
Abstract
Keywords
Introduction
Family burden refers to the presence of problems, difficulties or adverse events that affect the life of the psychiatric patient’s significant others, for example, members of the household and/or the family (Platt, 1985). For a number of years, it was believed that bipolar affective disorders with episodic course and better inter-episodic recovery do not cause chronicity or have an adverse effect on the functioning of the patient, thereby incurring minimum burden on the family. However, research in the last two decades has documented a high level of burden in caregivers of bipolar disorder. Manic episodes in bipolar affective disorder causes disruption in the social and functional well-being of the affected individual and often requires hospitalization resulting in significant burden on the family. Moreover, bipolar disorder has been reported to be the most expensive behavioural healthcare diagnosis, both for patients with bipolar disorder and for their insurance plans (Goetzel et al., 2003; Peele et al., 2003). Almost all (93%) the caregivers of patients with bipolar disorder experienced moderate or severe degree of burden in at least one domain and about half (54%) reported overall severe levels of burden (Perlick et al., 1999). The relatives of patients with bipolar affective disorder rated manic symptoms more burdensome as compared to those of patients with schizophrenia (Mueser et al., 1996). Evaluation of the impact of family burden and symptoms status on the course of bipolar disorder revealed that the greater the burden, the greater are the chances of relapse (Perlick et al., 2001). Family burden was noted to be higher when patient’s symptoms and disability were more severe, and when the relatives had less psychological support and help in emergencies from the social network (Magliano et al., 2009). Primary caregivers of patients with bipolar disorder experience moderate or higher burden in relation to patient problem behaviours, role dysfunction and disruption of household routine. Those with higher burdens reported more physical health problems, depressive symptoms, health risk behaviour, health service use and less social support. They also provide more financial support to their bipolar relatives (Perlick et al., 2007). The caregivers of patients with bipolar disorder were found to be burdened for about 8–10 months of the year during one year of follow-up (Zergaw et al., 2008). They showed a significant reduction in burden one year after their ill relative was discharged from the hospital (Heru and Ryan, 2004).
In low-income countries like India, where the majority of mentally ill patients stay with their families, the already meager resources of the family may be disproportionately affected by having a family member with bipolar disorder. This is further compounded by the lack of adequate resources and psychiatric facilities in the country. In the 1990s, studies from India reported that burden of care experienced by family members of bipolar affective disorder is considerable and is experienced in the areas of family routine, family leisure, family interaction and finances; the pattern of burden is almost the same as that in relatives of patients with schizophrenia (Chakraborty et al., 1992, 1995). However, these studies were cross-sectional; there is a lack of follow-up studies of the caregivers of patients with bipolar disorder documenting change in the burden they experience. These studies are required to plan and initiate family interventions at the time of hospitalization of the ill relative to reduce family burden. The present study was designed to evaluate the change in family burden in the short term in the caregivers of hospitalized patients with bipolar affective disorder currently in mania, with the following objectives.
To assess the burden experienced by family members caring for patients with bipolar affective disorder, currently in mania.
To assess the changes in family burden with treatment in the short term at follow-up four weeks after discharge.
Material and methods
Study design
The present study had a longitudinal prospective design.
Universe
The study was conducted in the department of psychiatry, All India Institute of Medical Sciences (AIIMS), a tertiary care general hospital in northern India. The psychiatry ward of AIIMS is 30 bedded; one family member has to stay with the patient during the period of hospitalization.
The general hospital psychiatric units are the mainstay of clinical services, teaching and training, and research in mental health in India. These units came into being in independent India at the beginning of the 1950s. Before then, all mental healthcare was custodial in nature and limited to mental hospitals only. This led to the care of the mentally ill being inaccessible and stigmatized. Now almost all medical colleges, which necessarily have a general hospital with all medical disciplines, have such psychiatric units serving all these functions. The basic idea of starting psychiatric services in a general hospital setting was to integrate mental health services with general health services to make them easily accessible to the general population and to reduce discrimination and stigma suffered by mentally ill patients.
The outpatient services of such units are open to all, and a patient can just walk in and seek help on a voluntary basis. The inpatient services are also voluntary in nature and patients are admitted in an open ward like any other ward (medical, surgical, gynaecological, etc.). It is mandatory for a family member to accompany the patient for admission and remain with him/her throughout the period of stay. During hospitalization, the family can replace one relative with another. This practice was introduced and has remained over time for the family to provide much-needed support to the patient, so that he/she does not feel abandoned. The family also witnesses improvement in its own patient as well as other patients, which helps to fight the stigma. The patient and relative stay in the same room or cubicle (where more than one patient stays).
Since the hospital in the present study is a government-funded institution, the charges are minimal and it provides patients with all clinical care, medicines and food. Laboratory investigations are charged to the patient, which are again highly subsidized.
Inclusion criteria
Patients with bipolar affective disorder currently in mania diagnosed according to International Classification of Diseases and Related Health Problems – 10th revision, Diagnostic Criteria for Research (ICD-10, DCR) (World Health Organization, 1993).
Either gender, aged between 25 and 45 years.
Availability of a family member for study who was staying with patient, fulfilling any three of the following criteria:
– Parent or spouse
– Had most frequent contact with the patient
– Helped to support the patient financially
– Had most frequently been a participant in patient’s treatment
– To be contacted by treatment staff in case of an emergency.
Both patient and relative willing and able to give informed consent.
Exclusion criteria
Patients with any other major physical or mental illness.
History of substance abuse other than tobacco both on the part of patient or the family member.
Unwilling to participate.
Instruments
International Classification of Diseases and Related Health Problems – 10th revision, Diagnostic Criteria for Research (World Health Organization, 1993).
Structured proforma to collect clinical and sociodemographic data.
Young Mania Rating Scale (YMRS) (Young et al., 1978).
Family Burden Assessment Scale (FBAS) (Pai and Kapur, 1981), which is a semi-structured interview schedule and assesses objective and subjective family burden in the Indian context. Objective burden is assessed by 24 questions covering six areas such as financial burden, disruption of routine family activities, disruption of family leisure, disruption of family interaction, effects on physical health of other family member and effects on mental health of other family member. Subjective burden is rated by the family member.
Procedure
The consecutive hospitalized patients with a diagnosis of bipolar disorder were screened and those meeting the inclusion and exclusion criteria were enlisted for the study. They were assessed twice: first, within three days of admission and then during follow-up at four weeks after discharge. Informed consent from the relative and patient was taken for the study. At the time of the first assessment, sociodemographic and clinical information was collected on a semi-structured performa, YMRS was applied to the patient to rate the severity of mania, and the family member was interviewed using FBAS to assess burden. At four weeks after discharge, the same family member was again assessed on FBAS. The plan for management and discharge of patients was decided by the treating team. This team comprises consultants, junior and senior residents, a ward nurse and a social worker. The decision is based on the clinical parameters as well as assessment on objective structured rating scales.
Statistical analysis
Descriptive analysis was done for continuous and categorical variables. To study the relationship between various parameters of family burden at admission and follow-up, paired t-test was used. Pearson’s correlation coefficient was used to find a correlation between various clinical variables and parameters of family burden.
Results
Participants’ characteristics
A total of 82 patients admitted consecutively over a period of 15 months were screened. Forty six patients were excluded; 29 patients did not meet the inclusion criteria for age (19 patients < 25 years and 10 patients > 45 years), 9 patients had problems in diagnosis, 6 patients had co- morbid medical or substance use, and 2 patients came from a long distance away. Thirty six patients could be included in the study; two patients were lost on follow-up due to distance and lack of communication. Thus, a total of 34 patients completed the study. The mean age of the study population was 29.50 years. About three fifths (58.8%) of the patients were male, the majority (94.1%) were Hindu and about two thirds were married. All the patients were educated and about 90% were educated to at least 12th standard. Half (50%) of the patients were employed. The majority (94.1%) were from an urban area. The majority also had a family income of ≥ INR 5,000 per month. About three quarters (79.4%) of the patients belonged to a nuclear family.
The mean age of the relatives was 44.65 years. There was an equal number of males and females; 64.8% were married, 20.6% were divorced, separated or widowed and 14.7% were unmarried; 58.8% of them were parents, 26.5% were siblings and 14.7% were spouses. About half had studied to at least 12th standard; 44.1% were housewives, 38.45% were employed, 8.8% were students and 8.8% were retired.
The clinical variables
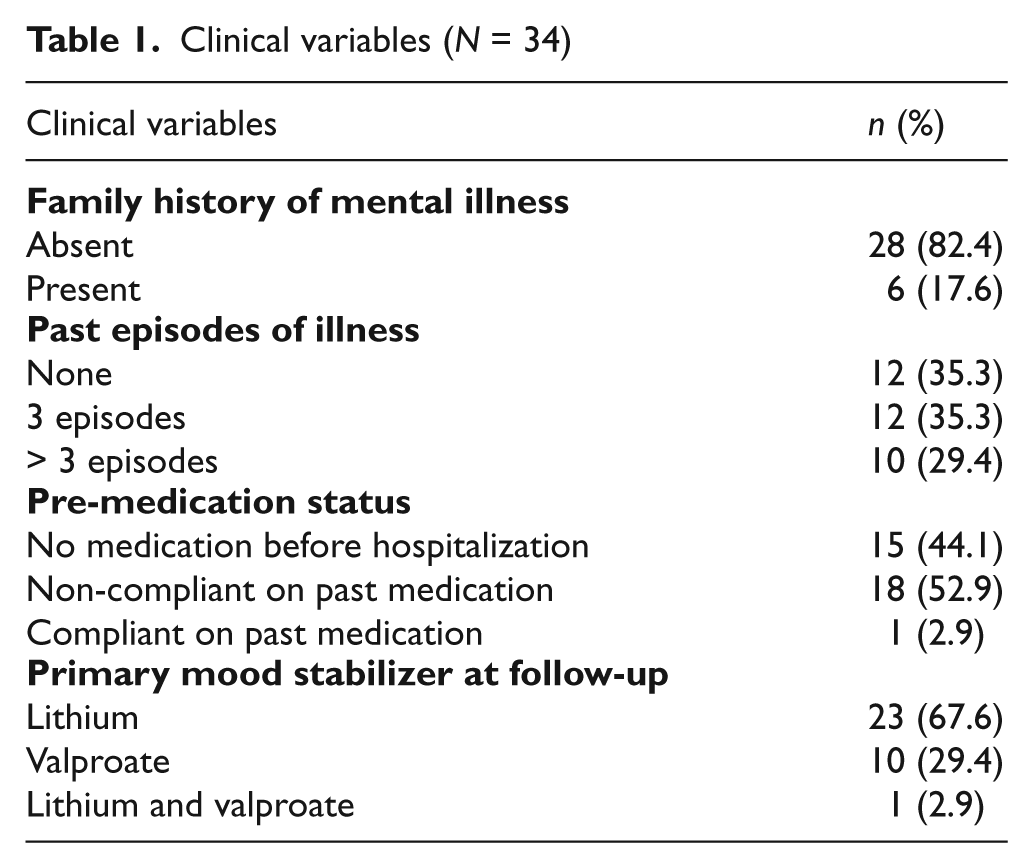
In four fifths of the patients, a family history of psychiatric illness was absent; in patients with a positive history, all the affected family members had affective disorder; 64.7% had had episodes in the past; 8.8% had had their last episode five years before and had remained symptom free since then. Of the patients, 35.3% had had up to three episodes, 29.4% had had more than three episodes and for 35.3%, the presenting illness was their first episode. 44.1% were not on any medication before the current hospitalization; 52.9% were non-compliant with the medicines prescribed at the outpatient service. One patient was fully compliant (adequate serum level of lithium maintained) but he still had the current episode. At follow-up, 67.6% of the patients were receiving lithium as the primary mood stabilizer while 29.4% were on valproate. Only one patient was receiving both lithium and valproate (Table 1).
Clinical variables (N = 34)
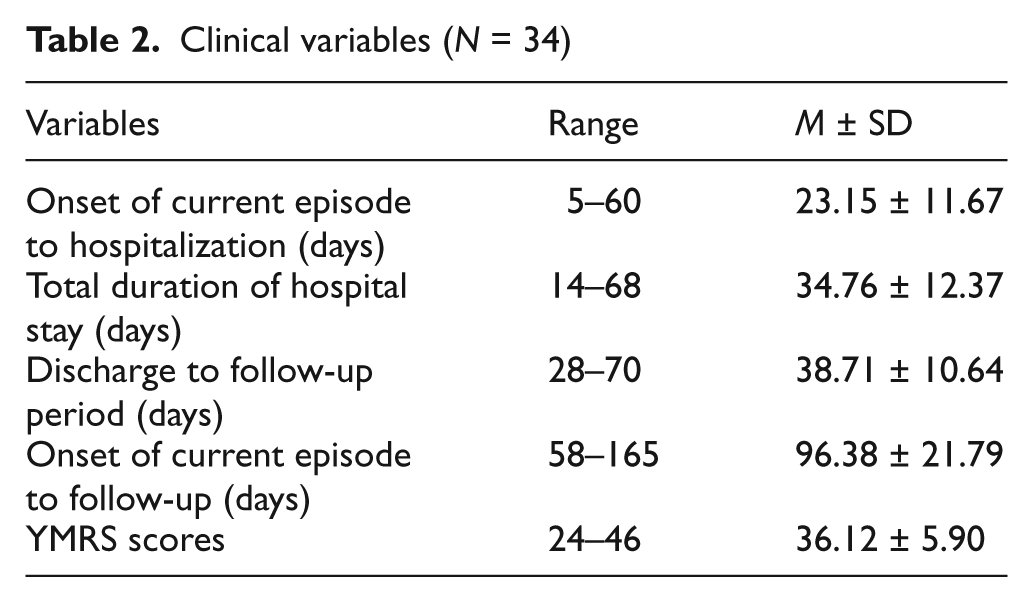
The mean duration from the onset of the current episode to hospitalization was 23.15 days. The mean duration of hospital stay was 34.76 days. At the time of the second assessment, the mean duration of follow-up was 38.71 days. The mean YMRS score at the time of admission was 36.12 (Table 2).
Clinical variables (N = 34)
Family burden
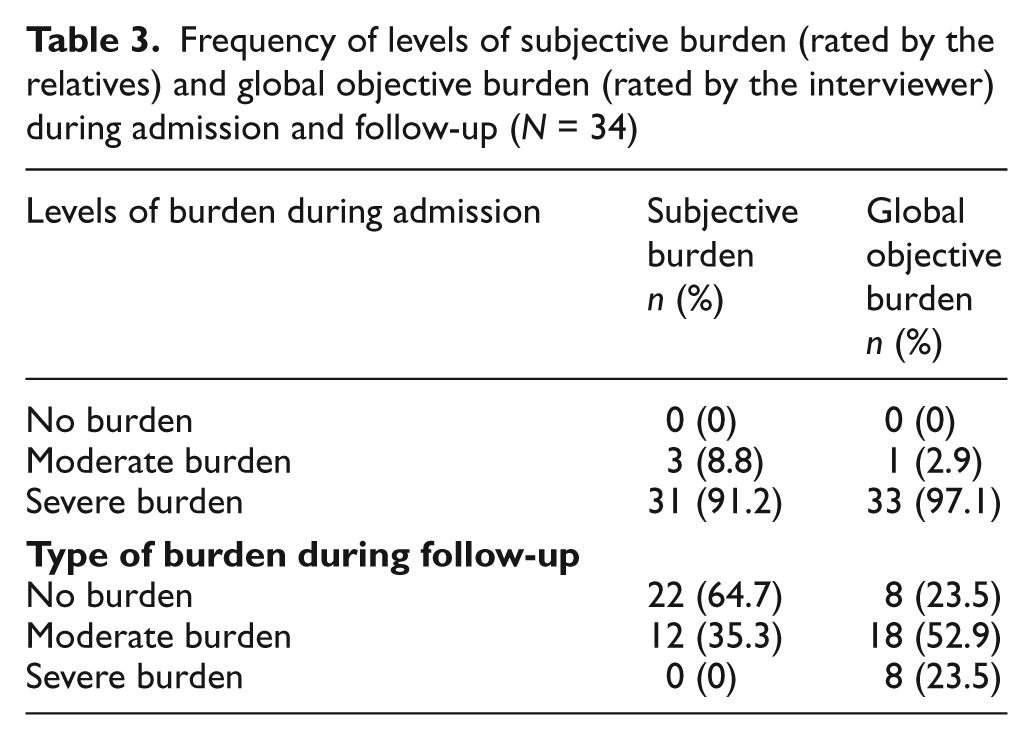
The frequency of levels of subjective burden was rated by the relatives and total objective burden was rated by the interviewer. At the time of hospitalization, the subjective and objective family burden was severe in 91.2% and 97.3% and was moderate in 8.8% and 2.7% of the family members, respectively; none of the family members was free from burden. At the time of discharge, none of the family members reported severe burden subjectively while the objective burden was rated to be severe in about a quarter (23.5%). The subjective and objective family burden was moderate in about one third (35.3%) and about a half (52.9%) of the family members, respectively; a quarter (23.5%) and two thirds (64.7%) of the family members did not experience any burden (Table 3).
Frequency of levels of subjective burden (rated by the relatives) and global objective burden (rated by the interviewer) during admission and follow-up (N = 34)
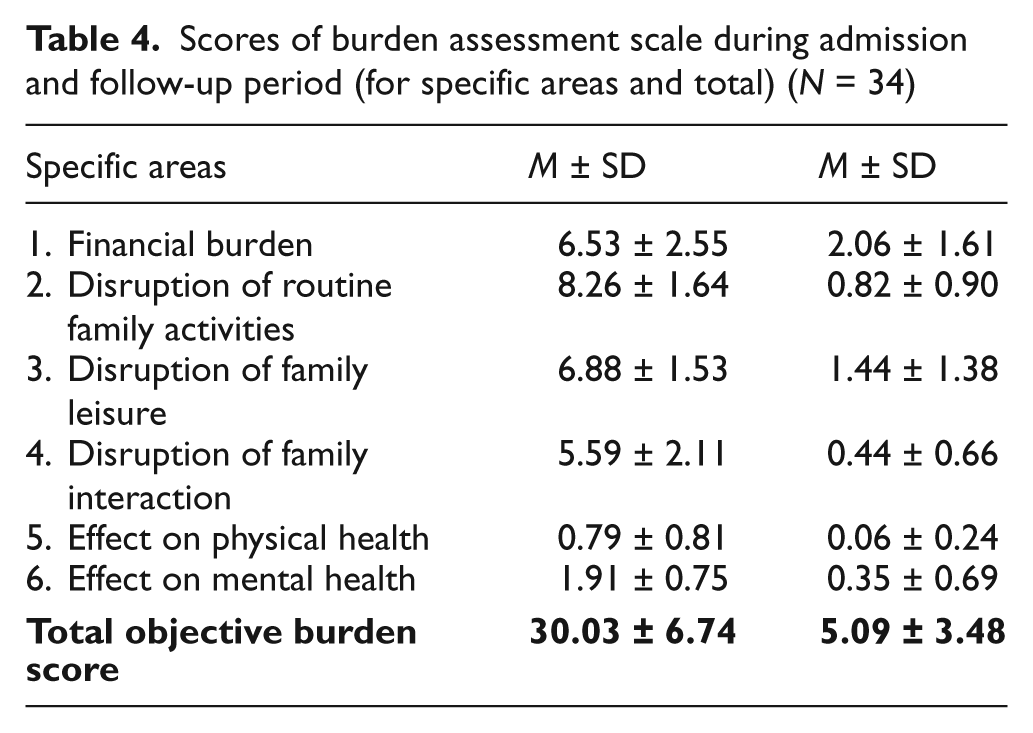
The family burden was further assessed for effect on finances, routine family activities, family leisure, family interaction, physical health and mental health. Higher mean scores were found in the disruption of routine activities, family leisure activities and financial burden. However, the scores for effect on mental health and physical health remained lower. At follow-up, there was a substantial reduction in the mean scores in all areas of burden, but the scores remained highest in the area of financial burden. At admission and at follow-up, mean scores of total objective burden (total sum of scores in all areas of FBAS) were 30.03 and 5.09, respectively; there was a substantial reduction in the total objective burden score during the follow-up period (Table 4).
Scores of burden assessment scale during admission and follow-up period (for specific areas and total) (N = 34)
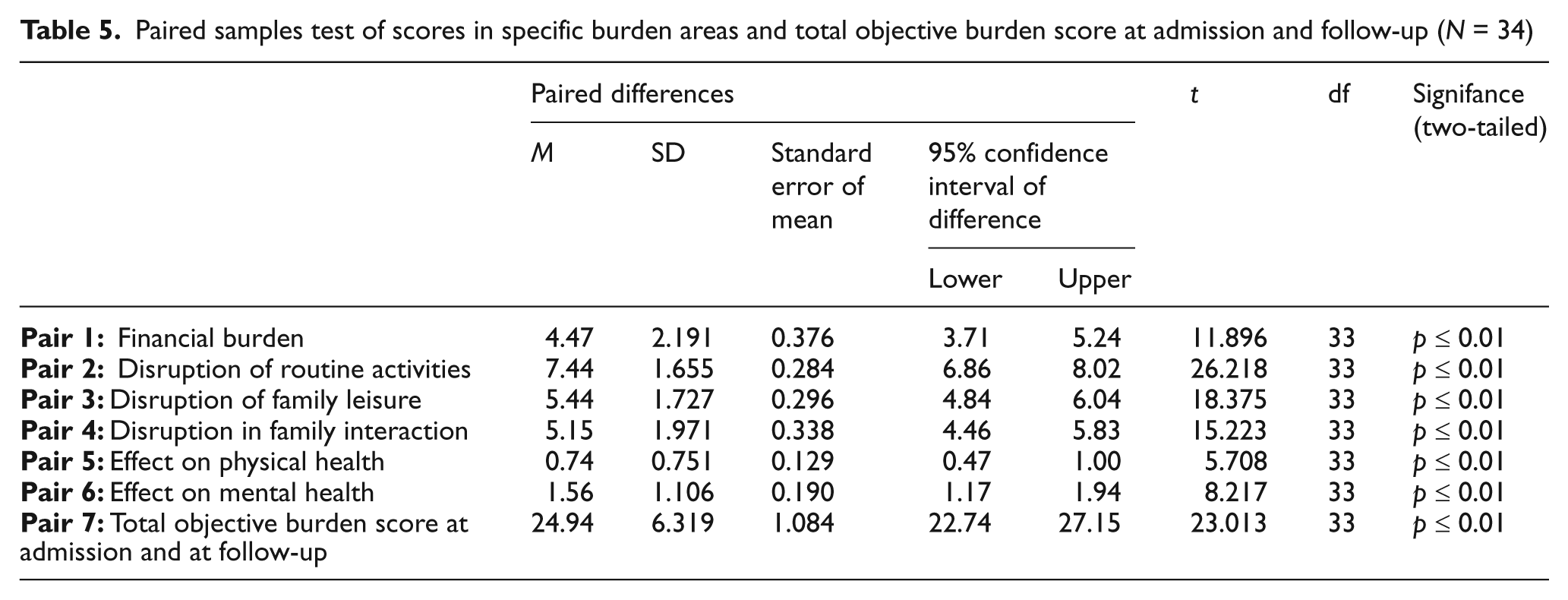
There was a highly significant difference on the paired samples test of scores in specific burden areas and total objective burden score at admission and follow-up (Table 5).
Paired samples test of scores in specific burden areas and total objective burden score at admission and follow-up (N = 34)
At the time of hospitalization, there was a positive correlation between symptoms severity with period since onset of current symptoms. A positive correlation was also found between total objective burden score and subjective and global objective burden score. There was also a positive correlation between total objective burden and each area of FBAS. Subjective burden score and global objective burden score also had a positive correlation. There was no significant correlation between symptoms severity on YMRS scores with the sociodemographic profile of patients and relatives. Neither was there a significant correlation between sociodemographic profile of patients and relatives and different burden scores and with other clinical variables (Table 6).
Correlations of clinical variables during admission and follow-up (N = 34)

At the four-week follow-up, total objective burden score had a positive correlation with subjective burden score. Total objective burden score also had a positive correlation with scores of financial burden, disruption in routine activities, family leisure and effect on mental health. There was no significant correlation between sociodemographic variables and clinical variables (Table 6).
Discussion
Thirty four consecutive hospitalized patients with bipolar disorder currently in mania of either gender, with an age range of 25–45 years, were prospectively recruited over a period of 15 months to evaluate the family burden due to the patient’s illness at the time of admission and during follow-up at a minimum of four weeks after discharge. This is the first study from India exploring changes in family burden in the short term.
The mean age of the patients was 29.50 years with male preponderance. About two thirds of the patients were unmarried, divorced, widowed or separated; this probably reflects difficulties in maintaining relationships. These findings are in line with earlier studies; 50%–80% of patients with bipolar disorder were noted to be single, divorced, separated or widowed (Dore and Romans, 2001; Gitlin et al., 1995; Perlick et al., 1999). Most of the patients hailed from nuclear families, belonged to lower and middle socioeconomic status and were educated, reflecting the urban nature of the sample which clearly corroborated the urban residence of the patients.
The mean age of the relatives was 44.65 years, with an equal number of males and females. Most were married and employed. Their relationship to the patients suggested that the majority of the patients were cared by their parents, with good support from other family members. The findings of this study are in line with others. Perlick et al. (1999) found that parents (44.3%) were the main caregivers, and mothers (73%) were the main caregiving parent (Dore and Romans, 2001).
A family history of psychiatric illness was present in one fifth of the patients; all had had affective disorder. Vocisano et al. (1996) observed a similar finding. About two thirds of the patients had had more than one episode, suggesting early onset and recurrent episodic nature of bipolar disorder. Similar results showing that a significant number of patients (44%–80%) would have multiple episodes or relapse have been reported (Gitlin et al., 1995; Miklowitz et al., 1988; O’Connell and Mayo, 1981). More than half of the patients were non-compliant with the treatment regime, which is consistent with previous studies where it was reported that 40%–60% of patients were non-compliant (Gitlin et al., 1995; Miklowitz et al., 1988). During the follow-up, most of the patients were receiving mood stabilizers. The mean time period from onset of current symptoms to hospitalization was about three weeks. The mean duration of hospital stay was almost five weeks; this is shorter than reported in an earlier study of hospitalized patients with mania (Olie and Levy, 2002). The short duration of hospitalization could be because of the resource crunch, a perennial problem associated with the availability of psychiatric beds in low-income countries like India. It may also reflect family’s preference to take care of the patient at home, once the patient becomes manageable. Since it is mandatory for a family member to stay with a patient who has been admitted to the inpatient facility in this study, to provide personalized care as well as to make the hospitalization experience informal, this may inconvenience the family by disrupting its routine activities. Although these patients were hospitalized for a short time, they all came for follow-up in the outpatient department. About three months had passed between the onset of current symptoms and the second evaluation during follow-up. The average mean score on YMRS was quite high at admission, reflecting the need for admission. During follow-up, patients did not have any symptoms of mania as per ICD-10, DCR; therefore, YMRS was not applied.
At the time of hospitalization when the patients had acute illness, all the family members reported having burden and more than 90% of them perceived severe burden, indicating the effect of severity of mania on the family. This is consistent with earlier findings (Dore and Romans, 2001; Perlick et al., 1999) and is in line with earlier studies where FBAS was used to assess family burden (Chakraborty et al., 1995; Gautam and Nijhawan, 1984; Martyns-Yellowe, 1992). After discharge at follow-up, the patients had improved significantly but family burden persisted in more than half of the family members. A rapid decrease in burden score suggests that with treatment, there was a significant improvement in patient’s illness, which probably came as a relief to the relative. It also signifies the impact of the sudden and acute nature of a manic episode on the subjective and objective burden experienced by the family. There is no study evaluating the changes in family burden in the short term for comparison, however, at one-year follow-up a reduction in burden has been reported (Heru and Ryan, 2004) and the burden persisted for 8–10 months (Zergaw et al., 2008).
At the time of admission and follow-up, the scores in specific areas of family burden highlight the fact that initially at the time of acute illness and subsequent hospitalization, the disruption of family routine and other activities is the major worry for the family. However, later on, as the patient recovers, the finances become a major concern as the money for treatment for the episode comes out of the family’s resources; this is compounded by the loss of employment opportunity for both the patient and the caregiver. Another interesting finding was the discrepancy between the objective and subjective burden; Chakraborty et al. (1992, 1995) noted a similar discrepancy between two burden types in patients with bipolar affective disorder. This suggests that family members perceive less burden, suggesting coping, adjustment and increased tolerance on their part.
Limitations
This study had a few limitations. The hospitalization may be a confounding factor as it in itself contributes towards the family burden. Therefore, to tease out the effect of hospitalization from the patient’s illness, a control group from an outpatient setting could have been taken for better comparison. As the same interviewer did the ratings at both points, this might have resulted in observer bias. Also, only patients aged 25–45 years were included in the study which restricted entry of many younger patients; therefore, the burden experienced by families of younger patients cannot be commented upon.
Conclusion
Like any other mental illness, bipolar affective disorder also has adverse effects on the patient’s family. In this study, all the family members experienced burden initially due to the acuteness of the manic state of the patients; in the majority of the cases, the burden was severe. Specific areas where burden was noticed were in finance, routine activities, leisure and interaction of the family. Even when symptoms subsided, the family members continued to experience burden, specifically related to finances. This study supports earlier observations that objective burden as assessed by the interviewer was significantly higher than the subjective burden as experienced by family members. In the future, to document changes in family burden and factors associated with its decrease or increase, there is a need for longitudinal, multicentric studies recruiting subjects from community, outpatient and hospital settings, which are designed to unravel the complex association between various variables and burden experienced by family members of patients with bipolar affective disorder. This will help in planning specific interventions to reduce burden experienced by family members of patients with bipolar disorder.