
Abstract
This article examines the distribution patterns of primary health care centers (PHCC) in the 30 Local Government Areas (LGAs) of Osun State, Nigeria, using secondary data. The study focused on the problem of inequality and inadequacy in the distribution pattern of PHCCs among the population. The provision of PHCCs in the state was analyzed using three criteria: among the three senatorial districts; among the 30 LGAs; and on the basis of population per PHCC. Findings revealed that although PHCCs were almost equally distributed among senatorial districts, disparities exist in distribution patterns among the LGAs and within each senatorial district and in terms of population ratio per PHCC in the state. Sixty percent (60%) of the LGAs had fewer than 26 PHCCs, which is the expected average number of PHCCs in the state. The inequalities observed in the study favored rural areas against urban areas. The study further revealed inadequacies in the provision of PHCCs in terms of the population ratio per PHCCs. The study concluded that to achieve the Sustainable Development Goals (SDGs) by 2030—and to contain the COVID-19 pandemic—there is a need for government intervention in the provision of PHCCs in Osun State for equal and adequate distribution.
Keywords
The International Conference on Primary Health Care held on September 12, 1978, in Alma-Ata, the capital of the Soviet Republic of Kazakhstan, located in the Asiatic region of the Soviet Union, expressed the need for urgent action by all governments, all health and development workers, and the world community to protect and promote the health of all the people of the world, and hence made declarations, some of which include 1 : “The conference strongly reaffirms that health, which is a state of complete physical, mental and social well-being, and not merely the absence of disease or infirmity, is a fundamental human right and that the attainment of the highest possible level of health is a most important world-wide social goal whose realisation requires the action of many other social and economic sectors in addition to the health sector.”
The conference went further in its 1978 declaration to state that 1 : “The existing gross inequality in the health status of the people, particularly between developed and developing countries, as well as within countries, is politically, socially, and economically unacceptable and is, therefore, of common concern to all countries.”
Considering the extent of health problems and the inadequate and unequal distribution of health resources between and within countries—and, more importantly, believing that health is a fundamental human right and worldwide social goal—the conference advocated for a new approach to health and health care to bridge the gap between the “haves” and “have nots,” achieve more equitable distribution of health resources, and attain a level of health for all the citizens of the world that will permit them to lead socially and economically productive lives.
To achieve this objective, the conference introduced the primary health care (PHC) approach. PHC was defined as: “The essential health care that is based on scientifically sound and socially acceptable methods and technology, which makes universal health care accessible to all individuals and families in a community. It is through their full participations and at a cost that the community and the country can afford to maintain at every stage of their development in the spirit of self-reliance and self-determination. 2 ”
PHC is an approach to health and a spectrum of services beyond the traditional health care system that focuses on health equity-producing social policy.3,4 That is, PHC includes all services that play a role in health, such as access to health services, environment, and lifestyle. 5 Thus, PHC and public health measures, taken together, may be considered as the basis of universal health systems. 6
The World Health Organization (WHO) further expatiates on the goals of PHC as defined by three major categories: “empowering people and communities, multisectoral policy, and action; primary care; and essential public health functions as the core of integrated health services”. 7 According to these definitions, PHC can not only help an individual after a diagnosis of disease or disorder, but also actively prevent such issues by understanding the individual as a whole.
PHC is believed to form an integral part both of the country's health system, of which it is the central function and main focus, and of the overall social and economic development of the community. It is the first level of contact of individuals, the family, and the community with the national health system, bringing health care as close as possible to where people live and work, and constitutes the first element of a continuing health care process.
Despite all the intensive efforts to achieve universal health for all in 2000, many countries, including Nigeria, could not provide adequate and equitable health for all their citizens. Hence, the introduction of the Millennium Development Goal (MDG) agenda, which was signed by 134 countries in 2000 and expected to achieve some development before the end of 2015.
Due to the failure of many developing countries, including Nigeria, to meet the MDG targets, the Sustainable Development Goals (SDGs)—a collection of 17 global goals set by the United Nations (UN) General Assembly that serve as the blueprint to achieve a better and more sustainable future for all—were adopted in 2015, to be met by the year 2030, by 193 countries of the UN General Assembly to succeed the MDGs. 8 The SDGs address the global challenges facing UN member countries, including those related to poverty, inequality, climate, environmental degradation, prosperity, peace, and justice. The SDGs interconnect and attempt to leave no one behind.
SDG 3 emphasizes ensuring healthy lives and promoting well-being at all ages. It aims to achieve this goal by ensuring universal health coverage, including access to essential medicines and vaccines. 9 It also proposes to end the preventable death of newborns and children under age 5 and to end epidemics such as AIDS, tuberculosis, malaria, and water-borne diseases.
Currently, the world is facing a global health crisis known as coronavirus (COVID-19), which started as an epidemic in the Wuhan province of China in December 201910,11 and was declared by the WHO as a pandemic in March 2020.12,13 COVID-19 has affected more than 222 countries worldwide, 14 creating public health emergencies with considerable incidence of morbidity and mortality and destabilizing the economy. Thus, the health emergencies related to COVID-19 have posed a global risk and have necessitated the need for many governments, including Nigeria, to embark on lockdown measures that include stay-at-home orders; closure of financial markets, corporate offices, and businesses; travel restriction locally and internationally; postponement or cancelation of events; curfews; and physical distancing to control the spread of COVID-19.
The continuous spread of the virus and the lockdown measures, such as stay-at-home-orders and physical distancing, put in place to contain the spread of the virus emphasize the need to improve accessibility to PHC through increased access to physicians, efficient funding of the health systems, and equality and adequacy in the distribution pattern of PHC centers (PHCCs). This is necessary to enable people to access PHCCs closer to their homes to seek health care, especially at a time of a pandemic lockdown, which may not permit people to seek care from higher levels of health care facilities due to lack of mobility enforced to contain the spread of the virus and to prevent excessive mass gathering/overcrowding of patients in the secondary and tertiary health care facilities in the state and in Nigeria generally.
As of January 5, 2022, in Nigeria, 856 new confirmed cases of COVID-19 were recorded, 245 404 cases had been confirmed, 217 247 cases had been discharged, and 3058 deaths had been recorded in 36 states and the Federal Capital Territory. 15 Common symptoms of COVID-19 include fever or chills, cough, shortness of breath or difficulty breathing, fatigue, muscle or body aches, new loss of taste or smell, loss of speech or mobility or confusion, chest pains, congestion or runny nose, nausea, and vomiting.16,17 Less common symptoms of COVID-19 may include a rash on the skin or discoloration of fingers or toes, red or irritated eyes, sore throat, headache, diarrhea, aches, and pains. 18 Complications may include pneumonia and troubled breathing, organ failure in several organs, heart problems, a severe lung condition that causes a low amount of oxygen to go through the bloodstream to the organs (acute respiratory distress syndrome), blood clots, acute kidney injury, and additional viral and bacterial infections. 19
COVID-19 has been presented in variants including Alpha, Beta, Gamma, and Delta. 20 The latest COVID-19 variant, which raised much concern for WHO, was named Omicron on November 26, 2021, 21 on the advice of WHO's Technical Advisory Group on Virus Evolution (TAG-VE). The Omicron variant (also known as B.1.1.529), a variant of concern, was first reported in Botswana and then South Africa, but has since spread to many other countries. Omicron was reported to have an unusually high number of mutations, which allows it to penetrate and infect more people. The origin was initially said to be unknown, but scientists in South Africa alerted the WHO recently that the Omicron variant was found among travelers arriving from several countries, from Australia to Israel to the Netherlands, 22 and it is likely to circulate more widely and for a longer time. Among the unknowns about the Omicron variant are its severity, its ability to evade vaccines, and its transmissibility. Some health authorities currently believe the variant to be more contagious. 23 However, the same rules for containment apply to Omicron as to any other variant: vaccine equity; universal access to treatments, masks, and hygiene maintenance; and poverty reduction measures. 22
Amid the panic over Omicron, Nigeria, Africa's most populous nation, which has recorded more than 3000 COVID-19 deaths, recently implemented a requirement that all federal government employees get vaccinated against COVID-19 or present a negative COVID-19 test completed in the last 72 h. 23
As of December 1, 2021, Nigeria had confirmed its first cases of Omicron variant of the coronavirus in three travelers from South Africa. This made Nigeria the first West Africa country to have recorded cases of the Omicron coronavirus variant. 23 Canada had already reported cases of the variant in Canadians who had recently returned to Canada from Nigeria and expanded a travel ban around the globe, to include Nigeria and nine other African countries. 24 As December 21, 2021, Nigeria Centre for Disease Control had confirmed 49 cases of the COVID-19 Omicron variant in Nigeria. 25
Currently, in Nigeria and in Osun State, the federal government under the leadership of President Muhammad Buhari is determined to ensure that every eligible Nigerian and indeed every person in Nigeria has access to the COVID-19 vaccine. As a result of this commitment to all Nigerians, COVID-19 vaccines have been designated to various public primary, secondary, and tertiary health care facilities, as well as private health facilities, in order to recover quickly from the social and economic losses due to the COVID-19 pandemic. 26
However, for effective management of victims with symptoms of COVID-19, the article argues that because only three Local Government Areas (LGAs) (Ife Central, Ilesha East, and Osogbo local governments) have one teaching hospital each, out of the 30 LGAs, 27 it may not be easy for these three teaching hospitals alone to identify all patients with COVID-19 symptoms in the state. Additionally, only five general hospitals are available in the state, and they are all situated in rural LGAs (Ejigbo, Ife North, Ife South, Odo Otin, and Oriade) 27 ; therefore, these general hospitals cannot be suitable and adequate for proper management of patients with COVID-19 symptoms and dissemination of COVID-19 vaccines to all 30 LGAs. The absence of general hospitals in urban areas will also limit the benefits of COVID-19 vaccines and treatment of the urban population.
Based on these facts, the article therefore argues that because PHCCs are available in all the LGAs of the state (rural and urban), and they are equipped with personnel adequately trained in COVID-19 presentation and referral systems to get COVID-19 patients to designated centers in the state while they are fully involved in the vaccination process, it is believed that equal and adequate distribution of PHCCs would facilitate easy identification of patients with COVID-19 symptoms and treatment, on a local government basis, and that this would also help to avoid overcrowding in the few available secondary and tertiary health care facilities designated for COVID-19 vaccines and treatment.
Many studies have been conducted on COVID-19, but to the best of the researchers’ knowledge, none has been conducted on the distribution pattern of PHCCs and its implications for sustainable development and containment of the COVID-19 pandemic in Nigeria. It is against this backdrop that this study has set out to analyze the distribution patterns of PHCCs in Osun State, focusing on the problem of inequality and inadequacy, as well as the implications of these problems on the SDG 3 agenda (healthy living for all at all ages) and containment of the COVID-19 pandemic in the state.
One of the major inspirations for PHC was the global popularity and the expansion of rural medical services in Communist China, especially the “Barefoot Doctors.” They demonstrated the effectiveness of having a health care professional at the community level with community ties. Barefoot Doctors were selected group of village health workers who lived in rural areas of China and received basic health care training. They were more concerned with rural rather than urban health care and focused on preventive rather than curative services. They also provided a combination of Western and traditional medicines. The Barefoot Doctors had close community ties, were relatively low-cost, and, perhaps most importantly, encouraged self-reliance by advocating prevention and hygiene practices. 28 The program experienced a massive expansion of rural medical services in China, with the number of Barefoot Doctors increasing dramatically between the early 1960s and the Cultural Revolution (1964-1976). 28
Since the post-colonial administration, Nigeria has had four successive national development plans, namely: the First National Development Plan (1962-1968), Second National Development Plan (1970-1974), Third National Development Plan (1975-1980), and Fourth National Development Plan (1981-1985). 29 The Second National Development Plan (1970-1974) clearly indicated that situations in which some parts of the country experienced rapid growth and development while other parts lagged behind could no longer be accepted. 30 The thrust of the Second National Development Plan, therefore, was “to establish Nigeria as a united, strong, and self-reliant nation; a great and dynamic economy; a just and egalitarian society; land of bright and full opportunities for all citizens; and free and democratic society”. 31
The Third Development Plan (1975-1980) for Nigeria focused on inequality in the distribution of medical facilities and health manpower in the country. The Plan, therefore, accelerated health manpower production and aimed to reduce the imbalance in the distribution of facilities. The Fourth Plan (1981-1985) categorically stated the need to ensure a more equitable distribution of health facilities and manpower for every part of the Federation. 32
In 2005, Federal Ministry of Health estimated a total of 23 640 health facilities in Nigeria, of which 85.8% are PHC facilities, 14% secondary, and 0.2% tertiary. Thirty-eight percent (38%) of these facilities were owned by the private sector, which provides 60% of health care in the country. 33 While 60% of the public PHC facilities were located in the northern zones of the country, they are mainly health posts and dispensaries that provide only basic, curative services. Private, out-of-pocket expenditure in Nigeria accounts for more than 70% of the estimated $10 per capita expenditure on health, 34 limiting equitable access to quality health care.
The public health service is organized into primary, secondary, and tertiary levels. While the Constitution is silent on the roles of the different levels of government in health services provision, the National Health Policy ascribes responsibilities for PHC to local governments, secondary care to states, and tertiary care to the federal level. At the same time, a number of parastatals based at the federal level—for example, the National Primary Health Care Development Agency—are currently engaged in PHC services development and provision; the latter is evidently part of its mandate. Although national policies formulated by the Federal Ministry of Health provide some level of standardization, each level is largely autonomous in the financing and management of services under its jurisdiction. 35
The health system is in a deplorable state, with an overall health system performance ranking 187th out of 191 member states by the WHO. 36 The health system remains overstretched by its expanding population,35,37 physical facilities are decaying, equipment is obsolete, and there is scarcity of skilled health professionals.35,38 Low salaries and poor working conditions have resulted in a mass exodus of health professionals 38 that, together with widespread poverty and lack of financial resources for the provision of health facilities/infrastructure, 37 accounts for the poor provision and differentials in health care facilities in Nigeria. As reported previously,32,38 there has been too much concentration of medical personnel in urban areas, to the neglect of the rural areas.
In addition, the roles of stakeholders are misaligned, and coordination systems are weak. These are further compounded by the dearth of data that renders evidence-based planning, policy formulation, and health systems management weak.35,39
PHC, which forms the bedrock of the national health system, is in a prostrate state because of poor political will,35,39 gross underfunding, and lack of capacity at the LGA level, which is the main implementing body. 35
One of the numerous functions of the local government is the provision of PHC facilities, especially to bring health care facilities closer to the grassroots. However, achieving this function by most local governments in Nigeria has been a major challenge. This is due to a number of factors that include inadequate medical personnel who are forced out by inherent “push factors,” including economic uncertainty, insecurity, tribal and religious crisis, and uneven distribution of health care facilities, not only in rural areas of the developing world but also in urban areas, because of limited health care facilities and the fact that the few health professionals prefer to work in the urban centers where they can be well remunerated. 40
Lack of infrastructure in rural sectors, including inadequate health care facilities, contributes to inefficiency in production and declining productivity. 41 Hence, provision for adequate health facilities in rural areas requires adequate information and data about the present situation to determine which areas require what and which strategies to adopt in providing facilities where there are gross inadequacies.
Despite government efforts to ensure a more equitable distribution of resources, disparities are still obvious. Although the financial capacity to implement the plan was there, the political will was almost completely absent. 39 Nigerians were more concerned with sharing the oil booty than implementing the development plan. Factors such as misplacement of priorities, poor planning discipline, lack of effective executive capacity, public-sector inefficiency, technology transfer syndrome, systemic corruption, inefficacious public–private partnership,31,39 and lack of comprehensive statistics 39 have made a genuine development plan unrealistic. These and many other factors have contributed to the unequal distribution of health care facilities in Nigeria, Osun State, Southwestern Nigeria inclusive.
Study Location
Osun State is an inland state in southwestern Nigeria. Its capital is Osogbo. Having been established on August 27, 1991, during General Ibrahim Babangida's administration, the State of Osun is one of the younger states in Nigeria, and in recent years the state government has made ambitious efforts to expand and develop the local economy. Named after the River Osun, linked to the Yoruba goddess of fertility, the state was carved out from the former territory of Oyo State during a boundary re-drawing in the 1990s. Over the past two and a half decades, Osun has grappled with many of the same challenges as other states in the country—poorly maintained infrastructure, irregular federal funding, and inadequate social services—but a spate of reforms are aiming to address those issues. 42 The Osun State Government has made efforts to renovate the PHCCs and general hospitals.
Osun State is bounded in the north by Kwara State, in the east partly by Ekiti State and partly by Ondo State, in the south by Ogun State, and in the west by Oyo State. It is one of the 36 states that make up Nigeria, and it occupies 9251 square kilometers. Osun State is located within the cocoa belt of southwestern Nigeria. Although there are patches of savannah in the northern part of the state, most of the state is still tropical rainforest vegetation.
Osun State can be classified as a largely rural state, with 20 out of 30 LGAs being non-urban local government councils, accounting for more than 65% of the projected population in 2016 43 —that is, local government with one or two towns with basic infrastructural development as the major settlement, while a larger percentage of the local government lacks basic infrastructural facilities. Yoruba and English are the languages of the people for official and business transactions.
Materials and Methods
The study employed secondary sources of data collection obtained from Osun State Ministry of Health, 44 Osun State Hospital Management Board, 27 and projected National Population Commission, 2016, and National Bureau of Statistics, 2016. 43 The raw secondary data from these sources were compared for confirmation and to avoid inaccuracies in the data set. The data were categorized based on the three senatorial districts and the 30 LGAs in the state. The 30 LGAs were also categorized into rural or urban areas based on level of infrastructural facilities development in each LGA, such as roads, electricity, drinking water, housing, communication services, and sewage treatment. Categorization also includes the nature of occupational opportunities in each LGA.
Thus, the categorization of the data produced the distribution pattern of PHCCs in the state. The indicator of inadequate and unequal distribution pattern of the PHCCs in the state was computed using population ratio to number of PHCCs (Pop/PHCC) available in each senatorial district and LGA in the state. The choice of this indicator was influenced by the fact that the WHO in its Alma Ata Declaration 1 and the Second, Third, and Fourth National Development Plans emphasized a balanced development across the countries,29–32,38,39 which includes equal distribution of medical facilities and manpower/personnel.
Results
The result of the study is discussed here using three approaches. The first approach adopted analyzed the result in Table 1 based on senatorial districts. The second approach adopted in the analysis was based on LGAs (Table 2), and the third approach was based on number of population per PHCC (Table 3). Data obtained from Ministry of Health in Osun State (2016) on available numbers of PHCCs in the state and the projected population for 2016 were used for the analysis.
Distribution Patterns of PHCCs at the Senatorial District Levels in Osun State.
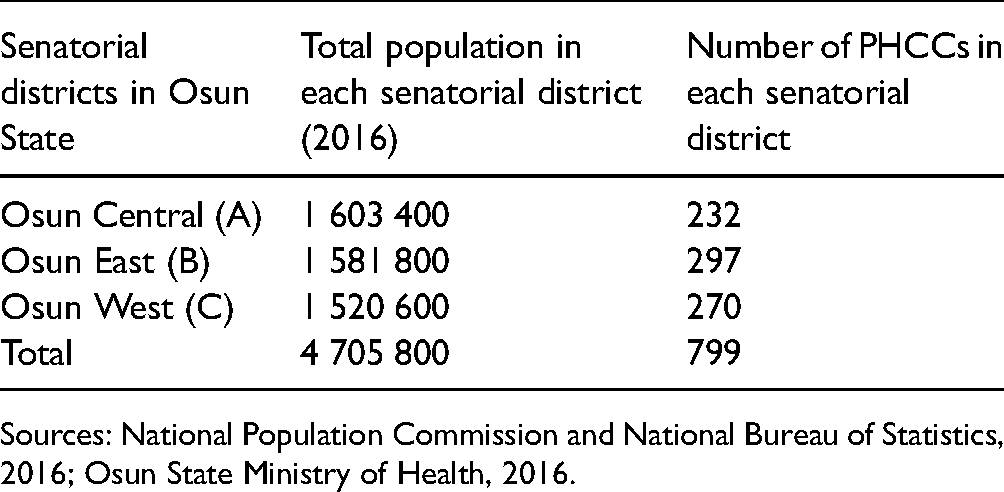
Sources: National Population Commission and National Bureau of Statistics, 2016; Osun State Ministry of Health, 2016.
Distribution Patterns of PHCCs at the LGA Levels in Osun State.
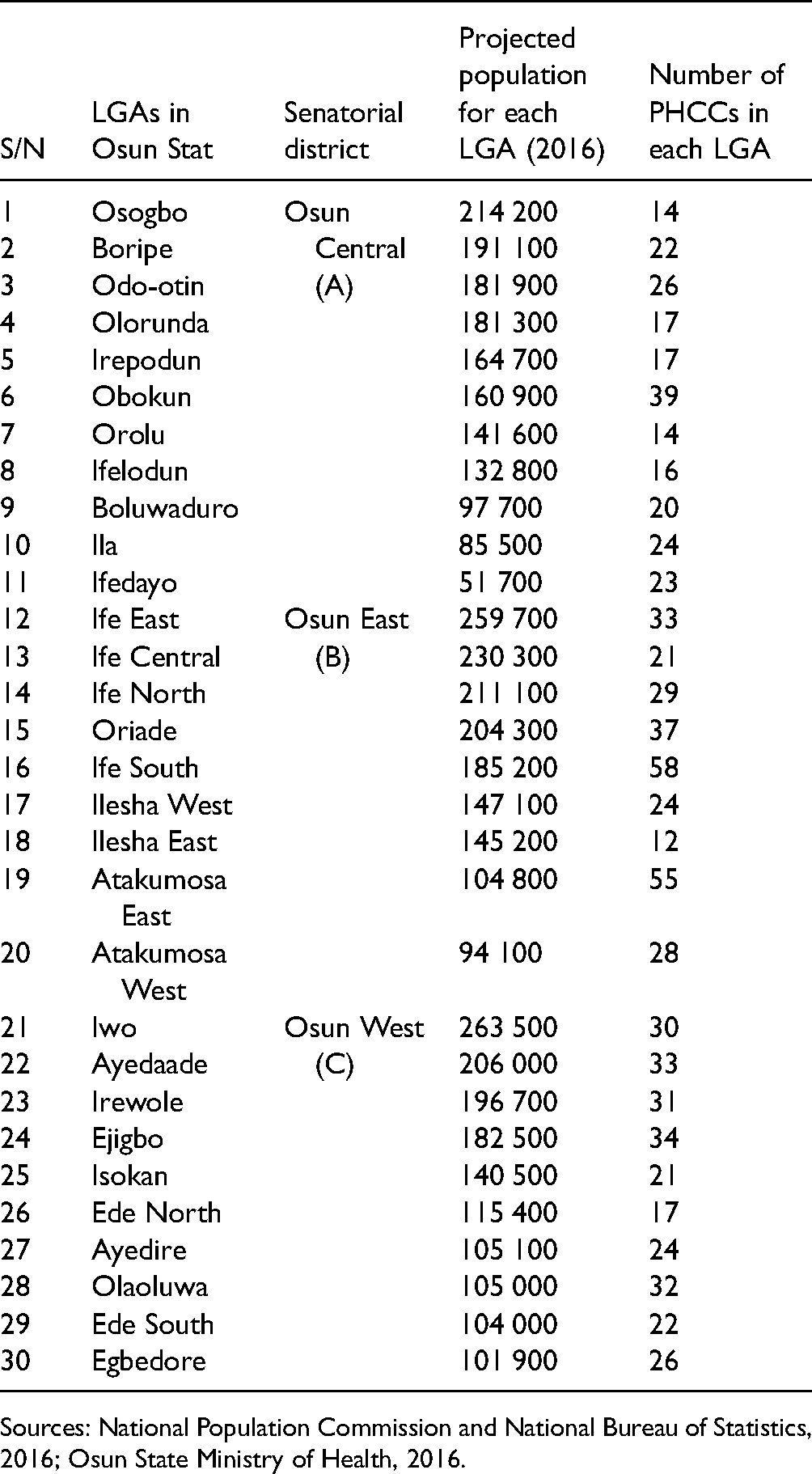
Sources: National Population Commission and National Bureau of Statistics, 2016; Osun State Ministry of Health, 2016.
Distribution Patterns of PHCCs in Osun State, Considering Population Ratio/PHCC.
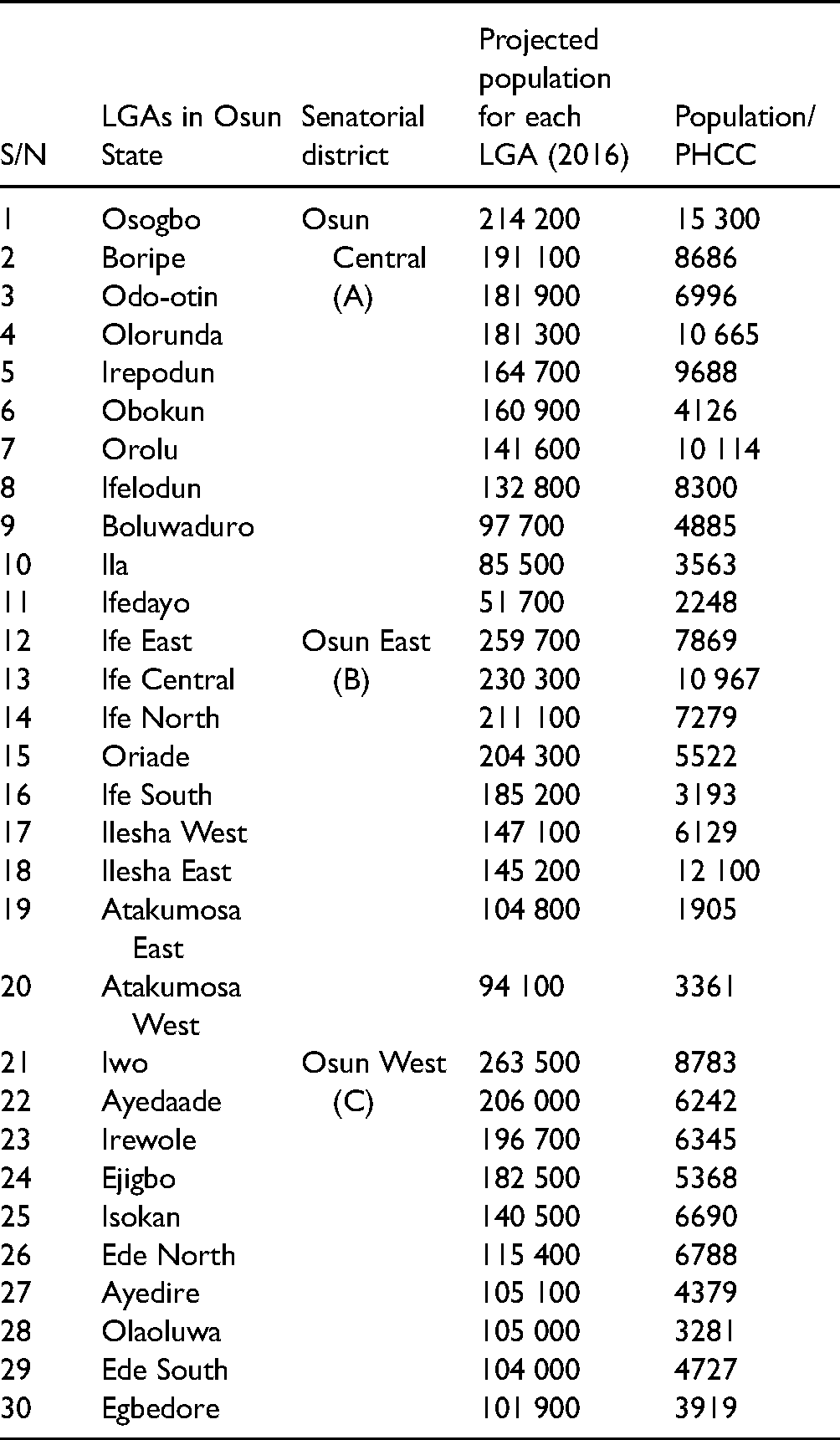
Table 1 shows the distribution pattern of PHCCs at the senatorial district levels in Osun State. There are a total number of 799 PHCCs in Osun State. 44 The distribution pattern of PHCCs among the three senatorial districts seems to be fairly equitable. This may be due to government policy to ensure a balanced development in the state. However, with equal distribution of PHCCs among the three senatorial districts, it would be expected that each district should have at least 266 PHCCs. If the population of each district is also taken into consideration, it would be expected that Osun Central senatorial district should have the highest numbers of PHCCs in the state because it has the highest population when compared to the other two senatorial districts—Osun East and Osun West, as shown in Table 1—but this is not the case.
Despite the fact that Osun Central senatorial district has the highest number of population (1 603 400), it has the lowest number of PHCCs (232) when compared to Osun East with a population of 1 581 800 and 297 PHCCs and Osun West with a population of 1 520 600 with 270 PHCCs.
Table 2 shows the distribution pattern of PHCCs at the LGA levels in Osun State. With a total of 799 PHC facilities, and with even distribution of PHCCs in the state, each of the LGAs should have at least 26 PHCCs. However, there are inequalities in the distribution pattern of PHCCs among the LGAs. Ife South LGA, with a population of 185 200, has the highest number of PHCCs (58) in the state, as against Osogbo, which has 14 PHCCs and a population of 214 200, and Boripe, with 22 PHCCs and a population of 191 100 in Osun Central senatorial district.
Also in Osun East senatorial district, to which Ife South LGA belongs, there are gross inequalities in the distribution pattern of PHCCs among the LGAs in the district. Ife East has 33 PHCCs with a population of 259 700, Ife Central has 21 PHCCs with a population of 230 300, Ife North has 29 PHCCs with a population of 211 100, and Oriade has 37 PHCCs with a population of 204 300. All four LGAs (Ife East, Ife Central, Ife North, and Oriade) in Osun East senatorial districts have a higher population than Ife South LGA, yet Ife South had almost twice the number of PHCCs when compared to these four LGAs. This is a gross inequality in the distribution pattern of PHCCs in the district and in the state generally.
The unequal distribution of PHCCs is also reflected in Osun West senatorial district when compared to the number of PHCCs allocated to Ife South LGA as against 58 PHCCs in Ife South LGA, with a population of 185 200. In Osun West senatorial district, Iwo LGA has 30 PHCCs and a population of 263 500, Ayedaade LGA has 33 PHCCs with a population of 206 000, and Irewole LGA has 31 PHCCs and a population of 196 700.
Generally, the Ife South LGA has the highest PHCCs (58) in the state with a population of 185 200. Next is Atakumosa East LGA, with 55 PHCCs and a population of 104 800. This is followed by eight LGAs (Iwo [30], Irewole [31], Olaoluwa [32], Ayedaade [33], Ife East [33], Ejigbo [34], Oriade [37], and Obokun [39]) having between 30 and 39 PHCCs. Thirteen LGAs have PHCCs within the range of 20 to 29: Boluwaduro (20), Isokan (21), Ife Central (21), Boripe (22), Ede South (22), Ifedayo (23), Ila (24), Ayedire (24), Ilesha West (24), Egbedore (26), Odo-Otin (26), Atakumosa West (28), and Ife North (29). The remaining seven LGAs—Ilesha East (12), Osogbo (14), Orolu (14), Ifelodun (16), Olorunda (17), Irepodun (17), and Ede North (17)—have between 12 and 17 PHCCs.
Generally, 16 out of 30 LGAs in the state have fewer than 26 PHCCs, which is the average, while 12 LGAs have above the state average and only two LGAs have exactly the expected, average number of PHCCs. 26 It is also important to note that 13 out of the 33 PHCCs in Ife East LGA belong to the Modakeke Area office. 44
The most marginally disadvantaged local governments in the provision of PHCCs in Osun Central senatorial district are Osogbo and Orolu LGAs, with each LGA having 14 PHCCs. Osogbo LGA has the highest population in the district (214 200), but is one of the LGAs with the lowest PHCCs. The implication of this distribution pattern is that there will be more pressure on the few PHCCs in the LGA.
The distribution pattern of PHCCs in Osun State in relation to the population ratio is shown in Table 3. The distribution pattern in the provision of PHC facilities in Osun State revealed many disparities, especially in the LGAs, and revealed inadequacy for the growing population. For instance, in Osun Central senatorial district, Osogbo LGA has a population of 214 200, which is the highest in the district. This implies having a population of about 15 300 per PHCC in the LG (see Table 3). The distribution pattern also affects Orolu LGA, having only 14 PHCCs with a population of 141 600. This also implied a population of 10 114 per PHCC in the LGA. There is a gross inequality in this distribution pattern when compared with the number of PHCCs in Ifedayo LGA, which has 23 PHCCs and a population of 51 700, or a population of 2248 per PHCC. Olorunda LGA is also at a disadvantage in terms of the PHCC distribution, having a population of 181 300 and 17 PHCCs, thus implying a population of 10 665 per PHCC in the LGA.
In Osun East senatorial district, the most marginally disadvantaged local governments in the provision of PHCCs are Ilesha East and Ife Central. Ilesha East has only 12 PHCCs with a population of 145 200. This implied a population of 12 100 per PHCC, and it is the second most marginally disadvantaged LGA in the provision of PHCCs in the state after Osogbo LGA. Ife Central LGA is also at a disadvantage in Osun East senatorial district in the provision of PHCCs, having 21 PHCCs and a population of 230 300. This implied a population of 10 965 per PHCC. These two LGAs (Ilesha East and Ife Central) are highly marginalized in Osun East senatorial district when compared to Atakumosa East and Atakumosa West, which have 55 and 28 PHCCs and populations of 104 800 and 94 100, respectively. Thus, in Atakumosa East, there is a population of 1905 per PHCC, while in Atakumosa West, there is a population of 3361 per PHCC.
The two most marginally disadvantaged LGAs in Osun West senatorial district are Iwo and Ede North LGAs, with Iwo having 30 PHCCs and a population of 263 500, which is the highest population in the district; thus, a population of 8783 per PHCC. Ede North also has 17 PHCCs and a population of 115 400. This also implied a population of 6788 per PHCC. These two LGAs (Iwo and Ede North) in Osun West senatorial districts are said to be at disadvantage because they are incomparable to other LGAs in the provision of PHCCs. For instance, Olaoluwa and Egbedore LGAs in Osun West senatorial district have 32 PHCCs and 26 PHCCs, respectively, with populations of 105 000 and 101 900, respectively. This implied Olaoluwa LGA has a population of 3281 per PHCC, and Egbedore LGA has a population of 3919 per PHCC.
Discussion
The total number of PHC facilities for Osun State was estimated at 610 in 2005 41 and at 799 in 2016. 44 However, the increment is in favor of the rural areas, and the distribution pattern of PHCCs in the state still reflects disparities among the three senatorial districts and among LGAs, as observed by the previous study. 41 The disparities in the distribution pattern of the PHCCs revealed that the location of these health facilities could have been influenced by politicians and administrators to favor some LGAs at the expense of others. Corruption is the order of the day in present-day Nigeria and exists in different forms, such as nepotism, bribery, extortion, and so on. Nepotism is the application of selfish and biased ways of distributing resources. Sometimes, nepotism could be done in favor of friends, family, or LGAs to the detriment of those who have no godfather 45 and without recourse to merit and necessity. Due to weak institutional governance, the public sector in Nigeria has become a bed of nepotism, 46 with the allocation of resources not necessarily based on needs but on those holding political positions and their affiliations in society. To enhance sustainable development in the management of publicly owned health care facilities, the distribution patterns of these facilities must be done in such a way that the principle of fairness, justice, and equity applies.
Unlike previous studies,37,38,41 whose findings revealed that most rural areas in Nigeria were at disadvantages in the provision of health care facilities when compared to urban areas, the present study has revealed a contrary finding: the inequality in the distribution of PHCCs favored rural areas at the expense of urban areas. The essence of development plans was to ensure balanced development, as pointed out earlier; however, balanced development should not imply that one area (urban or rural) should be marginalized at the detriment of the other. For instance, in Osun Central senatorial districts, there are 11 LGAs in the district, but only four LGAs belong to urban areas (Osogbo, Olorunda, Ifelodun, and Ila), and of these four LGAs, three (Osogbo, Olorunda, Ifelodun) have fewer than 20 PHCCs, while those that belong to the rural areas have 20 PHCCs and above, with the exception of Orolu and Irepodun, which have 14 and 17 PHCCs, respectively.
Also, given the available population statistics and the numbers of PHCCs in Osogbo and Orolu LGAs (Osun Central senatorial districts), there is the possibility of having more pressure on the PHCCs in these two LGAs, if they are adequately utilized. There are alternatives: For instance, while Osogbo LGA has one teaching hospital, one state hospital, and one comprehensive health center in addition to the 14 PHCCs, Orolu LGA, on the other hand, has one comprehensive health center in addition to the 14 PHCCs. 27 However, the utilization pattern of these PHCCs was not captured by the study. Hence, this calls for further research.
In Osun East senatorial district, a similar distribution pattern can be observed. Osun East consists of nine LGAs, out of which only three LGAs are urban areas (Ife Central, Ilesha West, and Ilesha East) having 21, 24, and 12 PHCCs, respectively. It is important to note that although these three LGAs belong to urban areas, they have the lowest number in the provision of PHCCs.
Considering the provision of PHCCs in Osun West senatorial districts, 10 LGAs make up the district, and only three LGAs (Ede North, Ede South, and Iwo) belong to urban areas, each having 17 and 22 PHCCs, respectively, except Iwo, which has 30 PHCCs. The remaining seven LGAs in the district belong to rural areas, and they have 24 or more PHCCs, with the exception of Isokan LGA, which has 21.
Although early findings suggested that the state of PHCCs in Nigeria, Osun State inclusive, is deplorable 36 and in a prostrate condition,35,39 recognition of the above-stated challenges as they affect the nation's health system triggered the Osun State Government to embark on the renovation of 332 PHCCs and the provision of equipment and essential medicines, together with the recruitment of adequate personnel in all the PHCCs in the state between 2019 and 2020, 47 with the promise of continuous availability of essential medicines.
This action changed the narrative to what we have now in the state—that is, well-renovated structures with essential medicines, equipment, and well-manned PHCCs for effective performance, which also helped the state in enhancing management of the COVID-19 pandemic.
In all, and contrary to previous findings, the majority of the PHCCs belong to rural areas, while very few belong to urban areas. Studies have revealed that the majority and almost two-thirds of Nigeria's population resides in rural areas.38,48 It was also argued that the most important sector of the Nigerian population is the rural area. 49 This is because a study has shown that the rural sector is, indeed, vital in the socioeconomic development of the nation. 50 Rural areas, for instance, are the major source of capital formation for the country and a principal market for domestic raw materials for industrial processes. Indeed, the rural areas engage in primary economic activities that form the foundation for the country's economic development. 43 Thus, for these reasons, one cannot condemn outright this distribution pattern.
However, another study 51 noted that rural poverty persists in Nigeria despite the prosperity created by the country's oil wealth, as evidenced by the difficulty experienced in getting basic daily needs such as food, water, and shelter. Lack of these basic needs in rural areas has made a number of rural dwellers migrate to urban areas with high hopes of improving their standard of living. Thus, the movement of people from rural areas to urban areas in search of greener pastures, which has led to congestion of the urban population, necessitated equal and adequate distribution pattern of PHC facilities in the state.
The implication of having equal and adequate PHCCs in the state for the attainment of SDG 3 (healthy living for all at all ages) and for the containment of the COVID-19 pandemic is that PHCCs are usually the closest health care facilities at the grassroots level, thus, equal and adequate distribution patterns will help the population access health care facilities closer to them. In order to ensure equitable access to quality health care services, which is one of the main thrusts of the present administration in Osun State, the national situation notwithstanding, the state government launched the Osun Health Insurance Scheme in 2018. 52 The essence of this plan is to guarantee universal health coverage to enable the citizenry to have access to quality health care services53,54 throughout the nooks and corners of the state.
During public health emergencies such as the COVID-19 pandemic, PHCCs have a significant role to play by helping to sort out patients (triaging) for screening, to be able to make diagnoses as early as possible, and to help reduce overcrowding in higher health care facilities as a measure to contain the spread of coronavirus in the state.
Aside from the disparities, the study also revealed inadequate provision of PHCCs for the growing population in each of the LGAs. The analysis of the distribution pattern of PHCCs in the state is far from the reality of the UN target of achieving universal health coverage, including access to essential medicines and vaccines, which are usually the functions of PHCCs. This is a great concern for the attainment of SDG 3 and containment of the COVID-19 pandemic, because when too many people have to rely on or share a health care facility such as a PHCC, this will enhance the spread of the disease rather than contain it. Additionally, as the global community is making efforts to vaccinate citizens against the deadly virus, the significant role of the PHCCs cannot be underestimated.
Recommendation
PHC facilitates community outreach and health promotion, as well as long-term monitoring and management of complications. PHCCs are also less expensive than health care facilities at the secondary and tertiary levels for patients, communities, and governments. In other words, PHC is cost-effective and, thus, governments should endeavor to invest more in PHCCs, especially those at a disadvantage in the senatorial districts/LGAs in Osun State, to achieve important health benefits; to contain the spread of COVID-19, which may result from overcrowding in higher health care facilities; and to enhance the dissemination of COVID-19 vaccines to community members.
Conclusion
Achieving the SDGs agenda and containing the COVID-19 pandemic are the most recent attempts at improving the standards of living of UN member states and the global community. However, attaining SDG 3 (healthy living for all at all ages) will likely not be achieved by the target date of 2030 in Osun State, Nigeria. This is because the result of this study has shown that the number of available PHC facilities is not evenly distributed and cannot adequately cater to the growing population, especially at a time of the unexpected COVID-19 pandemic, particularly in urban areas that have been largely congested due to rural poverty.
A strong understanding of the vital role of PHCCs in the health care delivery system will enhance the necessary response to the COVID-19 pandemic and the containment of the virus, especially in reducing overcrowding at higher levels of health care facilities and in the distribution of COVID-19 vaccines to community members. Thus, there is a need for government intervention in the provision of PHC in Osun State for adequate and equal distribution to achieve SDGs and to contain the COVID-19 pandemic in the state.
Footnotes
Acknowledgments
The authors are grateful to Osun State Ministry of Health and Osun State Hospital Management Board for providing data for the study.
Authors’ Contributions
All the authors made sufficient contributions to this work, and the content of the manuscript has never been previously published or submitted elsewhere.
Declaration of Conflicting Interests
The authors declare no potential conflict of interests.
Funding
Authors received no financial support for the research, authorship, and/or publication of this article.