
Abstract
With the economic crisis in Spain, austerity measures were applied. However, it is unknown how these measures have affected the pattern of use of health services for the immigrant population. Thus, the objective of this study was to examine the inequalities in access to different levels of health care services according to place of birth. We used data from the 2014 Foreign Immigrant Population Survey (n = 1,908) and the Basque Health Survey 2013 for the native population (n = 4,232) for adults aged 16–59 years residing in the Basque Country, Spain. Log-binomial regression was used to quantify the association between country of origin and use of different levels of care in men and in women. We found a higher probability of using general practitioner (GP) services in immigrant women (PR: 1.19; 95% CI: 1.12–1.26) and men (PR: 1.11; 95% CI: 1.01–1.23) than in natives. This was also true for emergency services with immigrant women (PR: 1.97; 95% CI: 1.43–2.69) and men (PR: 1.50; 95% CI: 1.01–2.25). However, for specialized medicine services, there was no association. This study suggests the importance of guaranteeing access to health care to the entire population. Hence policies to eliminate barriers to health care are essential to ensure health for all.
During the last decades, the growth of the immigrant population from low-income countries has transformed the demographic and social milieu in Europe, with major challenges for access and use of health care services. 1 This transformation has generated a growing interest in the inequalities between native and immigrant populations in the use of health care services.2–8 Two recent reviews conducted in European countries show that, compared with the native population, immigrants use different levels of care for the same need, with greater, equal, or lower use for such levels of care.3,5 The characteristics of the immigrant population, the different models of health care systems, and the organization of services are named as relevant elements explaining the unequal access to the different levels of care for this population according to the country of birth.2,5
Spain is the fourth country in the European Union in terms of immigrant population (n = 6,123,769) and one with the highest proportions of immigrants relative to the total population (13.6% in 2017). 9 During the last decade, an increased level of universal health care has been achieved, with equal health care for the population, regardless of nationality or administrative status in Spain. 10 In fact, Spain is considered one of the countries with the most inclusive and equitable health care policies. However, the immigrant population faces barriers to accessing health care. 2 With the economic crisis, which began in 2008, the proportion of people in situations of social and economic vulnerability increased, specifically among the immigrant population, a segment of the population already worse off. 11 In addition, as a political response to the crisis, austerity measures were applied. The measures resulted in the reduction of public spending and limited access to health care services for the irregular immigrant population with the enforcement of the Royal Decree-Law 16/2012 (RDL 16/2012). These measures, although applied unequally due to the decentralization of the health care system in the 17 autonomous communities, produced changes in the health care model 12 and increased the barriers to access health care services.13–15 However, it is unknown how these measures have affected the pattern of use of health care services among the immigrant population, despite the evidence of increased barriers to access health care and decreased quality of care. 16
While most studies have not accounted for the potential role of the social determinants of health to explain inequalities in access to health care services, the evidence suggests that gender, length of stay, knowledge or command of the language, educational level, employment status, and administrative or legal situation have a substantial impact on health care use.17–19 In addition, while most studies have used population health national14,19,20 or regional surveys,21,22 they do not capture information specific to migration. Thus, with the implementation of policies of health care cuts in 2014, the second Foreign Immigrant Population Survey was conducted in the Basque Country. This survey included health and health care system questions comparable to those included in the Health Survey of the Basque Country 2013 conducted in the native population. Using these data, this study aims to examine inequalities in access to different levels of health care services (general practitioner, specialist, and emergency department) between the immigrant and native populations residing in the Basque Country, Spain. Because men and women tend to use health care differently, results were presented according to sex. 19
Methods
Study Design and Population
We used data from for individuals aged 16 to 59 years old who participated in 2 cross-sectional surveys, the Foreign Immigrant Population Survey 2014 (EPIE’14) for the immigrant population and the Health Survey of the Basque Country 2013 (ESCAV’13) for the native population. Both surveys were conducted with representative samples of private households, covering the non-institutionalized population. Data were collected through face-to-face interviews at the participants’ home.
The EPIE’2014 collected information on the living conditions, health status, and health care utilization for the immigrant population aged 15 years and older, residing in the Basque Country. Using information from the 2013 census data, a random sampling design stratified by place of birth and of residency was used. We used information obtained from the individual questionnaires conducted in selected households, including a sample of 2,350 adults representing a completion rate of 69.3%. All the interviews were performed in Spanish. The ESCAV’13 collected information on the health status, use of health services, and social determinants of health among people aged 15 years and older residing for more than a year in the Basque Country. As with the EPIE’2014, we used information obtained from the individual questionnaires, for a sample of 8,036 adults and a completion rate of 86%. The interviews were performed in Spanish and Euskera. A full description of these survey methodologies has been published elsewhere.23,24
Variables
The outcome variables were the use of health care specified as general practitioner (a visit to a primary care practitioner in the past year before the interview), specialized care (a visit to a specialist in the past year before the interview), and emergency services (a visit within 6 months before the interview), with responses of yes or no for each service. The independent variable was birthplace, classified as born in Spain or born in a country with a Human Development Index (HDI) non-very high in 2015 or >0.83 (Europe, Africa, Latin America, Asia). While the cutoff point for HDI non-very high is 0.80, 25 we used 0.83 given the data available in the surveys. Individuals from high-income countries were excluded because they have similar or better socioeconomic position than the native population, and thus, inequalities between native and immigrants may not be observed.
Consistent with previous studies,14,23 we considered as covariates age (16–29, 30–44, and 45–59 years), length of stay in Spain (<5, 5–10, and >10 years), administrative or legal situation (permanent resident, nonpermanent resident, and irregular resident), understanding of Spanish (no difficulty/fluent and very little/with difficulty), educational attainment (primary or less, secondary, and graduate or higher), employment status (employed, unemployed, and others), living arrangement (couple and other), and self-rated health as good (very good or good) and poor (fair, bad, or very bad). For Spanish natives, it was assumed that they were permanent residents and spoke Spanish.
Of the total EPIE’14 participants (n = 2,350), we excluded individuals older than 59 years of age (n = 144), those born in countries with a HDI ≥0.83 (n = 176), and those who did not have a health card (n = 60) or had missing information on the outcomes – general practitioner (n = 8), specialized care (n = 20), and emergency services (n = 34). These exclusions resulted in an analytical sample of 1,908. For the ESCAV’13 (n = 8,036), we excluded individuals younger than 16 years of age (n = 55) and older than 59 years of age (n = 3,267), those born outside Spain (n = 371), and those who did not have a health card (n = 67) or had missing information for employment status (n = 1), living arrangement (n = 2), or the outcomes of interest – general practitioner (n = 19), specialized care (n = 21), and emergency services (n = 1). These exclusions yielded an analytical sample of 4,232.
Statistical Analysis
Descriptive statistics for selected characteristics were calculated for the total population and according to birthplace in women and in men. In addition, prevalence estimates for use of different levels of care were calculated for each covariate according to sex within immigrant and native populations. Chi-square and Cochran–Mantel–Haenszel statistics were used to assess significance associations between (1) each covariate with sex or each outcome and (2) each covariate with each outcome, between the immigrant and native populations, respectively. We used log-binomial regression to quantify the associations between birthplace and each outcome in men and in women before and after controlling for selected covariates. We tested interaction terms between country of origin and age in the fully adjusted model in both women and men.
Data management procedures were carried out using SPSS 22.0 (IBM, Armonk, NY), whereas the statistical analyses were conducted using SUDAAN 11.0.1 (RTI, Research Triangle Park, NC) to take into account the complex sampling design and yield unbiased standard error estimates. Sample sizes presented in Table 1 were unweighted, but all other estimates (proportions, standard errors, prevalence ratios (PR), and their 95% confidence intervals (95% CI) were weighted.
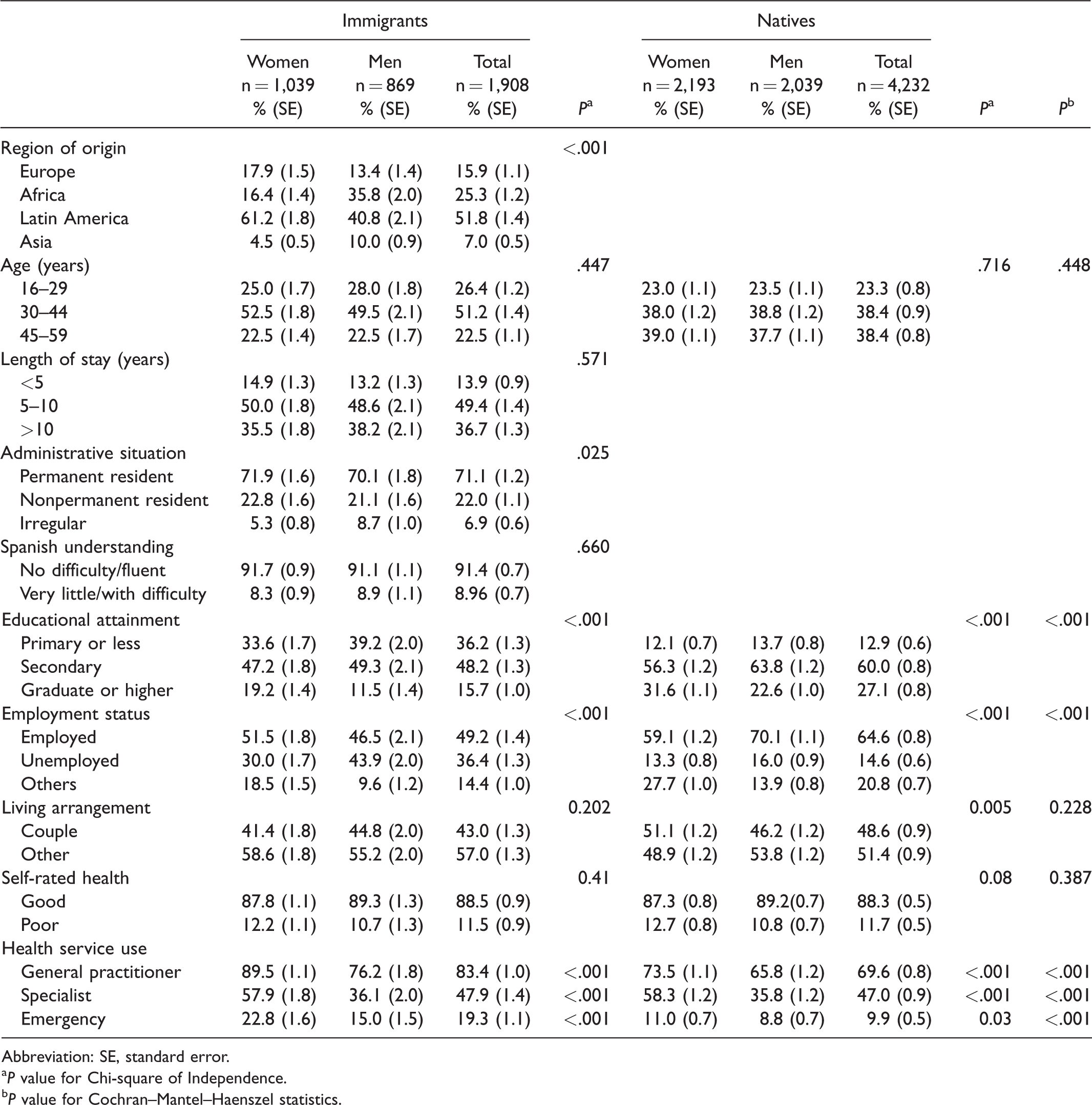
Distribution of Sociodemographic, Health, and Service Utilization Characteristics for Participants in the Survey of the Foreign Immigrant Population 2014 and Health Survey 2013, Basque Country, Spain.
Abbreviation: SE, standard error.
aP value for Chi-square of Independence.
bP value for Cochran–Mantel–Haenszel statistics.
Results
Table 1 shows the distribution of sociodemographic, health status, and use of health care among immigrant and native population in women and men. Compared with the native population, the immigrants were less educated, more likely to be unemployed, and more likely to use general practitioner (GP) and emergency services regardless of sex (P values < .001). More than half of the immigrant population came from Latin America (51.8%), and almost half (49.4%) had lived between 5 and 10 years in the Basque Country. Over two-thirds (71.1%) were permanent residents, and the majority understood Spanish (91.4%). Moreover, among immigrants, women are more likely to come from Latin America (61.2%) than men (40.8%; P value < .001), while men are more likely to have an irregular situation (P value = .025), have primary education or less, or be unemployed (P value < .001) and less likely to have a visit to any of health care services (all P values < .001).
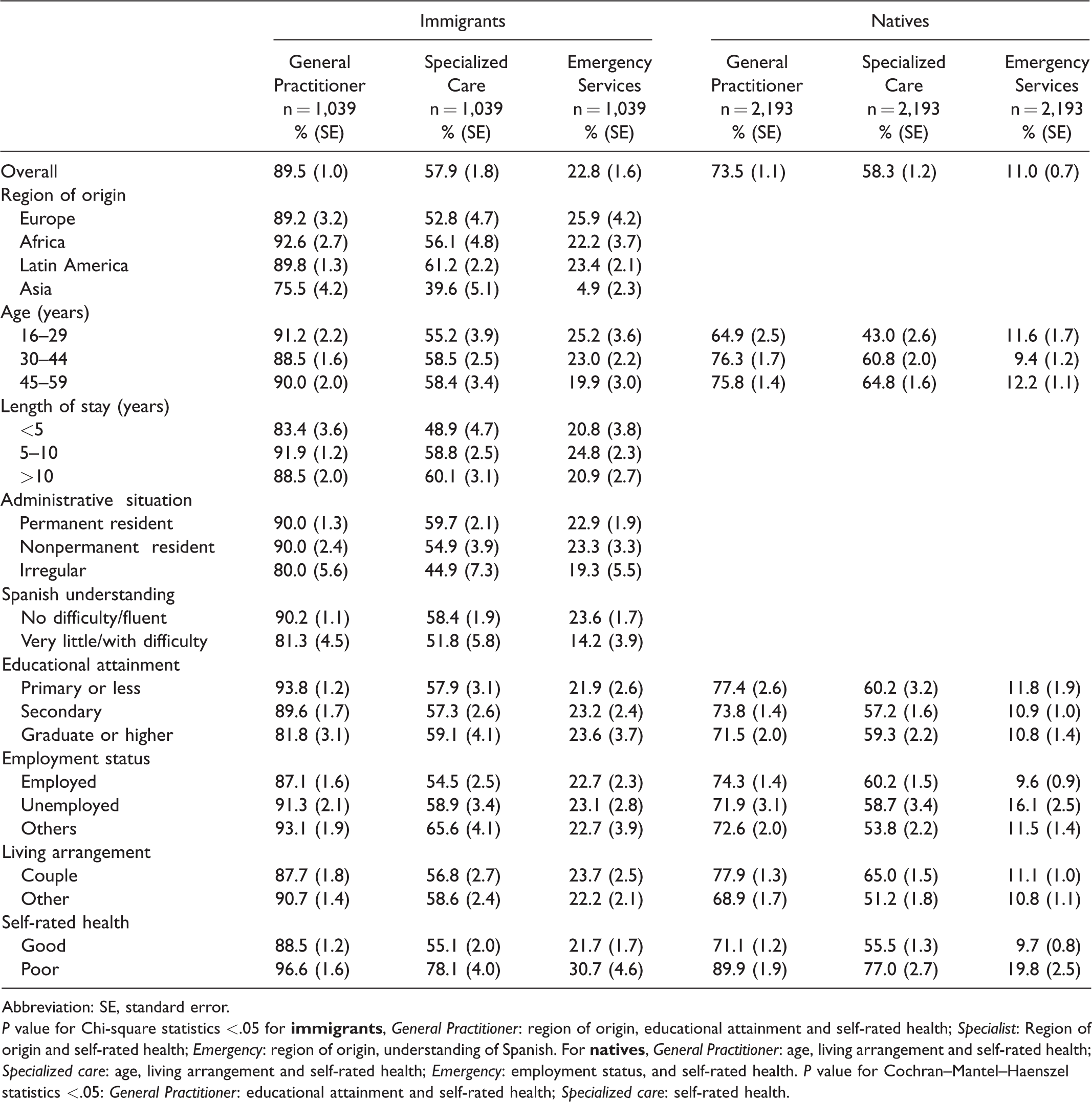
For women, the prevalence for use of general practitioner (GP) and emergency health services was higher in immigrant women than in natives (Table 2; P values < .001). However, when compared to native women, higher prevalence for GP visits was associated with education and self-rated health and for specialized care with self-rated health among immigrant women. Among immigrant women, being from Asia was associated with lower GP use, while having low educational attainment and poor health was associated with a higher prevalence of GP use. Moreover, for immigrants, lower use of specialist care was observed among women from Asia and a higher use of specialized care among women from Latin America and those with poor health. Finally, women from Asia and those having difficulties with the Spanish language exhibited a lower use of emergency services. For native women, older age, living with a partner, and poor self-rated health were associated with a higher prevalence of GP and specialist use. Moreover, native women who were unemployed and rated their health as poor were more likely to use emergency care services.
Prevalence of Utilization of Health Services in Immigrant and Native Women: Survey of the Foreign Immigrant Population 2014 and Health Survey 2013, Basque Country, Spain.
Abbreviation: SE, standard error.
P value for Chi-square statistics <.05 for
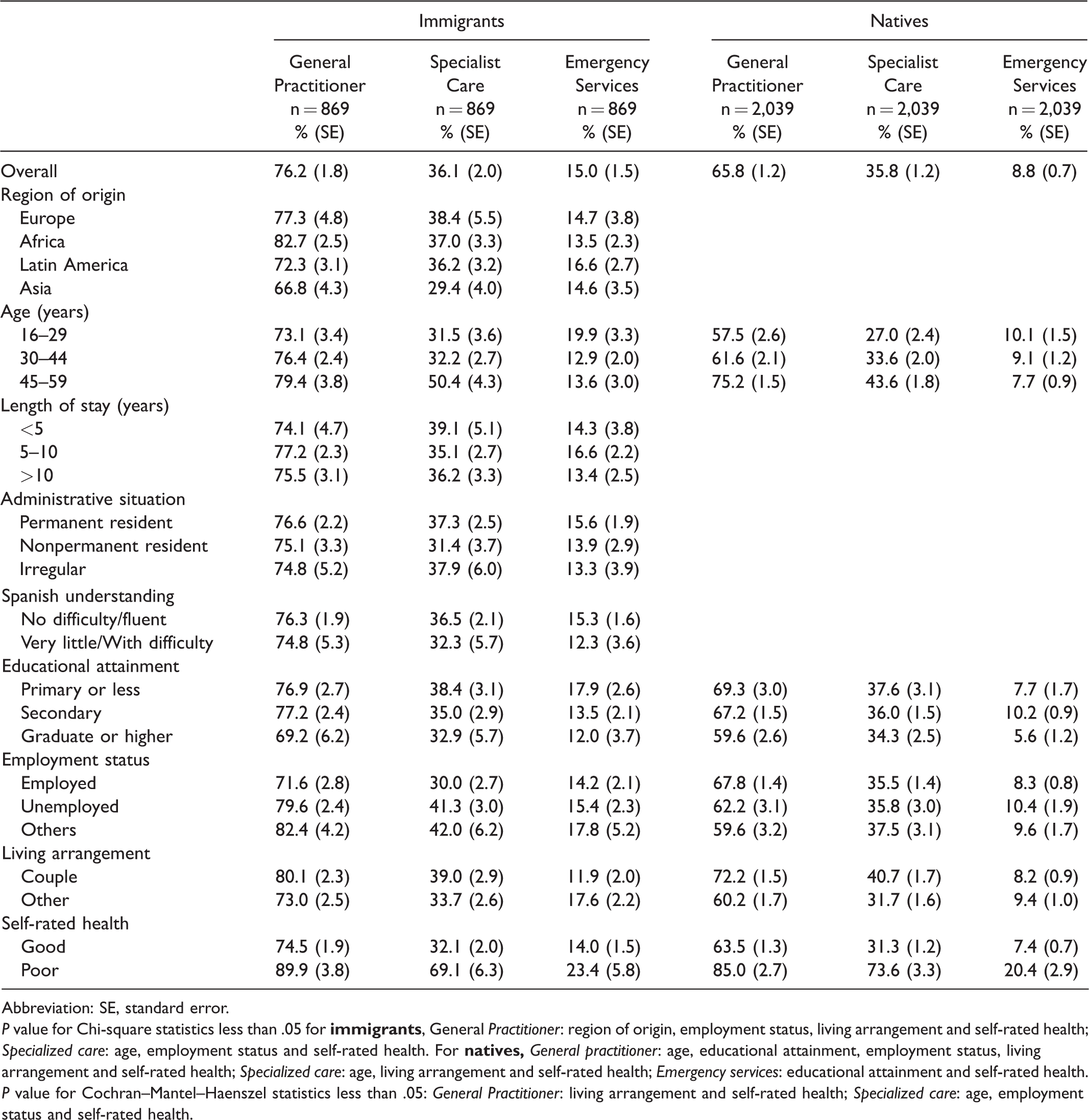
Similar to women, immigrant men tend to use more GP and emergency services than their native counterparts (Table 3). For immigrants, a lower use of GP care was observed among men from Asia and high educational attainment while higher use of GP services was observed in men from Africa and those unemployed, living with a partner, and having poor health. Immigrant men also used more specialized care if they were aged 45–59 years, were unemployed, and reported poor health. Among native men, use of GP care services was associated with older age, low educational attainment, cohabitation, and poor health. In addition, use of specialist services was higher in older native men, those living with a partner, and those reporting poor health, while for emergency services, use was higher among native men with secondary education and those with poor health.
Prevalence of Utilization of Health Services in Immigrant and Native Men: Survey of the Foreign Immigrant Population 2014 and Health Survey 2013, Basque Country, Spain.
Abbreviation: SE, standard error.
P value for Chi-square statistics less than .05 for
P value for Cochran–Mantel–Haenszel statistics less than .05: General Practitioner: living arrangement and self-rated health; Specialized care: age, employment status and self-rated health.
Table 4 shows the adjusted prevalence ratios (95% CI) of birthplace for the use of health services in both women and men. In women, the probability of using GP services was 22% (PR: 1.22; 95% CI: 1.17–1.26) higher in immigrants than in natives. This probability remained nearly unchanged regardless of the variables adjusted, with the fully adjusted model showing a 19% (PR: 1.19; 95% CI: 1.12–1.26) greater probability of GP use among immigrants relative to native women. For specialized services, there were no differences between immigrants and natives regardless of the variables controlled for. For emergency services, immigrant women had a 2.08 (95% CI: 1.72–2.51) greater probability of use than their native peers. This association was slightly attenuated when adjusted for all covariates but remained significant (PR: 1.97; 95% CI: 1.43–2.69).
Prevalence Ratios and Their 95% Confidence Intervals of Birthplace on Utilization of Health Services in Women and Men: Survey of the Foreign Immigrant Population 2014 and Health Survey 2013, Basque Country, Spain.
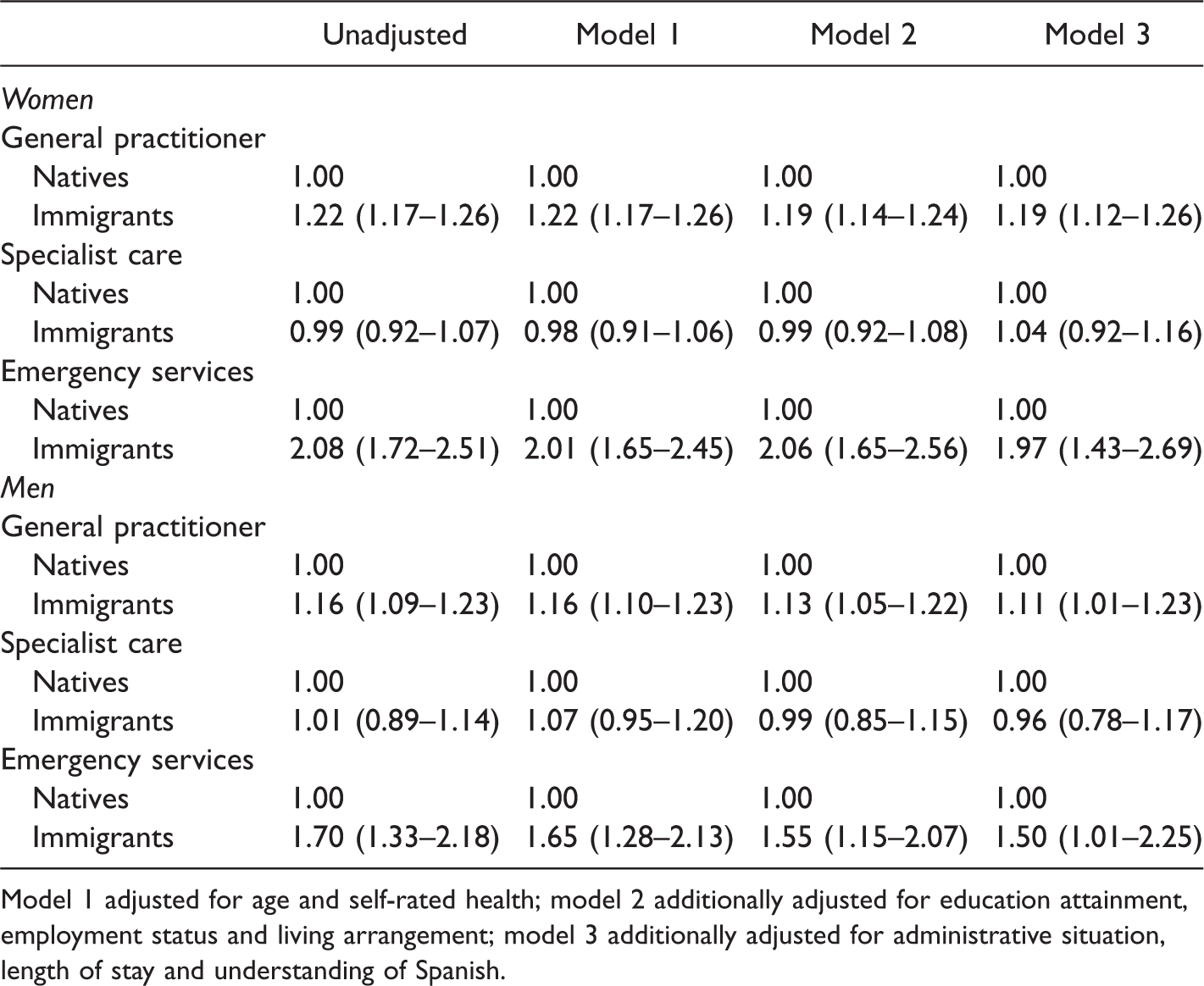
Model 1 adjusted for age and self-rated health; model 2 additionally adjusted for education attainment, employment status and living arrangement; model 3 additionally adjusted for administrative situation, length of stay and understanding of Spanish.
In men, the probability of using GP services was 16% (PR: 1.16; 95% CI: 1.09–1.23) higher in immigrants than in natives. This probability was slightly attenuated after full adjustment (Model 3: PR: 1.11; 95% CI: 1.01–1.23) but remained significant. Similar to women, there was no association between birthplace and specialized services use. Finally, immigrant men had a 1.70 (95% CI: 1.33–2.18) higher probability of using emergency care services than their native peers. This association was reduced after adjustment for all covariates (PR: 1.50; 95% CI: 1.01–2.25).
We observed heterogeneity of the associations of birthplace and use of GP and specialized services according to age (P interactions: .018 and .001, respectively) among women and of birthplace and GP services use according to age among men (P interaction: .019; Table 5). Among women, although use of GP services was significantly higher among immigrants than among natives, this probability was higher among women aged 16–29 years (PR: 1.43; 95% CI: 1.24–1.64). For specialized care, the use was higher among immigrant women aged 16–29 years relative to their native counterparts. When compared to native men, only GP services use was higher among immigrant men aged 30–44 years (PR: 1.18; 95% CI: 1.03–1.37).
Prevalence Ratios and Their 95% Confidence Intervals of Birthplace on Utilization of Health Services in Women and Men According to Age Groups: Foreign Immigrant Population 2014 and Health Survey 2013, Basque Country, Spain.

Adjusted for age, self-rated health, education attainment, employment status, living arrangement, administrative situation, length of stay, and understanding of Spanish.
Discussion
This study shows that immigrants and natives use the health care services available differently even though these services are a free and universal in their coverage. Specifically, immigrants, both women and men, were more likely than natives to use GP and emergency services. There was no difference for specialized services use, except among younger immigrant women, who tend to use more services than their native counterparts.
With regard to the greater use of GP services among immigrants, our results are inconsistent with previous national studies showing similar or lower use of GP services.2,5,26,27 It is worth noting that in our study the probability of GP use in immigrants hardly changed after adjusting for relevant variables, including migratory ones. The characteristics of both the health care system and those of the population may help explain these results. For instance, in the Basque Country, as in the rest of the autonomous communities, primary care constitutes the entry and first point of contact with the health care system. However, in response to the economic crisis, political measures were introduced that included a reduction in public health expenditure and health care rights. In the Basque Country, these measures were applied in a less strict way, and access to health care services for immigrants was not limited. 28 However, spending in primary health care stagnated, and as a consequence, working conditions for health care personnel deteriorated. 29 This deterioration led to an increase of unnecessary consultations due to the inability to solve problems at the GP level of care, and although it affected the population as a whole, it did so especially for the immigrant population.13,16 Regarding the characteristics of the population, the higher use of GP in immigrants could be because, for this level of care, solutions to needs are not always related to health alone but also to social or economic problems.30,31 In the case of immigrant women, their higher birth rate together with their highest teenager pregnancy rates14,20 may explain the increased use of GP appointments in our sample.
For specialized medicine, we did not observe differences in the use of services between immigrants and natives, with the exception of higher use in immigrant women aged 16–29 years. The latter is inconsistent with most studies indicating a lower utilization of specialized care in immigrants.2,26 Thus, our findings may indicate an equitable access and a good performance of the health care system, that during the economic crisis period maintained not only universal access 28 but also an increase in public spending for specialized care. 29 In addition, in the pre-crisis period, strategic changes were introduced to improve system efficiency and continuity of care. 32 The latter could also have contributed to reduce inequalities in the use of specialized care.
Consistent with a recent review conducted in 6 European countries, we found a higher use of emergency services in immigrants than in natives. 33 However, we found that the use of emergency services does not mean less use of another level of care.27,34,35 Emergency services are easy to access, free, and available 24 hours a day. The accessibility has been used as a rationale to explain the greater use of this service in immigrants. 26 In our study, the greater use of emergency services could be related to the higher fertility rate20,27,34 and work-related conditions in immigrant women. In the Basque Country, almost half of working immigrant women are domestic servants and home aids. 36 High employment rates without contracts, long working hours, low wages, and lack of 2 consecutive days of rest37,38 could explain the use of emergency services to respond quickly to health problems without hampering their work activities. 22 Similarly, reasons related to precariousness and job instability, especially during the crisis period, may also explain the increased use of emergency services in immigrant men.14–16
This study has some limitations that must be underscored. First, it is a cross-sectional study and does not allow a temporal relationship between birthplace and the need to use health care services. While it is possible that the immigrant population represents a healthy effect, the surveys do not provide information on health status of the immigrant population upon arrival in Spain. Due to this selection bias, there is evidence of underrepresentation of immigrants with lowest socioeconomic status, residential instability, or low proficiency in the Spanish language. 39 The exclusion of this subgroup of immigrant requiring a higher level of health care services may have underestimated our results. Second, we could not present information according to country of birth for the immigrant population. The lack of this information may have masked variability in the use of each level of care according to country of origin for the immigrant population. However, we repeated the analyses using region of birth (Europe, Latin America, Africa, and Asia). The results were statistically significant, consistent to the ones reported here for women in the use of GP and emergency services except for Asian women. When compared to native women, Asian women exhibited similar use of GP and emergency services and lower use of specialized care. Among men, although not statistically significant, the results were consistent in the use of GP and emergency services and specialized medicine services with the exception of Asian men, who exhibited similar use of GP than their native counterparts. However, it is important to emphasize that our study is based on representative samples for both immigrant and native populations and that includes important immigration-related variables associated with the use of health care services. Hence, this study examines the differences in access to health care services between immigrant and native populations, including factors that may explain this relationship in the context of the privatization and sanitary austerity that took place in the period of the economic crisis.
Our study shows access to specialized care is fairly and evenly distributed among natives and immigrants. However, use of health care was more prevalent among immigrant women and men for GP and emergency services. These findings were observed after controlling for all variables, within the framework of a universal health care system and with little to no policy of austerity or privatization. These results underscore the importance of guaranteeing access to health care to the entire population, to reduce the impact that structural determinants of living and working conditions may have on the population health, especially the immigrant population. Hence, policies to eliminate barriers to health care are essential to ensure health for all. Such policies need to be proportional to the degree of disadvantage to provide equal access to the different groups such as immigrants in our society.
Footnotes
Compliance With Ethical Standards
Ethics approval and consent to participate. This article is based on secondary data. Data were collected by the Department of Health and the Department of Employment and Social Policies (Basque Country) following the Law 4/1986 of the Basque Government. The records were validated, encrypted, and processed according to established protocols by the Ministry of Health, Social Services and Equality (Spain).
Acknowledgments
The authors acknowledge Luis Sanzo and Xabier Aierdi (Department of Employment and Social Policies of the Basque Government, Spain) for providing the data.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the University of the Basque Country UPV/EHU [project EHU14/55] and by the Basque Government Research Fund to consolidate research groups (Ref. IT977-16).