
Abstract
Informed by the theoretical perspective of the political economy of health and in the context of the recommendations of World Health Organization’s Commission on Social Determinants of Health, this article examines the political explanations of geographical health inequities in 2 extremely different settings: Ghana and England. Based on the “north-south health divide” in the 2 countries, the article finds that, while the drivers of health inequities in both countries are policy driven, historically situated contextual factors (colonialism in the case of Ghana and deindustrialization in the case of England) offer explanations for health inequities in both countries. We conclude by discussing the importance of paying attention to structural factors such as colonialism for understanding contemporary health inequities in formerly colonized countries such as Ghana.
Keywords
The problem of health inequalities and inequities (unfair health differences) has been widely documented both within and among countries. In 2008, the World Health Organization’s Commission on Social Determinants of Health (CSDH) published 3 broad goals for tackling health inequities: to improve the daily living conditions of people; to tackle the inequitable distribution of money, power, and resources; and to monitor and measure health inequities to help assess the impacts of policies and programs targeted at reducing health inequities. 1 A decade after this publication, social and health inequities continue to persist globally. 2 An interesting question is whether the drivers of health inequities in countries with varied historical and political contexts differ significantly. For example, how different (or similar) are the drivers of Ghana’s or Nigeria’s “north-south health divide” 3 from those of England’s “north-south health divide” or Germany’s former “east-west health divide”? 4 Additionally, if the causes and explanations of health inequities in such varied contexts differ significantly, how might policy makers in these varied settings respond appropriately to the WHO’s recommendations? This article explores the political explanations of health inequities in 2 very different countries, Ghana and England, in order to compare and contrast the political drivers of health inequities in both countries. After providing a brief account of the theoretical perspective of the political economy of health which informs this work, we explore and compare the drivers of England’s and Ghana’s north-south divide in health, trying to offer some insight on the policy-driven nature of health inequities in the two settings.
Rationale and Basis for Comparison
The choice of comparing radically different cases (a method of case selection referred to in comparative policy research as the “least-likely” method5,6) offers an excellent opportunity for theory building 7 and for understanding whether a given relationship (e.g., between political choices/public policy and health inequities) continues to exist when radically different cases are compared. We have therefore chosen to focus our comparison on Ghana and England because of the significant differences in the contexts of both countries and also because of the north-south divide that affects both countries. A country like Ghana has a colonial past which might be important for tackling social determinants of health in a way that might not be the case for England. Our review, therefore, uses highly different settings to examine some major factors important for understanding contemporary health inequities.
The Political Economy of Health
Varied accounts exist for explaining how and why health inequities occur. These range from individual differences 8 to differences in the organization of societies.9,10 The political economy of health approach presents politics as an explanation for population-level health inequities. According to this body of research, the entire organization of a society affects health inequities. For example, highly unequal societies have more health inequities. 11 From the political economy perspective, the distribution of power, the level of economic and social rights, and political and economic relationships among societies together determine the level of health inequities and vulnerability to societal risks that lead to poor health among population groups.12,13
According to the existing literature in this field, 3 main approaches explain the relationships between politics and health inequities: the welfare regime approach, the politics approach, and the individual policy approach. 14 In the welfare regime approach, various welfare state models (e.g., liberal, corporatist, and social democratic) 15 are compared to investigate their impact on health. 16 The taxonomies above are mostly based on countries in Europe, North America, and Australia – often excluding other regions of the world. 17 The second approach – the politics approach – examines the relationship between various political arrangements, ideologies (e.g., neoliberalization), institutions (e.g., political parties), or processes (e.g., democratization) and health. 14 The final approach examines how specific public policies and political choices relate to health and health inequities. 14 Our study draws on the last 2 approaches as Ghana is not categorized under any of the welfare state regimes.
The English Health Divide
Health inequities exist in England at various geographical levels ranging from regional down to the neighborhood level. 4 Although the concept of a “north-south health divide” is an oversimplification, 18 we use it as an entry point for our research for analytical purposes. Different ways to “divide” the north and south of England have been proposed (the Humber-Mersey line, the southern limit of the “seven-county north,” the Lowry line, and the Severn-Wash line), 4 but for the purposes of this study, by north we mean the 3 northernmost regions (North East, North West, and Yorkshire and Humber) and by south, the rest of the country. Comparing health indicators in the north to the rest of the country reveals several inequities. For example, a girl born in Richmond (in the south) can expect to live 15 years longer than another in Manchester (in the north). 18 These differences in life outcomes occur across multiple indicators. In the sections that follow, we describe major public policies and political choices that are critical for understanding the north-south health divide.
Thatcherism and the Advent of Neoliberalization
Politics in Britain over the past century has seen significant shifts in the role of the state in the provision of welfare services, from maximum to limited intervention.19–21 After the second world war, there was general consensus in England on the need to provide various social benefits for employment, sickness, and pensions for citizens.
19
The 1980s, however, saw a significant shift from such ideas to the embracing of neoliberalization – the idea that markets should determine “all forms of human interaction.”22(p13) While a comprehensive analysis of the concept of neoliberalization is beyond the scope of this study, it is worth noting how different authors have interpreted the term.
23
Wacquant,
24
e.g., distinguishes 2 different approaches to interpreting neoliberalization: one in the narrow sense of hegemonic market rule (“the triadic combination of deregulation, privatization, and the withdrawal of the state from many areas of provision”24(p69)) and the other as an overly broad approach that relies on the Foucauldian idea of governmentality (shifting from a narrow economic view to a broader ideology affecting the overall action and conduct of society “according to principles of competition, efficiency, and utility”24(p70)). Ward and England
25
have also emphasized 5 key aspects of neoliberalization: clarifying first that neoliberalization is a process (as opposed to a static single “neoliberalism”) and that it has 4 key dimensions (at the same time (1) an ideology, (2) a set of policies or programs, (3) an institutional form, and (4) a way of conceptualizing normative ideas of individual responsibility). In whatever way neoliberalization is conceptualized, its advent in England contributed significantly to the north-south health divide. For the purposes of this study, we draw on the narrower economic approach, where neoliberalization tends to advocate a tightly delimited role for the state in regulating economic activity. As a result, it is an agenda that promotes not just the withdrawal of the state from market regulation, but the establishment of market-friendly mechanisms and incentives to organize a wide range of economic, social and political activity.23(p172)
The neoliberal turn in England had important impacts on population health and health inequities across the country. The job losses associated with Thatcherism, primarily through deindustrialization, disproportionately affected the north of England. 27 The retrenchment of the welfare state disproportionately affected unemployed northerners, and attempts to resist such policies received harsh responses with documented instances of brutal and violent subjugation of trade unions (mandated to protect wage levels and working conditions) in Liverpool in the north of England. 28 These have laid a solid foundation for the economic and employment insecurity and the “low-pay no-pay” cycle that has come to characterize employment in former industrial regions in the North East of England. 22
Deindustrialization and the Creation of a London-Centric Economy
Closely related to the point above are the distinct effects of deindustrialization. Deindustrialization over the past 3 decades has occurred mainly in old industrial regions (OIR) located in northern England. 29 Deindustrialization, primarily a Thatcherite legacy, was initially aimed at creating a competitive service-based economy that encourages labor and capital mobility with a global outlook. However, it had a significant effect on the north, causing manufacturing employment to fall from 8.9 million to 2.9 million within the last half century.21,27 In the coal industry – mostly based in the north of England, Scotland, and Wales – 500,000 job losses have occurred, with these falling on former industrial areas in the north while leaving much of the south and the rural north untouched. 21 Although the decline in manufacturing jobs is not unique to England or the United Kingdom, the scale of deindustrialization in the United Kingdom has gone further than most other advanced economies. Over 3 million jobs were lost between 1973 and 2007 in United Kingdom, compared to 0.798 million in Italy, 1.631 million in France, 2.04 million in Germany, 1.994 million in the United States, and 0.72 million in Japan. (Data from the United States starts from 1979 and data for Japan is from 1973 to 2006.)30,31 It is important to state that job losses in England did occur in the south as well; nevertheless, the economic rejuvenation that occurred in places such as London and the South East simultaneously with deindustrialization offset such job losses in a manner that did not occur in the north.27,32
The economic shifts that began during the era of Thatcherism created an economy with visible winners and losers. The “big bang” deregulation of the 1980s and simultaneous public expenditure and investments in banking, finance, and service industries – mostly located in the south (London) – led to southern growth that did not happen in the north. 27 By 2022, the U.K.’s Trade Union Congress (TUC) projects that the United Kingdom will become more unequal, with London and the South East alone accounting for 40% of GDP compared to 2.9% of GDP in the North East. 33 Such economic variations are partly explained by the weakening of northern industries. More recent data showing the North East in particular as the “zero hours contract capital of the UK” 34 gives further credence to the fact that the region may not have recovered from the economic policies of the 1980s. Policies of northern neglect became so entrenched that a former governor of the Bank of England (in)famously stated that “northern unemployment is an acceptable price to pay for curbing southern inflation.”35(p47) The creation of this kind of economy has important implications for the distribution of health inequities in England (see Table 2).
Key Health Indicators Across the 9 Administrative Regions of England.
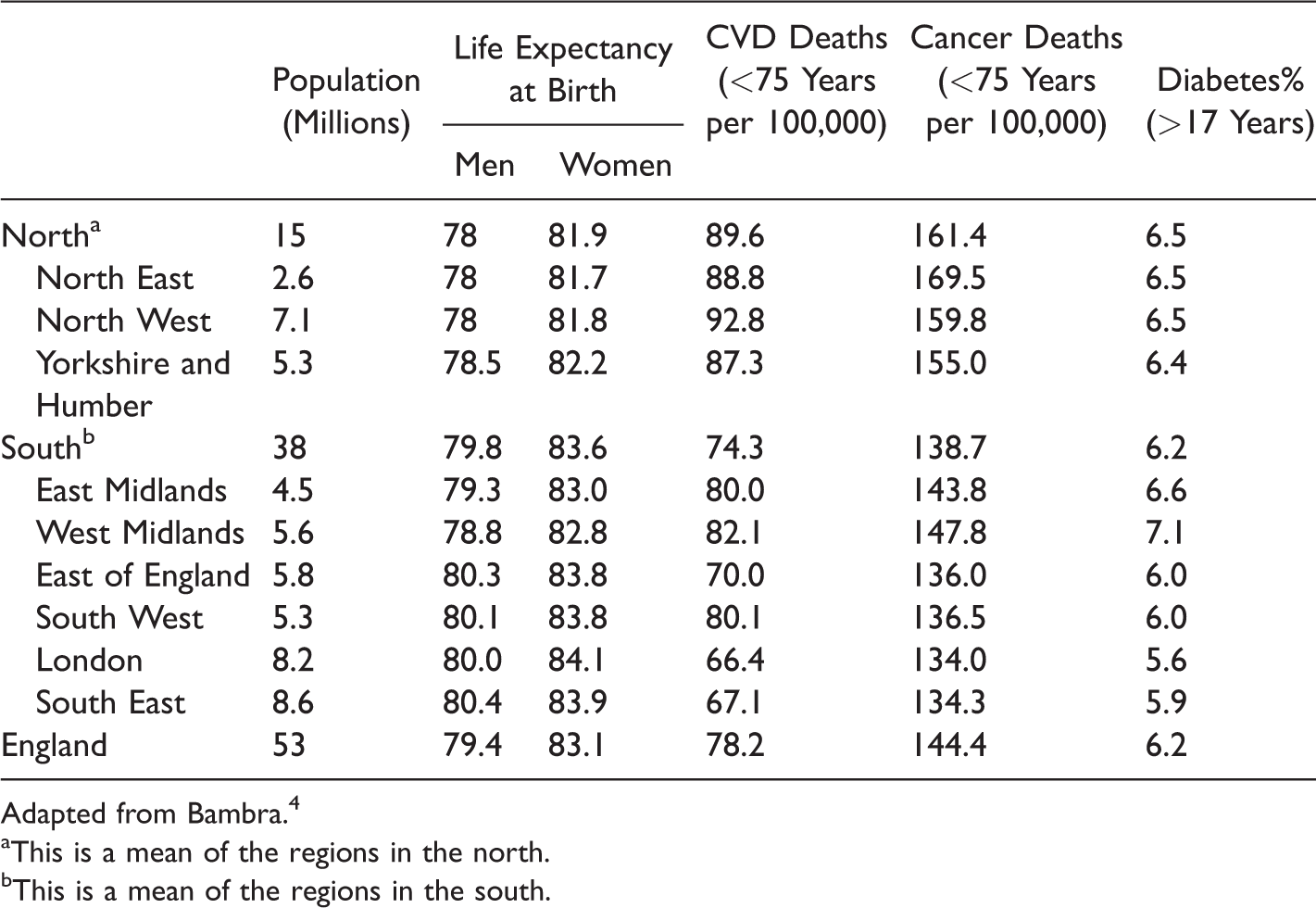
Adapted from Bambra. 4
aThis is a mean of the regions in the north.
bThis is a mean of the regions in the south.
Connecting Public Policies and Political Choices to Health Inequities in England.
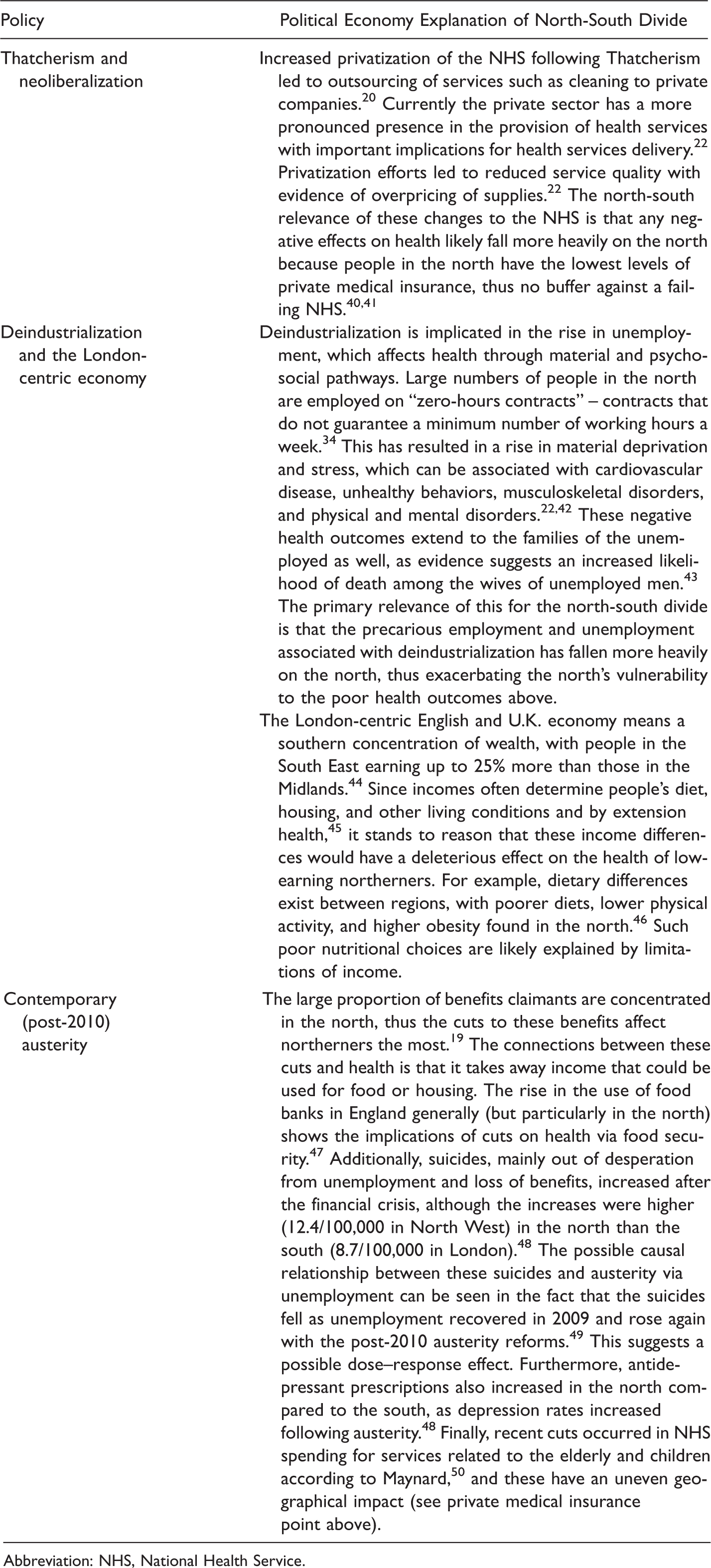
Abbreviation: NHS, National Health Service.
Contemporary Austerity Measures
In more recent times, an important and widely investigated area of study relates to the impact of austerity – “drastic but selective expenditure cuts” – on health.22(p69) Following the 2008 global financial crisis, several countries have pursued austerity as a means to economic recovery with disastrous public health consequences, such as in Greece where public expenditures on health were cut by up to 40%. 36 Between 1921 and 2010, different levels of austerity have been pursued in England, with the post-2010 cuts described as the toughest in recent memory.37,38 The cuts have had a distinct geography disproportionately falling on the poorest local authorities, mostly found in the north of England. In Blackpool in the North West, e.g., every working age adult was projected to lose £720 per year beginning from 2016, compared to £130 in Hart in the South East, due to differential cuts in social programs and differential distribution of claimants nationally. 39 A comparison of the 50 most affected and 10 least affected districts revealed a north-south divide in favor of the south (although some rural areas in the north of England similar to London and the South East were fairly insulated from these cuts). 39 A useful summary of the welfare reforms can be found elsewhere.4(p175) Understanding the relevance of these cuts for the north-south health divide requires an understanding of the geography of welfare recipients in England, which shows that many recipients of various benefits in England live in the north.19(p494)
The implications of these public policies and political choices for north-south health inequities is that the policies engender and entrench inequities. Similar but slightly different is the issue of government spending, which also disadvantages the north. Government expenditure in various sectors – including transportation – shows lower spending in the north compared to the south. 51 Such spending differentials adversely affect the northern economy and leads to a migration of the “best and brightest” from north to south.52,53 A summary of the key implications of these public policies and political choices on north-south health inequities are shown in Table 2. In the sections that follow, we describe the major political factors driving geographical health inequities in a radically different setting – Ghana.
The Ghanaian Health Divide
The past 3 decades have seen remarkable improvements in various health outcomes in Ghana. These improvements, however, have not been experienced similarly across Ghana’s 10 regions (e.g., child mortality rates were twice as high in Ghana’s north as its south in 20033), with the 3 northern regions (Northern, Upper East, and Upper West regions) lagging behind the rest of the country.
Health improvements are also increasingly threatened by the rise in noncommunicable diseases driven by epidemiological and nutritional transitions, 54 although some social interventions such as Ghana’s National Health Insurance Scheme (NHIS) have had a positive impact on health. Table 3 shows that for various health outcomes, except HIV, the north consistently performs worse than the south.
Regional Inequalities in Key Health Outcomes Across Ghana’s 10 Regions.

aCalculations for the north and south are the authors’ own calculations made by simply finding the average of the rates for all regions in the north or south.
bThese are actual national averages and are not calculated by the author.
Data on Malaria case fatality and HIV prevalence (among preganant women attending ANC clinic) come from Ghana Health Service whilst all other health related data come from the Demographic and Health Surveys.
Connecting Public Policies and Political Choices to Health Inequities in Ghana.
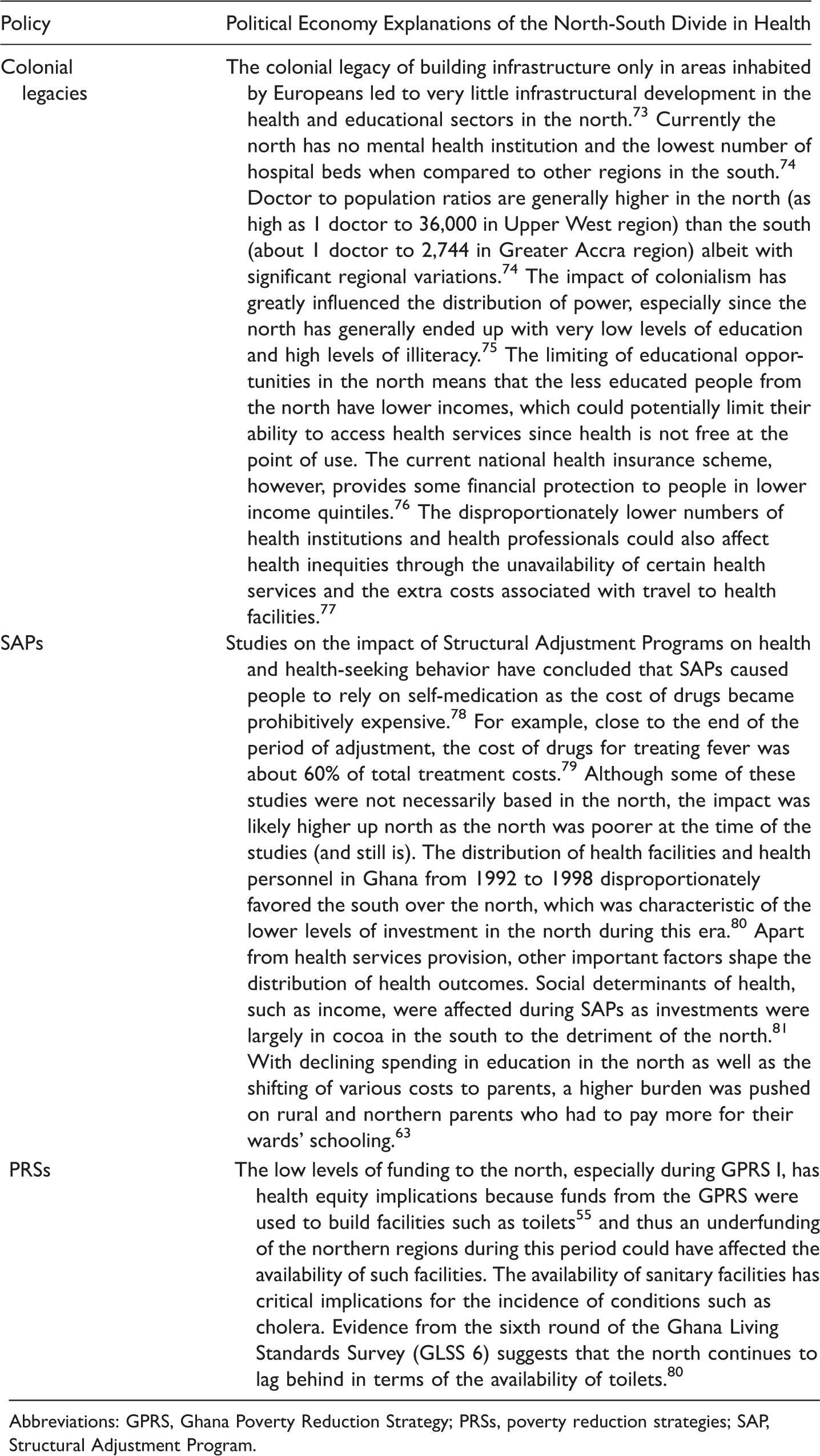
Abbreviations: GPRS, Ghana Poverty Reduction Strategy; PRSs, poverty reduction strategies; SAP, Structural Adjustment Program.
As we did previously for England, in the sections that follow, we explore some of the public policies and political choices that are relevant for understanding Ghana’s north-south health divide. Explaining social inequities in Ghana can be contentious. Indeed, some have emphasized unfavorable climatic conditions as a sufficient explanation for inequities, although some literature exists to dispel such “bad geography arguments.”55(pp28–31)
From Colonialization to Structural Adjustment Policies
European settler colonialism lay a crucial foundation for contemporary socioeconomic differences between the north and south of Ghana.
56
Colonial governments did not find northern resources (e.g., cotton) useful and thus discouraged – through uneven government investment and malicious competition – the development of such resources. This was aimed at producing a proletariat who would serve as cheap labor to advance the capitalist interests of the colonial economy.57,58 Perhaps the most succinct description of the sentiments and agenda of the colonists towards northern Ghanaians comes from a colonial report describing northerners as: [A] n amiable but backward people useful [only] as soldiers, policemen, and laborers in the mines and cocoa farms, in short, to be hewers of wood and drawers of water for their brothers in the colony and Ashanti.59(p375)
Postcolonial governments generally followed the trend of northern neglect and underinvestment described earlier. In the era of World Bank and International Monetary Fund (IMF) Structural Adjustment Programs (SAPs), known in Ghana as Economic Recovery Programs (ERPs), various governments pursued political choices that exacerbated the vulnerability of the north and deepened the north-south divide.62,63 (SAPs were a set of programs that sought to restructure the economies of countries in the developing world or in transition, mainly by advocating cuts in public spending and sale of public assets as a means of ensuring economic growth. Ghana was considered a “star pupil” because of its strict adherence to SAP recommendations. 64 )
Ghana adopted SAPs between 1983 and 1998 in a desperate attempt to salvage a moribund economy and to escape the economic decline of the 1970s. A profound result of the austerity measures associated with the SAP-era cuts in education and health was the disproportionate impact on the north compared to the south.63,65 In this period, government expenditure on health (as a proportion of total expenditure) fell from 10% in 1982 to a paltry 1.3% in 1997. 66 The introduction of hospital user fees also led to a 25%–50% fall in hospital visits in urban areas in the country and a 45%–80% fall in hospital visits in rural areas. 63 The paucity of data makes it difficult to know the exact north-south difference in falls in hospital visits. However, given that the northernmost regions were less than 20% urbanized compared to about 80% urbanization in the Greater Accra region, with over 20% urbanization in 5 of the southern regions, 67 it is reasonable to assume that these drops in hospital visits disproportionately affected the north compared to the south.
While education generally remained free during this period, the cost of “books, furniture, and other supplies” kept children in the north and other areas with high deprivation in the country from going to school.63(p475) Government spending within the period (e.g., in the 1990s) was also detrimental to the north, such that while the north accounted for 19% of the population, only 11.6% of government spending on education went to the north. 62
Ghana Poverty Reduction Strategy I and Growth and Poverty Reduction Strategy II
After the SAPs came Poverty Reduction Strategies (PRSs). With these programs (which occurred in other low- and middle-income countries as well), countries typically produced plans to show how International Monetary Fund (IMF) allocations would be used to reduce poverty and the other deleterious impacts of IMF/World Bank-recommended SAPs, which had turned out to be nostrums – some have argued that PRSs were simply repackaged SAPs. 68
The Ghana Poverty Reduction Strategy I (GPRSI) and the Growth and Poverty Reduction Strategy II (GPRSII) were comprehensive poverty reduction strategies in Ghana in the 2000s.69,70 These strategies were created to demonstrate how debt relief from the IMF under the Heavily Indebted Poor Country (HIPC) initiative would be used to reduce poverty in the country. While the GPRS I, expressly aimed at reducing regional inequities in poverty in the country, had stated it would disburse 48% of funds to the north, only 6.8% of these funds were disbursed to the north during actual implementation. Many of the projects aimed at closing the divide never came to fruition. For example, plans under GPRS II to create a rail line to connect the north of Ghana to the south have remained in the eternal political pipeline, so that although the first railway in the country was established in 1901, 71 118 years later there is no railway in the north of Ghana. Figure 1 shows deviations between actual and expected regional expenditure during implementation of HIPC. At the planning stage it was agreed that 48% of funding would go to the 3 northern regions, 4% to Greater Accra, and another 48% for the rest of the south. 69

Deviations between actual and expected regional Highly Indebted Poor Country (HIPC) expenditures 2003–2005. Source: Based on data from Abdulai. 55 Bars to the right denote over disbursement of funds to a region relative to the planned spending. All 3 northern regions received much less than promised. (See Table 3 for names of regions.)
The reason for the deviations from the earlier poverty criteria stated in the strategy documents was because of a political choice to allocate funds according to metropolitan status, which clearly placed the north at a disadvantage as it had (and still has) only one metropolitan assembly in the Northern Region. (Local government in Ghana can be metropolitan [population of over 250,000], municipal [population of over 95,000], or district [population of 75,000 and above].) A more political explanation is the power differential between the northern elite and their counterparts in the south, which constrained the northern elite from ensuring that previous poverty criteria were followed in disbursement. 72 The allocation of GPRS II did favor the north compared to the south, although in absolute terms the money and resources involved were significantly below the amounts in GPRS I. 72
Synthesis of Findings
Interrogating the North-South Divide in Health
As stated in earlier sections, although the north-south divide is a meaningful way to explain substantial geographical health differences within the 2 countries, it also has some limitations. First, for some diseases, the divide is not so evident (with some diseases actually showing a southern disadvantage). A typical example in Ghana is HIV, where rates have been lower in the north compared to the south (see Table 2). This is compatible with the political economy perspective described earlier, because the factors that drive HIV infection do not only reside with the poor but are very context-specific, depending on several other social characteristics. 83
Further, a binary (north-south) way of thinking about health inequities in both countries is challenged by living conditions of some population groups within the supposedly wealthy parts of both countries. A case in point in relation to England was the tragedy of Grenfell tower, which is located in the wealthiest borough in London and yet whose casualties lived in unbelievable squalor. 84 An equally good example of this in Ghana is that of people in the informal sector in Accra (in the south) most of whom suffer extreme hardship and in some cases forced relocations. 85
Differences and Similarities
Looking at similarities and difference in both countries, an important difference in both countries comes from history. The historical explanations of health inequities in Ghana and England differ when one considers colonization and deindustrialization. In England, deindustrialization played a crucial role in creating a new sort of economy in which the north was likely to lose – i.e., financialization increased and old industrial areas in the north declined. 27 In Ghana, colonialization led to a similar north-south divide by creating an economy in which people from the north would necessarily have to be the uneducated proletariat offering cheap labor.56,57 In both cases, livelihoods and health of people in the disadvantaged regions were affected with implications for health equity. While the impacts of the 2 policies have been similar, the policies themselves are different, and this is noteworthy.
Several similarities emerged from the review. In England, central government spending on different infrastructure has been significantly lower in the north than in the south. In transportation, e.g., comparisons of per capita government expenditure indicate that the north of England would have received an extra £59 billion had the government spent proportionately in northern England as in London or an extra £10 billion if it spent the U.K. average in the north of England. 51 In addition to the lower education spending in the north, the north is underfunded in other sectors. Households in London receive more housing benefits, tax credits, and child benefits compared to the north and indeed the rest of the country. They also receive extra “benefits in kind” in per capita terms on bus travel subsidy (£90), rail travel subsidy (£50), housing subsidy (£30), and school meals and healthy start vouchers (£20). 86 These spending differentials negatively affect the economic potential of the north and also lead to London sucking the “best and brightest” from the north through migration. The policy decisions described can have impacts on various social determinants of health with implications for health equity.
Government underspending has had essentially similar if not the same effects on north-south social and health inequities in Ghana. Spending during GPRS I neglected the north. A similar and perhaps more tragic example of the disproportionately low infrastructural spending, particularly in transportation in the north of Ghana, is the 118 years of no rail transport in the north of Ghana noted earlier. 71 What these macrosocial defects in policy have meant for the north of Ghana is also very similar to the case of England: the “best and brightest” in northern Ghana move to the south, and many professionals such as teachers and doctors refuse posting to the north mainly because of the poor infrastructural development.87,88 Northern schools remain in conditions of disrepair with few teachers, low enrollment rates, high dropout rates, and poor performance. 89 The young men and women who try to escape these unfavorable conditions and move to the south end up in menial jobs, which perpetuates the cycle of poverty and health inequity. 90
Austerity-related policies have also disproportionately affected the northern parts of both countries. Post-2010 austerity measures in England disproportionately impacted the poor with 10% of the net household income lost among the poorest decile, women, the disabled, larger families, and the unemployed compared to everyone else. 38 The distinct geography of such cuts has meant a disproportionately affected north as noted earlier, and this has important implications for health and well-being of people in the north.
In the case of Ghana, the SAPs era laid a solid foundation for future austerity in the country. 65 The cuts of the period had disproportionately negative effects on the north, although more rigorous research needs to be conducted to understand the nature and magnitude of such effects and, more importantly, the contemporary implications of such effects on health, given current knowledge from life course epidemiology. More recently the government of Ghana has had to implement more austerity measures in light of a $1 billion loan, 91 although data on the geography of such cuts are not always available. Table 5 provides a summary of the thematic similarities and differences in terms of explanations of the north-south health divides in both countries.
Summary of Similarities and Differences.

Abbreviations: GPRS, Ghana Poverty Reduction Strategy; SAP, Structural Adjustment Program.
Discussion
The political economy of health offers an excellent opportunity to think about the connections between politics and health beyond medical explanations. Although considerable research has been conducted on politics and health in England to explain how politics is implicated in north-south health inequalities in England, 4 a paucity of research remains on politics and health in Ghana. The approach and rationale adopted in our review is similar to Chabrol et al., 92 who use France and Cameroon to demonstrate the “pharmaceuticalization of health systems” in the context of austerity policies. Such comparisons of distinct settings are useful, as they show the specific contextually situated and historically relevant factors necessary for responding to the challenge of health inequities in different parts of the world. Our review demonstrates the complex relationship between place and health and the important role of political context in shaping people’s health and life chances. As demonstrated from our review, while there are challenges with conducting such comparisons, the impacts of government spending and the differential impacts of austerity policies on people depending on where they live can be quite profound. Our review also shows that while public policies (which may not necessarily be health policies) can be manifestly different in different settings, if they are underpinned by a logic of neglect of specific parts of a country, they can increase intra-country health inequities.
Additionally, we note the paucity of research connecting history (colonialism) and health in settings such as Ghana, where the current geography of various socioeconomic inequalities mirrors colonial policies of neglect of certain parts of the country. This calls for more research on the contemporary health relevance of colonialism in Africa, particularly as such research exists in other contexts (such as Canada, the United States, New Zealand, and Australia)93,94 and has shown that colonialism explains some contemporary health inequities.
Conclusion
Our review has revealed a number of issues on the relationships between politics and health in the context of distinct geographic settings. While a north-south health divide exists in both countries, a binary categorization can be problematic because some diseases do not follow a clear divide and some people living in the southern parts of both countries suffer significant health disadvantages too. Uneven government spending and uneven impacts of austerity both demonstrate the implications of political choices and public policies on health inequities in both countries.
Our review also provides a picture of the complexity of the politics of health: in acting on the recommendations of the WHO’s Commission on Social Determinants of Health, countries need to pay attention to historical context, which in many cases underpins contemporary social relations. This focus would allow for a deeper understanding of structural root causes of health inequities and could offer insights on how to better distribute resources within society. Future research could focus on comparing other extremely different settings to investigate difference and similarities between political drivers of health inequities in different countries in order to propose policy interventions for reducing health inequities.
Finally, we note the crucial role of history (colonialism) in explaining health inequities in Ghana and the need for more political economy of health research in African settings with a colonial past.
Footnotes
Acknowledgment
The authors wish to thank Professor Ted Schrecker for his comments on earlier versions of this manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.