomes as conditional on broadly shared national social, political, and economic characteristics that vary between countries and within countries across time (Beckfield et al., 2013; Bakhtiari et al., 2018; Olafsdottir et al., 2014; Olsen and Dahl, 2007; Präg et al., 2013, 2016). Motivated by these insights, we examine how between-country inequalities in GDP per capita, which we use as a general proxy of economic development, influence participation in key health behaviors, and how variable health outcomes follow from the enactment of otherwise similar health lifestyles in more or less affluent countries. We extend health lifestyles theory by connecting country-level economic development to individual-level participation in multiple and potentially contradictory health behaviors (Cockerham, 2005; Saint Onge and Krueger, 2017). While health lifestyles research offers a framework well-suited for this type of analysis, it has typically restricted the importance of social context to subnational features of households or neighborhoods. Yet, a country’s economic development similarly provides a broadly shared context that, as we will show, associates with participation in health lifestyles.
We assess these issues with data from the 2011 wave of the International Social Survey Programme (ISSP) and 2014 European Social Survey (ESS). Both surveys include information on similar health behaviors and health outcomes for 52 country-years nested in 35 countries, as well as repeated observations from 17 European countries. We draw three main conclusions. First, we find that respondents on average engage in health promoting lifestyles—eating healthy foods and exercising more while smoking and drinking less heavily—more frequently in more affluent countries compared to less affluent ones. Second, we find that associations between health lifestyles and self-rated health are greater in higher income countries. Third, results replicate in models pooling datasets and accounting for time-invariant country-level characteristics, bolstering confidence in main conclusions.
Background
Economic development and between-country inequalities in health
A substantial body of research shows that country-level economic development affects health outcomes. Following economic growth, populations typically experience improvements in living conditions and improved access to medicine, medical innovations, technologies, healthcare providers, and healthcare systems, culminating in improved population health (Farmer et al., 2013; Olsen and Dahl, 2007; Semyonov et al., 2013; Subramanian et al., 2002). For example, scholars find that higher levels of development correspond to gains in life expectancy and improvements in other health outcomes such as infant mortality and childhood health (Bloom and Canning, 2007; Clark, 2011). Other studies have explored the shifting etiology, onset, and types of disease most prevalent in nations across levels of development (McKeown, 2009; Wahdan, 1996). These studies show how development has affected individual behaviors and national institutions and cultures, resulting in substantial shifts in health, disease, and mortality (Drewnowski and Popkin, 1997). 2
Specifically, studies demonstrated a relationship between health behaviors and economic resources at both the individual and country levels (Pampel et al., 2010). For example, economic development has been associated with shifts in: diet (Drewnowski and Popkin, 1997), exercise or physical activity (Guthold et al., 2018), smoking (Pampel and Denney, 2011), and alcohol consumption (Graham et al., 2011; Grittner et al., 2013). However, findings from this research indicate engagement in health behaviors is complex and higher levels of economic development are not always associated with uniform engagement in health promoting behaviors. For instance, studies on the nutrition transition document a relationship between economic development and increased consumption of animal fats and added sugars in low and middle-income nations (Drewnowski and Poulain, 2018). The multifaceted and potentially conflicting relationship between individual health behaviors and health outcomes suggests an examination of multiple health behaviors and structural factors simultaneously as a way of capturing the relationship between economic development and overall health lifestyles of an individual or population.
Therefore, in the current research, we assess how between-country variation in economic development influence participation in key health behaviors, and how such health lifestyles differences translate into health outcomes. As noted above, research has established that social conditions within countries influence health through a variety of mechanisms, including participation in a variety of health behaviors, with those in higher economic positions typically more likely to engage in health enhancing or protective behaviors (Phelan et al., 2010). Yet, it is unclear how country-level development influences participation in multiple and potentially contradictory health behaviors, and whether the health benefits associated with health behaviors are similarly distributed both across national contexts based on economic development and within countries based on health behavior participation. Based on the extensive findings in previous research of the importance of cross-national context for health outcomes (e.g. Beckfield et al., 2013), we apply a similar logic to between-country associations in economic development, health behaviors, and health outcomes. Should such associations be found, they would beg the question of whether the benefits of participating in certain health behaviors are equally beneficial between countries. To assess these relationships, we use health lifestyles theory to develop a theoretical foundation for expectations in how country-level variation in economic development may covary with individual-level participation in multiple and potentially contradictory health behaviors (Cockerham, 2005; Saint Onge and Krueger, 2017).
Health lifestyles
We develop our expectations from health lifestyles theory, a mature theory in medical sociology used to explain the combination of health behaviors and their associations with health outcomes. Health lifestyles are “collective patterns of health-related behavior based on choices from options available to people according to their life chances” (Cockerham, 2005: 55, see also Saint Onge et al., 2014; Saint Onge and Krueger, 2017). This definition builds upon the classic Weberian concept of lifestyle, whereby social action is understood through its regular and predictable manifestation across multiple individuals over time. According to this theory, health lifestyles are a form of consumption that one engages in to produce good health and directly associates health behaviors to status group participation, akin to the more general process of consumption as a tool to signal status (Cockerham, 2000). Individual health behaviors are thus partially enacted in relation to how they signify larger group affiliation and social structures (Cockerham, 2000).
Key to this theory is the status group, which is comprised of individuals who share class and status backgrounds (Cockerham, 2005). To maintain or gain membership in a status group, one must adopt the group’s lifestyle (Cockerham, 2005). Typically, the forms of consumption or practice include behaviors such as diet, exercise, smoking, and alcohol use (Cockerham, 2000; Cockerham et al., 2004). The pattern of these behaviors reflects a population’s “knowledge and norms about what constitutes healthy, stress relieving, or pleasurable behaviors” (Saint Onge and Krueger, 2017: 89). Health lifestyles theory calls attention to the fact that specific health behaviors—such as diet, exercise, and use of drugs and tobacco—neither happen in isolation from one another nor are based entirely on individual choice. Rather, one health behavior occurs in connection with another, is influenced by beliefs about health and illness, is shaped by, and signals, group identity, and is enabled or constrained by the particular context in which someone lives (Mollborn and Lawrence, 2018). In addition, it is important to recognize that groups may alter their engagement in health behaviors over time as new knowledge, norms, or access to consumer goods emerge. Furthermore, individuals may be motivated simultaneously by multiple logics to engage in health behaviors affiliated with a particular status. As an extreme example, Becker (2004), finds that during a time of great economic and social transition, young women in Fiji reported altering their dietary and exercise practices based on several different reasons including new cultural norms of body image, public health messages about obesity, and emerging economic opportunities. Relatedly, research on smoking diffusion and utilization of health technologies across socioeconomic status groups highlights the importance of status alongside public health knowledge and broader social changes as motivations for engagement in different health behaviors (Chang and Lauderdale, 2009; Link and Phelan, 2009; Pampel, 2002, 2005). While it is beyond the scope of the current study to assess specific motivations behind behaviors, we believe these studies offer further support to examine multiple and potentially conflicting patterns of health behaviors within a broader shifting social context (Burdette et al., 2017; Christensen and Carpiano, 2014).
Health lifestyles theory has mostly been used to study variation within a single country. However, previous studies provide important motivations to consider national context as a major influence for health lifestyles, whether through local cultural norms (Cockerham et al., 1988, Christensen and Carpiano, 2014) or through country-level structural constraints or ideologies (Cockerham, 2000). For example, Cockerham (2000) explores health lifestyles in Russia and finds that working-class middle-aged men may be at a greater risk of participating in negative health behaviors, in particular high levels of alcohol consumption and to a lesser extent smoking and eating an unhealthy diet, due to cultural norms surrounding these activities and social structures that limit available alternate choices. A few studies have included comparisons of health lifestyles between nations with similar political legacies, such as former communist or socialist states (Cockerham et al., 2004, 2006). Taken together, these studies demonstrate the utility of extending the health lifestyle theoretical framework to the cross-national case.
Social context and health lifestyles
Health lifestyles research has only rarely been conducted cross-nationally, and so we extend this line of research in three critical ways. First, previous studies do not include a range of nations with varying levels of economic development (Cockerham et al., 2006, for an exception see Olsen and Dahl, 2007). Focus on a smaller set of institutionally and culturally similar countries restricts analytical capacity to assess the link between health lifestyles and between-country inequality. Second, several studies that do assess health lifestyles cross-nationally focus on a single health behavior. Similarly, Olsen and Dahl (2007) measure alcohol consumption as an indicator of health lifestyle participation, while Cockerham et al. (2006) examine alcohol consumption, smoking, and food consumption separately. Third, while previous work suggests that changes in broader institutional contexts impact health lifestyles (Cockerham et al., 2006) and that health lifestyles change across the life course, particularly in relation to an individual’s early life socioeconomic context (Burdette et al., 2017), scholars have not tested empirically how changes in country level economic development influence participation in health lifestyles and subsequent health outcomes. Understanding shifts in health lifestyles as enabled or constrained by broader social contexts is an essential part of the theoretical underpinnings of health lifestyles theory. However, this facet of the theory largely remains empirically unexamined.
We argue that integrating health lifestyles theory into cross-national studies of health inequalities provides a unique opportunity to extend scholarly understanding of the relationship between social context and health behaviors. Two aspects of health lifestyles theory are particularly well suited for the integration of a cross-national study of between-country inequalities in development. First, we argue that the theory’s inclusion of group-level analysis offers a useful method for conceptualizing between-country differences in health behaviors. As countries experience economic growth, there may be a corresponding widening of access and availability to new goods and services that ease participation in a particular set of health lifestyles. Participation in health behaviors can serve as a marker of status that may be used to align with, or signal, participation in a country’s newly realized development (Becker, 2004; Drewnowski and Popkin, 1997; Popkin, 2001). Of course, overall economic growth that results in between-country inequalities coexists with the unequal distribution of economic resources within countries. Although the latter is beyond the scope of the current study, we consider its implications in the Conclusion.
Second, the theory’s concept of “living conditions” can integrate country level development into heath lifestyles. Living conditions are one of four structural variables that Cockerham (2005) identifies as influencing life chances, processes of socialization, and experience, all of which motivate the enactment of particular health behaviors. 3 Living conditions refer to things that are associated with housing, utilities, neighborhoods, and safety. Conceptualized more broadly, living conditions can be understood as a set of contextual economic conditions above the individual household that allow for access and availability for participation in health lifestyles. To date, few empirical studies have examined variables associated with living conditions (Cockerham, 2005). Yet, some research suggests that both health lifestyle participation and the relative consequence of lifestyle participation on health outcomes are channeled through living conditions (Cockerham, 2013). Furthermore, living conditions are often viewed through the lens of individual-level socioeconomic differences within a contained geographical region, such as the unequal distribution of access to grocery stores (Cockerham, 2005). Restricting geographical region allows for a deep understanding of how local conditions may structure individual agency and group norms surrounding health lifestyle participation. Yet, it necessarily shuts off broader questions of development that are broadly shared across individuals within a country. We agree that this is an important aspect of the theory that should be maintained and view our study as complementary to studies that focus on regional or neighborhood definitions of living conditions. For instance, country level economic development may be associated with smoking and alcohol regulations, policies that promote increased access to green space, bike lanes, or the availability of gyms and other infrastructure that contribute to the establishment of health lifestyles. We argue that when considered in a cross-national perspective, country-level development can be conceptualized as a broadly shared living condition that influences life choices and life chances of the population, which in turn determine health lifestyles.
We believe extending living conditions to the country level is supported by previous research that finds differences in health behaviors between countries based on their grouping into categories of economic development (Pampel and Denney, 2011; Pampel et al., 2012; Sosnaud and Beckfield, 2017). Specifically, while large variation exists in access to resources at the subnational level, we argue that economic development represents an important shared context for those living in a nation as it impacts institutions and systems that may inform the life chances, or access and availability of health behaviors from which individuals may choose. For example, varying levels of economic development may influence change in: education, public health infrastructure, housing, occupational industries, food systems and transportation systems, all of which influence health behaviors, as well as, the norms and knowledge surrounding health beliefs and practices at the population level.
In total, we consider how the living conditions associated with between-country variation of economic development associate with different levels of engagement in health lifestyles. Furthermore, we test whether nation-level economic conditions allow for greater engagement with healthier health lifestyles. We are not aware of a cross-national study of health lifestyles examining this question, and so beyond the innovation of bringing health lifestyles theory to the cross-national study of health, the current study theoretically innovates health lifestyles theory by testing the key concept of living conditions.
We argue that an individual’s health lifestyle participation should be influenced by the broadly shared living condition of their resident country. Given that improvements to these living conditions should not only motivate increased participation in health positive health lifestyles but also increase the effectiveness of translating these health lifestyles into positive health outcomes (Cockerham, 2013; Link and Phelan, 1995), it is reasonable to expect growth in shared living conditions to affect both health lifestyle participation, as well as subsequent associations with health outcomes. With the above discussion in mind, we test the following hypotheses:
Data
We use data from two cross-national surveys, the ISSP 2011 Health module and the 2014 ESS Social Inequalities in Health module. Both surveys include similar questions on health lifestyles and health outcomes, allowing us to cross-verify results with two high-quality cross-national datasets. In total, we have representative survey information from 52 country-years nested in 35 countries; 17 countries are sampled in both surveys, which we use to further test expectations. Countries in these samples primarily come from high- and middle-income countries (see the Online Appendix and notes in Figure 2 for a full listing of countries in the ISSP and ESS datasets). Unfortunately, the countries with the lowest levels of economic development are not available in these data. Nevertheless, we highlight the fact that these samples of countries provide a much wider range of countries used in health lifestyles studies.
We construct health lifestyles measures using four health behavior indicators frequently used health behavior measures in the health lifestyles literature (e.g. Cockerham et al., 2006; Saint Onge and Krueger, 2017): the frequency of eating fresh fruits and/or vegetables, physical exercise, heavy alcohol consumption, and smoking cigarettes. To make answer choices more comparable across surveys, we recode survey-specific responses for the first three measures to indicate the number of days per week the respondent engages in the health behavior. For categories indicating ranges, we take the average of the minimum and maximum possible values for the answer. For smoking, we recode responses as the number of cigarettes they smoke per day, from 0 to 40, multiplied by seven. Question wording, survey-specific outcome categories, and additional discussion of comparability are included in the Online Appendix.
We use self-rated health (SRH) as a general measure for overall health. The ISSP includes a question asking, “In general, would you say your health is” [1] Excellent, [2] Very Good, [3] Good, [4] Fair, or [5] Poor. The ESS includes a question asking, “How is your health in general? Would you say it is” [1] Very good, [2] Good, [3] Fair, [4] Bad, or [5] Very bad. We follow Bakhtiari et al. (2018) and recode responses of “Very Bad,” “Bad,” “Poor,” and “Fair” as 0, and “Excellent,” “Very Good,” and “Good” as 1. The difference in response choices raises concern about comparability across surveys. We discuss this point in greater detail in the Online Appendix. We also replicated all main results using obesity status as an outcome and reached the same conclusions (available upon request).
Our main country-level indicator for living conditions is logged GDP per capita (Olsen and Dahl, 2007), with values measured in 2011 US dollars, collected from the World Bank. We use a one-year lag and match values to country-survey specific years of survey administration. We include replications of interaction results without logging GDP per capita in the Online Appendix.
Individual- and country-level variables
We adjust for all individual-level characteristics available and similar across datasets. We primarily focus on demographic and socioeconomic characteristic that may confound the association between health behaviors and health outcomes. These include age, sex, educational attainment (less than lower secondary, lower secondary upper secondary, post-secondary, advanced vocational, lower tertiary, upper tertiary), marital status (married/partnered, separated/divorced, widowed, never married), work status (employed, unemployed, student, permanently sick or disabled, retired, other), relative income, 5 the number of individuals in the respondent’s household, and frequency of religious attendance. 6 In supplementary analyses that attempt to better establish the ordering between health behaviors and SRH (in the Online Appendix), we include measures of whether a respondent has a chronic condition and a respondent’s BMI in categories of underweight, normal weight, overweight, obese I, and obese II. We also adjust for country-level characteristics that might confound the relationship between logged GDP per capita and health outcomes and lifestyles: infant mortality, the percent of individuals aged 65 and older, healthcare spending as a percent of GDP, the unemployment rate, and the percent of a country’s population living in an urban area. Some of these measures, such as the age distribution and urbanization, could potentially be mechanisms of development. Country level controls are included in the Online Appendix. Similar to the conceptual setup of Alderson and Nielsen (2002), we assess associations between development and our health outcomes without country controls as well as with all controls. Remaining associations between logged GDP per capita and health dependent variables should more directly measure the influence economic development specifically, rather than the mechanisms caused by economic development.
Methods
We employ a multilevel modeling strategy often used in cross-national studies of health behaviors and outcomes (Bakhtiari et al., 2018; Präg et al., 2016). When modeling results separately by survey, we use two-level regression models, with individuals nested in countries. In some analyses, we pool surveys and estimate three-level models, with individuals nested in country-years nested in countries. We use linear mixed-effects regression models when predicting health lifestyles, and mixed-effects logistic regression models when predicting SRH. Models predicting health outcomes include random coefficients for health lifestyle scales, allowing slopes to vary across countries, as well as cross-level interactions between individual- and country-level measurements of socioeconomic status. We make additional adjustments, described below, when estimating cross-level interactions based on methodological developments by Giesselmann and Schmidt-Catran (2019). 7
Special consideration of the difference between observational and causal effects is warranted. Our assessment of the association between health behaviors and health outcomes cannot demonstrate a causal effect because of the cross-sectional and observational nature of our data. We include these results to demonstrate that associations in our study align with the vast majority of studies examining the link between health behaviors and health outcomes. Our main innovation comes from the association of within-country GDP change and change in mean health behavior and health outcomes. This moves the study of health lifestyles and living conditions closer to a causally identified association. Yet the standard and well understood cautions of quantitative analyses of observational datasets apply to our study, and we are aware that we model descriptive associations and not clean causal effects. 8
Health lifestyles
We conduct weighted principal components analysis (PCA) on our four health behavior indicators to construct health behavior scales. In single country studies, it is common for researchers to use some form of latent class analysis when combining health behavior indicators (e.g. Saint Onge and Krueger, 2017). Unfortunately, preliminary testing of multilevel latent class analysis, an approach appropriate for the current study’s data structure had convergence issues. We therefore settled on principal components analysis because of the simplicity of the assumptions behind this scaling approach and the restriction of research degrees of freedom in its implementation compared to other scaling methods. We are cognizant that any scaling decision could be reasonably argued against compared to a favored alternative.9,10 Results in Table 1, estimated separately by survey and pooled together, show response patterns primarily load onto two components. High values for the first component identify those who frequently eat fruits and vegetables, exercise, refrain from heavy drinking, and do not smoke cigarettes. We label this factor universal health lifestyle, as this scale differentiates those who frequently partake in all healthy behaviors versus those who partake in none. High scores on the second component identify individuals who frequently eat fruits and vegetables, heavily drink alcohol, smoke cigarettes, and exercise. We label this factor compensatory consumption, as respondents with high values on this factor consume substances, whether healthy or not, and engage in frequent exercise. Additional discussion of scale construction, and tests of individual items are both included in the Online Appendix.
Weighted principal components analysis for health behaviors.
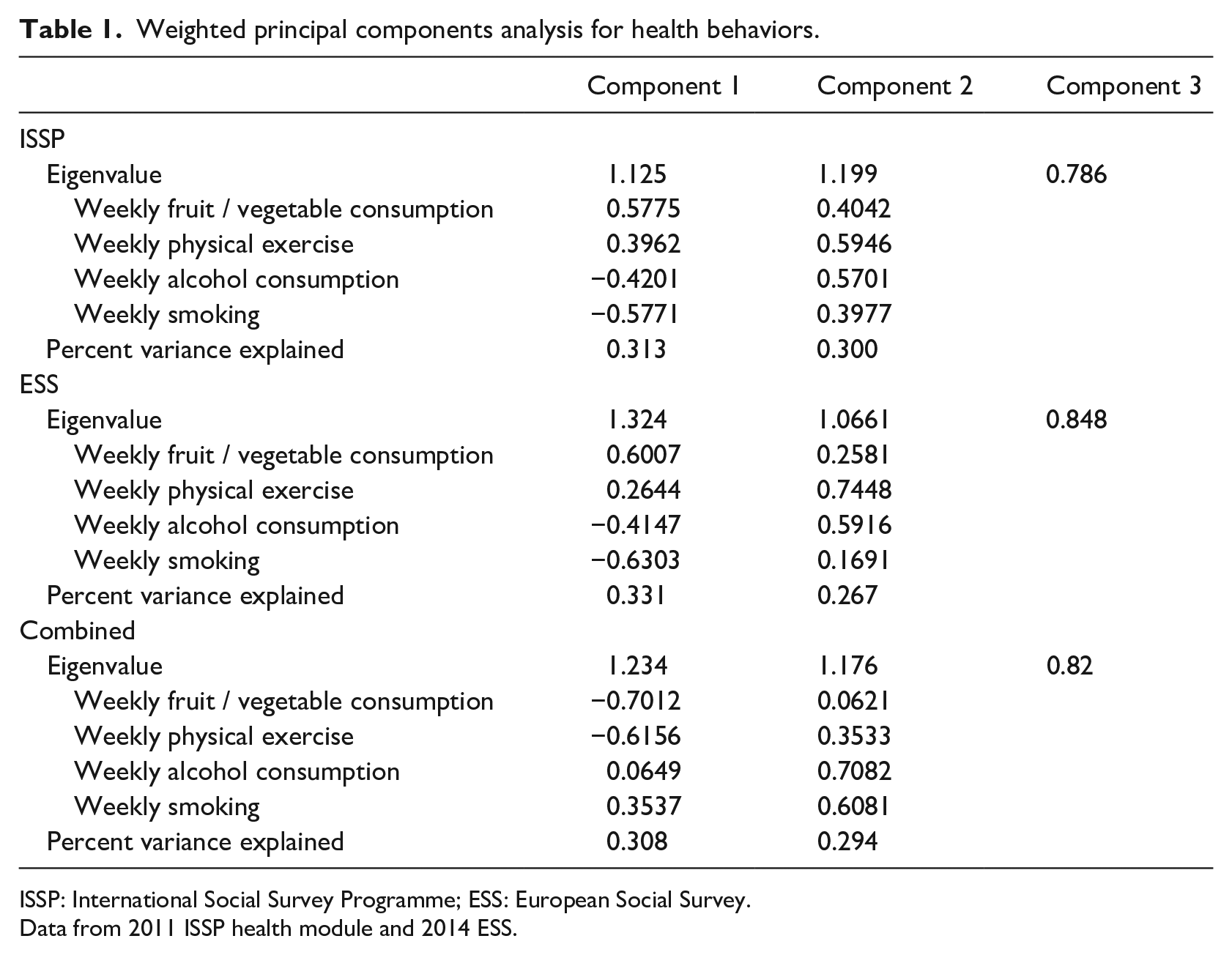
ISSP: International Social Survey Programme; ESS: European Social Survey.
Data from 2011 ISSP health module and 2014 ESS.
Figure 1 visualizes country-year means of our main health lifestyle scales—universal health lifestyle and compensatory consumption—and SRH against logged GDP per capita. We observe a positive relationship between universal health lifestyles and logged GDP per capita, and to a lesser extent, compensatory consumption and logged GDP per capita. The correlation between mean health lifestyles and logged GDP per capita are 0.58 and 0.32, respectively. Mean universal health lifestyles and compensatory consumption differ by a maximum of 1.23 and 1.25 across countries, respectively, each of which is slightly larger than a standard deviation of the distribution of health lifestyle scales at the individual level. The right panels show average SRH across logged GDP per capita. Markers are weighted by the country-year specific correlation between the health outcome and universal health lifestyle. As found in previous research, we observe that higher logged GDP per capita levels tends to associate with higher self-rated health.
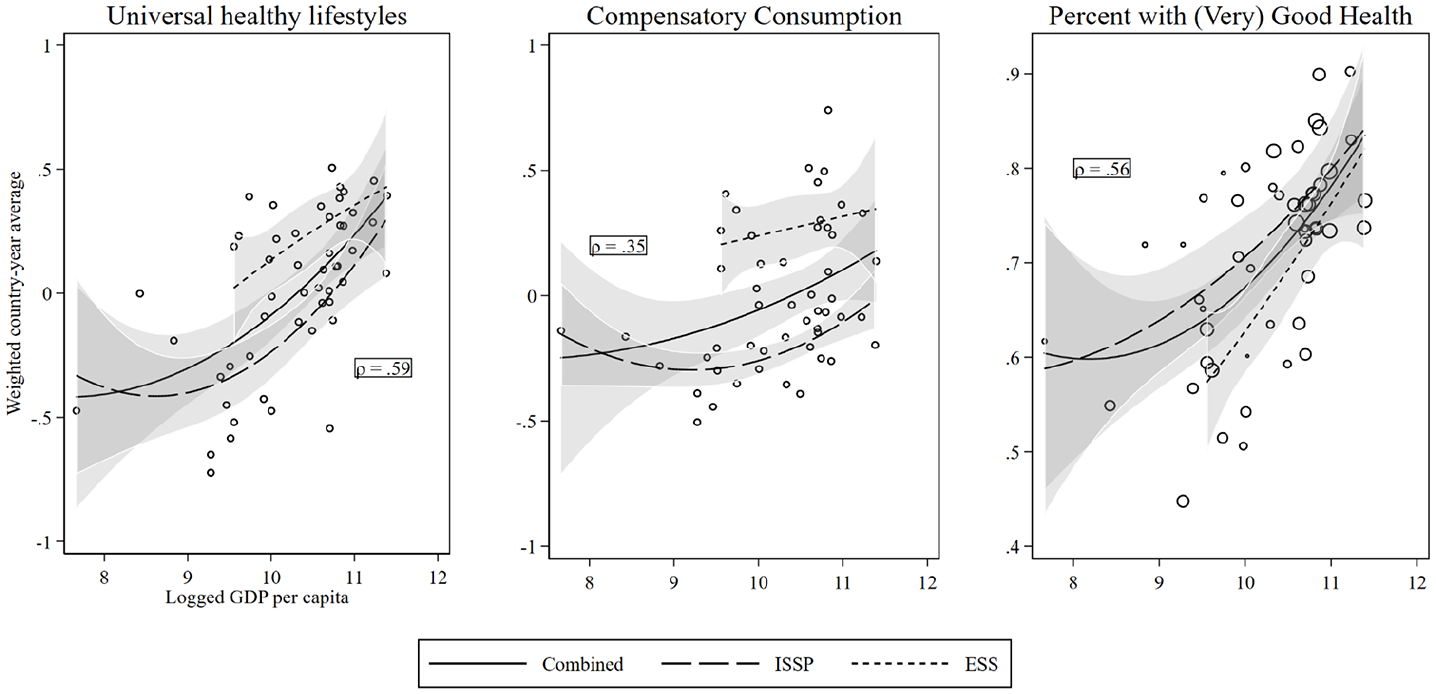
Weighted country means of health lifestyles and health outcomes against logged GDP per capita.
Results
Predicting health behavior
Our first hypothesis, that respondents in countries with higher logged GDP per capita participate in health promoting lifestyles more frequently than respondents in poorer countries, receives support. This finding is unsurprising and is included to verify that results from the ISSP and ESS reproduce findings from previous research. Table 2 shows results from multilevel linear regression models predicting the association between logged GDP per capita and health lifestyles. Models build from simple bivariate associations between health lifestyles and logged GDP per capita, adjusting first for individual-level variables and then country-level ones.
Mixed effects linear regression models of health lifestyle behaviors on logged GDP per capita.
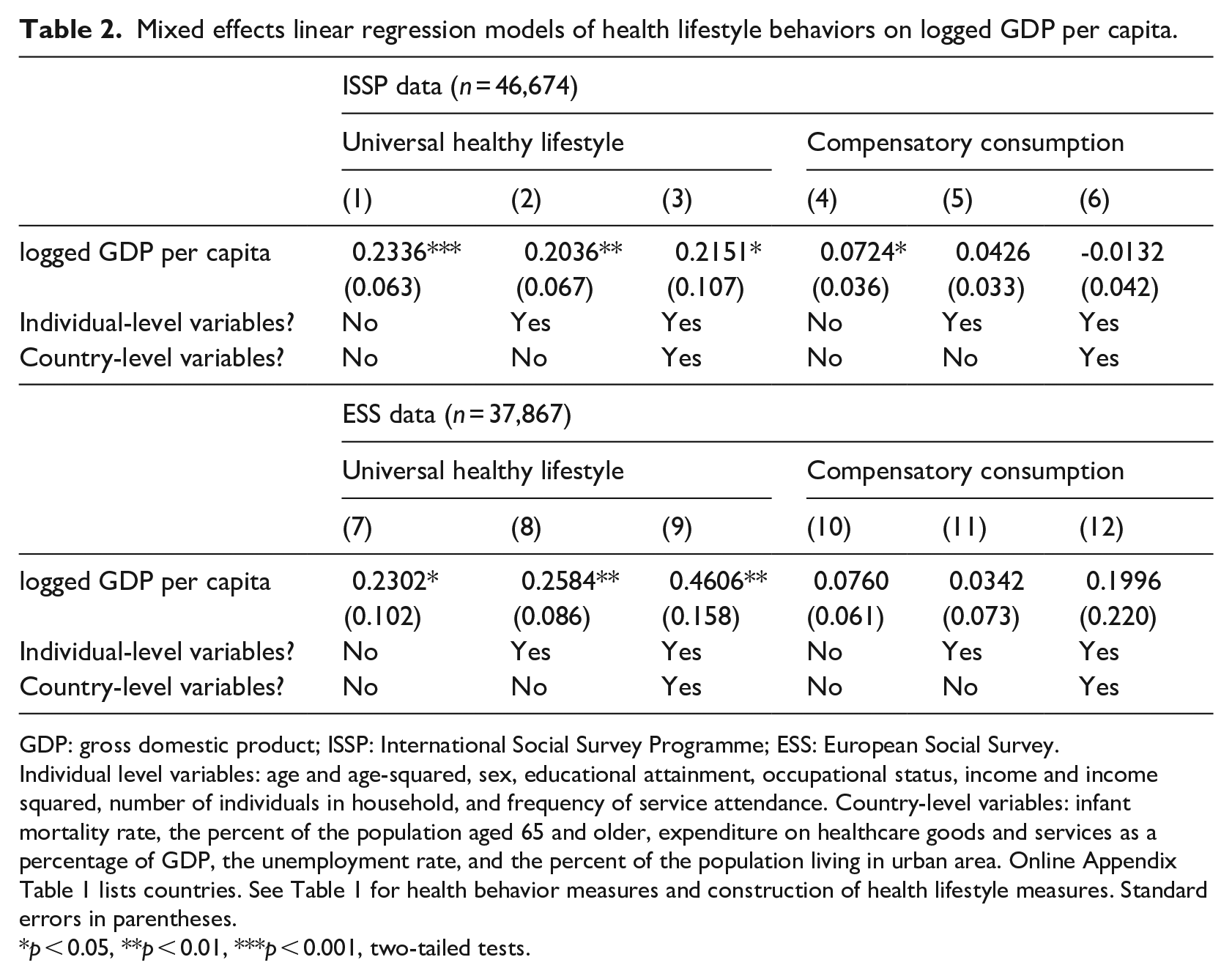
GDP: gross domestic product; ISSP: International Social Survey Programme; ESS: European Social Survey.
Individual level variables: age and age-squared, sex, educational attainment, occupational status, income and income squared, number of individuals in household, and frequency of service attendance. Country-level variables: infant mortality rate, the percent of the population aged 65 and older, expenditure on healthcare goods and services as a percentage of GDP, the unemployment rate, and the percent of the population living in urban area. Online Appendix Table 1 lists countries. See Table 1 for health behavior measures and construction of health lifestyle measures. Standard errors in parentheses.
p < 0.05, **p < 0.01, ***p < 0.001, two-tailed tests.
Looking across the models of Table 2, we draw two main conclusions. First, across all modeling specifications, we observe a positive and significant association between logged GDP per capita and universal healthy lifestyles. We assessed the magnitude of this positive association using results in Models 3 and 9, by comparing predicted values of universal health lifestyles between logged GDP values of 9.5 and 11.3, the common range in the two datasets. 11 This change associates with a 0.39 (ISSP) and 0.83 (ESS) increase in universal health lifestyles, or roughly a 35 and 75 percent standard deviation change in health lifestyles participation. 12 Second, across models and across datasets, we observe no meaningful association between compensatory consumption and logged GDP per capita. In total, results are suggestive that universal healthy lifestyle participation expands with country affluence, while compensatory consumption does not.
Predicting health outcomes
To test our second hypothesis—participation in health promoting lifestyles is uniformly associated with positive health outcomes across countries—we next examine how the two health lifestyle scales associate with SRH. To provide a descriptive understanding, we first estimate logistic regression models by country-years adjusting for individual-level variables. We then compute the discrete change in the predicted probability of positive SRH associated with a country-specific standard deviation increase in universal healthy lifestyles or compensatory consumption. Results are shown in Figure 2.
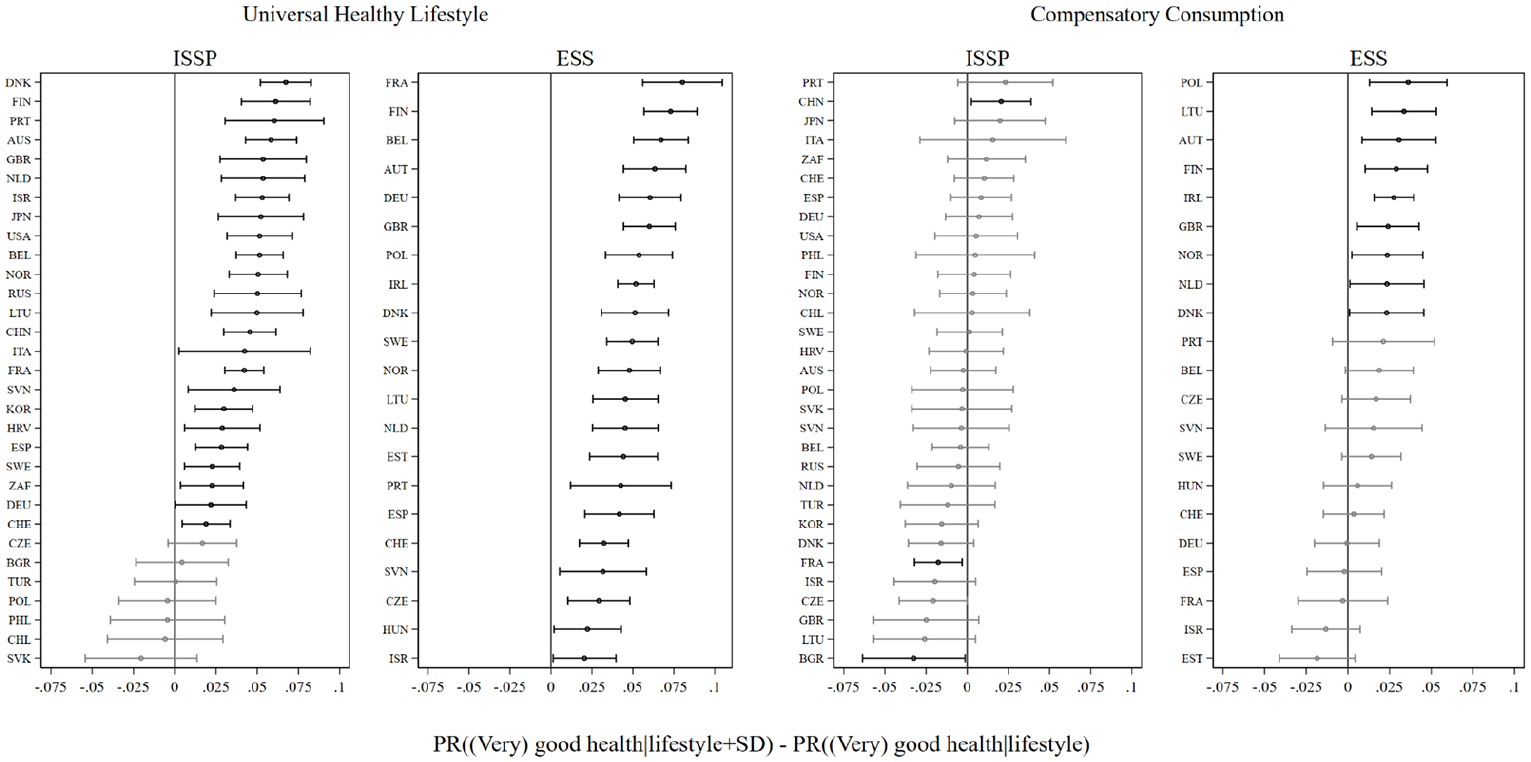
Difference in the predicted probability of (very) good self-rated health for universal and compensatory consumption health lifestyles.
The left panels of Figure 2 show results for universal health lifestyles. In 45 of the 52 country-years across the ISSP and ESS data, we observe a positive and significant change in the probability of high SRH associated with a standard deviation increase in universal healthy lifestyles. The significant changes in the predicted probabilities range between 0.02 and 0.08. Given that a standard deviation in the predicted probabilities of SRH in both samples are approximately 0.17, 13 the probability changes associated with universal healthy lifestyles are relatively large.
In contrast, we observe few significant associations between compensatory consumption and SRH. In the ISSP, we observe a significant positive association in China and a significant negative association in France. In the ESS data, 9 of the 21 countries have significant and positive associations, with magnitudes between 0.025 and 0.04. Overall, whereas results clearly highlight a relationship between SRH and universal health lifestyles, we find no clear patterns between compensatory consumption and SRH.
Notably, we observe larger changes in probabilities associated specifically with universal health lifestyles among countries with higher logged GDP per capita (ρ = 0.51), providing preliminary evidence that universal health lifestyles have larger relative associations with health outcomes among countries with higher economic development. We formally model this relationship to test our third hypothesis.
We estimate multilevel logistic regression models predicting SRH. Models in Table 3 include random coefficients for health lifestyle scales and cross-level interactions between health lifestyles and logged GDP per capita.
Mixed effects regression models of self-rated health on health lifestyle measures, logged GDP per capita, and country- and individual-level variables.
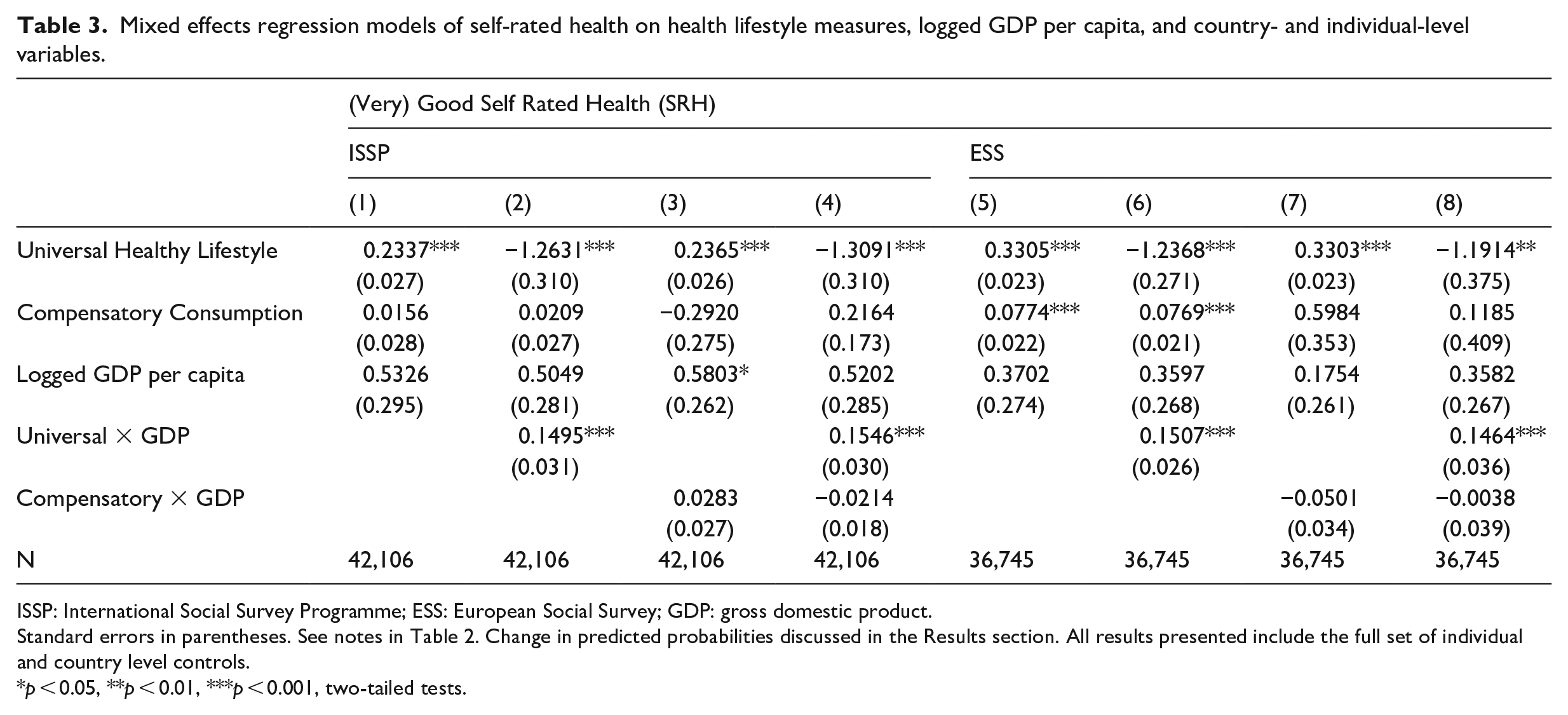
ISSP: International Social Survey Programme; ESS: European Social Survey; GDP: gross domestic product.
Standard errors in parentheses. See notes in Table 2. Change in predicted probabilities discussed in the Results section. All results presented include the full set of individual and country level controls.
p < 0.05, **p < 0.01, ***p < 0.001, two-tailed tests.
Across models and datasets, we observe similar patterns as those displayed in Figure 3. Universal heathy lifestyles have larger associations with SRH in affluent countries. In support of our third hypothesis, we uniformly observe a significant and positive interaction between universal healthy lifestyles and logged GDP per capita. To substantively interpret results, we computed the discrete change in the probabilities of SRH associated with a standard deviation increase in universal healthy lifestyles at logged GDP per capita values corresponding to those in Norway (11.3) and Poland (9.5). 14 An increase in universal healthy lifestyle participation is associated with an increase of 0.027 in the probability of SRH in a country with lower economic development (0.705–0.678 = 0.027, p < 0.001) and 0.048 in a country with higher economic development (0.863–0.814 = 0.048, p < 0.001). Notably, the second difference, or the difference in these discrete changes, is statistically significant at conventional levels.

Probability change in self-rated health, universal health lifestyle and logged GDP per capita.
Results thus far demonstrate how health lifestyles contribute to unequal health outcomes across countries. Individuals in more affluent countries tend to participate in universal heathy lifestyles more frequently, which, because these health lifestyles tend to associate with positive SRH, are more tightly coupled with health outcomes. Moreover, confirming Cockerham’s (2013) assertation of the importance of living conditions for the relative magnitude of health lifestyle participation, participation in universal healthy lifestyles has greater consequence for health outcomes in countries with higher levels of economic development. These findings suggest that the broadly shared context of economic development both expands access to participate in more health positive health lifestyles and increases the benefits of such lifestyles.
Change in health outcomes and behaviors
To further scrutinize our first and third hypotheses, that change in development increases both the healthy health lifestyle participation and the magnitude of the effect of health lifestyle participation on health lifestyles, we analyze combined ISSP and ESS data. The repeated samples of these data provide a unique opportunity to address the extent to which associations between economic development, health lifestyles, and health outcomes are robust to time invariant unobserved heterogeneity, such as country-level institutional, cultural, and historical characteristics. In the following results, we restrict our sample to the 17 European countries with samples in both the ESS and ISSP. 15
Table 4 shows results from three-level linear regression models predicting health lifestyles using logged GDP per capita, sequentially adjusting for individual- and country-level variables. All models include a variable indicating ISSP or ESS survey, while country fixed effects are included in Models 2 through 4. We thus assess the association between health lifestyles and health outcomes associated with within-country change in economic development. We observe a consistent finding in models predicting universal health lifestyles: within-country logged GDP per capita change positively associates with higher values of universal health lifestyle participation. Thus, the associations found in Table 2 hold not only between countries, but also within-countries as well (Models 2–4). In contrast, associations between compensatory consumption and logged GDP per capita are inconsistent across modeling decisions. Although we observe positive and significant associations in Models 2 and 3, the significant association is removed when adjusting for other country-level variables. 16 These findings provide further confidence in our first hypothesis, as they are suggestive that the positive association between universal health lifestyles and country-level economic development can be observed in within-country changes, not only between-country differences.
Change in logged GDP per capita against change in health lifestyles.
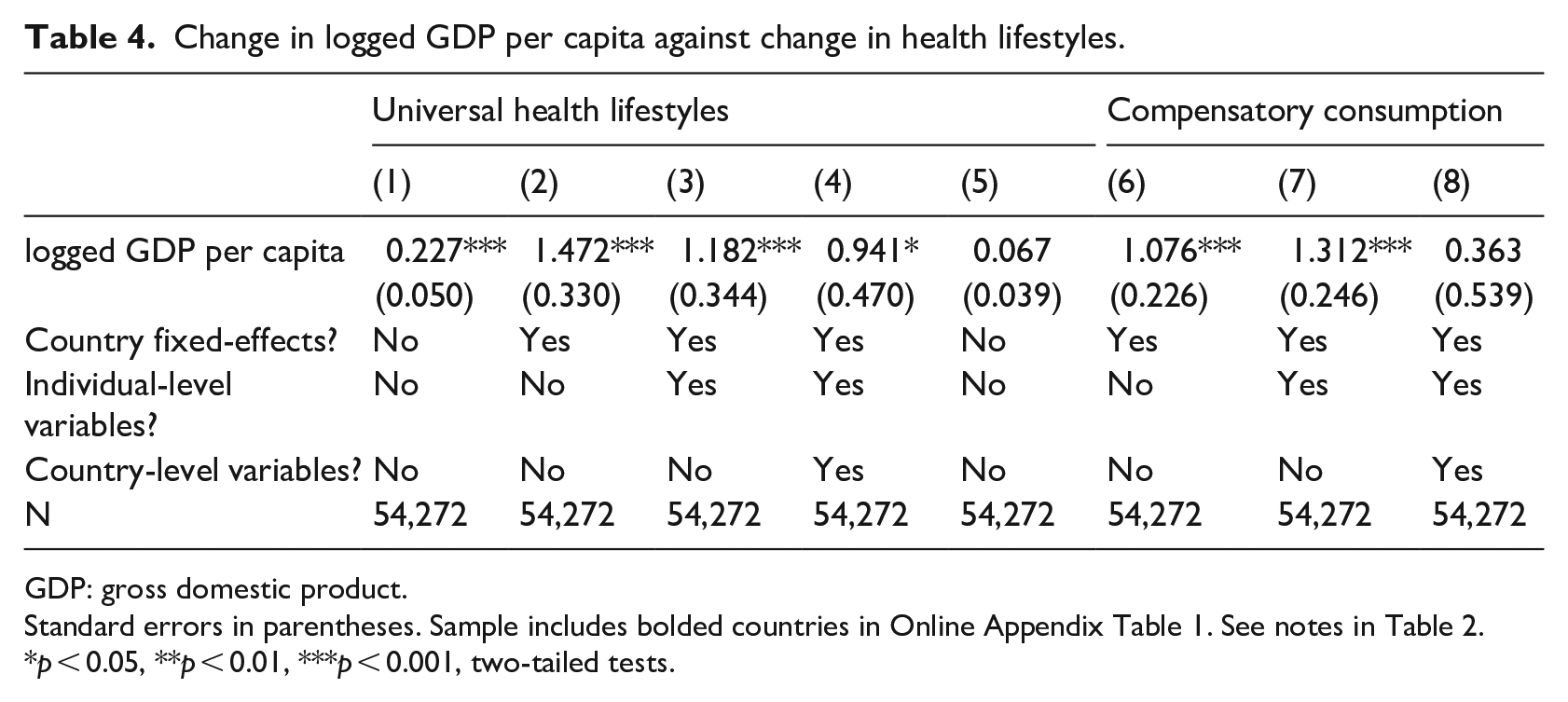
GDP: gross domestic product.
Standard errors in parentheses. Sample includes bolded countries in Online Appendix Table 1. See notes in Table 2.
p < 0.05, **p < 0.01, ***p < 0.001, two-tailed tests.
How do these findings translate to our third hypothesis? We replicate the logic of Table 4, assessing a cross-level interaction between logged GDP per capita and universal health lifestyle, focusing specifically on universal health lifestyles and within-country logged GDP per capita change. For these results, two methodological adjustments are needed. First, Giesselmann and Schmidt-Catran (2019) demonstrate the risk of biased results when modeling a cross-level interaction including a variable measuring within-country change. We therefore follow their suggestions by adjusting multiple potential cross-level associations between health lifestyle and logged GDP per capita to more directly detect our cross-level interaction of interest. 17 Second, caution is needed when interpreting interactions of nonlinear models, as regression coefficients might not accurately represent changes in the distribution of the more appropriate metric of the predicted probabilities (Doan et al., 2015). We therefore present discrete changes in probabilities associated with standard deviation increase in universal health lifestyles across logged GDP per capita. Figure 3 shows results. 18
A standard deviation increase in universal health lifestyles tends to result in larger magnitudes in the change of the probability of positive SRH among higher values of logged GDP per capita, to a point. For country-years with values of logged GDP per capita below about 10.2 (Czech Republic, Lithuania, Poland, Portugal, Slovenia), a standard deviation increase in universal health lifestyles results in an insignificant change in the probability of SRH. From logged GDP per capita values of about 10.3 to about 11.1 (Spain, Israel, Great Britain, France, Germany, Belgium, Finland, the Netherlands, Sweden, and Denmark), higher values of logged GDP associate with larger changes in the probability of (very) good health, with the magnitude of a standard deviation change increasing from about 0.035 to 0.06. At logged GDP per capita values corresponding to the two most affluent countries (Switzerland and Norway), an increase in universal health lifestyles participation is again statistically insignificant. These results could reflect the ceiling effect of economic development on health noted by Olsen and Dahl (2007), should they prove to be repeated in additional cross-national surveys when data are available. Overall, the above results provide two extensions of hypotheses two and three. First, results suggest that associations between health lifestyles and economic development might occur within countries, as well as between them. Second, increase in economic development may, up to a point, increase the magnitude of the association between health lifestyles and SRH. In total, we conclude that a robust association between country-level economic development and health lifestyles exist in our sample of 52 country-years, one that cannot be easily reducible to unobserved time-invariant differences across countries.
Discussion
In this article, we examined how health lifestyles, and their subsequent influence on health outcomes, vary across countries based on between-country inequalities of economic development. To do so, we harmonized data from the 2011 wave of the ISSP and 2014 ESS program, constructed two dimensions of health lifestyles based on four health behavior measures, and examined how these health lifestyles, as well as self-rated health, vary across countries along economic development.
We draw three main conclusions from results. First, we observe that individuals in countries with higher GDP per capita tend to engage in universal health lifestyles—eating fresh fruits and vegetables, exercising, and refraining from smoking and heavy drinking—more frequently than those in less affluent countries. Our second health lifestyle dimension, compensatory consumption, associates with country-level development more sporadically.
These results suggest that engagement in particular health lifestyles is partially dependent upon a country-level economic context that provides access and availability for engaging in health behaviors. We argue that as nations grow in economic development, residents gain access and opportunities to participate in health positive health lifestyles. We are not aware of health lifestyles research making this point. However, our results highlight the importance of situating health lifestyles research in a particular national context at a particular point in its development trajectory.
Second, we find that the positive effects of health lifestyles have a tighter association with health outcomes in higher income countries. Across both datasets, and for self-rated health, we find higher probability changes in higher income countries compared to lower ones. Thus, differences in health outcomes, as they relate both to between-country inequalities and to health lifestyles, are due to two complementary factors: more frequent participation in health lifestyles, and a greater payoff for greater involvement in health lifestyles.
Simply put, two otherwise similar individuals in our sample who engage in all positive health behaviors can expect different predictive values for health outcomes depending on the inequalities that exist between countries in terms of economic development. We argue that a country’s system of economic development provides access and availability for the participation in health lifestyles that facilitates in making such health behaviors more or less effective. This medical sociological theory of health and health outcomes illustrate how individual agency in health behavior participation is enabled by broadly shared macrolevel conditions.
Results from this article provide clear conceptual innovations for comparative and cross-national sociological research. Health lifestyles theory provides a coherent and mature line of research to incorporate into comparative and global studies of health. Our focus on the Weberian concept of living conditions highlights how macrolevel characteristics can be used to assess heterogeneity in health behaviors as well as heterogeneity in the association between health behaviors and health outcomes.
Of course, we are limited by the observational nature of our data and so cannot precisely estimate the causal ordering of health outcomes and health behaviors: surely an improvement in a person’s health holds the capacity for them to behave in a more health promoting way. We partially address this concern by replicating all results while including information on whether a respondent has a chronic condition and their BMI status. Presumably, these conditions should precede the more immediate health behavior information provided on the surveys. Nevertheless, we cannot wholly rule out the potential of reverse causality. Future research on this topic is needed.
Third, we extend understanding of health lifestyles research by showing that change in country level development is positively associated with change in country average health lifestyles. We exploit the similar health behavior questions in the ISSP and the ESS to allow for a country level analysis of change. To our knowledge, no study demonstrates what motivates change in health lifestyles over time. We argue that growth in country-level economic development allows for greater access and availability of a healthy lifestyle. This expectation is supported and cannot be explained fully by unobservable time invariant differences between countries.
These findings provide theoretical innovation for health lifestyles theory. Scholars repeatedly call for greater attention to be paid to this aspect of health lifestyles theory (Cockerham, 2005, 2013), but research on the importance of living conditions remains scarce. To our knowledge, no previous research tests the ordering of living conditions and health lifestyles. We demonstrate that growth of country level development, which we conceptualize as a macrolevel living conditions, cooccurs with a population-level increase in both of our health lifestyles measures. These findings present more rigorous evidence than currently exists showing the importance of living conditions for influencing health lifestyle participation.
This study provides two innovations to the study of health lifestyles. First, this is the most extensive study of the combination of multiple health behaviors in a cross-national study. Medical sociologists are increasingly turning to cross-national variation to understand the importance of social context for health outcomes (e.g. Beckfield et al., 2013; Präg et al., 2016). We similarly demonstrate how health lifestyle participation, and its subsequent influence on health outcomes, depend on national context. Second, we provide the most robust evidence to date on the importance of a shared national living condition for health lifestyle participation. Living conditions receive relatively little attention in studies of health lifestyles. Our study shows the importance of this component of the theory and demonstrates methods to extend its implementation to the cross-national case.
Our study has several important limitations. We highlight five. First, our harmonization of the ISSP and the ESS necessarily involves choices and decisions in an attempt to make the data comparable, creating a risk that we made suboptimal decisions, or that inherently incompatible data are treated as compatible. Unfortunately, these are the only data available that provide similar health lifestyle and health outcome behaviors from high quality data sources repeated across countries. Results from the current study highlight the benefits that will be gained from the release of additional health modules in both the ISSP and ESS.
Second, we only focus on four health behaviors. Other studies of health lifestyles focus on a much richer variety of health positive and negative behaviors, such as meat or junk food consumption (Mollborn and Lawrence, 2018). Our scale construction, and analyses of cross-national variation of more contradictory combinations of health behaviors, would undoubtedly be improved with additional health behavior information. This is a necessary tradeoff, as we chose to extend this smaller number of health lifestyle measures to a larger number of country contexts than were included in previous research.
Third, the countries in our sample do not include those with the lowest levels of economic development. While we included as much country level variation as was available in the data, and while our study represents a substantial expansion of countries included in cross-national studies of health lifestyles, our study cannot generalize to those regions and countries where many of the world’s poor reside. We suspect that much is to be learned by examining variation of the link between health lifestyles, health outcomes, and development among developing nations.
Fourth, we focused on a relatively short time frame to measure changes in economic growth. On the one hand, such a focus brings with it many strengths. We do not need to be concerned that results are biased by such factors as intergenerational changes in culture and value systems, major changes to healthcare implementation, or demographic transitions. On the other, we cannot precisely discern whether health lifestyles change in response to long-run development factors or short-run economic shocks. Future research incorporating additional waves of cross-national data, when available, would be useful.
Fifth, we suspect that the influence of economic development interacts with the levels of economic inequality in a country. Cross-national scholars of health have demonstrated the central importance of inequality for health outcomes (e.g. Sosnaud and Beckfield, 2017). We suspect that inequality should be consequential insofar that it concentrates the benefits of economic development among higher income residents. In that case, we would expect the association of overall economic growth to be partially accounted for by unequal changes across individuals along the earnings distribution in more economically unequal countries. That is, the effect of growth may be more concentrated among higher income earners in more unequal countries. Given that economic inequality is a contributor to negative health outcomes (e.g. Beckfield et al., 2013), it is worthwhile to investigate its contribution to health lifestyles. A full assessment of country-level inequality’s influence on health lifestyles is beyond the scope of the current study, yet we acknowledge that its omission from the current study represents a significant limitation. Future research examining more complex and stratified associations across country-level income inequality and individual-level income is needed and would help specify when, and how, macrolevel context translates into an individual’s living conditions.
Similarly, the overall influence of economic growth may be differentially channeled into local and regional infrastructure that may motivate changes to health behavior: grocery store openings, bike lane constructions, local policy incentive for positive health, and so on. Such locally channeled development may result in greater within-country differences of health behavior outcomes. Unfortunately, we are not aware of any high quality cross-national data on regional health infrastructure development that can be harmonized with our data. Yet, research on this topic would help specify the mechanisms linking overall economic development and health behaviors.
In total, we demonstrate the utility of connecting health lifestyles research with cross-national studies of development and health. Between-country inequalities in economic development influence population’s participation in particular health lifestyles. Similarly, country affluence influences the relative payoff of such health lifestyle participation. Thus, the connection between country-level living conditions and health lifestyles are critical for understanding cross-national variation in health outcomes.
Supplemental Material
sj-docx-1-cos-10.1177_00207152211041385 – Supplemental material for Between-country inequalities in health lifestyles
Supplemental material, sj-docx-1-cos-10.1177_00207152211041385 for Between-country inequalities in health lifestyles by Tom VanHeuvelen and Jane S VanHeuvelen in International Journal of Comparative Sociology
Footnotes
Acknowledgements
The authors thank Shawn Bauldry, Matthew Grace, and Shiri Noy for their thoughtful feedback.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.