
Abstract
Since the outbreak of the SARS epidemic in 2003, the Chinese government has increased inputs to bolster the health care system. However, the COVID-19 pandemic has exposed the geographic maldistribution of health resources in China. We examine the spatial and temporal variation of the SARS epidemic using a difference-in-differences strategy. Our empirical results show that, compared with cities without SARS case reports, exogenous health shocks significantly increased the affected cities' medical resources supply. We provide multiple robustness tests to examine the validity of the main findings. Further study shows that the mechanism is because the SARS event increased the financial autonomy of the epidemic-affected cities, thus providing an incentive for local governments to increase health resources. Meanwhile, health shocks have little influence on the regions with only imported cases than the infected area. These findings provide a possible explanation for the inequality in the distribution of health resources.
At the beginning of 2020, the new coronavirus outbreak had spread to most parts of China, becoming a public health emergency of international concern. COVID-19 is highly contagious, difficult to control, and uncertain, which poses great challenges to China’s health care system. Although the Chinese government has invested significant money to improve the health care system since the SARS outbreak, it has not effectively solved the problems of unbalanced development and distorted layout of medical resources.1,2 The uneven distribution of medical resources between regions and between urban and rural areas seriously threatened the ability of some regions to cope with health shocks. During the outbreak of the COVID-19, many medical institutions in Hubei, Jiangxi, and other locations became overcrowded. Problems such as patients’ lack of treatment and medical security have exposed the imbalance of primary medical resources between regions in China. Interestingly, based on the data we have collected on the epidemic situation of SARS in Chinese cities from the Ministry of Health, together with announcements regarding the availability of medical resources in certain cities during the early days of COVID-19, we find that during the COVID-19 pandemic period, these cities with insufficient medical resources were either not affected or had only imported cases in 2003. From a vertical perspective, the overall level of fiscal health expenditure and health services in Chinese cities has been greatly improved in recent years. 3 Meanwhile, from a horizontal perspective, it is undeniable that the gap in the supply of health resources between regions is widening. A typical fact is that first-class physicians and hospitals are all concentrated in big cities. Conversely, the number of health institutions in small cities has increased, but the growth rate is obviously low. 4 Consider the unbalanced growth of China’s medical resources: If the outbreak of diseases occurs in areas with poor public health services and densely populated areas, it will be even more difficult to control the epidemic. 5
Medical resources are essentially local public goods. Many scholars have pointed out that the level and quality of the local public goods supply in China fundamentally depend on the structure of the intergovernmental competition and fiscal decentralization, which directly determines the local government's decision-making preferences. 6–8 To understand Chinese local governments' behavior providing medical resources, it is necessary to analyze the institutional background of economic decentralization under political centralization.9,10 Fiscal decentralization, as an important component of economic decentralization, determines the extent of local governments’ willingness to increase public goods spending. 11 The reason is that the official promotion system based on economic development has given local governments a strong incentive to increase infrastructure construction and other expenditures to show their achievements, reducing their attention to non-economic public services. 12 Reflection on the SARS epidemic stimulated the reform of public finance and health policy, subsequently increasing the fiscal autonomy of local governments to equal their fiscal duties and powers, especially in the affected areas. Encouraged local officials have more motivation to support post-disaster health care systems and improve public governance. 13 A possible explanation is that the central government will strengthen local supervision of fiscal expenditures when decentralizing fiscal power, thus increasing the responsibility of local officials for territorial construction. Therefore, when it comes to public expenditure issues, local governments will pay more attention to cost-effectiveness ratios.14,15 As pointed out by Ahmed and Iqbal, when natural disasters such as earthquakes, tsunamis, or large-scale infectious diseases occur, the central government will increase the transfer payments to governments that are more responsible and have a better image and reputation in disaster mitigation. 16 At the same time, local governments will pay more attention to construction of public services after the disaster to prevent the disaster from happening again. The Decision on the Authorization and Entrustment of Land Examination and Approval Rights, issued by the State Council of China on March 12, 2020, states that the local government’s fiscal autonomy can be further expanded by releasing land endowments, and its strength can be exerted in post-disaster reconstruction. Whether cities not affected by health shocks will pay less attention to local health care systems, leaving the growth of health resources behind the affected areas. In response to this puzzle, we use plausibly exogenous variation induced by the SARS epidemic under prefecture-level panel data from 2000 to 2013 in China to examine the effect of health shocks on unbalanced growth of medical resources under the circumstances of the unique fiscal autonomy and governance system. Our findings provide a possible explanation for the regional imbalance of medical resources exposed by the coronavirus pandemic.
This article is organized as follows: We first present the theoretical framework of the causal relationship between health shocks and regional growth of medical resources. We then describe the methodology, variables, and data and report the empirical results. Finally, we present our conclusion.
How Health Shocks Affect Unbalanced Growth of Health Resources
Epidemic and Medical Resources
With the inclusion of health into the national strategy, the realization of universal health coverage is on the agenda. 17 As a core part of the strategic framework for a healthy China, the supply of medical resources has become a mainstream topic in academic circles. Extra-welfarism theory points out that the government should dominate health resource allocation and aim to maximize national health service allocation through the use of public funds. Specifically, the government should give priority to basic medical services and public health and increase the level of coverage for medical treatment insurance to improve the availability of the national health service.18,19 However, under the promotion competition system, local governments are usually attracted by capital and labor, compared with non-economic public goods, such as medical services and public goods. 20 The official promotion system, based on economic assessment, gives local governments more incentives to increase fiscal and economic expenditure, thereby further reducing the proportion of health expenditure. Tulchinsky and Varavikova found that medical reform in Russia after the collapse of the Soviet Union strengthened medical insurance and services, thus improving its ability to cope with malignant infectious diseases. 7 Further, El Masri and Tipple evaluated post-disaster reconstruction in developing countries and found that the area of natural disasters in subsequent years would improve the level of public services, thereby reducing the uncertain risk in the risk society. 21 Waring and Brown pointed out that natural disasters would compel local governments to optimize public health systems, promote medical reform, and strengthen the health security of local citizens. 22 From the perspective of government motivation, increasing public health expenditures to combat the spread of disease can also effectively improve national health status and life expectancy. The enhanced human capital provides the impetus for economic growth. 23 Health shocks, on the other hand, can also lead to increased health awareness and improved demand for health services among people in the affected areas and encourage local governments to increase medical resources. In responses to cases of hookworm in early 20th-century America, for example, Rockefeller’s health council not only provided the necessary treatment for local victims receiving treatment, but also provided for prevention, education, and medical training and thereby increased the local demand for health. 24 Accordingly, for cities unaffected by the SARS epidemic, and because of their lower fiscal revenue, the growth of medical resources will be significantly lower than in the affected areas, in the absence of preventive motivation and medical demand growth.
Epidemic and Fiscal Decentralization
According to the principle of beneficiary decentralization, the state should use the beneficial scope of public goods as the basis for the distribution of fiscal power, which requires that the central government provide public goods benefiting the whole country and the local government supply public goods for local benefit. However, under the promotion evaluation system, the unique information advantage of local governments is undermined by the non-economic nature of public goods. 25
In addition to ensuring the total supply, the central government can also promote the growth of the supply of medical resources through tax cuts, transfer payments, and regional policies. But for the central government, after the health shocks, how to ensure that local governments improve public health systems and the supply of medical and health resources has become another important issue. Bossert evaluated the incentives provided by the central government to local policymakers. Based on empirical data from Colombia, he found that decentralized fiscal authority encourages local governments to make better choices than central leaders in achieving health service targets. 26 In addition, Chapman believed that when local governments encounter external shocks, such as force majeure natural disasters, regions with fiscal autonomy are more flexible in how they deal with them. 27 Further, Skidmore and Toya used transnational panel data from 1970 to 2005 regions and find greater autonomy in fiscal decentralization, fewer deaths caused by natural disasters, and faster post-disaster reconstruction. 28 In short, in the face of risk governance, the combination of central centralized control and decentralization can effectively improve the capacity of public service construction in the affected areas. 10 Similarly, based on the evidence of China, the increase of local fiscal revenue autonomy can effectively improve the supply of public goods. 29
In conclusion, it is reasonable to believe that improvements in fiscal decentralization can effectively stimulate local governments to improve public services and accelerate the construction of health care systems after the epidemic. In fact, since the SARS outbreak, the Chinese government has expanded the fiscal power of local governments to leverage their advantage in post-disaster construction and boost the supply of medical resources.
Econometric Strategy
Identification
At the end of 2002, the world’s first reported case of SARS occurred in Heyuan, Guangdong province. The disease then broke out the following year, worsening into a wave of infectious diseases across the country. Subsequently, the Chinese government announced that large-scale public epidemic prevention efforts had contained the outbreak in July 2003. The deaths of 319 patients, including medical staff, led to a rethinking of the problems exposed by China’s public health system. According to a report by the World Health Organization in 2002, the proportion of China’s health expenditure in the gross domestic product (GDP) is only 96th among 191 member states, explaining why the health system infrastructure and prevention were passive during the SARS epidemic. After the SARS outbreak, the proportion of the Chinese government’s health spending began to increase. However, due to the inconsistent goals of the central and local governments, low degree of local fiscal autonomy, and unmatched fiscal and government power in the region, unaffected cities lack the motivation to improve their local public health systems. Therefore, we use the SARS outbreak as an exogenous variation to examine whether health shocks have heterogeneous effects on the growth of medical resources in different cities and then to explore existing problems in the implementation of medical reform after the SARS epidemic, in order to provide enlightenment for China’s health system reform in response to the COVID-19 pandemic.
According to the data we collected, SARS cases were reported in 113 cities in China. Based on this, we use a difference-in-differences (DD) strategy to identify the effect of health shocks on the growth of medical resources. In order to more intuitively show the changes in medical resource supply in each city, we depict the number of health institutions, hospitals, hospital beds, and physicians per 1,000 persons in experimental group and control group cities before and after 2003, as shown in Figure 1. The results show that medical resources in affected cities increased significantly after 2003, whereas in unaffected cities, they also increased, but to a lesser extent than in the experimental group, which initially supports the above hypothesis. It is worth mentioning that the SARS epidemic occurred primarily in large cities with relatively sound medical systems, and there were also differences in the governance ability and policy thinking of officials in developed and less developed regions; accordingly, the results of the experimental group and the control group before the event intervention were unlikely to fully meet the parallel trend hypothesis, which may lead to a certain deviation in the DD estimator. To solve this problem, we used the trajectory balance method proposed by Hazlett and Xu in their counterfactual analysis. 30 Based on the kernel function method, we balance the trajectories of the covariates between the experimental group and the control group in the high-dimensional space, further estimating the causal effect.

The trend of medical resources between the control group and the experimental group.
Methods
We use variations of the following DD model on prefectural-level data to identify the effects of health shocks on medical resource:

The traditional DD requires that parallel trend tests—that is, the average change between the experimental group and the control group that are not affected by exogenous shocks—are the same, so that their paths are parallel. In addition, the study of Imai and Kim shows that DD under the fixed-effect model also implies additional assumptions: (a) event impact is uniform, (b) impact only affects the results of the same period, and (c) past results do not affect the impact effect of the future. 31 To avoid these potential problems, we draw on the trajectory balancing method in the generalized DD setting proposed by Hazlett and Xu. 30 The model allows shocks to have a long-term impact on the outcome variables, and the average trajectory of the control group is similar to the experimental group under nuclear equilibrium treatment, so we can directly compare the potential differences between the results. In addition, Hazlett pointed out that mapping feature variables to a high-dimensional space for nuclear equilibrium does not require more pretreatment cycles, and any function obtained in the process has the same effect in the experimental group and the control group. 30 Because part of the data before 2000 is significantly missing in this article, the pretreatment group only contains three years, which is more in line with the requirements of the trajectory balancing method. If the treatment after trajectory balance is significantly positive, the results suggest that after taking into account the difference between the two groups, health shocks still have heterogeneous impacts on the increase of medical resources in different cities.
Data
The data used in this article are collected primarily from statistical material for cities and provinces (National Bureau of Statistics, 2000–2013), covering all prefectural-level administrative units, detailed information on local governments’ revenues and expenditures, and basic socioeconomic variables, such as domestic product and population size. We limit our sample period to 2000–2013 because certain key variables are missing from the pre-2000 period. We deleted variables with serious missing values, used linear interpolation methods to fill in missing values, and reduced each variable to the upper and lower 1 percent quantile, finally getting the balance panel data of 211 cities. Among these, 81 cities were affected by the SARS epidemic and 130 cities were not.
Our outcome variables, such as urban medical resources, are primarily composed of medical care and epidemic prevention services. Therefore, we selected the four indicators of the number of health institutions, hospitals, hospital beds, and doctors per 1,000 persons in each city to measure the availability level of medical resources for local residents.
We chose the following indicators for the covariates: First, a regional fiscal state will directly affect the degree of local government public health input—that is, the higher per capita fiscal expenditure and revenue (FE and FR), the higher level of fiscal resources of local government, and the more urban medical resources available to the local government. As noted above, local fiscal decentralization may severely restrict the level of local public services. As part of this mechanism, we refer to the two indicators of fiscal decentralization measured by Jia and colleagues—that is, fiscal expenditure and revenue decentralization, which can reflect different realities.
25
The specific calculation process is shown below:


Secondly, in terms of population indicators, we select the total population of each city at the end of the year and the population per square kilometer to measure population size and density (PS and PD), respectively. The higher the population level, the greater the demand for medical resources. At the same time, population size is also positively correlated with the number of local physicians. Therefore, it is expected to have a positive impact on the supply of medical resources. Thirdly, as regional economic development is conducive to local public health services, we choose per capita GDP as the proxy variable for economic level (ECON). In addition, regional education reflects local governance capabilities and understanding of the importance of public service, so we select the number of full-time teachers in colleges and universities as the proxy variable of education level (EDU). Fourthly, the regional openness of public transport will also affect medical resources, so we chose passenger transport volume per 10,000 and the urban taxi number to measure them (OPEN and TRANS), respectively. Finally, because urban greening in the region is closely related to the health of residents, it probably affects the demand and supply of medical services, so we chose the built-up area green coverage rate to measure it (GRENN). The above variables in the regression model are logarithmic processes.
Table 1 presents two groups’ descriptive characteristics before and after the SARS epidemic. Panel A shows that, before the SARS epidemic, the gap of medical resource indicators between the experimental group and the control group—such as health institutions, hospitals, and hospital beds per 1,000—is not large. However, as we can see in Panel B, the gap between these indicates has widened, which provides preliminary support for our hypothesis.
Descriptive Characteristics.

Results
Main Findings
Controlling for the prefectural and years fixed effects, the estimation results for Equation (1) are presented in Table 2. After health shocks, compared with unaffected cities, the number of health institutions per 1,000 persons increased by 3.44 percent, the number of hospitals per 1,000 persons increased by 0.79 percent, the number of beds per 1,000 persons increased by 10.16 percent, and the number of physicians per 1,000 persons increased by 15.94 percent in the affected cities. The health shock has prompted the affected cities to increase the level and efficiency of public health expenditure, thus improving the resources of local medical facilities. Undeniably, the medical resources of the control groups also increased after the SARS epidemic, but as mentioned above, the DD model implies that the treatment is the difference between the experimental group and the control group. Therefore, this result shows the unbalanced growth of medical resources among regions caused by health shocks. The central government, after the SARS epidemic, spent large amounts of money to improve public health in underdeveloped regions, but due to the nonconformity of central and local governments, unaffected cities may be in pursuit of economic growth while ignoring health care system construction. As a result, the gap in medical resources between regions has been further widened. 32 In further analyses, we will find that health shocks have a strong heterogeneity in the growth of medical resources in cities with different degrees of epidemic impact, so as to further examine the causal fact that health shocks lead to the unbalanced growth of medical resources.
The Impact of Health Shocks on Growth of Medical Resources.
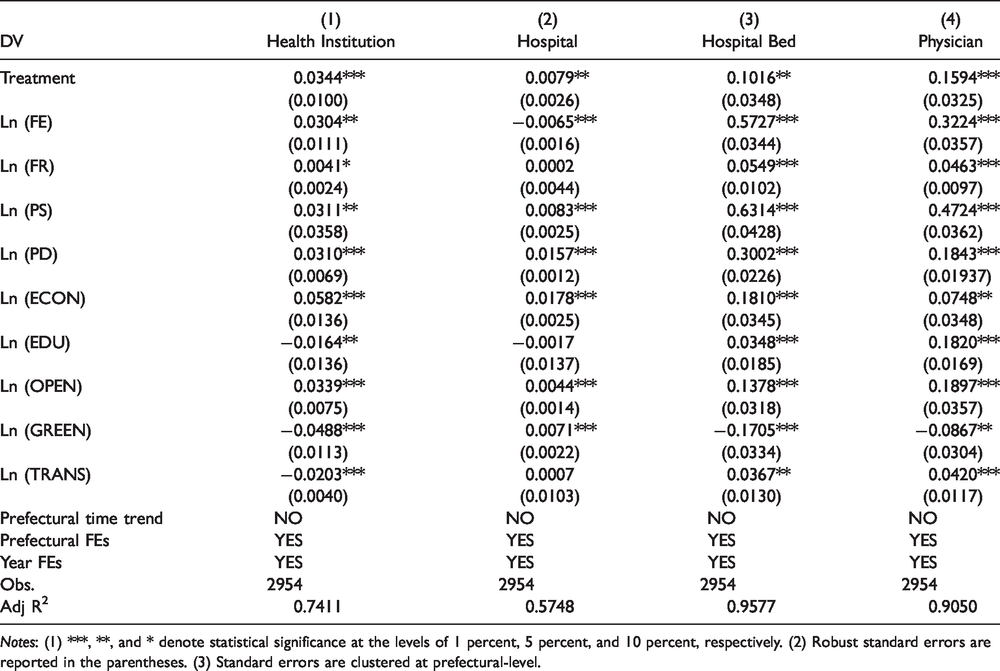
Notes: (1) ***, **, and * denote statistical significance at the levels of 1 percent, 5 percent, and 10 percent, respectively. (2) Robust standard errors are reported in the parentheses. (3) Standard errors are clustered at prefectural-level.
As for the covariates, the direction of the estimated coefficients is basically consistent with the theoretical prediction above, and most of the covariates are statistically significant at the 5 percent level. First, the per capita fiscal expenditure significantly increases the number of urban health institutions, number of beds, and number of physicians, but negatively affects the number of hospitals, hospitals, and hospitals that serve patients and their families. A plausible explanation is that after the SARS outbreak, China’s medical reform advocated for controlling the number of large hospitals and strengthening primary medical resources, thus making the fiscal expenditure more inclined toward other public services, which is not conducive to an increase in the number of hospitals. Second, fiscal income per capita is advantageous to the number of Medicare beneficiaries and statistically significant. Thirdly, the population and openness indicators all reflect that given an increase of urban population and density, the city will provide more medical resources. There is a negative impact of urban greening on medical resources, probably because it reduces the likelihood of people falling ill, thus reducing the supply of health resources and decreasing medical demand.
Trajectory Balancing
We use the kernel function to map the covariates of the experimental group and the control group to a high-dimension space and to map the covariates to a high-dimension space. Because the basic function is linear, the optimal equilibrium can be achieved by weighting the trajectories of the vectors in the experimental group and the control group whose trajectories are approximately the same before the health shock. Table 3 reports the estimated results of this counterfactual analysis.
Counterfactual Analysis of the Impact of Health Shocks on Medical Resources.

Notes: (1) Results of the average treatment are based on the “tjbal” package in R and obtained by 500 jackknife simulations. (2) ***, **, and * denote statistical significance at the levels of 1 percent, 5 percent, and 10 percent, respectively. (3) Robust standard errors are reported in the parentheses. (4) Standard errors are clustered at prefectural-level.
Table 3 shows that health shocks do increase the number of health institutions, hospitals, and physicians in affected cities by the 5 percent significance level, compared to unaffected cities. Furthermore, we present graphically the disproportionate effects of the SARS epidemic on the supply of medical resources between affected cities and unaffected cities, as shown in Figure 2. From the validity viewpoint, the key point is how closely the pattern of the pre-treatment health shocks of medical resources in affected cities (the solid line) resembles the analogous trend in the weighted unaffected cities (the dashed line). The evidence shown in Figure 2 is convincing. During the pre-treatment period, the discrepancies between the two units being compared tended to be minor, consistently falling below the statistical significance level (i.e., the lines falls in common shaded areas). Meanwhile, after 2003, the increase in health resources in affected cities was significantly higher than in unaffected cities, which further supported our theoretical hypothesis.
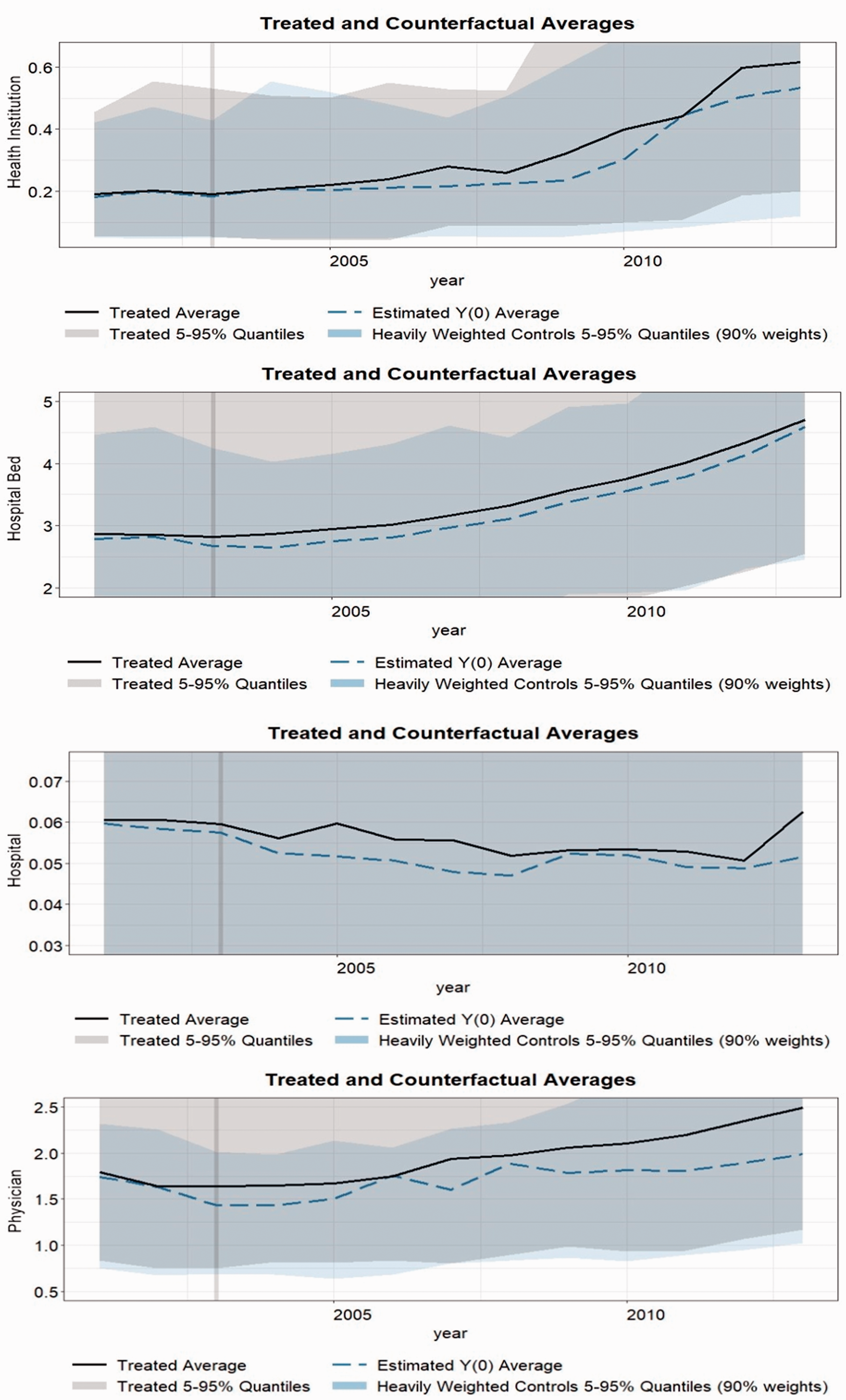
Band plot visualizing treated and counterfactual averages.
Robustness Checks
Exclude New Medical Reform Implication
Because the data span a period of 14 years, the estimation of the average treatment of health shocks on health resources in affected cities is inevitably influenced by other policies, leading to overestimates or underestimates. To identify and address this problem, we further examine other health care reform events that occurred in the years following the SARS outbreak. We find that the China State Council issued a reform of the deepening medical health system in 2009 (hereinafter referred to as “new medical reform”). The new medical reform points out that the medical and health undertakings should be governed by a new way of thinking, the government’s responsibility for health financing should be enhanced, and the performance appraisal should be gradually changed to “people’s livelihood indicators.” 33 Since 2009, China’s fiscal health expenditure has been growing rapidly, with two characteristics: increasing subsidies to primary medical and health institutions and continuously investing in medical security, thus accelerating the goal of equal access to medical services for all people in the country. Therefore, it is reasonable to believe that the new medical reform has reduced the unbalanced growth caused by the SARS epidemic, which leads to biased estimation in baseline regression. To identify this effect, we add dummy variables of the new medical reform policy of 2009 into the benchmark regression model of the 2009 health care reform law. The dummy variables in Columns 1, 3, and 4 in Table 4 are all statistically significant at the 5 percent level, implying that medical reform increased medical resources. At the same time, the positive impact of health shocks on health institutions is no longer significant with the introduction of dummy variables. This shows that the new medical reform policy has significantly improved the number of unaffected health institutions and strengthened primary medical resources, thus offsetting the impact of health shocks. In addition, the treatment of health shocks on hospitals, hospital beds, and physicians has been weakened, reflecting that the new medical reform has reduced the unbalanced growth of medical resources after the SARS outbreak, but it still exists.
Robustness Checks 1 : Excluding New Medical Reform Implication.

Notes: (1) Set the ones in 2009 and after as 1 and the others as 0 in dummy variable of the new medical reform policy. (2) ***, **, and * denote statistical significance at the levels of 1 percent, 5 percent, and 10 percent, respectively. (3) Robust standard errors are reported in the parentheses. (4) Standard errors are clustered at prefectural-level.
Supportive Verification
To further test whether cities not affected by SARS pay more attention to economic construction and neglect to make up for the shortage of medical resources, we provide supportive verification. Specifically, we construct a new dummy variable and switch the value of the variable on the interaction item in model 1 —that is, the experimental group is the cities without SARS cases and the control group is the affected cities. Furthermore, we construct a new outcome variable (EFE) by calculating the fiscal proportion of per capita fiscal expenditure minus per capita expenditure on science and technology, education, and health. The prefectural fiscal budget expenditure in the national bureau of statistics only discloses the expenditure on science and education, so in order to separate out the public health expenditure, we use the provincial per capita public health expenditure to replace the prefectural per capita health expenditure. Although there may be some measurement errors, it is generally more conducive to economic growth and the emphasis on local finance rather than science, education, and health care.
Table 5 shows that after the SARS outbreak, compared with the affected cities, unaffected cities increased their emphasis on fiscal economic expenditure by 0.28 percent, which is statistically significant at the level of 5 percent. After adding control variables, the net effect of health shocks on the proportion of fiscal economic expenditures in these cities is 0.14 percent. This result supports our previous analysis that, compared to affected cities, unaffected cities are more focused on infrastructure than on public health expenditure.
Robustness Checks: 2 The Impact of Health Shocks on Non-Productive Fiscal Expenditure.

Placebo Test
Considering that unobserved factors may also lead to unbalanced growth of urban medical resources, we conduct a placebo test to further verify the impact of the health shock. For each specific operation, we randomly allocate the interaction terms out of order and calculate the corresponding second result according to the generated interaction terms, while the other variables remain unchanged. Finally, we use the same method to test the randomly ordered samples. We tested the four outcome variables for 1,000 times respectively and obtained their corresponding regression coefficients and standard errors. The kernel density distribution is shown in Figure 3, where the dotted line is the estimated coefficient of the treatment during the baseline regression. The results show that the actual treatment is significantly different from those estimated by the placebo test. Therefore, we assume that the baseline regression is robust.

Placebo test.
Mechanism
The theoretical analysis points out that health shocks will prompt the central government to increase the fiscal autonomy of affected cities, leading to the growth of medical resources. Therefore, to verify whether this mechanism is valid, we use the causal mediation effect model under the counterfactual framework proposed by Imai and colleagues to test this hypothesis. 31 Average Direct Effect (ADE) and Average Causal Mediation Effect (ACME) reflect the influence of treatment and mediator on the outcome variables. According to Imai and colleagues, ACME and ADE can be identified as non-parameters under the assumption of sequence ignorability. 31 However, these assumptions cannot be directly tested, and we can only examine their sensitivity in reverse—that is, how our estimation results will change when those assumptions are not satisfied. In the sensitivity analysis below, we find that the average causal effect of the experimental group changed from positive to negative only when the heterogeneous effect generated by the interaction between each mediator and the treatment indicator could explain at least 7 percent of the variation in treatment, which indicates that the results are reliable.
The process of estimating causal mediation effects is divided into several steps: First, we posit and fit regression models for the mediator (local fiscal autonomy) and outcome of interest (medical resources). The mediator model includes the treatment indicator (affected cities) as well as other covariates. The outcome is modeled as a function of treatment indicator and the mediator. Based on the fitted mediator model, we then generate two sets of predicted mediator values for affected and unaffected cities, which are then used to determine the effect of the mediator. We use the outcome model to impute potential outcomes. For each city, we first obtained the predicted value corresponding to the results of no health shocks and the predicted mediator value for the treatment condition (obtained in the previous step). We then generate the predicted counterfactual outcome—that is, the outcome where the treatment indicator is still set to 1 (affected cities), but the mediator is set to its predicted value in the unaffected cities. Finally, we calculate the average causal mediator effect by averaging the differences between the predicted outcomes of the two values of the observations.
Table 6 reports the average causal effect of fiscal autonomy, the direct effect of health shocks, and the total effect of both. The results show that the SARS epidemic has significantly increased the expenditure and revenue decentralization of the affected cities, thus improving the level of local government and improving the supply of public services. In contrast, the percentage mediated by expenditure decentralization on health institutions, hospitals, hospital beds, and physicians were 8.86 percent, 14.29 percent, 28.48 percent, and 36.34 percent, respectively. According to the theory of public goods and fiscal decentralization, local governments, as opposed to the central government, have the advantages of information and flexibility. Therefore, with improved fiscal expenditure decentralization level, local governments can improve the quantity and efficiency of public service expenditure, which is conducive to meeting the demand of local residents for health services. Interestingly, the mediating effect of revenue decentralization is generally lower than that of expenditure decentralization. The explanation is simple: Increased fiscal revenue autonomy means that the central government gives local governments more revenue power. Because additional capital is allocated to the local government, the central government has fewer constraints on local governments and the affairs for which they are responsible. Given the intergovernmental competition, local governments have more power to put additional fiscal funds into the construction of economic infrastructure, rather than increasing the supply of public services.
The Causal Mediating Effect of Expenditure Decentralization and Revenue Decentralization.
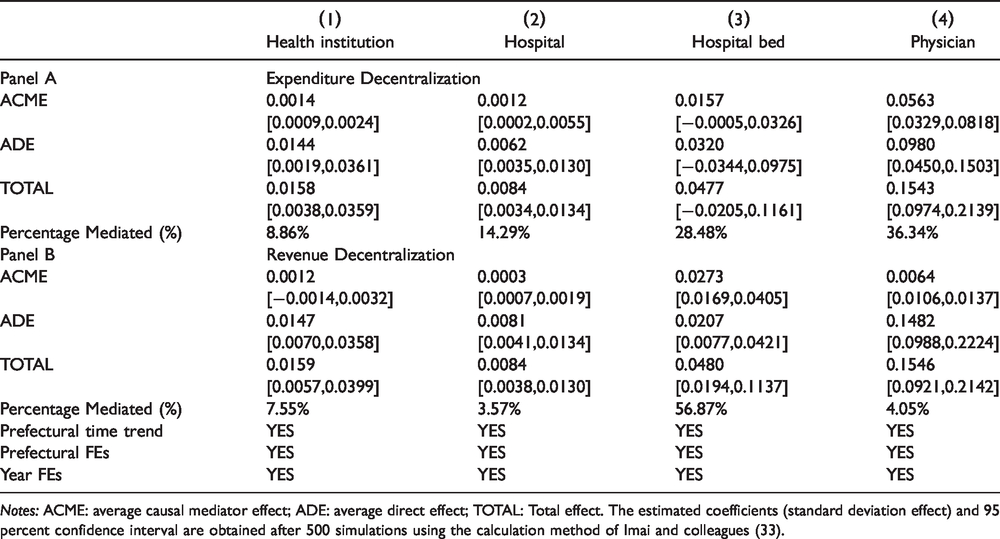
Notes: ACME: average causal mediator effect; ADE: average direct effect; TOTAL: Total effect. The estimated coefficients (standard deviation effect) and 95 percent confidence interval are obtained after 500 simulations using the calculation method of Imai and colleagues (33).
Heterogeneity
After the outbreak of SARS in 2003, the World Health Organization successively listed 10 provinces on the Chinese mainland as epidemic areas. According to its definition, among the 24 provinces reporting SARS cases, five provinces (Beijing, Tianjin, Shanxi, Inner Mongolia, and Guangdong) are areas of high transmission; two provinces (Hebei and Jilin) are areas of moderate transmission; three provinces (Guangxi, Sichuan, and Shaanxi) are areas of low transmission; and 14 provinces are areas of imported cases. Therefore, to further investigate whether health shocks may lead to heterogenous growth of medical resources among regions with different levels of transmission, we define different experimental groups according to the epidemic transmission. In Table 7, Panel A reports the impact of health shocks on cities in the epidemic provinces compared with unaffected cities after removing the samples from provinces that had only imported cases. The results show that the treatment is higher than the baseline estimate and that all the changes are significant at the 5 percent level. This means that in cities with more severe outbreaks, local governments are paying more attention to medical services. On the other hand, Panel B reports the results after removing the provinces listed as epidemic areas. We find that although health shocks have a statistically significant positive effect on the number of health institutions and hospitals in the non-epidemic areas, it is lower than the treatment in the epidemic areas. This suggests that local governments in non-epidemic areas are significantly less likely to increase their levels of public health services than those in cities severely affected by the outbreak. More importantly, the health shocks have no significant effect on the number of beds and physicians available in non-epidemic areas. It is worth mentioning that in baseline regression, we have verified that the affected cities significantly improve the level of medical resource supply compared to other cities. Thus, we argue that unaffected cities and mildly affected cities also lack sufficient performance in improving their local public health systems. This can be explained in two ways. One is that when local leadership changes to bring in new leaders who lack experience with the SARS epidemic, they may lack attention to the local health system. Another is that local government spending on fiscal expenditures is lower. With the outbreak of COVID-19, we find there is a shortage of primary medical resources in many places, making it more difficult for governments to control the epidemic. The fact that most of the regions lacking medical resources were cities that were less affected or not affected by the SARS disease confirms the robustness of our conclusions from a practical perspective.
Heterogeneity of Epidemic Areas and Non-Epidemic Areas.

Notes: (1) ***, **, and * denote statistical significance at the levels of 1 percent, 5 percent, and 10 percent, respectively. (2) Robust standard errors are reported in the parentheses. (3) Standard errors are clustered at prefectural-level.
Conclusion
In this article, we first bridge the literature regarding the occurrence of infectious diseases and the distribution of medical resources. Although many studies confirm that fiscal autonomy has a causal relationship with the distribution of medical resources, they ignore the intermediary role of fiscal decentralization between health shocks and medical resource growth. Based on the panel data for 292 prefecture-level cities from 2000 to 2013, we take the SARS epidemic as an exogenous shock and identify the impact of health shocks on medical resources under the DD strategy. Our study find that health shocks significantly increased the availability of health resources in affected cities, relative to cities with no cases. Furthermore, we find that the new medical reform policy weakens the influence of an unbalanced growth of medical resources between cities to a certain extent. At the same time, we confirm that unaffected cities relatively increase their economic expenditure proportionately after health shocks, proving our analysis conclusion that cities lacking preventive motivation and attention to public health expenditure. Finally, the mechanism shows that health shocks encourage affected cities to improve their health care systems by increasing their fiscal autonomy.
Our conclusions provide a new perspective and policy implications related to deepening the medical reform and promoting the equalization of medical resources. First, although the Chinese government invested significant money to build the public health system after the SAR epidemic, it has also contributed to problems such as misallocation of medical resources. Therefore, it is necessary to implement the healthy China strategy, promote tripartite sector reform, and strengthen the community-level health care system and the ranks of general practitioners. Secondly, the government should shift its thinking on support and upgrade from whole-coverage support in the entire region to precise support in regions with unbalanced supply and demand. Thirdly, China needs to improve the fiscal decentralization system, clarify fiscal and duty power, and improve institutional norms, incentives, and restraint mechanisms. The autonomy of government revenues and expenditures at all levels shall be stipulated, and the scope of authority for fiscal management, responsibility for expenditure, and policy support shall be clarified.
Our article is not free of limitations, but it could be used to extend this work in several directions. First, future research may be directed toward the identification of other fiscal strategies that could enhance the effects of allocation of medical and health resources. Second, it remains to be solved how to equalize the breadth and depth of basic public medical and health services through public finance.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This article was supported by the National Nature Science Foundation of China (71771126).