
Abstract
Drawing from 56 semi-structured interviews, this article details how undocumented Latina immigrants living in Atlanta, Georgia, in 2013 cultivated health and well-being in an insecure environment. In addition to the myriad challenges that immigrants face in accessing health care in their new communities, undocumented immigrants living in Atlanta at that time faced the legal barrier presented by Georgia’s new “show me your papers” law, which imbued public space with the risk of deportation for those who are undocumented. This law complicated health care access by making the trip to the doctor’s office risky. Immigrants’ health care decisions were thus shaped by the “geography of fear” that permeated their new communities. This fear presented itself not only in public space but also in clinics and hospitals, where many immigrants feared – and sometimes received – bad treatment. Despite the obstacles fear and immigrant policing presented, many of the women I interviewed showed boldness in their health care decisions, staking their claim to medical attention where they saw fit. Additionally, many maintained transnational networks and continued with familiar health practices from home. Combined, these strategies worked to create complex and shifting “therapeutic landscapes” in an environment permeated by insecurity and fear.
Introduction
Many people think that, if you go to the hospital, they won’t help you because you’re not legally here. Many of my customers, my acquaintances, they’re scared.
Clara, a 28 year-old immigrant from Mexico, who works as an insurance agent
I am sitting in an apartment in suburban Atlanta with my interpreter and Marisol, an undocumented immigrant and mother of 3 who is originally from Mexico. As we are discussing her experiences with health care in the United States, she begins to talk about the health-fortifying foods that she made in Mexico and continues to make here. Among them is homemade yogurt, which she regularly prepares for her family and which I gratefully accept after she offers it to me. This yogurt is one way that she maintains her health and that of her family, and it is considerably less complicated than the more “formal” routes to well-being, such as going to see a doctor. For the cases when she does need to see a doctor, a major obstacle is getting there. Marisol has access to a car and knows how to drive, but instead of making a routine doctor’s appointment by car, which would take about 20 min, she chooses to get there through a combination of walking along Atlanta’s busy streets and navigating the city’s often-undependable bus system. She picked this doctor because he has a reputation for treating immigrants kindly, but the trip to the clinic will cost her 8 h of her day, long waiting time included. To her, however, it is the lesser evil: by not driving she won’t have to worry about the risk of being pulled over by the police and asked for immigration papers.
This is a common scenario for undocumented Latina immigrants in Atlanta, which is located in what immigration scholars have termed the New South, 1 or the group of states in the southeastern United States that has experienced a drastic increase in immigration from Latin America within the past 2 decades. Within the same time period, and especially after September 11, 2001, many states in this region and elsewhere have initiated a localization of immigrant policing, rescaling immigration law from its largely federal purview down to state and municipal laws, which are facilitated by local police officers who often work in collaboration with national agencies such as Immigration and Customs Enforcement.2,3 Georgia’s own HB 87, passed in 2011, allows police officers to ask anyone for immigration papers while investigating unrelated offenses. (Portions of HB 87, not including the section that makes it lawful for law enforcement officers to ask for immigration papers, were struck down in March of 2013. This included the section that made it unlawful to transport undocumented immigrants.) While this legislation has been propagated in the name of national security, it has worked to intensify insecurity in the lives of undocumented migrants by making detention and deportation a possible outcome of mundane tasks, such as driving to the doctor’s office.2,4 HB 87 prompted many to flee the state, but for those who stayed, like Marisol, the law has become a largely invisible, yet powerful force in their everyday lives. The self-policing immigrants undertake to avoid being caught generates new geographies of space and time. If one were to map Marisol’s path to the doctor’s office, the map would seem nonsensical, as it would show a circuitous and time-consuming trek between 2 relatively close places. To Marisol, however, this route makes perfect sense, as it is a route that lends some sense of control and security to her life.
By examining how undocumented Latina immigrants seek health and health care in the context of localized immigrant policing in the New South, I seek to contribute to understandings of how experience of place intersects with, and shapes, health and access to health services, and add to the literature on how immigrants and other marginalized groups experience barriers to health care. 5 Little research, however, directly addresses how marginalized groups experience these spatial barriers to health care access. 6 Drawing from 2 literatures in the field of geography, I combine the concepts of “therapeutic landscapes” and “geographies of fear” to detail the strategies that Latina immigrants employ to foster security through health, and in accessing health care, in an environment that is, for them, characterized by insecurity. In addition to the threat of policing, Latina immigrants are susceptible to discrimination in a New South city that sees Latin American immigrants’ “new faces” as threatening and dangerous, 7 and Latina women in particular as threatening due to their perceived “hyper-fertile” status8–10 and their presupposed drain on the health care system. 11 I therefore examine how fear affects health care access and experiences for undocumented Latinas, both in the form of face-to-face discrimination as well as the ever-present, yet intangible, threat of immigrant policing of which it is part and parcel. With deportation as a ubiquitous threat (as well as other aspects of the immigrant experience that make life precarious, such as unstable employment and income 12 ), the Latina immigrants I spoke with invested much energy and time into carefully cultivating the health of themselves and their families, both through formal and informal routes. Like Marisol, interviewees considered doctors’ reputation with immigrants before visiting them, and the trip to the clinic was undertaken carefully. As with many immigrants, an important piece of their therapeutic landscapes was incorporating health knowledge from their home countries into their medical treatment here. This included eating certain foods, as with Marisol’s preparation of yogurt using techniques from Mexico.
The study of therapeutic landscapes has an innate focus on how place is constitutive of – or prohibitive of – well-being, and, importantly, it showcases how well-being is actively cultivated in situ. In doing so, this literature draws out how health and well-being can simultaneously exist and be absent at the same site for different people, 13 as well as how “larger” tides, such as geopolitics and economics, influence the shape and scope of therapeutic landscapes. 14 Relatedly, geographies of fear literature focuses on how certain spaces can be conducive to fear and anxiety for some (mostly women), while not others (mostly men). In combining therapeutic landscapes with geographies of fear, I aim to contribute to studies of the active, fragmented, and highly contingent nature of therapeutic landscapes. Specifically, following a review of therapeutic landscapes and geographies of fear and a discussion of my field site and methods, I detail how undocumented Latina immigrants made decisions and undertook actions that would provide some semblance of security through pursuing health and health care in a place that could be fear-inducing and dangerous.
The Intertwining Geographies of Fear and Health
The concept of therapeutic landscapes originated within medical geography in the early 1990s with Gesler, 15 who defined the term as “a geographic metaphor for aiding in the understanding of how the healing process works itself out in places (or situations, locales, settings, milieus).” Gesler16,17 first used the concept to examine the reparative qualities of “natural” or non-medical settings that were thought to have healing and therapeutic capabilities, such as the Asclepian Sanctuary in Epidauros, Greece, and the Marian Shrine in Lourdes, France. Since then, the term has been diversely employed by Gesler and other health geographers, who have transformed it to include sites beyond the exceptionally healing, such as formal health settings (e.g., hospitals and clinics), 18 places of addiction recovery, 19 community health organizations, 20 and mundane settings such as domestic gardens 21 and the home. 22 Thus therapeutic landscape can be seen as active tableaus that must be constantly and consciously curated to foster the “therapeutic” elements; these landscapes often exist within larger contexts that are anything but therapeutic. 23 In this sense, therapeutic landscapes are reparative, everyday incarnations of people’s desire to enable well-being despite living in environments that are often disabling of well-being. Therapeutic landscapes are thus now recognized as being hardly ever purely or immediately therapeutic: “It is already apparent that there can be less positive shades of therapeutic landscapes than have been previously considered.” 24
More recent literature has also highlighted how marginalization and “difference” impact individuals’ facilitation of well-being and how this process is contextual. 25 For example, Wendt and Gone 20 look at indigenous groups in the midwestern United States, and Alaazi and colleagues 23 explore the health practices of the indigenous homeless population in Winnipeg, while Milligan and colleagues 21 have examined the therapeutic landscapes of the elderly. However, little has been written about immigrants and their experiences with therapeutic landscapes, which has prompted Dyck and Dossa 26 to declare immigrants “invisible in the ‘cartography’ of healthy spaces.” In the same breath, Dyck and Dossa also insist that “[t]he gendering of the productive action in constructing healthy space . . . has received little attention.” 26 Their study of how 2 different groups of female migrants living in British Columbia – Sikhs from the Punjab and Afghan-Muslim refugees – make leeway in amending these omissions. They look at how these 2 groups of immigrants construct healthy environments for themselves and their families using a diversity of modalities, including preparing the foods of their home countries. Dyck and Dossa 27 thus illustrate that therapeutic landscapes are gendered and never purely local and that home for them should be “understood in the sense of a transnational domain.” While wealthier migrants and those who are documented may travel back home to maintain connections with their home countries, 28 many immigrants are less mobile and therefore depend greatly on communication technology to sustain the transnational elements of their therapeutic landscapes. 29 In the context of localized immigrant policing in the New South, long-distance transnational connections are more necessary than ever, because unlike immigrants living closer to the border, 30 and during its less-militarized times, return trips are lengthy and dangerous, therefore forcing migrants to stay in one place. Parsing out the local and transnational topographies of immigrants’ therapeutic landscapes therefore highlights immigrants’ agency and structure within larger socioeconomic and geopolitical contexts.
Health geographers have also investigated how affect and emotions like fear play into therapeutic landscapes. For instance, Andrews
31
talks about the fear of needles, while Oster and colleagues
18
discuss how fear shapes women’s childbirth choices in hospitals. Unlike therapeutic landscapes studies that talk about fear in relation to individuals’ phobias and preferences in the medical setting, geographies of fear literature seeks to connect identity and cultural elements, such as race and gender, to a group’s experiences of fear in public space. Geographies of fear have been a longstanding interest in feminist geography.32–34 Focusing largely on women and, increasingly, other marginalized groups,
35
this literature explores how fear (or its absence) shapes experiences of public spaces,34,36 such as college campuses.
37
In drawing attention to how women’s geographies are circumscribed by fear, this literature has also questioned the assertion that women’s fear of violence in public space is irrational because men are more likely to be victims of violence.36,38 As Koskela
39
says: It has been demonstrated that fear is connected not only to the crime-rate but also to the degree to which people feel they have control over their lives. A sense of danger is often linked to feelings of uncertainty, helplessness and vulnerability. Thus, fear is closely connected to social well-being: the people who feel most vulnerable in society and have the least faith in the future tend to be most afraid. Further, criminal victimisation is often culturally channelled into existing racial and class conflicts. In this sense it can be claimed that the groups that suffer the most oppression are the ones that understandably are most afraid. (Emphasis mine)
Geographies of fear literature has been critiqued, however, for reifying the perception that women are constantly fearful in public. Some feminist geographers therefore focus instead on how women display boldness in public places.38,40 Women are not merely objects in space where they experience restrictions and obligations; they also actively produce, define and reclaim space. The interpretation of boldness can be seen as evaluating and analyzing women’s capacities, abilities and strengths and using these as means for a potential transformation of power relations, in order to serve the emancipatory aims of feminist research.
41
Site and Methods
Since 2000, Georgia’s Hispanic population has nearly doubled – largely through immigration – reaching 819,887 in the 2010 census (the number is in reality higher, of course, because undocumented individuals aren’t included in this count). It is estimated that around 50% of these immigrants live in just 4 counties: Fulton, where Atlanta is located, as well as the metro counties of Cobb, Dekalb, and Gwinnett; these counties have diverse economies and are home to many stable and growing industries in which immigrants find employment.42,43 In addition to HB 87, Fulton, Cobb, DeKalb, and Gwinnett Counties were part of the Secure Communities Program (which was replaced by the Priority Enforcement Program in 2015). 44 This joint federal, state, and local program enlisted local law officers to participate in immigration enforcement through the use of a national fingerprint database, which aids officers in identifying “criminal aliens.” Once identified, Immigration and Customs Enforcement (ICE) can detain and deport criminal aliens. 45
As an emerging immigrant destination, the Atlanta metropolitan area does not have the extensive social aid structures for immigrants that many longstanding immigrant destinations do. Atlanta’s immigrant support systems are instead relatively nebulous and often difficult to navigate. According to the National Council of La Raza 46 (NCLR), an estimated 41% of those who are without health insurance in Georgia are Hispanic. Although the Affordable Care Act (ACA) provides low-cost health insurance options, immigrants who are undocumented are explicitly excluded from any ACA benefits. Currently, health care options are limited for undocumented immigrants, who, if they do seek out health care, mostly rely on low-cost or free clinics. 46 For example, the report 47 from the Hispanic Health Coalition of Georgia’s 2012 Summit shows that only about a dozen facilities offer low-cost reproductive health care in the Atlanta metro area.
From August of 2012 to September of 2013, I conducted research while living in Decatur, Georgia, on the outskirts of Atlanta proper and adjacent to the Buford Highway corridor, a sprawling and diverse multiethnic region where the city’s immigrants are highly concentrated. During this time, I conducted in-depth, semi-structured interviews with 56 immigrants from Mexico (46), Venezuela (4), the Dominican Republic (2), Guatemala (2), Honduras (1), and Colombia (1). Except for 3 interviews performed in English, all interviews were done with the help of a Spanish-speaking interpreter from Mexico City and translated into English. Interviewees’ ages ranged from 19 to the early 60s. The vast majority was of low socioeconomic status and had at least 1 child (5 had no children at the time of this research). Table 1 offers a more comprehensive look at participant demographics.
Participant Demographic Information.
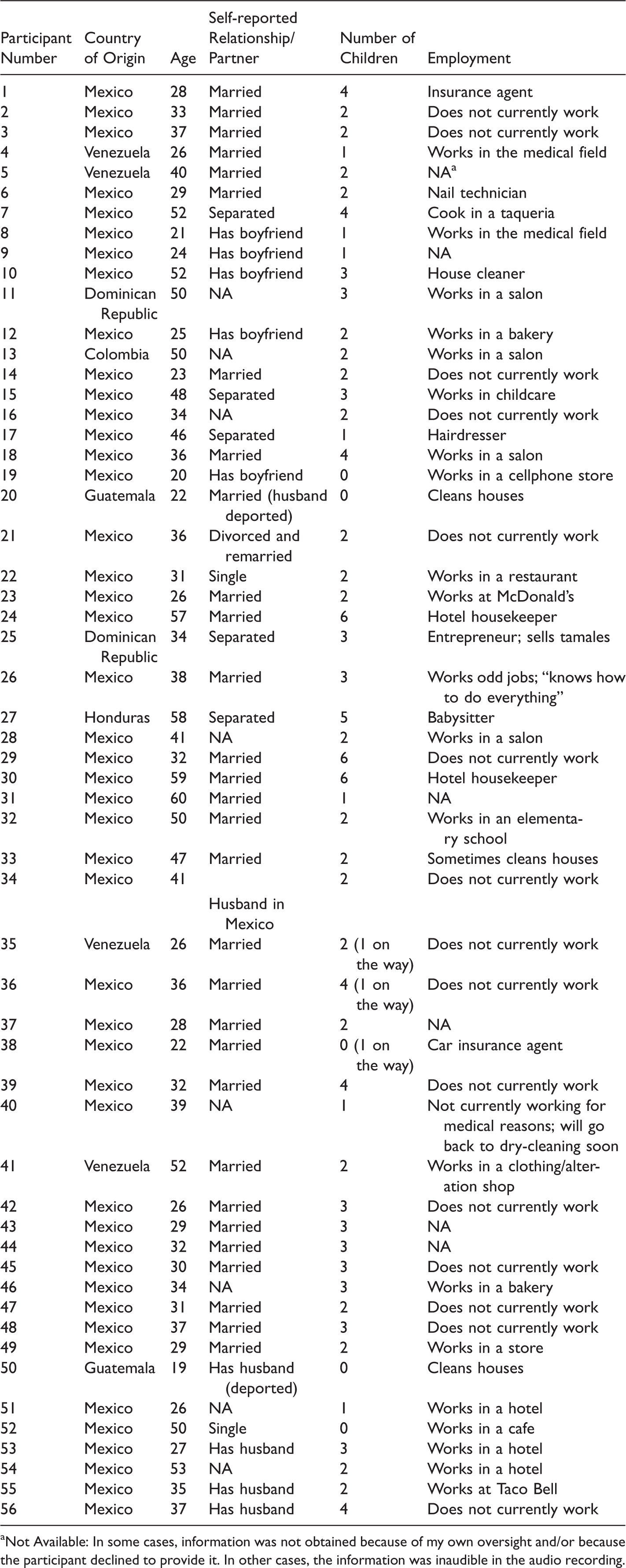
aNot Available: In some cases, information was not obtained because of my own oversight and/or because the participant declined to provide it. In other cases, the information was inaudible in the audio recording.
Most interviews revolved around reproductive health care and childbirth: that was a top priority of interviewees and the reason most of them saw the doctor. I was careful never to inquire as to the immigration status of anyone I interviewed; however, many were forthcoming and revealed during our interviews that they were undocumented. I estimate that about three-fourths of my interviewees were undocumented. My interpreter and I recruited most women by sitting in a Mexican bakery on the Buford Highway and telling customers who came in about the project. Although I was an unfamiliar white woman, I feel that in situating recruitment within a place familiar and “safe” to my informants and having a Mexican interpreter, I was able to recruit interviewees more easily than I had anticipated.
I chose in-depth, semi-structured interviews because I wanted to uncover the distinct variables that go into health and health care decisions. These decisions are irreducible to 1 single factor and are often largely determined by “immeasurable” factors. 48 This is especially notable in the case of immigrants, for whom many diverse cultural considerations go into the decision of when and where to receive health care.49,50 Such information is best gleaned from ethnographic research, or, as Dyck puts it, “Talking to people, rather than about ‘dots on maps’ [referencing Parr 51 ].” 52 Because I wanted to find out how fear and other intangible, aspatial factors would be one such consideration, in-depth interviews about women’s experiences was the most fitting method. This paper thus also contributes to health geography’s more recent focus on the lived experiences of health and well-being,48,53 which can contribute to the concern across various disciplines, including health policy, on factors impacting health care access and health service delivery. Data from interviews were analyzed through close readings of interview transcripts and notes to draw out key themes. In keeping with health geography’s imperative to highlight the lived experience, diligence was undertaken to recognize the varying ways in which these themes were presented in each individual interview.
Fear of Immigrant Policing
Fear is not simply a response to an immediately tangible threat but also a mindset that can take hold in situations where someone feels that they do not have control, leaving them with a sense of vulnerability whose source is multiple.
38
Although the majority of women I interviewed had never had contact with the police in the United States (although most knew of someone, including close family members, who were deported), fear and vulnerability was something that permeated their daily lives. For them, accessing reproductive health care was an emotionally wrought and fearful endeavor due to various factors, not least among them the risk from localized immigrant policing. This was especially evident in the case of interviewees who purposefully quit driving after HB 87 was passed; in these instances, women would opt for public transportation or walking (and more commonly a combination of both), turning what could be a relatively short car ride into a trek of at least an hour or more (which of course was always the case for those who never drove in the first place). As most immigrants live in sprawling suburban Atlanta, walkability is not at its prime, and the Buford Highway is a 6-lane behemoth with few sidewalks or crosswalks. For many interviewees who did not drive, a clinic’s proximity therefore sometimes trumped its cost. Jasmin, 36 and from Mexico, told me of a particularly expensive experience: My pregnancy was high risk, so I had to pay for specialized consultations. I paid $1,000 a month, every ultrasound was extra. But I went there because it was close to home and I cannot drive. I thought that was amazing expensive.
Fearfulness was not limited to those who stopped driving. After the passage of HB 87, many women recognized the danger of driving but continued to drive because the inefficiency of MARTA, Atlanta’s public transportation system, was too risky in and of itself to deal with; this was especially the case for women who worked outside of the home and needed to be at their job on time. Paz, a 46-year old hairdresser from Mexico, told me, The police, they are making a lot of the stops and taking people. They are not doing that for criminals – they’re really looking for immigrants, Hispanics. And we need to get out of this – we need to drive. Even if there is transportation, the transportation is not good. The amount of buses is not good. Every time there is a stop I pray – I pray, I pray, I pray [gets emotional]. . . . There are police and I get so stressed. Last Wednesday I got out of job and I saw a patrol behind me. I was trained when I drive – I do that [imitates praying]. And when I saw that patrol, I was crying and when I saw the next car, and the next. . . . When we arrived at the Latin American Association, I flashed my lights to the other car because I was scared for them. . . . What I wanted was a ride home.
Public space was not the only place where interviewees experienced the fear of being “caught.” Unfamiliar with the purview of a doctor’s responsibility in the United States, some saw doctors as authority figures who could potentially ask them for documentation. In these cases, a doctor’s office became another “border” to try to cross safely or to avoid altogether. In talking to an immigrant health care advocate, she revealed that a women’s clinic popular among Latinas was moved to a different location, in part because it was near a police station and undocumented immigrants were afraid to go to the clinic after HB 87. Clara, a 28 year-old insurance agent from Mexico with 4 children, talked about how some women wait until they are in labor to see a doctor: Clara: A lot of people are scared that if you go to the hospital they won’t help you, because you’re not legally here. Many of my customers, my acquaintances, they’re scared. Author: But for pregnancy and childbirth, you kind of have to go, towards the end. Clara: Many people among the community, not particularly myself, they wait until the last moment to go to the emergency room. They don’t do any care. Many people that I know, they don’t go at all during the 9 months, until they give birth.
Seeking Kindness and Respect
The women I interviewed expressed anxiety about navigating a foreign medical system while not being able to communicate fully with doctors, fearing that their treatment would not be as good because they did not speak English. To them, poor treatment was both a result of the dynamics of medical interpreting (and a lack of interpreters in many cases), as well as a fear that some doctors would not treat them well because of xenophobic beliefs. A doctor’s reputation was therefore a consideration in deciding what clinic to visit, especially among immigrants who had been in the city for several years and had gained a knowledge of the medical terrain through experience and social networks. When I asked what doctors could do to provide better care for immigrants, the number 1 response was that they should have more patience, as well as some knowledge of Latino culture (i.e., cultural competency). For instance, Ursula, a 21-year old from Mexico, said that, “Doctors should be honest with immigrants and not treat them really bad. On a scale of 1 to 10 [with 10 being the most urgent], I would give doctors a 10 on the need to be patient.” Interviewees spoke of dealing with curtness and hostility from doctors, nurses, and receptionists, which they attributed partly to health service providers’ impatience when having to deal with someone who did not speak English. Patience was also discussed in regard to the amount of time doctors spent with them. The women I interviewed told me how they were surprised at the brevity of their interaction with doctors during appointments, as the doctors they were accustomed to in their home countries spoke to a patient a bit about their lifestyle before delving into diagnosis and treatment. Said Talia: A good doctor will be more sympathetic and they will be more . . . eclectic. They will check about your . . . the place where you live and what you do. So they really help you to find what the real conditions are that are causing your problems.
Concerning cultural competency, Lucita – 26 and from Mexico – told me, Doctors should try to make a cultural bridge with the Hispanic people. If any of them would say just 1 or 2 words in Spanish. Even if they just speak 2 words, I will feel much better, just because they try to use words to connect with us.
In populating their therapeutic landscapes with doctors who treated them with patience and respect, interviewees thought it was important both to avoid rude doctors – or counter their rudeness – and to actively seek kind and culturally competent care. In regard to the latter, a significant portion of the women I interviewed knew to avoid a certain large public hospital in Atlanta because it has a reputation for treating immigrants poorly, even if the service is relatively affordable. However, in being constrained by so many other factors, interviewees did not have the freedom to “shop around” for the perfect doctor. Instead many of them used boldness to, in a sense, demand respect and attention when they felt they weren’t receiving it. Many women proudly told me stories about how they stood up to doctors, which resulted in receiving better care. Dyanara, a 38-year-old mother of 3 from Mexico, described how she did this when she insisted on another nurse after the first nurse could not get a needle in her vein to draw blood during an appointment: When I was in for the cesarean, she [the nurse] pinched me here twice [trying to insert a needle]. I was working for a doctor and I learned how to do it [draw blood] in Mexico. I was telling her, “You’re wrong, you’re wrong.” And she told me, “Who has studied – you or me?” And I told her, “No, you don’t do it. Too many mistakes. Another nurse.” And I didn’t allow her. I already fight with the pediatrician – and he’s Hispanic, but he was very mean to me so now when he sees me, he’s, ‘Hi my lady – blah, blah, blah,’ and I’m sure he used to be ‘This woman!’ But that’s when I fight and defend myself and now he treats me with respect.
In light of the poor treatment the women I spoke with faced, it is evident how the therapeutic – in this case, receiving good medical care – can coexist with the non-therapeutic – in this case, the fear, mistreatment, and mental anguish that resulted. When these 2 things intermingle, a therapeutic landscape might be beneficial in the health sense but actually detrimental in a psychological and social sense, harkening back to Baer and Gesler’s 22 notion that therapeutic landscapes contain aspects that are not positive. However, many interviewees sought to reconcile the duality of the therapeutic and the non-therapeutic by seeking out doctors who would be kind, as well as exerting boldness and pushing back against doctors who were not.
Familiarity and Security
As is common with first-generation immigrants, the women I spoke with blended health care modalities from both their home countries and receiving communities.49,54 Interviewees communicated with family, friends, and health professionals from their home countries to obtain health knowledge and sometimes even medicine itself (before it became unlawful to do so), which was more affordable. Anita, who had no kids and was from Mexico, explained, I used to receive medicine like that [by mail], but now my mother cannot send me unless it’s with a person and the person is to have – at the airport – the prescription. Before, my mom, she sent me FedEx – now you cannot by FedEx.
Many sought advice on natural remedies and relied greatly on certain herbs and foods – which varied from person to person depending on the country and region they were from – to maintain their health. The majority of interviewees who used these remedies purchased them in Mexican-owned and -run stores located in immigrant enclaves, such as the Buford Highway corridor, where they felt safe going. Herbal remedies were commonly used for reproductive health purposes. This excerpt of the conversation between Clara and my interpreter (both from Mexico) illustrates the familial sharing and importance of herbal health knowledge: Author: Do you follow the advice of friends or family? Clara: Yes, I do. For example, after the pregnancy, they say take basil seed, because all the air that gets in the stomach pregnancy – it helps you return to your size . . . Also, when I went into labor with my last one, my due date was past, so I needed to take epazote. Interpreter: [To me] It’s a very, very native herb. It’s a plant. It’s great. Also helps you with the menstruation, the monthly cramps. But you cannot take too much, because then you will . . . Clara: Abort. Well, miscarriage. There are some people who use this to miscarry. I used it because I wanted to give birth faster, so I did use that. Author: I didn’t know that. Can you buy this in stores? Interpreter: Yes! In the Mexican stores. I can show you. Clara: As a community, we follow the traditions of our ancestors and what our grandmothers tell us. For example, my grandmother said that the purple onion helps to take out the flames [heartburn].
While for the women I interviewed – none of whom had homebirths in the United States – being pregnant necessitated going to doctors and interacting with them in a medicalized setting, it did not necessitate wholly subscribing to the U.S. brand of childbirth. However, interviewees did not necessarily see an irreparable conflict between their modalities and those of U.S. obstetricians and instead created their own hybrid system that drew from both sources. They stated that they followed the medical advice of both their doctors and their families, and if one seemed more logical than the other, then they disregarded the other. (Only 1 woman reported using no traditional medicine at all, stating adamantly that she was an independent thinker.) They did, however, hide certain practices from doctors. For instance, some interviewees tied a red string around a baby’s wrist to ward off ojo, or the “evil eye.” This was not always taken well by American doctors, who considered the string to be hazardous (of course, my informants viewed it as the opposite – as something protective). In response, some women simply took the string off only when seeing a doctor. Similarly, Jasmin talked about the practice of securing a marble in a newborn’s belly button. Knowing that her doctor would find it odd at the very least, Jasmin would take it out before doctor visits but did not always remember to do this: Jasmin: Yeah, in the belly button you put a marble because the belly can [makes bad sound] can come out, so that’s protection. The baby had fever so I took him to the doctor and because he had fever they take out all the clots and [the doctor] was, “What have you done to the baby? You should never do that!” But it’s very good. His belly button doesn’t stick out because we do that. Author: Did the doctor take it out? Jasmin: Yes, but I put it in again. I said, “Okay, okay.” But when I went back home, I did it again to my baby. But I was very – “Shit! I forgot to take out! I didn’t remember!” I always take it out before, but that day [shakes head] . . . When they checked my blood type [in Mexico], the person told my mother that when I got pregnant, I needed to have a special shot . . . because the type of blood that I have. My mother always said to remember your blood type. . . . In fact my mother was always reminding me, because an aunt has this kind of blood, and she has a lot of miscarriages.
For the women I interviewed, the use of elements from their home countries to construct their therapeutic landscapes was both practical (e.g., it saved money on doctor’s visits, and it prevented complications in the case of Rh negativity) and palliative in that it created a sense of familiarity and control for interviewees, both inside doctor’s offices and without (i.e., frequenting Mexican stores for herbs). While interviewees were selective about what transnational health knowledge they shared with their doctors, they did not express much concern about any irreconcilable conflict between this knowledge and medical advice from doctors, and instead they used both at different times to their advantage. This illustrates that therapeutic landscapes are complex, malleable, extra-local entanglements of knowledge and practice, as opposed to smooth and stable landscapes that are knowable upon first glance.
Conclusion
The therapeutic landscapes of the women I interviewed were shaped in large part by fear. While Georgia’s HB 87 remains an employable de jure mechanism to police those without documents, in the absence of its actual application (which has in fact decreased since the time the law was first passed, largely due to pushback from businesses that depend on undocumented laborers), it more often works as a de facto mechanism that propels immigrants to self-police. In the case of many interviewees, HB 87 exists as a specter that forced them out of their cars and into the streets. Those who kept driving tried to evade this specter with every trip and were selective about why they ventured out into public. For all interviewees, fear was an important yet intangible factor in deciding how, when, and where to seek health care. In detailing how fear plays into the construction of undocumented immigrants’ health care decisions, especially in regard to the places they choose to go and how they travel through public space to get there, it is apparent that therapeutic landscapes can be shaped and constrained by negative factors.
Cultivating therapeutic landscapes was also an essential place-making strategy that infused an unfamiliar environment (and an environment which may also be hostile and unwelcoming) with bits of familiarity, while at the same time trying to remediate the difficulties of dealing with a foreign health care system. As such, interviewees’ therapeutic landscapes included transnational elements, such as herbs and traditional foods, that lent a sense of familiarity and security in an environment that was very much unfamiliar and unpredictable. Going to a Mexican store to get herbs used in their home countries, for instance, was a healthy act that was met with far less fear than going to see a doctor. However, the fear of being rebuked by a doctor caused them to hide certain practices (such as the red bracelets), while the concern of medical emergency caused them to speak up about others (as with the case of Rh negativity). Moreover, in caring for their health through both formal and informal means, the women I spoke with were exhibiting control over their bodies, an act whose importance cannot be underestimated when so much outside of their bodies was out of their control.
My interviewees’ therapeutic landscapes were never fully therapeutic and were in fact fostered in an environment that could easily be characterized as the opposite of therapeutic for undocumented immigrants: it was risky, stress-inducing, and unfamiliar. However, in taking actions to alleviate the negative elements and incorporate familiarity, the women I spoke with were able to weave together therapeutic landscapes that were reparative in that they were conducive to both physical and mental health. Caring for the well-being of their bodies was healthy in and of itself, but so was the fact that, in doing so, interviewees were also reaping and sowing a sense of mental peace by feeling more secure in their health, regardless of the actual efficacy of the health care. Their therapeutic landscapes were thus dual not only because they at once contained therapeutic and non-therapeutic elements – with the former often being an attempt to assuage the latter – but also because they simultaneously worked to improve and maintain both physical and mental health through cultivating familiarity and well-being. This paper thus contributes to the study of the dynamics and contradictions of therapeutic landscapes while adding to it an emphasis on how fear (and boldness) is an important element in contouring these landscapes for undocumented immigrants in terms of both access to, and experiences of, health care. This is an especially urgent concern in light of the way that localized immigrant policing infuses everyday life with risk and uncertainty for undocumented immigrants.
Health service providers are not unaware of how fear impacts health care access for the undocumented population. The recent move by some clinics to deliver secure health care directly to the underserved Hispanic population of the Atlanta metro area through “mobile medicine” is recognition of the impediment that public space now poses to undocumented immigrants’ health care access. Worried that undocumented immigrants would not seek health care if it meant driving to far-flung places and risking deportation, providers like Northside Hospital now send trailers equipped to perform preventative and diagnostic tests, such as cancer screenings, to places where immigrants feel safe, such as their own neighborhoods and the Mexican consulate. This is a step in the right direction for addressing how fear and vulnerability affect health care access, although there is a ways to go: only 1 of the women I interviewed reported using mobile medicine, and only a handful knew of the option. This suggests that while solutions are on the rise for providing health care options to immigrants in a new immigrant destination city like Atlanta, an integral step to implementing these solutions is raising awareness of them among the targeted communities. The risk of deportation did not completely stop my informants from going to the doctor’s, at least in matters related to reproduction, when it is arguably imperative to see a medical professional. Bearing on this necessity, some women took steps to ensure that accessing a doctor was done in a manner that mitigates risk. They also sought out doctors that were kind and culturally competent, and when they were treated poorly, many acted boldly and confronted doctors, resulting in better treatment. Although kindness cannot be guaranteed, the increased availability of culturally competent care is therefore another practical step in alleviating the barriers to health care access for immigrants.
Footnotes
Authors' Note
The views presented in this work are the author's and do not necessarily reflect the position of the U.S. Marine Corps or Davis Defense Group.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a grant from the National Science Foundation (grant number 1303057).