
Abstract
In health care policy debates, discussion centers around the often-misperceived costs of providing medical care to immigrants. This review seeks to compare health care expenditures of U.S. immigrants to those of U.S.-born individuals and evaluate the role which immigrants play in the rising cost of health care. We systematically examined all post-2000, peer-reviewed studies in PubMed related to health care expenditures by immigrants written in English in the United States. The reviewers extracted data independently using a standardized approach. Immigrants’ overall expenditures were one-half to two-thirds those of U.S.-born individuals, across all assessed age groups, regardless of immigration status. Per capita expenditures from private and public insurance sources were lower for immigrants, particularly expenditures for undocumented immigrants. Immigrant individuals made larger out-of-pocket health care payments compared to U.S.-born individuals. Overall, immigrants almost certainly paid more toward medical expenses than they withdrew, providing a low-risk pool that subsidized the public and private health insurance markets. We conclude that insurance and medical care should be made more available to immigrants rather than less so.
Keywords
A common misperception among U.S. policymakers and the general public is that immigrants use more health care assets than those born in the United States, thereby draining our country’s medical resources 1 Certain advocacy groups have argued that providing health care to immigrants costs state and federal governments billions of dollars annually and that public funding for these expenses is unsustainable. 2 The majority of Americans hold similar opinions: slightly over half of all Americans (52%) currently believe that immigrants burden our country with excessive health care costs. 3 Two-thirds (67%) of the public believe that undocumented immigrants should not be eligible for social services provided by state and local governments. 3
Federal policies have limited the degree to which immigrants, particularly the undocumented, can access publicly funded medical care and insurance, based on the premise that their tax payments are insufficient to justify access. In 1996, the Personal Responsibility and Work Opportunity Reconciliation Act (PRWORA) barred legal immigrants from obtaining nonemergency Medicaid. 4 The 2010 Affordable Care Act (ACA) denied legal immigrants access to its health insurance plans until they had completed 5 years of lawful residency and denied undocumented immigrants access to plans, although it otherwise increased health insurance coverage to many low- and moderate-income individuals. 5 These restrictions and denials have produced substantial negative health consequences for immigrant populations in the United States. We consider the development of a comprehensive understanding of what is known about health care spending on and by immigrants to be important.
An increasing number of recent studies have investigated health care spending among immigrants. Yet, no prior studies have comprehensively reviewed this literature to evaluate health care expenditures among immigrant groups and compare health care expenditures between immigrants and nonimmigrants in the United States.
Methods
Our team systematically examined 188 peer-reviewed studies related to health care expenditures on and by immigrants in the United States.
Data Sources and Search Strategy
In 2016 and 2017, we searched PubMed using Medical Subject Headings (MeSH) designed to capture 2 main concepts: immigrants and health care expenditures (“emigration and immigration” [MeSH] OR “emigrants and immigrants” [MeSH] OR “transients and migrants” [MeSH]) AND (“health expenditures” [MeSH] OR “healthcare costs” [MeSH]). We limited our search to articles written in English that were published in the year 2000 or later. This strategy identified 188 articles.
Article Selection
We conducted a 3-stage screening process starting with a title review, followed by an abstract review, and ending with a full-text article review (Figure 1). Articles were included if they provided original data on health care expenditures for and/or by immigrants in the United States. Editorials and opinion pieces were excluded.

Flow diagram of selection process.
In our title review stage, authors independently reviewed the article titles to determine their relevancy. Articles that contained data from the year 2000 or later were included. The title review yielded a total of 40 relevant articles and excluded 148 articles. Through discussion and consensus, we reviewed the abstracts for eligibility and selected 18 papers for a full reading, excluding 22 papers. We ultimately identified 16 articles for inclusion that are summarized in Table 1.
Demographics.

Data Abstraction
The reviewers developed a data abstraction form and independently applied it to 3 articles. After a review of their findings, they finalized the data abstraction tool. Two authors (LZ, LF) abstracted the information from the articles, and 2 other authors (DM, JWB) then reviewed the abstracted information for accuracy and completion. We resolved discrepancies by consensus. Once the data abstraction was completed and reviewed, the authors developed themes and recommendations.
Results
Several articles focused on immigrants with particular legal status (e.g., undocumented immigrants),6–8 with particular conditions,9,10,11 particular ages,12,13 in particular settings (e.g., emergency departments 15 ), or with particular ethnicities (e.g., Latinos 16 ), while others focused on immigrant expenditures in general compared to U.S.-born groups.6,13,17–20 Most articles assessed data from the Medical Expenditure Panel Survey (MEPS).6,13,17 Two articles focused on the dollar amounts immigrants contributed to Medicare’s trust fund versus what they withdrew.8,19 Table 2 contains a full summary of results.
Expenditures by Immigrant Groups.

Expenditures in General
According to 1998 MEPS data, per capita total health care expenditures were lower for immigrants compared to U.S.-born individuals ($1,139 vs $2,546) for all age groups assessed. 13 Overall immigrants’ expenditures are one-half to two-thirds of U.S.-born individuals.13,17 In 2003, recent immigrants (living in the United States less than 10 years) spent $1,380 annually, whereas U.S.-born individuals spent $3,156 over that same year. 17
As a group, immigrants consume a disproportionately small percentage of health care costs compared to the U.S.-born population.13,17,20 Immigrants account for 12% of the population but only account for 8.6% of total U.S. health care expenditures.7,18 U.S.-born individuals account for 90% of the population but 93% of expenditures. 18 Nationally, from 2000 to 2009, immigrants accounted for $96.5 billion of health care spending annually compared with $1 trillion spent by the U.S. born. 7 Undocumented immigrants account for 1.4% of total medical expenditures in the United States, although they make up 5% of the population. 7 After 2003, U.S.- and foreign-born citizens’ expenditures were relatively proportional to their population sizes; by comparison, expenditures for undocumented immigrants were 50% to 60% less per capita. 6 In Los Angeles, immigrants are 12% of the population but only account for 6% of expenditures. 19
Expenditures Over Time
Three studies examined medical expenditures over time.6,15 Between 2000 and 2008, there was an overall increase in expenditures, but with a steeper increase for U.S.-born individuals. 6 Likewise, between 1999 and 2006, expenditures increased for all groups (undocumented, naturalized, and U.S. born); however spending for the U.S. born increased by twice the amount as spending for the undocumented ($1,000 vs $500). 18 In North Carolina between 2001 and 2004, emergency Medicaid spending on undocumented immigrants increased, primarily on labor and delivery costs as well as treatment for acute medical conditions, because of an increase in the number of undocumented immigrants covered by the program. 15 After age 65, the spending difference between immigrants and U.S.-born individuals decreased as individuals of both groups who paid into Medicare for at least 40 quarters gained access to it. 14 Among Latino immigrants, all subgroups (undocumented, naturalized, and US born) had lower expenditures than non-Latino white U.S. citizens That difference diminished when Latinos had been naturalized citizens for over 10 years. 16
Medical Expenditures by Citizenship Status
Immigrants, regardless of their legal status, had lower expenditures than their U.S.-born counterparts. Forty-seven percent of immigrants were citizens, and 53% were noncitizens. 18 Undocumented immigrants spent 40%–50% less than U.S.-born individuals.6,14,18 Based on data from 2000 to 2008, undocumented immigrants spent an average of $1,836 compared with $3,737 spent by foreign-born citizens and $4,478 spent by U.S.-born citizens. 6 Another study found that from 2001 to 2005, spending increased by all groups, but differences in per capita spending increased by over 30% between foreign-born noncitizens and U.S.-born citizens. 17 Spending by noncitizens went up by $500 after 1999, whereas spending by citizens went up by $1,000. 18 From 2000 to 2009, noncitizens spent $500 annually on health care, whereas citizens spent 5 times that amount on health care. 7
Expenditures by Source of Payment
Latino immigrants were 20% less likely to have health insurance than their non-Latino white U.S.-born counterparts. 16 Even when immigrants were insured, they had lower health care expenditures. Forty-four percent of immigrants who lived in the United States for less than 10 years and 63% of immigrants who lived in the United States longer than 10 years had health insurance during the 1-year period evaluated (see Table 3). 17 Expenditures of insured immigrants were 52% lower than those of insured U.S.-born individuals. Expenditures for uninsured immigrants were 61% lower compared to uninsured U.S.-born individuals. 13 When noncitizens were fully insured for a year, recent immigrants spent half as much as U.S.-born persons, while established immigrants – those in the United States for longer than 10 years – spent two-thirds that of U.S.-born individuals. 17 Per capita expenditures from private insurers for immigrants were lower than payments for citizens,7,17,20 although some studies failed to find significant differences 12 or did not comment on the significance.6,7,20 This indicated that immigrants may constitute a low-risk pool that subsidizes the insurance market for U.S.-born individuals. 17 Immigrants had significantly lower incidence of nonfatal occupational injuries than U.S.-born workers (560 occupational injury events vs 2,176). 10 However, even though immigrants sought medical care to the same degree as U.S. born individuals, workers’ compensation expenditures were smaller for immigrant workers compared to U.S.-born workers (workers’ compensation paid 57% of medical expenditures for U.S. born workers versus 43% for immigrant workers). 10
Expenditures by Source of Payment.
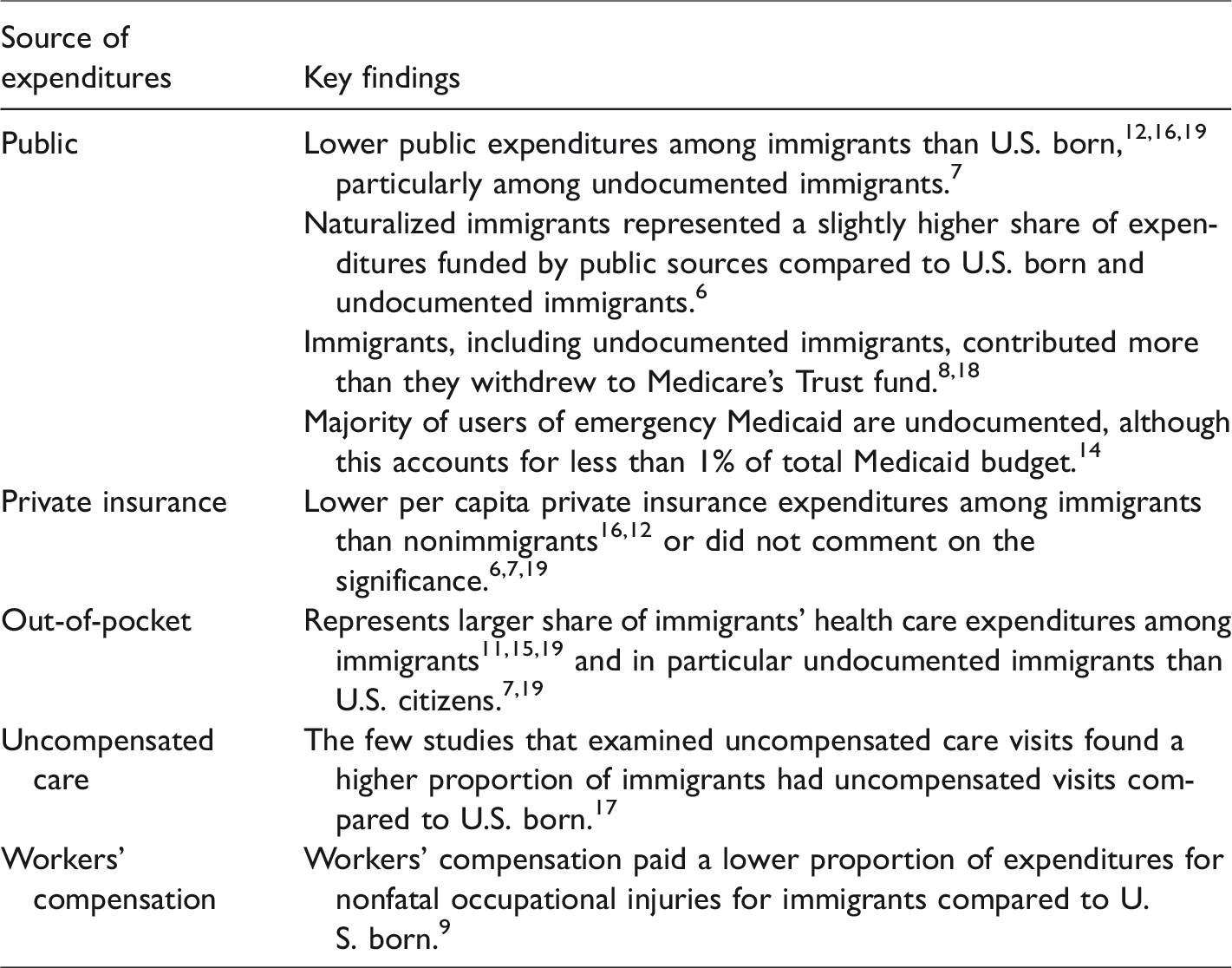
Per capita public expenditures were lower for immigrants overall,13,19 particularly for the undocumented. One reason may be that it is more difficult for immigrants to get coverage through public health programs than it is for U.S. citizens. During the 6 years studied, undocumented immigrants had median public per capita expenditures of $200 or less, whereas U.S.-born citizens had median expenditures closer to $1,100 annually. 18 From 2000 to 2009, 8% of undocumented immigrants received public sector coverage, whereas 30% of U.S.-born individuals received public sector coverage. 7 The 8% of undocumented immigrants with public sector coverage recieved an average of $140 per person per year compared to $1,385 per person annually for U.S.-born citizens. For undocumented immigrants, public expenditures represented one-eighth of total expenditures as compared to one-third for U.S. citizens. 7 In Los Angeles county, even though immigrants had disproportionately lower incomes than U.S. citizens, only 16% of medical costs for immigrants were paid through public sources compared to 21% for U.S. citizens. 20 Of note, Tarraf (2012) found that, from 2000 to 2008, foreign-born citizens had the highest use of public sources compared to both undocumented immigrants and U.S.-born citizens, with an especially sharp increase in 2007.6,12,16
Undocumented immigrants, particularly those both elderly and recently arrived, paid a large share of the out-of-pocket (OOP) expenditures made by all immigrants.6,12,16 This is due partly to lower use of public funds and lower rates of private insurance. In Los Angeles County, 27% of medical expenditures for immigrants were OOP expenses, compared to 20% for U.S. born. 19 From 2000 to 2008, the proportion of OOP expenditures was similar for foreign-born and U.S.-born citizens but higher for noncitizens. 6 From 2000 to 2007, Latino individuals consistently had OOP expenditures that were approximately 6% higher than their non-Latino white counterparts. 16 OOP expenditures were even higher for naturalized Latinos (42%), and undocumented immigrants (51%) than for non-Latino whites. 16 Choi studied financial burden, measured as the percentage of personal income spent on OOP medical payments. Recent immigrants over the age of 65 spent less OOP than their U.S. counterparts ($808 vs $1,571), although the financial burden was greater for recent immigrants (33% vs 12% of their income). 12 Low-income recent immigrants were 4 times more likely to spend 50% of their income on OOP payments than other groups. 12
Some studies examined use of uncompensated care by immigrants compared to other groups.7,18 Approximately 13% of undocumented immigrants had at least 1 uncompensated visit in a year, versus 11% of U.S.-born citizens; foreign-born citizens and U.S.-born citizens had similar rates of uncompensated care use. 18 Another study found that undocumented immigrants were twice as likely as U.S.-born citizens to use uncompensated care. 7 One study aimed to estimate the impact of the Personal Responsibility and Work Opportunity Reconciliation Act of 1996 (PRWORA) on hospital expenditures for uncompensated care, as PRWORA gave states the option to withdraw Medicaid coverage for nonemergency care from most legal immigrants. Curtis and colleagues (2003) found a 1% increase in the log of state’s immigrant population led to a 2.2% increase in uncompensated care that was nonsignificant. Apparently the decision to implement PRWORA and the number of immigrants in that state had no significant impact on the hospital expenditures for uncompensated care.
Two studies demonstrated that immigrants made high health care contributions in relation to expenses.8,19 Although this is not surprising, given that many undocumented immigrants contribute to the Medicare Health Insurance Trust Fund but do not receive benefits, it goes against the common misconception that immigrants are responsible for the high cost of health care in this country. From 2002 to 2009, immigrants paid more to the trust fund than they withdrew, generating a yearly surplus of $11–$17 billion. 19 From 2000 to 2011, undocumented immigrants contributed $2–$3 billion more to the trust fund than they withdrew, thereby extending the life of the fund. 8 The data suggests that immigrants’ payments similarly subsidize private insurance companies. 17
Expenditures by Age Group
The expenditures of immigrants compared to U.S.-born individuals varied according to age groups. Total health expenditures were lower for immigrants of all age groups compared to U.S. born, though there was not a statistically significant difference between the immigrants and U.S. born over age 65. 13 Immigrant children (below age 12) had medical expenditures that were 49% lower than U.S. children, and immigrant adolescents (ages 12–17) had expenditures 76% lower than U.S.-born adolescents. Immigrants between ages 55 and 64 spent $3,314 less on health care than U.S.-born counterparts, but after age 65 the differences in total spending disappeared, in part because after age 65, substantial numbers of immigrants qualify for Medicare. 14
Discussion
Many Americans, including some in the health care sector, mistakenly believe that immigrants are a financial drain on the U.S. health care system, costing society disproportionately more than the U.S.-born population, i.e., themselves. Our review of the literature overwhelmingly showed that immigrants spend less on health care, including publicly funded health care, compared to their U.S.-born counterparts.6,7,13,14,16–18,20 Moreover, immigrants contributed more towards Medicare than they withdrew; they are net contributors to Medicare’s trust fund.8,19
Our research categorized immigrants into different groups, but in all categories, these studies found that immigrants accrued fewer health care expenditures than U.S.-born individuals. Among the different payment sources – public, private, or out-of-pocket – public and private expenditures were lower for immigrants,7,13,17,20 with immigrants spending more out-of-pocket.12,20 Differences decreased the longer immigrants resided in the United States.14,16
While annual U.S. medical spending in 2016 was a staggering $3.3 trillion, 23 immigrants accounted for less than 10% of the overall spending – and recent immigrants were responsible for only 1% of total spending. 20 Given these figures, it is unlikely that restrictions on immigration into the United States would result in a meaningful decrease in health care spending. To the contrary, restricting immigration would financially destabilize some parts of the health care economy, as suggested by Zallman and colleagues, who found that immigrants contributed $14 billion more to the Medicare trust fund than they withdrew. 18
Apart from various barriers to access, part of the disparity in health care spending may be due to a “healthy immigrant effect,” meaning that recent immigrants tend to be young and robust when they arrive.16,24 On average, immigrants are younger and healthier than nonimmigrants and need less medical care. Still, the lack of insurance coverage and restricted access to care must be considered in a full accounting for the low amounts of spending on immigrants compared to nonimmigrants. Ku 17 found that less than half of recent immigrants are insured, partly because even documented immigrants are banned from getting government-sponsored health insurance for the first 5 years after entering the country. The disparity in health care spending tended to decrease as people aged, and when immigrants reached the age of 65, differences in total spending disappeared between U.S.- and foreign-born people. The nearly universal access to Medicare is partly responsible; however, the immigrant spending increase may also exist because they were unable to access preventive care earlier in their lives. 14 Additionally, when immigrants first arrive in the United States, they are less familiar with the system and less likely to sign up for care. Thus, it is not surprising that the existing differences between foreign- and U.S.-born people tends to decrease the longer immigrants live in the United States, particularly as many are eventually granted citizenship. 16
Even though recent immigrants could be vigorous, young financial assets for the health care system, they are systematically excluded from it. In addition to the 5-year ban on participation in public insurance programs as noted above, immigrants often rely on safety-net options that are limited and overburdened. 25 Those who do not are often obliged to rely on emergency care or pay OOP for services. When they succeed in receiving care, the quality of the care can be limited by various forms of discrimination, language barriers, and fears of deportation. Researchers have raised the concern that when immigrants are spending approximately one-third of their total income on OOP medical payments, they cannot build a middle-class life. 12
Risk of discovery and deportation have become even larger obstacles to immigrants obtaining health care. Families who do not know what will happen if their children are deported or if one or both parents are forced to leave the country may be particularly fearful. 25 The children of immigrants are disproportionately underserved by the health care system because of barriers their parents face. 13 When immigrants are under emotional stress because of fear of deportation and financial stress because they do not receive benefits available to low-income Americans, immigrants have less chance to enter the middle class. If immigrants had additional support to enter the middle class, they would be able to buy homes, purchase cars, buy goods, and further drive the growth of the U.S. economy.
The 8 papers of our review, which found immigrants had far lower expenditures than U.S. citizens, made similar policy recommendations. Nonfinancial barriers to health care must be decreased so that healthy immigrants can stay healthy. Providing bilingual primary care, high-quality interpreter services, 17 and access to preventive services, such as treatment of infectious disease, 7 would reduce barriers. Mohanty 13 suggested ending the option for states to restrict health care coverage for immigrant children because they grow up to be a major part of the American workforce; Tarraf suggested that emergency Medicaid be expanded to cover preventive care and screening services. 6
Fiscal responsibility is an important reason for the United States to provide insurance for newly arrived immigrants, as they could continue to enlarge the low-risk pool of healthy individuals that helps offset the cost of insuring high-risk individuals. Currently, under the ACA, undocumented immigrants cannot enroll in the state health care exchanges. If we are seeking to minimize costs, which would seem a major factor in the reasoning of policymakers who would deny immigrants care, then it makes financial sense to enroll individuals who will (on average) contribute more to the health care system than they withdraw. Healthy, young immigrants are precisely whom we should target for Medicaid enrollment, state exchanges, or private health insurance.
Among the limitations of this study was the inability to accurately assess how much uncompensated care is being delivered to immigrants. We have limited data on expenditures for undocumented immigrants as well as insufficient estimates of possible monetary losses to hospitals and other institutions. Additionally, we have insufficient information about expenditures on immigrant children. We did not include studies on expenditures outside the United States nor capture the extent to which immigrants may travel outside of the United States to receive care.
Further research is indicated, including examining how closely health care expenditures are related to the ability to access care as well as possible impacts of the ACA on immigrants’ ability to access health insurance. As the ACA’s mandates are eroded by the current administration, assessing the changing effects on immigrants will also be necessary.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.