
Abstract
This paper investigates the epidemiology and public health response of novel coronavirus infection (COVID-19) in the Nordic region. The data on cases and deaths due to COVID-19 were drawn from the European Centre for Disease Prevention and Control. The data on age- and sex-wise cases, deaths and intensive care unit (ICU) admissions, and public health interventions in the Nordic region through November 10, 2020, were obtained from respective countries’ health ministries. Sweden accounted for 60.59% of cases (162 240 of 267 768 cases) and 81% of deaths (6057 of 7477 cases) in the Nordic region. The incidence rate for the Nordic region was 989.59 per 100 000, varying from 327.30 per 100 000 in Finland to 1616.51 per 100 000 in Sweden, and the mortality rate for the region was 27.63 per 100 000, ranging from 5.3 per 100 000 in Norway to 60.35 per 100 000 in Sweden. The case–fatality ratio of the Nordic region was 2.79%. Females were more susceptible to COVID-19 infection than males (52.30% vs 47.66%), while males had a greater proportion of deaths (54.7%) and ICU need (71.99%) than females. It is imperative to continue with social distancing, mandatory masks, testing, prohibition of mass gatherings, isolation of confirmed cases, and preventing the importation of cases from other countries to avoid the further resurgence of cases.
Introduction
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), commonly known as coronavirus or COVID-19, a pandemic that originated in Wuhan, China in December 2019, 1 has led to substantial financial, economic, and health crises across the globe. Before SARS-CoV-2, two human coronaviruses emerged, namely, SARS-CoV, which emerged in 2003, and Middle East respiratory syndrome coronavirus, which appeared in 2012. These 2 epidemics did not lead to massive catastrophic transmission and impacted 29 countries (8096 cases, 774 deaths) and 27 countries (2494 cases, 912 deaths), respectively.2,3 In comparison, COVID-19 has already impacted 220 countries/territories, has claimed 1 261 075 lives, and has recorded over 50 million cases as of November 10, 2020. 4
The COVID-19 virus seems to be contained mainly in China, but the United States and Europe continue to be the global epicenters, and emerging economies such as India, Brazil, and Russia have emerged as new hotspots of the pandemic. There are still no approved vaccines 5 and effective treatment available for coronavirus infection; however, several medicines and vaccines are being studied in different clinical trials. In the absence of medicine and treatment paradigms, prevention via social distancing, mask-wearing, and isolation was adopted as the best defense line against the pandemic.
In this study, we examined the epidemiology of COVID-19 and public health response in the Nordic region: Denmark, Finland, Sweden, Norway, and Iceland. The epidemiology of COVID-19 was analyzed in 4 dimensions. First, we investigated daily cases, deaths, and case–fatality ratio (CFR) in all the 5 countries of the Nordic region. Second, we examined the incidence and mortality rates of COVID-19 in the 5 Nordic countries and in the first administrative units (regions/counties) in each country. Third, we conducted the age- and sex-wise examination of incidence, mortality, and intensive care unit (ICU) admissions in the Nordic region. Moreover, measures and interventions undertaken by the Nordic countries to restrict virus transmission were also reviewed. Lastly, we attempted to highlight the Nordic countries’ public health system response to combat the public health threat and its impact on the provision of elective care, screening, and follow-up activities of chronic diseases.
Data and Methodology
The data on cases and deaths per day of COVID-19 in the Nordic region through November 10, 2020, were extracted from the European Centre for Disease Prevention and Control. 6 The population estimates were drawn from the United Nations world population 7 prospects to calculate the incidence and mortality rates for the Nordic region. For Finland, the age- and sex-wise cases and deaths data published by the Finnish Institute for Health and Welfare were employed. 8 Intensive care snapshot: COVID-19 in ICUs report dated October 28, 2020 was used to extract information about the patients in ICU for Finland. 9 The information for Denmark through November 10, 2020, was obtained from data published by the Statens Serum Institut. 10 The information for Norway was extracted from the Norwegian Institute of Public Health, 11 and intensive care data were extracted from the COVID-19 weekly report—week 44, Wednesday, November 4, 2020. 12 Data for Sweden through November 11, 2020, were obtained from Folkhälsomyndigheten, Public Health Agency of Sweden. 13 The data for Iceland were extracted from a new website created by the Directorate of Health and the Department of Civil Protection and Emergency Management to publish all COVID-19 centric information. 14
Information regarding the public health system response toward the pandemic was extracted from COVID-19 Health System Response Monitor. 15 The public health system constitutes all public, private, and voluntary entities that contribute to the delivery of essential public health services within a jurisdiction, ie, monitoring population health status; diagnosing and addressing health problems and hazards; communicating with the general public; implementing plans, policies, and laws impacting health; maintaining a robust organizational infrastructure; building a skilled public workforce; enabling equitable access, and improving public health functions. 16 We categorized the public health response under health financing, health infrastructure, and healthcare facilities heads. We also examined the communication and interventional strategies adopted during COVID-19 and shown the deferral effect on non-COVID-19 health services due to the pandemic.
Results
Epidemiology of COVID-19
National and Regional/County Trends
In the Nordic region, the first case of COVID-19 was observed in late February (except Finland and Sweden, wherein the first case was confirmed on January 30 and February 1, 2020, respectively, and the next case was observed at the end of February). Since then, the Nordic region has reported 267 768 infected cases and 7477 deaths due to COVID-19 as of November 10, 2020. Sweden reported the highest number of cases (162 240) and deaths (6057) in the region, followed by Denmark with 56 958 cases and 750 deaths. Iceland recorded the least number of infected people (5142), albeit with the second-highest incidence rate (1516.67 per 100 000). Sweden recorded the highest incidence rate of 1616.52 per 100 000, whereas the lowest incidence rate was observed in Finland (327.3 per 100 000). The mortality rate ranged from 5.3 per 100 000 in Norway to 60.35 per 100 000 in Sweden.
The overall CFR of the Nordic region was 2.79%, varying from 0.47% in Iceland to 3.73% in Sweden. The CFR of the Nordic region ranged from 10.58% in April to 0.33% in October. (Monthly CFR is calculated as the percentage of total deaths in a county divided by total number of confirmed cases in that country per month.) In Sweden, CFR peaked at 15.14% in April (the highest in the Nordic region), only to come down to 10.24% in May and to 0.36% in October. The CFR in Iceland varied from 0.18% in March to 1.13% in April and turned zero from May to September while witnessing a slight rise in October (0.095%; the lowest in the Nordic region) (Supplemental Figure S1).
A high regional disparity was observed in the Nordic region in terms of COVID-19 cases (Figure 1) and incidence rates (Supplemental Figure S2). Among the 21 Swedish counties, Stockholm and Västra Götaland accounted for 48.20% of cases and 55.54% of deaths. Jönköping recorded the highest incidence rate (1956 per 100 000), followed by Örebro (1746.69 per 100 000), and the CFR was the highest in Sörmland (7.89%). Among all Nordic regions/counties, Stockholm has recorded the highest number of cases (38 123, 14.24% of Nordic cases) and deaths (2444, 32.68% of Nordic deaths).
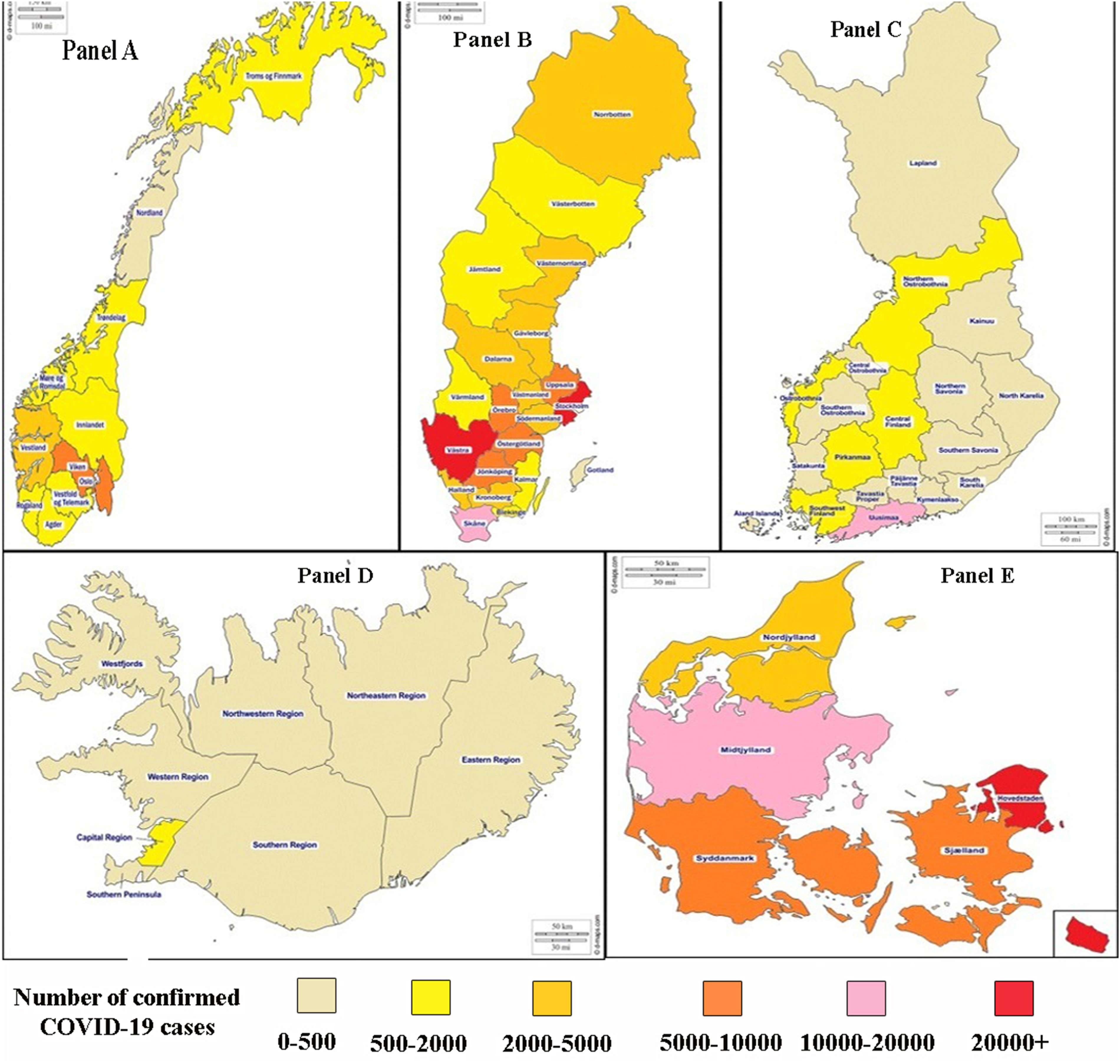
Confirmed COVID-19 cases across Nordic countries: (A) Norway, (B) Sweden, (C) Finland, (D) Iceland, and (E) Denmark. Data Source: Norwegian Institute of Public Health for Norway, Folkhälsomyndigheten for Sweden, Finish Institute for Health and Welfare (THL) for Finland, Covid.is for Iceland, and Statens Serum Institut for Denmark.
Among the 11 Norwegian counties, Oslo and Viken were the most severely affected counties with 7608 (1097.1 per 100 000) and 6912 (556.9 per 100 000) cases; these 2 counties accounted for 57.90% of cases in Norway. Among the 5 regions of Denmark, Hovedstaden was the most severely hit region with 27 271 cases (1477.3 per 100 000), while Nordjylland was the least affected region with 4728 cases. In Denmark, Hovedstaden alone accounted for 48.44% of cases and 56.93% of deaths, and the CFR was the highest in Sjælland (2%). In Iceland, Greater Reykjavík reported the highest number of cases (1320) and accounted for 72.93% of the cases. In Finland, Uusimaa had 61.98% of Finnish cases with the highest incidence rate (665.67 per 100 000), and the lowest incidence rate was observed in Satakunnan (69.20 per 100 000).
Gender-Wise Comparison
Figure 2 illustrates the gender-wise bifurcation of cases, deaths, and ICU admissions. In the Nordic region, females were more susceptible to COVID-19 infection (52.33%) than males (47.66%). Males, however, accounted for a higher proportion of deaths (54.7%) than females (45.29%) except for Finland, in which a higher percentage of deaths occurred in females (51%) than males (49%). Out of 267 768 confirmed cases, 1.47% of people required ICU care. A higher percentage of males (72%) required ICU care than females (28%) in the Nordic region (except Iceland). (Gender-wise distribution of deaths and ICU was not available for Iceland.)

Gender-wise bifurcation of COVID-19 cases, deaths, and intensive care admissions. Data Source: Covid.is for Iceland, Finish Institute for Health and Welfare (THL) and Intensive care snapshot: COVID-19 in intensive care units report dated October 28, 2020, for Finland, Statens Serum Institut for Denmark, Norwegian Institute of Public Health and COVID-19 weekly report-week 44, Wednesday, November 4, 2020, for Norway, and Folkhälsomyndigheten for Sweden.
Age-Wise Distribution of COVID-19
The distribution of COVID-19 cases, deaths, and ICU needs across different age groups is illustrated in Figure 3. The median age of confirmed COVID-19 cases was 40.63 years in the Nordic region (except Iceland). (Comparable age-wise distribution of cases was not available for Iceland.) In 4 Nordic countries, the highest number of cases, ie, 52 171 (19.87%) belonged to the 20- to 29-year-old age group, followed by 42 933 cases (16.35%) in the 40- to 49-year-old age group, and the least infected age group was 0 to 9 years with 5896 cases (2.25%). The 80- to 89-year-old age group recorded the highest percentage of deaths in the Nordic region: Sweden (2518 deaths; 41.57%), Finland (149; 41.27%), Iceland (4; 40%), Denmark (292; 38.93%), and Norway (102; 35.79%). The median age of death due to COVID-19 in the Nordic region was 83.60 years, with 25.75% of deaths reported in the 90 plus age group. The least number of deaths occurred in the 0- to 39-year-old age group (36 deaths; 0.48%).
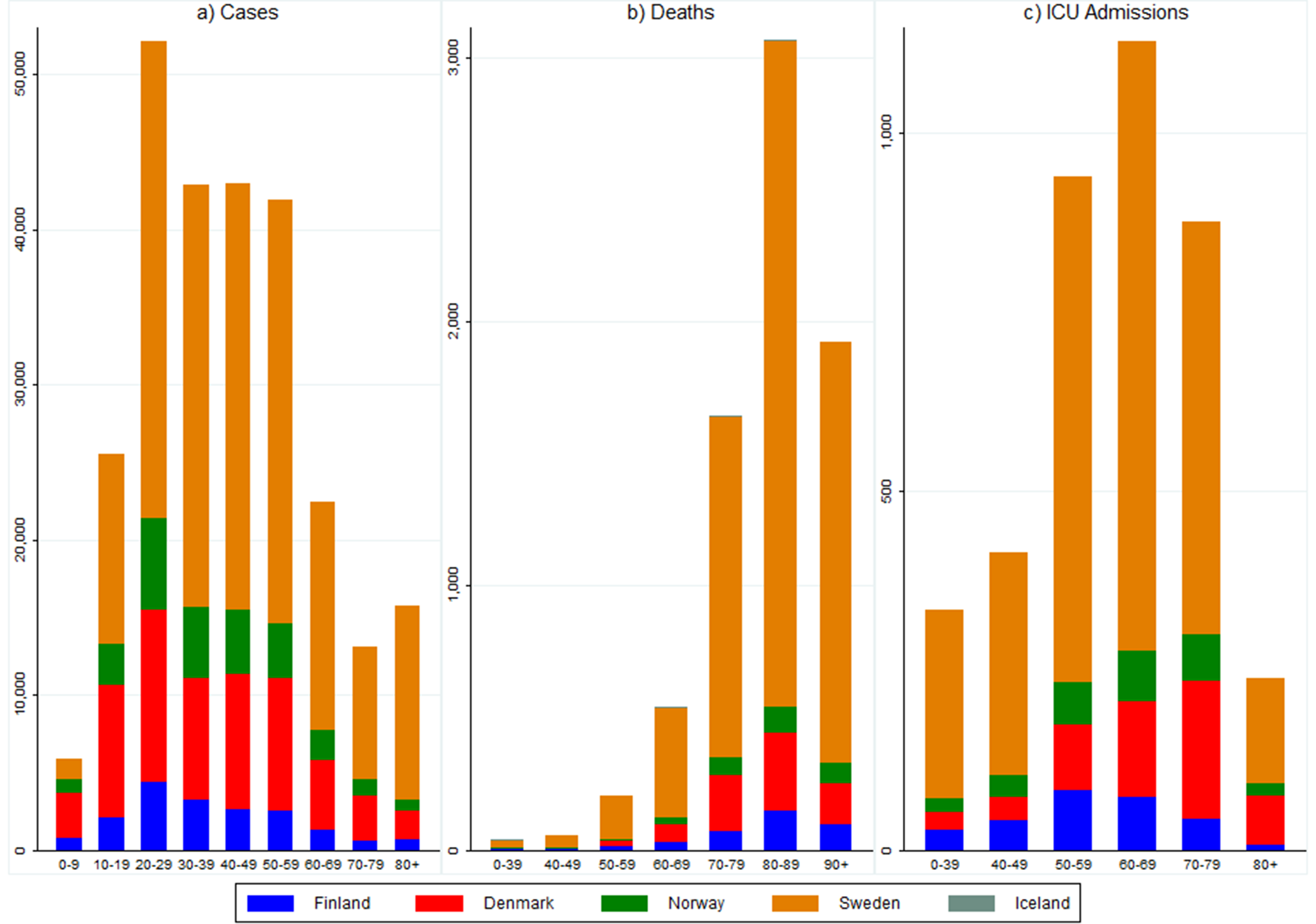
Age-wise bifurcation of COVID-19 cases, deaths, and intensive care admissions. Data Source: Covid.is for Iceland, Finish Institute for Health and Welfare and Intensive care snapshot: COVID-19 in intensive care units report dated October 28, 2020, for Finland, Statens Serum Institut for Denmark, Norwegian Institute of Public Health and COVID-19 weekly report-week 44, Wednesday, November 4, 2020, for Norway, and Folkhälsomyndigheten for Sweden.
In the Nordic region (except Iceland), (Age-wise distribution of ICU admissions was not available for Iceland.) patients in the older age groups were most prone to have required ICU care. A total of 3932 people (excluding Iceland) have been admitted to ICU, out of which 1128 cases (28.69%) belonged to the 60- to 69-year-old age group, followed by 939 cases (23.88%) in the 50- to 59-year-old age group, and 876 cases (22.28%) in the 70- to 79-year-old age group.
Interventions and Public Health System Response
The public health system is considered robust and resilient in Nordic countries and is characterized by tax-based funding, residency-based universal access, and comprehensive coverage. 17 In Nordic countries, trust in state institutions is also the highest 18 and authorities have tried to maintain that trust by undertaking multidimensional efforts to suppress, contain, and mitigate the virus spread. Nordic countries responded quickly by implementing restrictions within 6 to 19 days of the first reported case (for Finland and Sweden, from the second reported case) (Figure 4). All Nordic countries prohibited mass gatherings, imposed international travel restrictions, and prohibited non-essential services and businesses. The educational institutions (eg, schools and colleges) were closed, barring few exceptions, and online classes were promoted. Finland and Norway implemented lockdown, and Denmark declared partial shutdown while Iceland and Sweden did not impose lockdown. 15 The Swedish government's decision to remain open was due to the historical feature of the Swedish constitution, which does not allow the government to call a state of emergency in peacetime. 19 Fines and penalties were imposed to ensure adherence to restrictions; for instance, Iceland imposed a penalty for violation of quarantine rules and isolation.
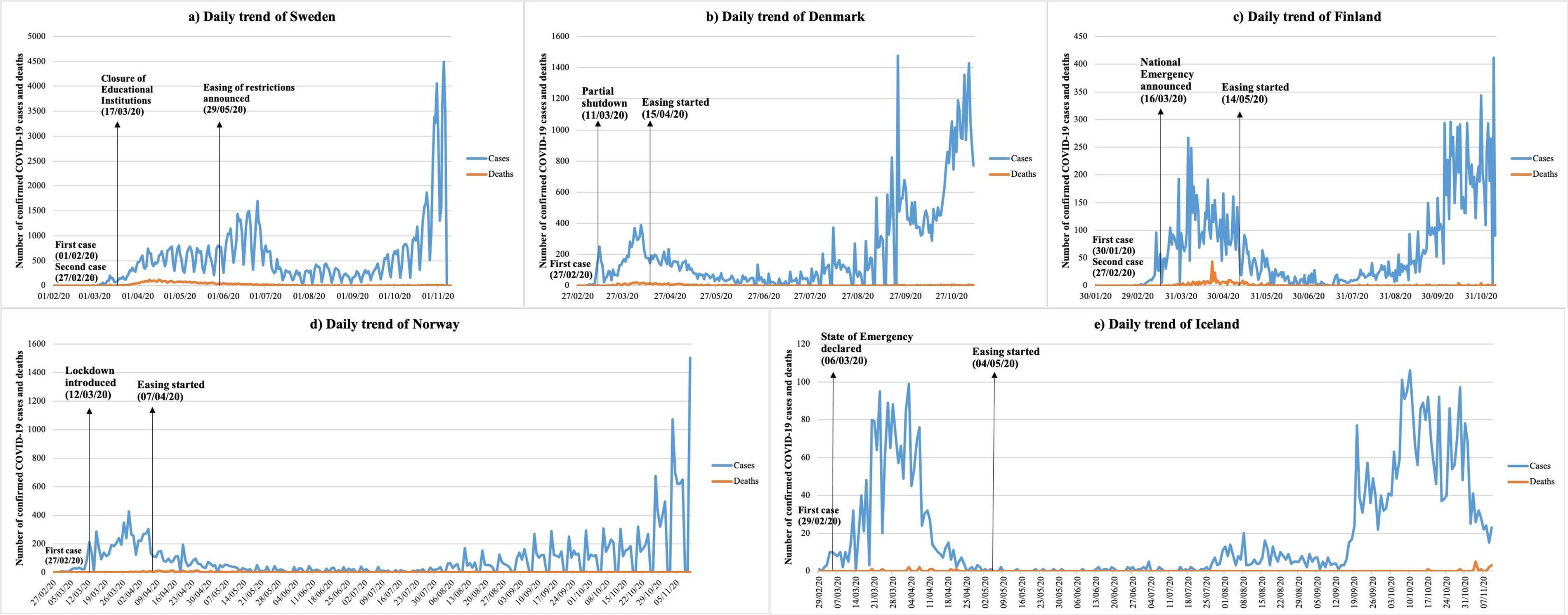
Daily trend of COVID-19 cases and deaths in Nordic countries as of November 10, 2020: (A) Sweden, (B) Denmark, (C) Finland, (D) Norway, and (E) Iceland. Data Source: European Centre for Disease Prevention and Control. The data pertained to confirmed cases and deaths through November 10, 2020. Dates of interventions imposed and restrictions eased were extracted from Health Systems Response Monitor.
Through a robust communication system, the public was kept well informed about hygiene, social distancing, and other preventive measures for COVID-19 through different media such as websites, posts, text messages, and email, or a combination of these. Nordic countries placed a rich emphasis on testing, isolation, and contact tracing, even after easing restrictions, to minimize the burden on the healthcare system. The government in all Nordic countries has borne the treatment costs of COVID-19 patients. Video and telephone consultations were scaled-up not only for COVID-19 but for other diseases, too, and the patients were encouraged to use those channels instead of presenting physically to the clinics. Despite having some of the best development statistics globally, Nordic countries have also encountered a few roadblocks, such as shortages of health resources and deferral of non-COVID-19 treatments while dealing with the pandemic (Table 1).
Response of the Public Health System in Nordic Countries.
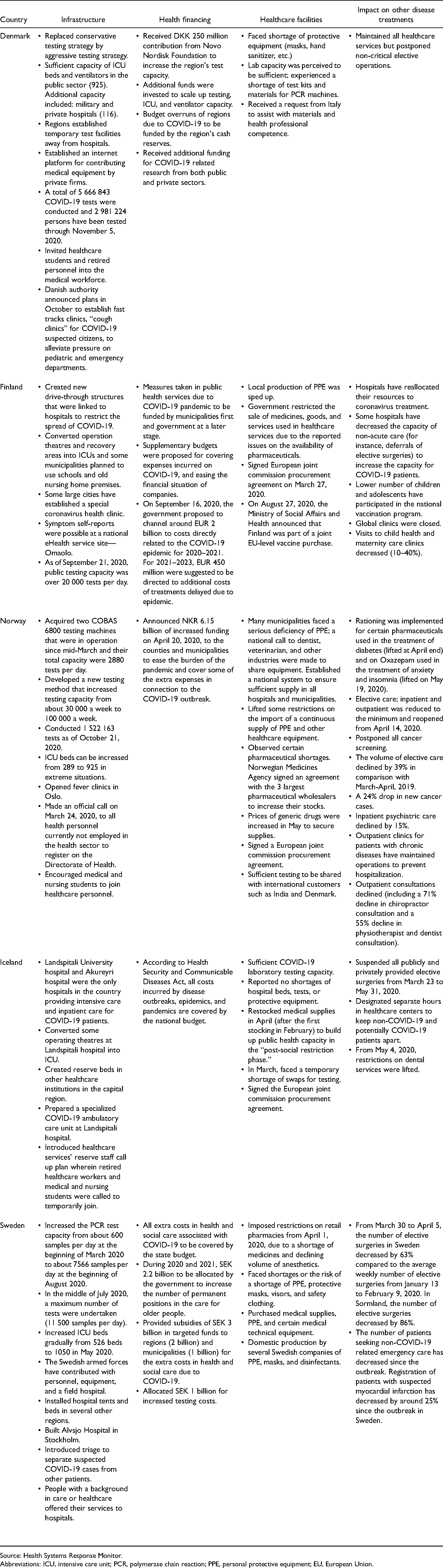
Source: Health Systems Response Monitor.
Abbreviations: ICU, intensive care unit; PCR, polymerase chain reaction; PPE, personal protective equipment; EU, European Union.
Discussion
To the best of our knowledge, this is the first comprehensive study of the COVID-19 epidemiology in the Nordic region, encompassing the public health system response to tackle the pandemic. Nordic countries constituted 3.62% of the European population and accounted for 2.07% of cases in Europe. Over 81.01% of deaths in the Nordic region were observed in Sweden, followed by Denmark (10.03%). In Sweden, 1 in 5 individuals was found at an increased risk of severe COVID-19. 20 The CFR of the Nordic region was 2.79%, which was close to the CFR of the global (2.51%) and European region (2.44%). Sweden (60.35 per 100 000) recorded the highest mortality rate among Nordic countries, yet its mortality rate was lower than a few European countries, such as Belgium (112.9 per 100 000), Spain (83.08 per 100 000), and United Kingdom (72.39 per 100 000). Other Nordic countries (eg, Norway [5.29 per 100 000], Finland [6.52 per 100 000], and Iceland [7.07 per 100 000]) were also among the European countries with low mortality rates.
Our findings reveal that females (52.33%) are more susceptible to coronavirus infection, while deaths (54.7%) and ICU admissions (72%) were higher among males. We also found that males were at a higher risk of being severely affected than females, which may be explained by immune regulatory genes encoded by the female X chromosome. 21 The female X chromosome causes lower viral load levels; thus, less inflammation occurs in females than males due to the virus. 21 Consistent with other studies, we found that COVID-19 susceptibility in the Nordic region varies across age groups, 22 with a low attack rate in individuals aged 0 to 9 years (5896 cases [2.25%]) and the highest incidence in the 20- to 29-year-old age group (52 171 cases [19.87%]). Our results are consistent with the 11th risk assessment report of European Centre for Disease Prevention and Control on the European Union/European Economic Area and the United Kingdom, which also observed the largest proportion of incident cases in younger adults (20-29-year-old age group) during June–July. 23 This finding has a significant public health implication; the younger population is responsible for driving virus transmission since this age group is socially and economically active. Young adults are more likely to be asymptomatic or have mild symptoms, and therefore, they may unknowingly spread the virus and increase the risk for vulnerable populations. 24 The distribution of COVID-19 deaths across different age groups was different from that of incidence; the highest number of deaths were reported in the eldest age group led by 80 to 89 years (3065 deaths [41.07%]) in line with previous research. 25
COVID-19 has impacted all the countries, but its consequences have been more severe on the lower socio-economic groups, disadvantaged and vulnerable sections of the population. For instance, a study found that being male, unmarried, having a low individual income, lower education, and being born in a low- or middle-income country all independently predict a higher risk of death from COVID-19. 26
The Nordic region was lauded for its early success in combating the virus spread, although it witnessed a resurgence in cases from September 2020. Nordic countries undertook proactive and prompt policy interventions compared to few severely hit European countries, such as Italy, Spain, and France, which were late in implementing restrictions. 27 For instance, Iceland was the quickest in implementing restrictions and declared a state of emergency on the same day when the domestic spread of the virus was identified first (March 6). 15 Similarly, Denmark was one of the first European countries to act firmly against the virus by declaring a national lockdown and closing its borders. 28 Nordic countries adopted different response strategies to tackle and curtail the virus transmission. Sweden followed a mitigation strategy that aimed to slow down the virus spread and reduce healthcare demand while shielding those at a higher risk rather than following a suppression strategy (which aims to rapidly reverse the epidemic growth). 29 Denmark adopted a mitigation strategy 15 and Norway resorted to a suppression strategy followed by a control strategy. 30 Norway was the first European country to have claimed the situation under control, as the number of hospitalized COVID-19 patients decreased and the number of deaths remained low. 30 Finland took stringent measures (eg, Emergency Powers Act) and moved gradually to a hybrid strategy to combat the virus spread (from extensive restrictive measures to enhanced epidemic management). 31 Although Iceland did not impose lockdown, due to low population density (3.52 people per square km of land area), 32 a small population (339 031), 7 intervention strategies (easing of restrictions after the first wave was over and a long period of 59 days from the first restriction implemented), 15 and aggressive testing, 33 the country has managed to maintain one of the lowest per capita mortality.
Few lessons and strategies could be learned from Nordic countries, such as their prompt response, strong information and surveillance system, and improved contact tracing through mobile apps in Iceland, Norway, Finland, and Denmark. 15 Even when used by a small proportion of the population, the contact tracing apps, subject to the isolation of symptomatic cases, can facilitate containment and achieve successful epidemic mitigation. 34 Norway resorted to contact tracing and testing since the first case was reported in late February 15 ; Denmark adopted a unique strategy to test even their blood donors, which is about 5% of their population 15 ; Iceland reported the highest per capita testing rate worldwide as of April, 2020. 33 The number of COVID-19 patients who survived in intensive care in Norway was among the highest in the world, illustrating the high-quality patient care and facilities in Norwegian hospitals. 30 To track healthcare facilities and resources, Sweden developed a platform to share real-time data with health authorities on the number of COVID-19 patients, ventilators, personal protective equipment, staff, and other health resources information. 35 In the Nordic region, access to medical and nursing care services was increased with better availability of telemedicine and healthcare advice via telephone calls. 15 Telehealth proved helpful in providing remote assessment and routine healthcare services and continuing non-COVID healthcare services without exposure to crowded hospitals and virus transmission. 36
The Nordic region did encounter some pitfalls and shortcomings. For instance, in Norway, widespread testing was not done, and it was reserved for people with symptoms, healthcare workers, and vulnerable population as of September 2020. 37 In Sweden, many deaths occurred in non-ICU patients, which suggests the prognosis of patients was considered in ICU admission that reduced the burden on healthcare but at the cost of decreased survival in patients not admitted. 38 Sweden did not impose lockdown but rather relied on its citizens’ voluntary social distancing and self-restraint to contain COVID-19. 15 A study conducted in the European context found a substantial effect of lockdown on reducing transmission with an estimated 81% (75%-87%) reduction in reproduction number. 39 Moreover, Sweden adopted fewer restrictions than Denmark, Finland, and Norway. 27
The Nordic region and other countries facing a recent upsurge in COVID-19 cases can learn from the experiences of other countries to contain the second wave. For instance, Germany and South Korea have maintained low fatality through widespread testing and digital health interventions40,41; China has used artificial intelligence-powered surveillance cameras and drones to monitor and restrict public gatherings 42 ; New Zealand adopted stringent countrywide lockdown (designated alert level 4) as a virus elimination strategy. 43 Early detection through comprehensive surveillance, aggressive testing, and contract testing has helped Singapore contain the virus. 44 South Korea, 41 Taiwan, 45 and Hong Kong 46 have adopted digital technology to monitor quarantined individuals to prevent the breach of isolation. Western Pacific countries have embedded preventive behaviors such as teleworking, mask-wearing, and physical distancing in their daily life as economies continue to unlock and revive. 47
We also observed that non-COVID-related healthcare services and elective surgeries had declined considerably due to the COVID-19 outbreak. There is a need to scale-up screening and follow-up activities of especially chronic noncommunicable diseases (NCDs) (eg, cancer, diabetes, and hypertension); the NCDs, cumulatively, are estimated to account for 90% of all deaths in Iceland and Denmark and 87% deaths in Norway. 48 Also, patients inflicted with NCDs are at a higher risk, 49 making it imperative to maintain a strict vigil on the elderly care and contain virus spread in those inflicted with NCDs. Sweden reported a 63% decline in the number of elective surgeries from March 30 to April 5, 2020, compared with January 13 to February 9, 2020, and Norway witnessed a 24% drop in new cancer cases, possibly due to the postponement of cancer screening activities due to the COVID-19 pandemic. 15 A streamlined response to COVID-19 in the context of NCDs is imperative to reduce the impact of this pandemic on the vulnerable groups.
Limitations of This Study
There was a lack of data availability on the gender-wise distribution of deaths and ICU admission and age-wise distribution of the ICU admission for Iceland. Also, data on the age-wise distribution of cases were not available for Iceland. Gender-wise distribution of cases and age-wise distribution of deaths in Iceland was only reported through June 14, 2020, and gender-wise distribution of cases in Finland was reported through September 7, 2020. Moreover, due to several data sources and lags in reporting from different agencies, data on different metrics (apart from the number of cases) is on different dates. Finally, we could not retrieve more detailed patient-level data on comorbidities of deceased patients. As a large percentage of deaths occurred in patients who had a history of some chronic disease or illness, 50 it would be worthwhile to examine the same in the context of Nordic countries as well.
Conclusion
Nordic countries controlled the virus transmission during the initial months; however, in line with the worldwide upsurge in the number of COVID-19 cases, Nordic countries are also witnessing an increase in cases recently; making it imperative to continue with extensive testing, contract tracing, and surveillance along with other measures such as social distancing, mandatory mask-wearing, and hand hygiene. Governments should focus on targeted response to asymptomatic transmission among the younger population, deliver age-appropriate prevention messages, identify and target new hotspots to contain virus spread, and develop a sustainable response model to suppress new COVID-19 cases while reviving their economies. Also, while the public health systems across the world are focusing on controlling the virus spread, the emphasis on screening, prevention, and follow-up activities of other chronic diseases is warranted, as any delay or further upsurge may lead to increased morbidity, disability, and increased mortality in patients with chronic conditions. Lastly, in this study, we focused on epidemiology and public health response in the Nordic countries; however, there would be several socio-cultural, economic, and environmental factors affecting the COVID-19 epidemiology. Such a detailed examination of the various factors on the virus spread and various epidemiological metrics can be an agenda for future research.
Footnotes
Acknowledgments
The authors would like to thank the European Centre for Disease Prevention and Control, Directorate of Health, Department of Civil Protection and Emergency Management, Finnish Institute for Health and Welfare, Statens Serum Institut, Norwegian Institute of Public Health, and Folkhälsomyndigheten for making the data publicly available.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.