
Abstract
The KORUS FTA includes various clauses on marketing approval of new medicines and their reimbursement decisions. We aim to capture the availability of new medicines, to measure drug lags for new medicines, and to demonstrate the effect of the KORUS FTA on the timely availability of new medicines in the Korean market. We selected new drug applications approved in the United States between 2007 and 2015, calculated the drug lag, which was defined as the time difference between the date of regulatory approval in the United States and in Korea, and constructed a logistic and Cox model to capture the effect of the variables of interest on the availability and drug lag of new medicines in the Korean market. The FDA in the United States approved 160 NDAs between 2007 and 2015. The KORUS FTA does not increase the availability of new medicines or shorten the drug lag of new medicines. However, the presence of the manufacturer in Korea was significantly related to the availability and drug lag in the Korean market. It is noteworthy that the presence of the manufacturer, which is a kind of by-product of free trade in pharmaceuticals, affected drug lag.
Regulatory approval and reimbursement decisions are both critical if new medicines are to be accessible in a timely manner.1,2 Not surprisingly, from the perspective of public health, the timing of drug approvals and the date of reimbursement decisions are essential to achieving access to new medicines.2,3 The regulations relevant to the process of regulatory approval and reimbursement decisions vary across countries.2–5 Many studies have been interested in the adoption of new medicines, including pricing and reimbursement decisions, based on a health technology assessment.4,6–8 However, it should be noted that no medicines can be reimbursed or even marketed unless the regulatory agency authorizes the drug. 2
The “drug lag,” which was defined as the time differences in drug approval among countries, has been a major public concern among high-income countries.9–12 The concept of the drug lag was first noted in the 1970s by Wardell10,11 and discussed mainly in the United States and European countries.13,14 Recently, drug delay appears to be a major public concern in high-income countries other than the United States and European countries.15–17 For instance, Japanese colleagues have continuously reported drug delays in their market. Notably, the median approval lag for new drugs approved between 1999 and 2007 in Japan was 41 months when compared with the United States and the European Union. 16 However, little is known about the South Korean (Korean) market. Specifically, empirical studies that measure the drug lag and predict the factors affecting the drug lag are absent.
Brief Sketch of the Korean Pharmaceutical Market
The Korean government established the National Health Insurance (NHI) system in 1989 and has successfully expanded the NHI system, including pharmaceuticals. 18 In 2007, the government introduced a positive list system for drugs to be reimbursed under the NHI system and adopted health technology assessment for reimbursement decisions for new medicines. 2 Accordingly, the Ministry of Food and Drug Safety (MFDS) in Korea approves medicines based on data regarding the safety and efficacy of the drug. After the MFDS approves the drug, the manufacturer voluntarily applies for reimbursement under the NHI system. 2 Being reimbursed under the NHI system is essential for manufacturers to successfully expand the market in Korea. Additionally, the pharmaceutical market in Korea represented 1.5% of the global market and was the 13th largest in the world in 2016, indicating that the market is attractive from the perspective of sales and market size. 19 As of October 2019, more than 80 global pharmaceutical companies have entered the Korean market. Meanwhile, the Korean government signed and implemented the Korea–United States Free Trade Agreements (KORUS FTA) in 2007 and 2012, respectively. The KORUS FTA includes various clauses on intellectual property and pharmaceutical affairs, such as marketing approval and reimbursement decisions,20–22 Therefore, it is necessary to evaluate the effect of the KORUS FTA on the drug lag.
This study aims to capture the availability of new medicines, to measure drug lags for new medicines, and to demonstrate the effect of the KORUS FTA on the timely availability of new medicines in the Korean market. We selected new drug applications approved in the United States between 2007 and 2015, calculated the drug lag, which was defined as the time difference between the date of regulatory approval in the United States and in Korea, and addressed various factors affecting the timely availability of new medicines in the Korean market.
Methods
Subjects
The new drug application (NDA) classification code provides a way of categorizing NDAs submitted to the U.S. Food and Drug Administration (FDA). The FDA tentatively assigns an NDA classification code, including 10 types, at the filing date (see www.accessdata.fda.gov/scripts/cder/daf/index.cfm?event=reportsSearch.process&rptName=2&reportSelectMonth=9&reportSelectYear=2018&nav#navigation). A type 1 NDA is for a drug that contains a new molecular entity (NME). An NME is an active ingredient that contains no active moiety previously approved by the FDA. 23 Building on this classification, we defined type 1 NDAs as new medicines. Specifically, we selected NDAs that were assigned to the type 1 NDAs from 2007 to 2015 and retrieved the date of drug approval by the FDA. Note that we excluded the following NDAs: NDAs withdrawn from the market; NDAs not for therapeutic use, such as those for diagnostic purposes; and NDAs not for oral use or injection (Figure 1). Then, we searched the availability and approval dates of the eligible ingredient in Korea. Similar to the FDA, the MFDS provides information about approved medicines, including the drug name, the active ingredient, the approval date, and the manufacturer (see https://nedrug.mfds.go.kr/searchDrug). Accordingly, we retrieved the 2 dependent variables: the availability of new medicines in Korea and the drug lag between the U.S. and the Korean market.
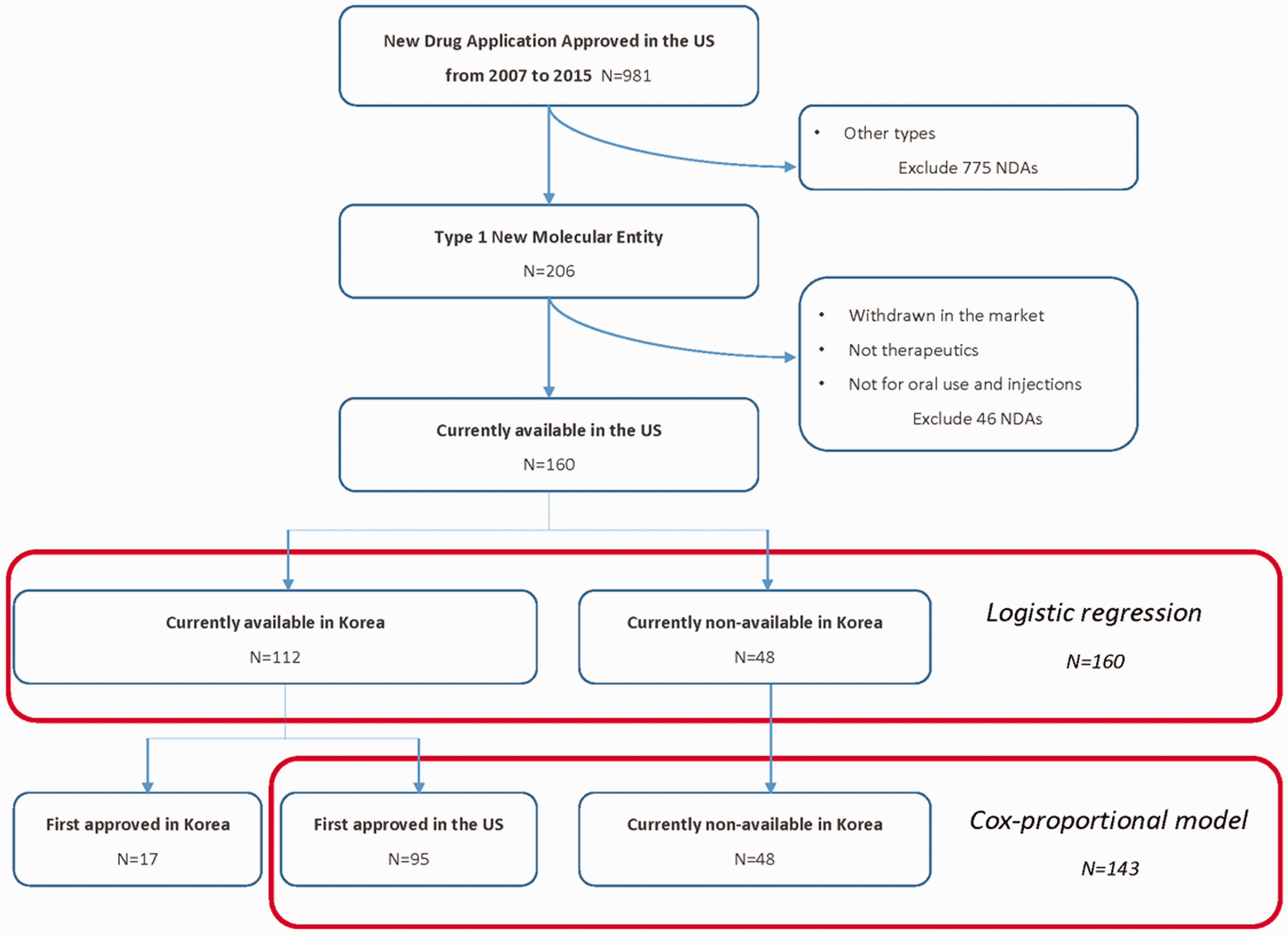
Sampling process for this study. NDA, new drug application.
Statistical Models
We constructed 2 models for the analysis: a logistic and Cox model. First, we provided the logistic regression to analyze the availability of new medicines in the Korean market. In this study, we separated the subjects into 2 groups: available and not available in Korea as of November 2018. Additionally, we included other criteria, such as the availability of new medicines after 2½ years from the date of approval in the United States, to adjust the time difference. Second, we are interested in the timely availability of new medicines in Korea. Therefore, we calculated the drug lag between the United States and Korea, and applied an event history model for a statistical estimation. However, it should be noted that drug lag is sometimes negative. This means that there are few medicines that were approved first in Korea and then approved in the United States. In this study, we excluded the subjects with a negative drug lag. Data management and analysis were performed using R statistical software (version 3.4.1). Statistical significance was defined as P values under .05.
Variables in the Model
We added a set of explanatory variables with various levels in the models: the characteristics of NDAs submitted in the United States, manufacturers in Korea, and time period.
First, we identified characteristics of the NDAs that were approved in the United States. We collected information on the route of the drug and the category of the Anatomical Therapeutic Chemical (ATC) classification system and review of the drug in the United States, such as standard review and priority review. Priority review indicates that drugs would be significant in the safety or effectiveness of the treatment, diagnosis, or prevention of serious diseases when compared to standard review. Specifically, significant improvement may be demonstrated by evidence of increased effectiveness and substantial reduction of a treatment-limiting drug reactions. 24 In this study, we used the variable of priority review as the proxy of therapeutic value of new drugs. Similarly, we identified the orphan status of the drug in the United States. We used the orphan drug product designation dataset provided by the FDA to note that if NDAs were designated as orphan drugs in the United States (see www.accessdata.fda.gov/scripts/opdlisting/oopd/). We assumed that the characteristics of new drugs, including the ATC classification, the designation as priority reviewed drugs and orphan drugs, and the route of the drug would affect the availability of the drug in the Korean market.
Second, we added the manufacturer variable. Specifically, we used the dataset provided by the Ministry of Trade Industrial and Energy to determine whether the manufacturers of the NDAs in the United States are present in the Korean market (see www.motie.go.kr/motie/py/sa/companyGuide/companyguide.jsp). Notably, we assumed that the presence of manufacturers in the Korean market would increase the likelihood of availability of new medicines and shorten the drug lag.
Finally, we added the period variable in the models: 2007–2011 and 2012–2015. In 2007, the Korean government adopted health technology assessments for reimbursement decisions for new medicines and then introduced a positive list system. 2 Therefore, we excluded NDAs approved in the United States before 2007. The KORUS FTA was conceived in 2007 and implemented in 2012. Accordingly, the period was divided into before the KORUS FTA and after the KORUS FTA. We assumed that the KORUS FTA, which was implemented in 2012, affected the availability and drug lag of new medicines in the Korean market.
Results
Characteristics of the Subjects
The FDA approved 160 NDAs in the United States between 2007 and 2015. First, we divided the NDAs according to the status of their market approval in Korea as of November 2018: available in Korea and not available in Korea. We subdivided the available NDAs in Korea into 2 groups: NDAs that were first approved in Korea and then approved in the United States, and NDAs that were first approved in the United States and then approved in Korea.
Table 1 presents descriptive statistics of the eligible drugs used in this study. Among 160 new drugs approved in the United States, 112 NDAs (70%) were also approved by the MFDS in Korea, while 48 new drugs (30%) are not currently available in the Korean market. We are interested in the order of the timing of the market approval for the 112 NDAs that were approved in both countries. Not surprisingly, 95 NDAs (85%) were approved in the United States and then approved in Korea, while 17 NDAs (15%) were approved in Korea, and then approved in the United States.
Characteristics of the Selected NDAs Approved by the FDA in the United States.
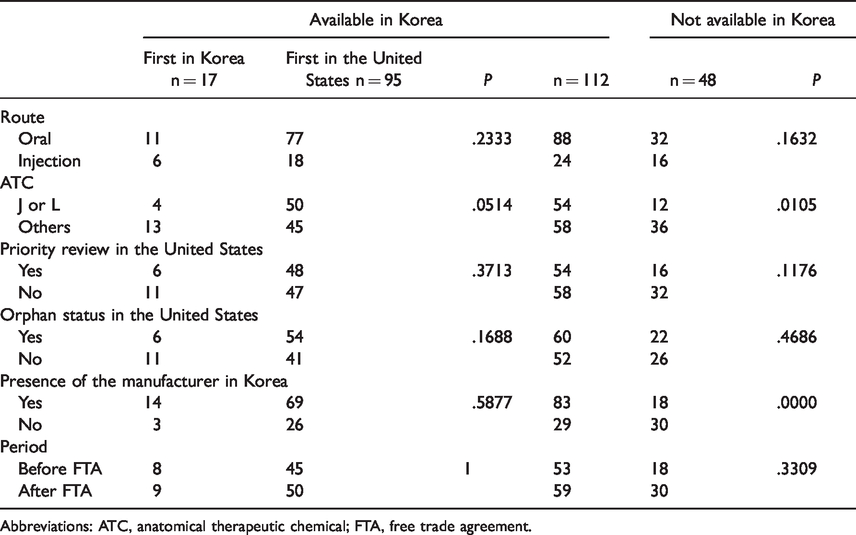
Abbreviations: ATC, anatomical therapeutic chemical; FTA, free trade agreement.
We performed a chi-square test to analyze the differences in the variables of interest among the separated groups. Interestingly, differences in the presence of the manufacturer in Korea and the ATC classification were captured among the groups: drugs available in Korea and drugs not available in Korea. However, the results were not consistent in the other groups: drugs first approved in the United States and drugs first approved in Korea.
In Table 2, we calculated the drug lag, which was sorted by the year of the NDA approval in the United States. For instance, 11 NDAs were approved in the United States in 2007. Among these medicines, 8 NDAs were approved earlier in the United States, including NDAs that have not been approved in Korea, while 3 NDAs were marketed faster in Korea. The mean time of the drug lag for 8 NDAs that were approved earlier in the United States was 5.84 years in 2007. However, it should be noted that these observations are right censored. Some drugs that have not been approved in Korea would be approved over time. Thus, we calculated the drug lag for NDAs that were also approved in Korea. We found that the mean time of the drug lag for 7 NDAs, excluding 1 NDA that was not approved in Korea, was 5.01 years in 2007. Similarly, we calculated different types of drug lags in 2015. It was 2.16 years for all 25 NDAs approved earlier in the United States and 0.98 years for 12 NDAs excluding NDAs that have not been approved in Korea. Furthermore, we performed a Cochrane-Armitage trend test to investigate the relationship between the variables, including the approval year in the United States and the availability of new medicines after 2½ years from the date of approval in the United States. Interestingly, the approval year is significantly related to the availablity of new medicines within 2½ years (P = .03893).
Duration of the Approval Date Between the United States and Korea, Sorted by the Year of NDA Approval, as of 2018.

Abbreviations: FTA, free trade agreement; NDA, new drug application; SD, standard deviation.
The Logistic and Cox Model
Table 3 provides the results of the logistic models. Various logistic regressions were conducted to address factors that affected the availability of new medicines in Korea. First, we fitted the simplest model with 4 factors at the NDA level: the route of the medicine, category of the ATC classification of the medicine, review type, and orphan status of the medicines in the United States. Second, we added 2 factors related to manufacturers and time in the expanded model. Specifically, we added variables regarding the presence of the manufacturer in Korea and the time period, including before the FTA and after the FTA. Medicines belonging to the ATC J or L (reference_others) in both models and the presence of the manufacturers (reference_non presence) in the expanded model were positively associated with being available in the Korean market. Interestingly, the period after the FTA (reference before the FTA) was not significantly related to the marketing of the drug in the expanded model.
Results for the Effect From the Logistic Model.

Abbreviations: ATC, anatomical therapeutic chemical; FTA, free trade agreement.
Second, we changed the dependent variable to adjust the time difference from the availability of new medicines in Korea to the availability of new medicines after 2½ years from the date of approval in the United States. In this model, we found consistent results for the variables of the ATC classification and the presence of the manufacturer in Korean. Additionally, we found that medicines for injection (reference oral use) were negatively related to the availability of the drug in the Korean market within 2½ years from the date of approval in the United States.
We also applied the Cox model. Figure 2 provides a descriptive overview of the drug lag of new medicines, approved earlier in the United States (n = 143), using Kaplan–Meier estimates. The first graph in Figure 2 presents a curve without group comparison, while the remaining graphs in Figure 2 offer a curve with group comparison, including the presence of the manufacturer in Korea, the ATC classification, the period, the route of the drug, and the review type in the United States. The survival difference was found in the group of review types in the United States (P = .0392), the presence of the manufacturer in Korea (P < .0001), the route of the drug (P = .0209), and the ATC classification (P = .0006).
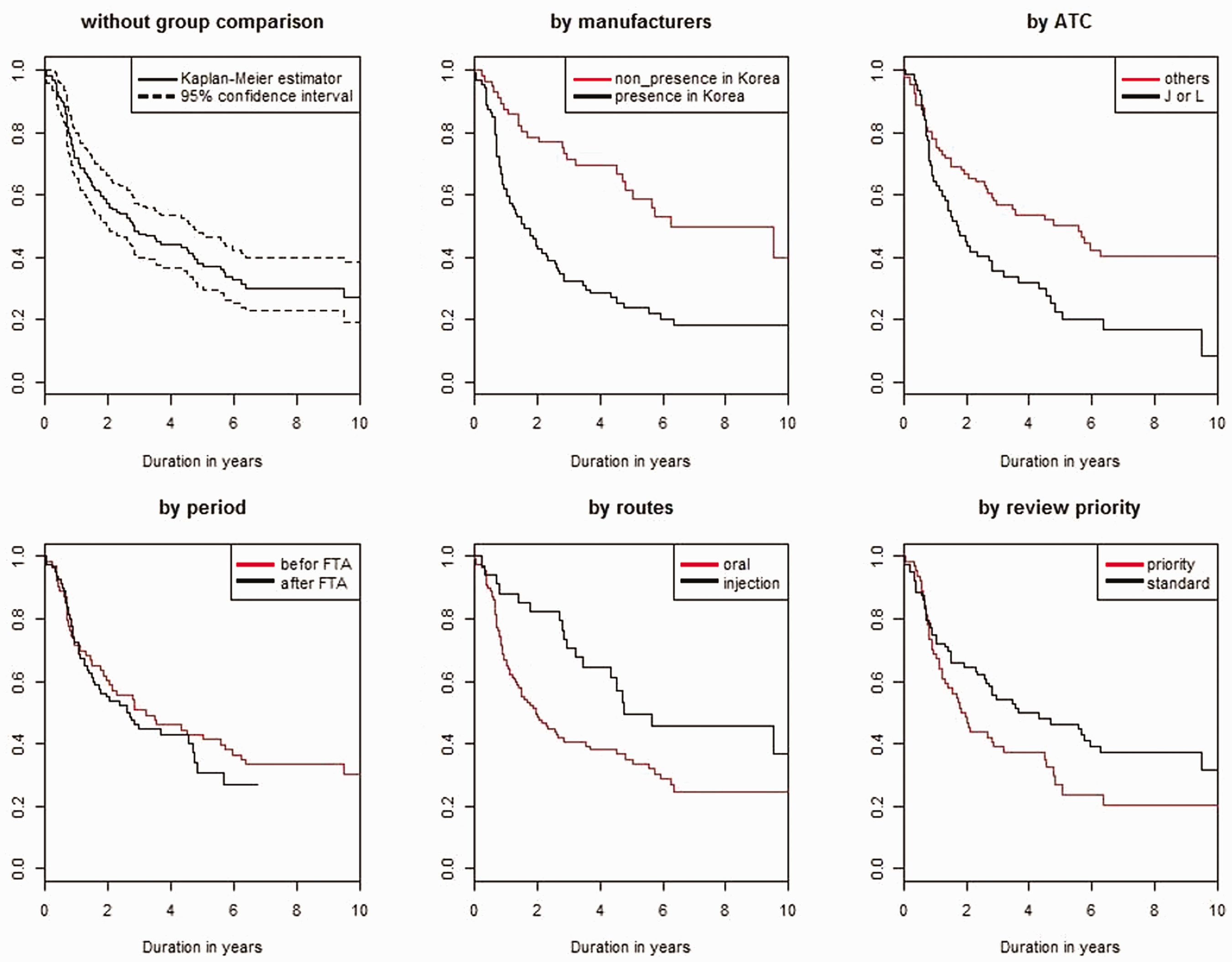
Kaplan–Meier estimates for the duration. ATC, anatomical therapeutic chemical; FTA, free trade agreement.
As the Kaplan–Meier estimates are a univariate tool, we also applied the proportional hazards model as a multivariate approach in Table 4. As we already performed in the logistic regression, we fitted the Cox model with 6 factors. Note that a positive coefficient means a short drug delay, while a negative coefficient means a long drug delay in Korea. In line with the results of the logistic regression, the presence of the manufacturer (reference_non presence) in Korea and medicines belonging to the ATC J or L (reference_others) accelerated the time to approval in Korea compared to the reference. Interestingly, medicines for injection (reference_oral) significantly delayed the marketing of the drug in Korea. Additionally, we added 6 medicines that were first approved in Korea and then approved in the United States within one year in the other model assuming that there have been no drug lags for these medicines. We found the consistent results in this model.
Results for the Effect From the Cox Model.

Discussion
No medicine can be marketed or reimbursed unless the regulatory agency authorizes the drug. Therefore, decreased “drug lag” is essential for new drugs to be accessible in a timely manner. We aim to capture the availability of new medicines, to measure drug lags for new medicines, and to demonstrate various factors, including free trade agreements, affecting the timely availability of new medicines in the Korean market.
The Concept of Drug Lag
As already explained, drug lag was defined as the time differences in drug approval among countries. It is also well documented that drug lag is influenced by several factors, including the product and its therapeutic area and value, the manufacturer and its strategy, quality of submissions from manufacturers, and review process that agency provides. 25
Drug lag could be separated into submission gap and review gap. 5 The former is closely related with strategic behavior of manufacturers, while the latter is influenced by the drug regulatory system. Manufacturers tend to file first in larger markets or markets where they could obtain high profits or higher prices to avoid the problem of the reference pricing in other countries. Similarly, small market size might deter manufacturers from incurring the cost associated with trying to get a new drug approved. Furthermore, review period in various regulatory systems are different. For instance, the FDA aims to take action on an NDA within 6 months and 10 months for priority review and standard review, 24 respectively, and the MFDS in Korea requires at least 120 days to review and approve new drug. 26 Note that if a request for supplementation of data is made, the review period will be extended in Korea. 26
The date of submission to a regulatory agency includes useful information in understanding drug lag. For instance, the Center for Innovation in Regulatory Science analyzed approval time, which is calculated from the date of submission to the date of approval by the agency, for 6 regulatory authorities in 2008–2017, and the submission gap between European Medicines Agency (EMA) and the FDA for new drugs approved in 2014–2016. However, the date of submission to the MFDS in Korea is not publicly available data. Thus, we measured drug lag in the Korean market as the time difference between the date of regulatory approval in the United States and Korea, indicating that we could not separate submission gap or review gap from drug lag in this study.
Summary of Findings
There are some interesting findings in this study. First, a number of new medicines (30%) approved in the Unites States are not currently available in the Korean market. Some variables, including the presence of the manufacturer in Korea and the ATC classification, were significantly related to the marketing of new medicines in Korea.
Second, we calculated the 2 different drug lags between the United States and Korea. On the one hand, we presented drug lags for new medicines that were approved earlier in the United States, including right-censored observations. On the other hand, we calculated drug lags for new medicines excluding new medicines that were not approved in Korea. We found that both median drug lags decreased: the median drug lag, including right-censored observations, ranged from 5.68 years in 2007 to 2.86 years in 2015, and the median drug lag, excluding right-censored observations, ranged from 1.84 years in 2007 to 0.70 years in 2015. We also found that the approval year is significantly related to the availability of new medicines within 2½ years.
It was well reported that drug lag among high- and middle-income countries has decreased over time.5,16,27 Our observations, which include updated data, are consistent with previous studies.5,16 For instance, Wileman and Mishra calculated drug lag in several middle-income countries compared with the United States from the 1960s to the 2000s. Notably, median drug lags decreased from 21.49 years in the 1960s to 1.53 years in the 2000s. 5 The authors separated drug lag into submission gap and review gap and explained the decreased drug lag as being the result of the rapid reduction in submission gap conducted by pharmaceutical companies that have commercial interests in these countries. 5 However, it should be also noted that approval time in a certain country, which is closely related with review gap, have notably decreased. For instance, median approval time for new active substance in Japan, particularly the Japan Pharmaceuticals and Medical Devices Agency (PMDA), was decreased from more than 600 days in 2009 to 300 days in 2017. 25
Similarly, Tsuji and Tsutani evaluated the drug lag of 398 new drugs that were approved between 1999 and 2007 in the United States, the European Union, or Japan. Not surprisingly, 82% of these drugs were approved in the United States, 79% in the European Union, and 55% in Japan. 16 Furthermore the median approval lag for the United States, the European Union, and Japan was 0 months, 0.23 years, and 3.42 years, respectively. 16 However, Maeda and Kurokawa argued that the drug lag of new medicines approved in Japan between 2001 and 2014 has significantly decreased to less than one year. 27
Third, we addressed various factors affecting the timely availability of new medicines in Korea. Interestingly, the KORUS FTA, which is the main interest of this research, does not increase the availability of new medicines or shorten the drug lag of new medicines. However, the presence of the manufacturer in Korea was significantly related to availability and drug lag in the Korean market. Given these observations, we can conclude that the free trade agreement itself does not affect availability and drug lag. On the other hand, the presence of manufacturers, which is a kind of by-product of free trade in pharmaceuticals, affects access to new medicines. For instance, many foreign manufacturers of the NDAs in the United States entered the Korean market before 2012 when the KORUS FTA was implemented. Therefore, we cannot capture the effect of the KORUS FTA with regard to drug lag. This finding is consistent with the previous study, presenting that a new medicine developed by a bigger company might be more likely to become internationalized beyond the first country of submission. 25
We also found that new medicines belonging to ATC J or L (reference_others) presented a significant likelihood of availability and shortened drug lag in our models: the logistic and Cox model. This finding is interesting when compared with the results of the previous studies. For instance, Son (2018) demonstrated that new medicines belonging to ATC J or L significantly delayed the duration between regulatory approval and reimbursement decision in Korea. 2 Specifically, the author argued that ATC J or L medicines require the Health Insurance Review and Assessment Service (HIRA) to prolong the time taken to evaluate the submitted dossiers and to make a favorable decision on reimbursement. Sometimes, the National Health Insurance Service (NHIS) might need more time to negotiate the final price of these new medicines. Given these observations, it seems that a manufacturer that wants to market new medicines belonging to ATC J or L in Korea is granted market approval earlier than other drugs. However, it took more time for these medicines to be reimbursed in the Korean market. Therefore, the shortened drug lag for ATC L or L medicines in this study might be closely related to the strategic behavior of manufacturers.
Study Limitations
This study has some limitations. First, this study is mainly interested in the date of marketing approval in the United States and Korea. Thus, we cannot comprehensively cover information on reimbursement decisions or the utilization of eligible drugs. However, it should be noted that marketing authorization is the first step when new medicines are to be accessible in a timely manner for patients. Second, drug lag is only relevant when new drug representing a significant therapeutic improvement over existing products are delayed. However, this study does not utilize information on clinical effectiveness, efficacy, or disease severity. Instead, we used the variable of priority review as the proxy of therapeutic value of new drugs, indicating that therapeutic value of new drugs would be needed to understand access to needed medicines in depth. Last but not least, information on the date of submission by manufacturers to the MFDS in Korea was not available in this study. Thus, we could not account for submission gap and review gap in drug lags in the Korean market compared to the Unites States.
Conclusions
Decreased drug lag is essential for new medicines to be accessible in a timely manner. Our study provided evidence of the KORUS FTA on drug lags of new medicines in Korea. We confirmed that drug lag in Korea has decreased over time, which is similar to other high- and middle-income countries. However, we cannot capture the effect of the KORUS FTA, which is the main interest of this study, with regard to drug lag in the Korean market. It is noteworthy that the presence of the manufacturer, which is a kind of by-product of free trade in pharmaceuticals, affected drug lag. Furthermore, drug lag is closely related to other pharmaceutical policies, including pricing and reimbursement decisions. The shortened drug lag of cancer drugs in Korea reflects the strategic behaviors of manufacturers that have commercial interests in the market. For instance, considering delayed duration between regulatory approval and reimbursement decisions for cancer drugs in Korea, manufacturers applied for regulatory approvals for cancer drugs earlier than other drugs.
Supplemental Material
JOH898335 Supplemental Material - Supplemental material for Do Free Trade Agreements Matter to Drug Lag? Recent Evidence From Korea After the Korea–U.S. Free Trade Agreement
Supplemental material, JOH898335 Supplemental Material for Do Free Trade Agreements Matter to Drug Lag? Recent Evidence From Korea After the Korea–U.S. Free Trade Agreement by Kyung-Bok Son in International Journal of Health Services
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Ministry of Education of the Republic of Korea and the National Research Foundation of Korea (NRF-2019S1A5A8032445).
Author Biography
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.