
Abstract
A cross-sectional study was conducted from April 2013 until March 2014 to explore the existence of inequalities in access to and utilization of health services by migrants compared to non-migrants in Greece and to test the influence of various factors on these disparities. Also, we investigated the influence of several socioeconomic and demographic characteristics. Study population included 1,152 migrants and 702 non-migrants. Migrants, participants suffering from a chronic disease, those without health insurance, and patients who assessed their health status as not at all good/a little good/moderate were statistically more likely to report unmet needs in getting their medication. Uninsured participants, females, those unemployed or without a permanent occupational status, and those who assessed their health status as not at all good/a little good/moderate were statistically more likely to report unmet needs in access to health services during the last year. Regarding the use of health services, those with health coverage, non-migrants, and females were statistically more likely to go for a blood test as a hospital outpatient. Greece, despite administrative delays and barriers, provided full coverage to the uninsured, asylum seekers, and migrants, even many groups of undocumented migrants.
Introduction
Inequalities in health care access constitute a complex issue representing variations and disparities in the health achievements of individuals and groups. 1 Especially in the field of health services’ provision, inequalities constitute a multifaceted social problem, 2 as they are linked with the fundamental human rights and the principles of equality, social justice, solidarity, and social embodiment.3,4 Despite the fact that health outcomes, in terms of life expectancy and other indicators, have improved significantly due to advances in health technology and knowledge, increasing progress in the prevention and treatment of diseases, and improvements in social conditions, disparities yet persist.
Situation Worldwide
Currently, due to the high population mobility, especially from Africa, Asia, the Middle East, and Eastern Europe to the European Union, another aspect of social and health inequalities has emerged. This has to do with the obstacles and difficulties migrants might face in accessing the health care services of the country of their new residence as well as the quality of any services provided. The inequalities in accessing and using health care services, particularly by migrants, is well documented in the literature.5–9 According to a number of studies, although migrants might have increased health needs due to their exposure to a number of health risks before, during, and after their journey, they face significant disparities related to access, use, and quality of social and health services.10–12
In general, migrants appear to have worse health outcomes than the native population of a country in a number of dimensions, such as emergency hospital admissions and the development of chronic conditions such as diabetes and heart disease,9,13 even though, upon on their arrival, they may be healthier than the native population, especially in terms of chronic diseases (healthy migrant effect). In addition to differences in objective outcomes, they rank lower in subjective health outcome measures, with lower self-perceived health status than the native population.14,15
The increasing number of migrants and the challenges posed to the health care systems of the receiving countries, including Greece, have led to a growing literature in the last decade on the challenges faced by this population.2,4,8,16,17 As the up-to-date research has shown, restrictive laws, lack of information, administrative, organizational, institutional barriers, and discriminatory barriers can decisively limit access to health care services for migrants and refugees, while, at the same time, the health of this population is compromised by unhealthy living conditions in the country of migration.18–24
Additionally, health insurance is considered to be one of the most significant factors affecting access to health care services for both migrants and non-migrants. As migrants often lack health insurance protection as well as lack of information about programs which may provide access to health care service as a “safety net,”25,26 they are more vulnerable to such restrictive barriers in accessing health care services. Therefore, health insurance coverage has been used as a proxy of health protection for a population. 27 Also, migrants may have a different disease profile, different socioeconomic and cultural characteristics, and a different perspective on how to cover those needs compared to the native population, and this imposes an additional challenge on a health system with regard to managing the needs of this vulnerable group.
Situation in Greece
Although Greece has been traditionally a country of economic workers migrating to wealthier countries, since the early 1990s it has transformed into a country that has been receiving migrants mainly from the Balkans. According to 2011 census, 912,000 migrants were estimated to be living in Greece, constituting 8.5% of the population; however, this number is considered an underestimation, as it does not include the majority of the undocumented migrants. 28
In recent years, however, migration patterns have changed. Due to the country’s geographical position, migration has become a modern social problem of various parameters, including migrants’ health and medical needs coverage. In 2015, Greece among other European countries (e.g., Italy) received extremely large immigrant and refugee influx waves. More than 857,363 immigrants and refugees reached Greece in 2015, and although there was a significant decrease of 79% in 2016, more than 176,000 migrants arrived in the country. 29 Syria, Afghanistan, and Iraq are listed as the top 3 countries of origin, based on the number of arrivals, while constant incoming flows are being observed from Pakistan and Bangladesh. 30 Greece along with Italy (181,436 arrivals during 2016) are the main arrival countries left to shoulder the bulk of the strain from the refugee crisis.
To this day, as the economic crisis has further deepened in Greece, health and social indicators have further deteriorated, especially among vulnerable population groups such as migrants. 31 Their access to fundamental rights for health care is limited; long waiting times in hospitals, bureaucracy, overcrowding in both primary and hospital facilities, inadequate infrastructure, difficulties in communicating with the health care professionals, and the high cost of health care emerge as the most important issues, although research is very limited in the field. 22 Yet, inadequate health care for migrants and refugees, due to access obstacles, poses serious threats to public health for the whole population as well as creating an environment of social exclusion and “ghettos” that endanger social cohesion. It is therefore important that conditions for adequate health care for migrants should be developed as soon as possible, but to do so, it is essential to address the problem in its real dimensions, to bring into light evidence on health care needs and the difficulties and obstacles in health care access, and to put forward specific suggestions for measures.
Policies in Greece
At the time this study was performed, access to care for the uninsured population, including migrants, was quite limited. In Greece, employment is linked with the right to access health care. In 2014, the number of employed amounted to 3.5 million persons, while the number of unemployed amounted to 1.3 million. The unemployment rate was 26.5%, and long-term unemployment was 67.1% of all unemployed. 32 Those who were unemployed for less than 12 months continued to have access to sickness benefits in kind for 1 year after the commencement of unemployment. For certain cases, after the expiry of the 1 year, a governmental organization aiming at employment advocacy (OAED) provided health coverage for up to 2 additional years. After a person had exhausted their insurance right for sickness benefits and eligibility for OAED programs, an option was available at that time to request a health voucher. The health voucher program was launched in September 2013 and targeted people who had lost their insurance coverage and allowed them access only to primary health care services. The voucher did not cover the cost of hospital care, so the scope of the measure was very limited; perhaps this explains why only a small number of vouchers were issued.
Another important reason may be the lack of information; indeed, the uninsured population (including migrants) in our study reported lack of information about the programs which at that time provided access to health care services. Similarly, a large majority of respondents in a study conducted in Athens in 201426 reported that they were not informed about their rights or the legislation passed for the health service coverage of the uninsured population. Other significant barriers in accessing health care services included the cost of the use of the services and bureaucratic procedures, as reported in the same study.
To try to overcome these problems, in June 2014, 2 ministerial decisions were issued, according to which all citizens and legal residents of Greece not covered by social health insurance, voluntary health insurance, or poverty booklets, as well as their dependents, would be covered for inpatient care (subject to referral from primary care plus approval from a hospital committee set up to certify patients’ need for hospitalization), as well as for pharmaceuticals (excluding co-payments) prescribed by an NHS (ESY) physician. Although it was expected that this measure would reduce gaps in coverage, issues were raised regarding its implementation in practice, including unaffordable co-payments for pharmaceuticals and differences in how hospitals interpreted the law. 33 Additionally, it was a rather stigmatizing procedure, given that a specific committee had to certify the need for hospitalization of the uninsured patients but not for the insured population. As a result, the uninsured who were seeking inpatient treatment faced serious unjustified administrative barriers in accessing health care.
The ineffectiveness of this second effort to ease the access of the population resulted in the amendment of the relevant legislation in 2016. 34 Finally, the new law, which is currently in effect, ensured free access to health services for uninsured citizens and legal residents, refugees, asylum seekers, as well as undocumented migrants, namely children, pregnant women, those in pain or life threatening situation, and those with chronic conditions or disabilities. They are now entitled to the same level of access as are Greek citizens as long as they have been issued a social insurance number or a migrant health care card. Undoubtedly this legislation is of key importance to improving equity and access to health care for vulnerable groups.
Yet, it should be noted that there was a remarkable delay of more than 5 years in adopting an effective reform to cover the uninsured and the poor. For more than 5 years, due to uncoordinated efforts, failure to strategically plan and support a structured policy for accessing health services, the implementation of semi-measures not succeeding in addressing the real needs of the population, and remaining administrative barriers, Greece failed to face the growing need for access to the health services by those most in need.
Aim
The objective of the present study was to explore if inequalities exist in accessing and using health services by migrants compared to non-migrants in Greece and to test the influence of various factors, including health care insurance, on any disparities identified. Also, we investigated the influence of several socioeconomic and demographic characteristics.
Materials and Methods
Study Population
As there is no consensus regarding the terminology about migrants, we partly followed the definition given by the MEHO group14 and included in our study any person who migrated to Greece from outside the EU-15 member states (i.e., the 15 E.U. member states before the expansion in 2004), while further excluding North America and Australia. Also, we followed the definition as it is published in the Glossary of Migration, 35 i.e., migrants are persons and family members moving to another country or region to better their material or social conditions and improve the prospect for themselves or their family. The migrant participants included in the study reported being documented migrants, although this information was not verified.
A cross-sectional study was conducted from April 2013 until March 2014. The study population consisted of 1,152 migrants and 702 non-migrants. An effort was made to ensure a maximum variation of the study population; therefore the study population, for both migrants and non-migrants, was from urban (Athens, Thessaloniki) but also rural areas of Greece (Creta, Lakonia, Larissa/Volos, Ioannina, and Lamia). A qualitative study 36 was conducted prior to this one to construct the questionnaire of this study. Afterwards, a pilot quantitative study was carried out to improve the reliability and the validity of the questionnaire. More information about the questionnaire development may also be found in the pilot study published. 22
Sampling Method
Regarding the sampling method, there is no accurate census of migrants residing in Greece, and thus probability or random sampling could not be used. Therefore, a convenience snowball sampling (a nonprobability sampling method) was applied. Initially, the researchers contacted key persons in migrant communities, such as their leaders or representatives. Those key persons acted as mediators between researchers and migrants to increase feelings of trust and asked everyone present in the gathering place at the time of the study if they wanted to participate. Migrants were located in social gathering places, religious places, and workplaces (mostly agricultural workers). An effort was made to have a same source population for the non-migrants; therefore, the researchers approached non-migrants in the same areas and similar places, e.g., churches, markets, squares. Migrants and non-migrants completed the questionnaire at the place where the researchers located them to improve their convenience and increase response rates. So, a convenience sample of non-migrants was achieved to be comparable with migrants.
The questionnaire was translated in all the languages of the sample population. The questionnaires were anonymous and self-completed by the migrants and non-migrants. However, migrants with a good level of Greek language proficiency facilitated the procedure as translators, in case questions were raised by the study participants. At least 1 researcher was also present during the completion of the questionnaires.
Ethics
Ethics approval for the study protocol was received from the Ethics Committee of the Department of Nursing, National and Kapodistrian University of Athens (date of approval 03/07/2013, number of approval 115). All the participants were informed comprehensively of the study protocol, and they gave their written informed consent. Participation was voluntary, and the participants completed the study questionnaires anonymously.
Questionnaire
The questionnaire included information on sociodemographic characteristics, health status, public health services knowledge, and utilization and perception of difficulties in health services access (view supplementary online material). A qualitative study 36 was conducted prior to this one and used to construct the quantitative questionnaire of our study. Following the qualitative study, a pilot quantitative study with 30 immigrants was carried out to improve the comprehensibility of the questionnaire and to test face validity. Internal consistency of the questionnaire was calculated by Cronbach’s alpha and was found equal to 0.7, which was considered acceptable. More information about the questionnaire developed may also be found in the pilot study published. 22
Sociodemographic characteristics included age, country of origin, months of stay in Greece, gender, marital status, number of children, educational level (less than high school, high school, at least some college), health insurance coverage, employment at the time of study, family monthly income, and living arrangements.
Information about health status included self-reported health status; medication use for chronic diseases; and existence of diagnosed hypertension, asthma, diabetes, cardiovascular disease, mental health diseases, sexually transmitted diseases, and diseases of the digestive system.
Public health care services knowledge was measured on a 5-point Likert-type scale (very poor, poor, moderate, good and very good), and public health services utilization included physician visits, dentist visits, visits to outpatient hospital services, use of emergency department services, and inpatient hospital care. Difficulties in public health services access was measured on a 5-point Likert-type scale (not at all, slightly, moderately, quite a bit, and extremely difficult). For statistical analysis purposes, not at all and slightly difficult were considered as one category; quite a bit and extremely difficult were also considered as one category.
Migrants answered the following additional questions: “Do you have residence permit documents for Greece?” “How would you describe your ability to understand, speak, read, and write Greek and English?” and “Do you believe that your access to public health care services is worse compared to Greeks?” To avoid confusion, the non-migrant questionnaire did not include the above questions. Also, the questionnaire was appropriately adjusted in some questions for migrants and non-migrants, e.g., the question “Do you believe that your friends in Greece are sufficiently supportive of you?” for the migrants was equal to “Do you believe that your friends are sufficiently supportive of you?” for the non-migrants.
Variables
Migrants were identified by country of birth. Access to health care, as the main outcome measure, was examined through 2 well-established measures of perceived access (dependent variables): unmet pharmaceutical needs of patients with chronic diseases and unmet medical needs for health services during the last 12 months. Both of these variables were dichotomous. Unmet health need was selected as an indicator of access to care, as it is one of the most widely used indicators and therefore easy to compare and measure. 37
Inequalities in use of health services were examined through visits to hospital outpatient services for a preventive blood test during the last 2 years. This dependent variable was also dichotomous. The variable was chosen to overcome the issue, demonstrated by a number of studies, that migrants are much less likely to use health services compared to the native population because they are in better health (healthy migrant effect).38–40 Our rationale for selecting a diagnostic hospital service was also that the use of hospital outpatient services in Greece by both native born and migrants may act as a substitute for primary preventive care services, as only very few urban health centers exist. It also represented the most affordable way to receive preventive services compared to the contracted private providers, as the co-payment for using outpatient services had been set to 5 euros at the time of the study (this fee was removed later to enhance the use of these services).
The independent variables (Table 1) associated with access to health services were nativity (migrant/non-migrant), health insurance status (yes/no answers), and other socioeconomic and demographic characteristics (age, sex [male/female], education [elementary school, junior high school, high school, vocational training diploma, higher education degree], employment status [workers/non workers], family income), and finally self-reported health status (not at all good, a little good, moderate, sufficiently good, and very good), which was used to assess the need for health services. To assess self-reported health status, a single question was asked, “In general, how would you rate your health today?” and answered on a 5-point Likert scale (with the following answers: very good, good, moderate, a little good, not at all good).
Demographic Characteristics of the Participants.
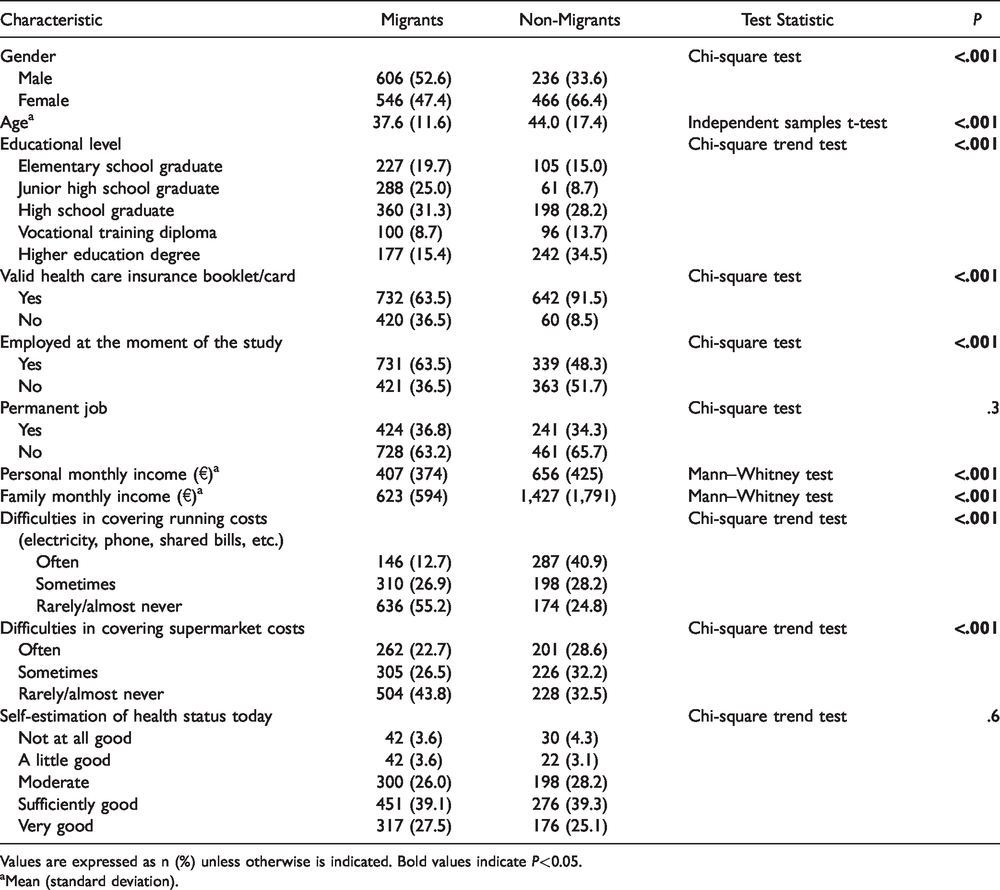
Values are expressed as n (%) unless otherwise is indicated. Bold values indicate P<0.05.
aMean (standard deviation).
The independent variables were selected based to the Andersen model, according to which health services utilization is a function of people’s predisposition to health services (e.g., age, sex), enabling resources (e.g., education, employment status), and need, as well as the characteristics of the health care system in terms of its organization, resources, and policies. 41 As migrants tend to be younger and also often socioeconomically disadvantaged compared with the native population, the risk adjustment for the abovementioned variables was considered necessary to assure comparability of data and quality of results.
During the period of the economic crisis (2010–2018) in Greece, access was reduced, due to reduced resources for health care, increased co-payments, and decreased ability of users to make formal and informal payments. 42 Therefore, economic hardship was further assessed by 2 variables associated with the inability to make payments for activities of daily life, namely difficulties shopping for everyday products at a supermarket (e.g., dairy products, vegetables, etc.) and paying for utility bills. Responses were made on a 3-point scale (with the following answers: never, sometimes, and often).
Statistical Analysis
Continuous variables are presented as mean (standard deviation), while categorical variables are presented as numbers (percentages). The Kolmogorov–Smirnov test and graphs (histograms and normal Q-Q plots) were used to test the normality of the distribution of the continuous variables. Age followed normal distribution, while personal and family monthly income did not follow normal distribution.
First, we performed bivariate analyses that included the following: chi-square test (for relation between categorical variables), chi-square trend test (for relation between nominal and ordinal variables), independent samples t-test (for relation between dichotomous and continuous variables that followed normal distribution), and Mann–Whitney test (for relation between dichotomous and continuous variables that did not follow normal distribution).
Then, independent variables with P < .20 in bivariate analyses were included in multivariate models. The backward elimination method was used for model development in multivariate logistic regression, since the dependent variables are dichotomous. Criteria for entry and removal of variables were based on the likelihood ratio test, with enter and remove limits set at P < .05 and P >.10. Multivariate analysis was applied for the control of each potentially confounding of each statistically significant factor to the others. The predictive variables were identified in terms of odds ratios with 95% confidence intervals and the respective P-values.
All tests of statistical significance were 2-tailed, and P-values of less than 0.05 were considered significant. Statistical analysis was performed using the Statistical Package for Social Sciences software (IBM Corp. Released 2012. IBM SPSS Statistics for Windows, Version 21.0. Armonk, NY: IBM Corp.).
Results
Descriptive Statistics
Demographics
In total, 1,152 migrants and 702 natives completed the questionnaire. The response rate was 60% (1,152 out of 1,920) for the migrants and 52% (702 out of 1,350) for the non-migrants. We used only the questionnaires with answers in all questions. Descriptive statistics by nativity are shown in Table 1. More than 52% of the migrants were men, and the respective figure for the non-migrants was 33.6% (P < .001), while 36.5% of the migrants and 8.5% of the non-migrants were uninsured (P < .001). The mean duration of living in Greece was 10.9 years for the migrants. Non-migrants had higher levels of education than did migrants, with >34% reporting a college degree or higher (P < .001). However, migrants were more likely than non-migrants to be currently employed (63.5% vs 48.3%, P < .001), but they reported much lower personal and family income than the non-migrants (P < .001 in both cases). Despite that, migrants reported much lower difficulties in covering recurring household expenses and costs for the supermarket compared to the non-migrants (P < .001 in both cases) (Table 1).
Unmet pharmaceutical needs
Migrants with chronic diseases had more often unmet pharmaceutical needs (55.7%) than non-migrants (22.3%). The main reasons reported by migrants for not receiving their medication were the high cost of the pharmaceuticals (co-payments and the total cost of the pharmaceuticals in case of non-insurance) (82.6%), the lack of information about the procedures needed to obtain the pharmaceuticals (7.4%), as well the perception that the pharmaceuticals prescribed were not really needed (9.5%).
Unmet medical needs and prevention services
Also, the main barriers reported by migrants in the use of outpatient health care services were bureaucratic procedures (43.8%) and the cost of using such services (47.9%). Moreover, unmet needs for health services during the last 12 months were almost equal for migrants (21%) and non-migrants (23.6%), while migrants had more often had a blood test during the last 24 months than non-migrants (86.6% vs 68.9%).
Bivariate and Multivariate Analysis
As mentioned in methods, nativity (migrant/non-migrant), health insurance status, and other socioeconomic and demographic characteristics were used as independent variables in the following bivariate and multivariate analysis.
Unmet pharmaceutical needs
Migrants more often had unmet pharmaceutical needs than non-migrants (55.7% vs 22.3%). Bivariate analysis for unmet pharmaceutical needs of patients with chronic diseases is shown in Table 2, while multivariate logistic regression analysis is shown in Table 3. Patients suffering from a chronic disease without health insurance (odds ratio [OR] = 3.4, 95% confidence interval [CI] = 1.87 to 6.20), migrants (OR = 2.41, 95% CI = 1.41 to 4.11), and patients who assessed their health status as not at all good/little good/moderate (OR = 1.71, 95% CI = 1.03 to 2.85) were more likely to report unmet needs in getting their medications. Also, reduced monthly family income was associated with an increased percentage of not taking medication for chronic disease (P < .001 for trend test). The above variables explain 34% of variance in the dependent variable.
Bivariate Analysis Between Independent Variables and Unmet Pharmaceutical Needs of Patients With Chronic Diseases, Unmet Medical Needs for Health Services During the Last 12 Months, and Performance of a Blood Test During the Last 24 Months.
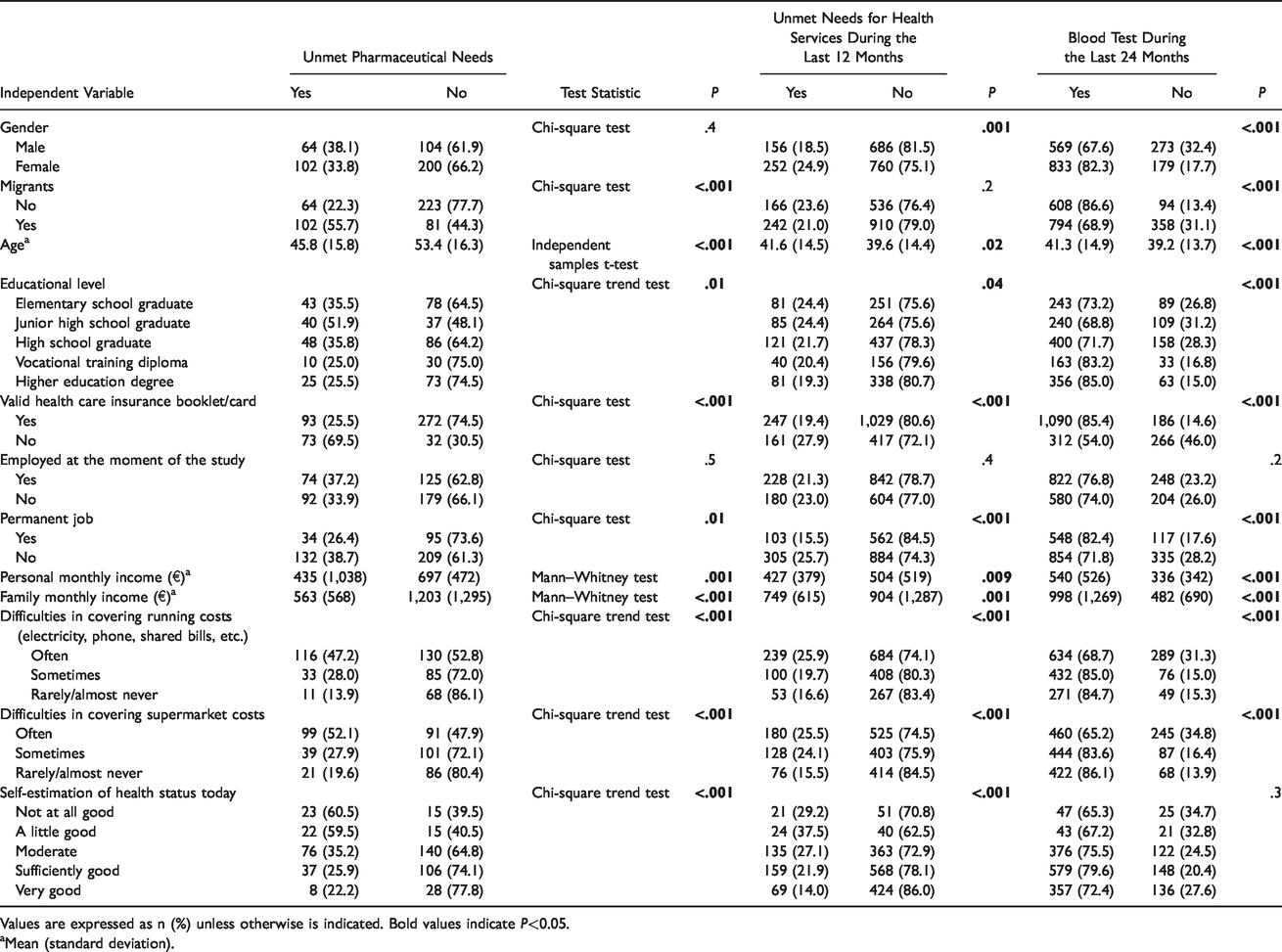
Values are expressed as n (%) unless otherwise is indicated. Bold values indicate P<0.05.
aMean (standard deviation).
Multivariate Logistic Regression Analysis With the Following Dependent Variables: Unmet Pharmaceutical Needs, Unmet Medical Needs for Health Services During the Last 12 Months, and Blood Test During the Last 24 Months.
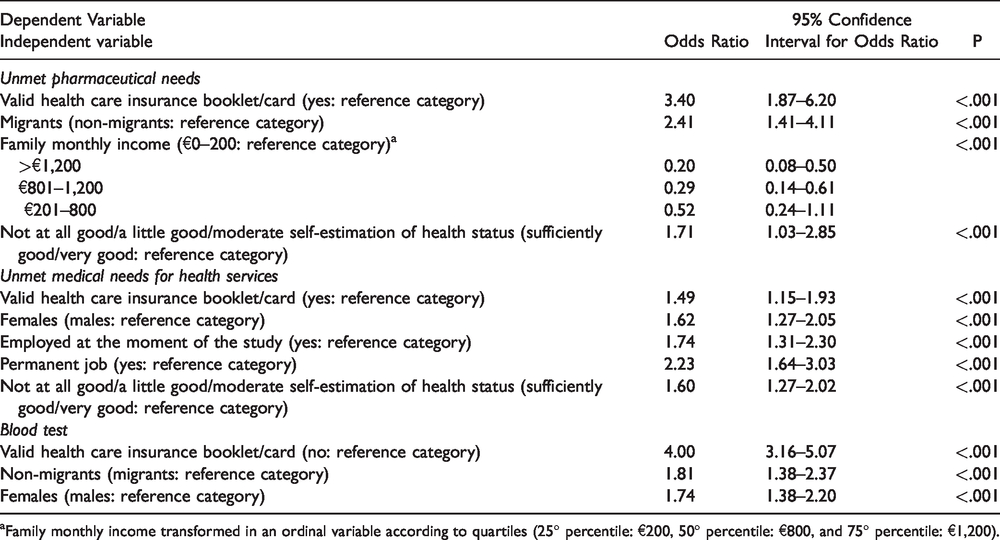
aFamily monthly income transformed in an ordinal variable according to quartiles (25° percentile: €200, 50° percentile: €800, and 75° percentile: €1,200).
Unmet medical needs
Bivariate analysis for unmet medical needs is shown in Table 2, while multivariate logistic regression analysis is shown in Table 3. Participants without health insurance (OR = 1.49, 95% CI = 1.15 to 1.93), females (OR = 1.62, 95% CI = 1.27 to 2.05), those who were unemployed (OR = 1.74, 95% CI = 1.31 to 2.30) or without a permanent occupational status (OR = 2.23, 95% CI = 1.64 to 3.03), and participants who assessed their health status as not at all good/little good/moderate (OR = 1.60, 95% CI = 1.27 to 2.02) were more likely to have unmet needs. Non-migrants had more often unmet medical needs than migrants (23.6% vs 21%), but this relationship was not statistically significant (P = .2).
Prevention services
Non-migrants went more often for a blood test than migrants (86.6% vs 68.9%). Bivariate analysis for the use of outpatient hospital services to go for a blood test is shown in Table 2, while multivariate logistic regression analysis is shown in Table 3. Participants with health insurance (OR =4.00, 95% CI = 3.16 to 5.07), non-migrants (OR = 1.81, 95% CI = 1.38 to 2.37) and females (OR = 1.74, 95% CI = 1.38 to 2.20) were more likely to go for a blood test.
Discussion
Logistic regression analysis showed that the unmet needs for pharmaceuticals and other health services were higher for participants with worse self-reported health status, the unemployed, the migrants, the uninsured, and the poor. Τhey were also more likely not to use the health services.
Unmet Pharmaceutical Needs
Health insurance is one of the most important factors affecting access and use of health services. For example, according to our findings, uninsured persons suffering from a chronic disease more often reported unmet needs in getting their medications compared to the insured. At the time this study was conducted, insured patients generally had to pay a 25% co-payment for the majority of pharmaceuticals (apart from some medicines for which co-payment was set at 10%) while the uninsured had to pay the full cost of their medication. These patients represent a high risk group, and noncompliance with therapeutic guidelines may dramatically affect their health status and impose further pressure on health care system funding. 40 Our results echo findings from other studies, according to which disparities in access and use of health services are greatly attenuated among the insured population.43–46 According to our findings, 36.5% of migrants were not covered by a health insurance scheme, a very high proportion compared to non-migrants (8.5%). This may be explained by the fact that migrants either are unemployed, informally employed, or undocumented (but were reluctant to state so) and therefore not able to apply for health insurance.
Migrants were 2.4 times more likely not to get their medicine compared with non-migrants. The high cost of pharmaceuticals (co-payment is set at 25%) and the bureaucratic procedures to get a prescribed medicine were 2 main reasons for not receiving their medications. These findings coincide with a number of studies that have shown that migrants face a number of barriers, including information gaps, restrictive laws, and other administrative barriers, which limit their access to health care services.19,20,47,48
Unmet Medical Needs
Our findings for the unmet medical needs were similar. Participants without health insurance were more likely to report unmet needs compared to those with health insurance. Other variables associated with increased unmet need for health services were gender, bad state of self-reported health, unemployment, and absence of a permanent job, with the latter 2 representing the most important factors in reporting unmet medical needs. This can be partly explained by the benefits provided at the time this study was conducted. In 2014, all population had access to medical visits in public primary health care facilities while on the other hand, to get medication or to go for laboratory tests, a co-payment was needed for the insured and a full out-of-pocket payment for the uninsured.
Prevention Services
As explained earlier (see Methods section), the use of hospital outpatient blood test services for preventive purposes was chosen to assess the use of health care services, to reduce the effect of the “healthy migrant” factor. Our findings confirmed our initial hypothesis that inequalities exist regarding the utilization of health services by migrants and non-migrants in Greece as well as for those not having health care insurance.
Comparison With Other Countries
Use of health services
Our results coincide with many studies according to which migrants tend to use less health services and especially prevention services than the native population. However, this phenomenon may lead to increased demand for inpatient or emergency services, having negative effects for the health outcome of the population, especially for vulnerable groups such as migrants, and also impose increased costs and pressures to the sustainability of the health system.2,49
As mentioned in the introduction, steps have been taken during the last 3 years to provide health coverage for the migrants, which are not without cost, however. The latest data referring to the financial burden associated to this decision are from the year 2017. The additional cost incurred because of the health coverage of the uninsured was estimated by the Ministry of Health at approximately €400 million (the amount represents 6.5% of public health expenditure for the abovementioned categories of services, while the total number of the uninsured represents approximately 19% of the population). 50 In particular, services were provided to 840,000 of the uninsured population (including migrants and refugees), and the relative costs were €165 million for pharmaceuticals, €57 million for laboratory and diagnostic imaging tests, and €185 million for inpatient care. 50
Despite the fact that the cost of the adoption of a universal health coverage policy is significant, the benefits are expected to outweigh this cost. Although data are scarce, an indicative economic model adopted for 2 separate medical conditions (hypertension and prenatal care) found that the provision of access to regular preventive health care for migrants in Greece would be economically sound. 51 Specifically, according to the findings, free access of migrants to prenatal care may generate savings of up to 48% in Greece (this amounts to about €52 per woman) over 2 years as the provision of prenatal care may actually be half as expensive as treating a low birth weight baby as a consequence of not providing access to care during pregnancy. Findings were similar for hypertension as well, as the cost-savings over a year were estimated around 9% compared to no access to health care. 51 If emergency care only was provided instead, the costs in the first year alone would amount to €66 per person. 51 Although there is no official cost-benefit analysis regarding the effects of this policy, these findings provide clear evidence of the cost savings incurred by providing access to primary health care to migrants.
Access to health care
Similar problems regarding the access of migrants to health care are also encountered by a number of European countries (such as Italy, Spain, Portugal, etc.) with large migrant influx as they also report existing health care disparities among vulnerable populations. A common agreed policy, regarding the most appropriate management of health care needs in sensitive populations, such as refugees and migrants, is to improve access to mitigate health care inequalities among non-migrant and migrant groups, and there are significant efforts toward this direction.16,52,53
Despite the latter positive measures, however, there is still room for improvement as some barriers for the uninsured in accessing health care services remain. Importantly, the 2016 law only allows access to public health care providers, but not private providers contracted with the National Security Fund (EOPYY) (e.g., private diagnostic imaging laboratories). Due to this limitation, accessibility problems are emerging in regions where public health care units are either understaffed or facing shortages of modern equipment (e.g., CTs and MRIs).
Additionally, in 2011, increases in co-payments for medicines for specific diseases were introduced, transferring more costs to patients. As the uninsured are not exempted from the co-payments for pharmaceuticals, they sometime become unaffordable imposing further barriers in the access to care. 54
Electronic prescription system
Finally, problems associated with the electronic prescription system are still imposing barriers to accessing benefits in kind, such as consumables for diabetic patients. Diabetics, for example, may not receive a prescription for the consumables they use daily (e.g., needles) as the doctors may not proceed with an electronic prescription for these categories of patients without having a social security number. Likewise, for the same reason, the uninsured lack other benefits in kind, such as glasses, respiratory devices, orthopedic supplies, headphones, decubitus pads, catheters, and other sanitary materials. To be compensated for the abovementioned benefits, a quite long and complicated bureaucratic procedure has been established. Regarding migrants, no effective measures to enhance communication and remove language barriers are in effect (e.g., absence of intercultural mediators or other facilitating tools), probably having an impact on the provision of quality care and to adherence to the treatment. Toward that direction, further studies to assess the effectiveness of this legislation and its impact on the access and use of health services by vulnerable groups (including migrants) should be conducted.
Public Health Policy Measures
Our findings suggest that migrants face more barriers in accessing health services than non-migrants, and this represents a great challenge to policymakers and health care professionals. A number of critical dimensions should be taken into account to improve health care access. As already discussed, efforts have been made in regards to the legal framework and entitlements to cover the right for access in health care as well as any potential for improvement.
Another important step would be to further include migrants’ access to health care issues in the national health policy agenda. Although discussions on a policy level have been made, no specific national plan has been developed to improve migrants’ access. Specific procedures or guidelines on how to overcome financial, cultural, and other barriers associated with health literacy issues should be included in the national policy documents. Until today, the health delivery model has not been adjusted to incorporate the population diversity (e.g., develop more targeted services for migrants’ health). However, the empowerment and facilitation of health care access for migrants in Greece is necessary.
Depending on the needs of the migrant population, simple measures, such as promotion of information and awareness of the migrant populations on health and hygiene issues, improvement of health literacy regarding the existing health services, and knowledge of how the country’s health system functions, will enable better access health services. 55 Promotion of intercultural mediation in health care services and improvement of provided services, through information, awareness, and training of staff to better understand the special needs of the migrants and the importance of accepting cultural differences, will eventually help to eliminate phenomena of discriminations in health care services. The diversity-responsiveness in health sciences educational curricula should be assessed and further improved with an intersectionality-based approach. 56
Public health policy measures related to appropriate coverage, as for example re-consideration of the levels of co-payments and access to all available services, including those provided by contracted providers, may improve accessibility by reducing waiting lists and increasing compliance with the prescribed therapies.
Conclusions
The issue of migrants’ health has been addressed many times by the European Union, which has identified access to health services as a factor of paramount importance in the effort to reduce health inequalities. Migrants’ access to health services is also considered as a prerequisite for social inclusion and integration of migrants,57,58 while the need for improved national policies to promote migrants’ access has been also stressed many times. 24 Although hosting countries recognize that these populations may have distinct needs from non-migrants and that they constitute a population group diverse in origin and ethnic background which is at risk of exclusion, many countries, including Greece, have not managed yet to develop effective services to meet these needs.
As shown in our analysis, health insurance is a major factor that interacts with migration status to play an important role in people’s ability to access and use health care. Universal health insurance coverage should be a major component of any strategy to reduce disparities in health care. It is worth noting that Greece, despite administrative delays and barriers, provided full coverage to the uninsured, asylum seekers, and migrants, even many groups of undocumented migrants. Despite the fact that the country is severally hit by the economic turmoil, having lost more than 25% of its GDP between 2008 and 2015, this reform represents a structured effort to address the challenges faced by the vulnerable populations, including migrants, as long as it has continuity and there are further policies not only to permit but also empower access and use of health services.
Limitations
Our study was a cross-sectional study providing only a snapshot of differences in unmet need and the use of health services between migrants and non-migrants, and other subgroups. Possible changes over time, especially during the severe economic crisis in Greece, are not depicted. Additionally, as data were self-reported, some issues of cross-cultural validity may be raised. Despite the fact that researchers facilitated the completion of the questionnaires to assure the understandability of the questionnaire, other issues related to the context of the questionnaire (e.g., the differences in the delivery of health services between the Greek health care system and the health system of the origin countries, the organization of the health system, and other cultural differences) should be taken into account when interpreting our results.
Moreover, exclusion of illiterate migrants may be introducing bias in our study, since this group probably faces more difficulties. Another possible bias may be introduced by the fact that the migrants agreed to fill out the questionnaire for fear of being denied access to services. Additionally, migrants were grouped and analyzed as a homogenous group, which is likely to obscure differences across migrant subgroups (e.g., by country of origin). Also, we did not use control variables, and we considered nativity (migrant/non-migrant), health insurance status, and other socioeconomic and demographic characteristics (e.g., age, sex, education, employment status, family income, etc.) and self-reported health status as the independent variables.
All these independent variables were included in the regression models. Unfortunately, we did not use control variables such as geographical distance to health care facilities, personal values and beliefs about health care, objective measures of health status, personal income, etc. These control variables could probably affect the results of our study, e.g., increased geographical distance to health care facilities is associated with decreased access and use of these facilities, while objective measures of health status are more valid than self-reported health status.
Also, we estimated face validity and reliability of the questionnaire but we did not perform rigorous test of validity, such as factor analysis or discriminant analysis. A qualitative study 36 was conducted prior to this one to construct the quantitative questionnaire of our study. Following the qualitative study, a pilot quantitative study with 30 immigrants was carried out to improve the comprehensibility of the questionnaire and to test face validity. Internal consistency of the questionnaire was considered acceptable (Cronbach’s alpha = 0.7). More information about the questionnaire developed may also be found in the pilot study published. 22
Finally, a convenience sample was used since the random sampling was impossible, especially in case of migrants. A convenience sample is more prone to bias than a random sample since participants with a better health usually have an increased response rate.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.